effects of monotherapy with sustained-release verapamil on blood pressure, lipid levels, renal...
TRANSCRIPT

CURRENT THERAPEUTIC RESEARCH VOL. 54, NO. 2, AUGUST 1993
EFFECTS OF MONOTHERAPY WITH SUSTAINED-RELEASE VERAPAMIL ON BLOOD PRESSURE, LIPID LEVELS, RENAL
FUNCTION, DIABETIC CONTROL, AND PATIENT WELL-BEING IN PATIENTS WITH MILD TO MODERATE HYPERTENSION
COLIN BARNES, 1 PETER G. HAMILTON, 2 AND MARCEL LEBEL s
Departments of Medicine, 1McMaster University, Hamilton, Ontario, 2University of Alberta, Edmonton, Alberta, and 3Laval University, Quebec, Quebec, Canada
ABSTRACT
The effects of sustained-release (SR) verapamil (Isoptin ® SR) mono- therapy on blood pressure (BP), lipid levels, renal funct ion, diabetic control , and pa t ient well-being were investigated in an open-label mul- t icenter t r ia l of 507 pat ients with mild or moderate hypertension. Newly diagnosed and previously treated pat ients received SR verapam- il 240 mg once daily for 6 weeks, with the option of t i t r a t ing dosage to a max imum of 480 mg/day. Equal numbers of men and women (251 men, 251 women, 5 not reported) with an average age of 60 years were enrol led in the study. The greatest decreases in BP were achieved between basel ine and week 2, when (mean -+ SD) BP fell from 163 - 20 mmHg systolic (SBP)/98 -+ 9 mmHg diastolic (DBP) to 149 -+ 17 mmHg SBP/88 +- 9 m m H g DBP. Blood pressure readings after 6 weeks of t r ea tmen t were 147 - 17 mmHg SBP/86 - 9 mmHg DBP. The mean percentage decrease in BP by week 6 was 9.24% for SBP and 12.21% for DBP. SR verapamil was found to be as efficacious in pat ients age >64 as in younger pat ients . No s ignif icant difference in BP response was observed when pat ients were stratified by age. Overall, 85% of pat ients a t ta ined goal BP (ie, DBP ~<90 mmHg or a ~>10-mmHg decrease in DBP). Target BP was reached by 80% of pat ients with mild hyperten- sion at basel ine and 87% of those with moderate hypertension. Treat- men t with SR verapamil had a beneficial effect on lipid levels and pa t ient well-being; no effects on renal func t ion or glycemic control were noted. Side effects were reported by 114 (22.5%) patients; the most commonly reported effect was mild const ipat ion (10.7%). The authors conclude tha t SR verapamil is a safe and effective drug in the t r ea tmen t of hypertension.
INTRODUCTION
Calcium channel blockers have gained greater acceptance as first-line drug therapy in the treatment of mild to moderate hypertension. 1-5 The increased use of both calcium channel blockers and angiotensin-converting enzyme (ACE) inhibitors may be partly related to the adverse metabolic
Address correspondence to: Dr. Colin Barnes, McMaster Clinic, Henderson General Hospital, 711 Conces- sion Street, Hamilton, Ontario, Canada L8V 1C3. Received for publication on May 6, 1993. Printed in the U.S.A. Reproduction in whole or part is not permitted.
127 0011-393X/93/$3.50

BP, LIPID, RENAL, GLYCEMIC, AND QOL EFFECTS OF SR VERAPAMIL
effects often experienced by patients taking diuretics and beta-blockers. 6 Because newer calcium channel blockers and ACE inhibitors do not appear to affect glucose metabolism and blood lipid profiles, their use in primary prevention might eventually help to reduce mortality and morbidity from coronary artery disease}
Although large, prospective, multicenter studies are needed to resolve this issue, it is unlikely that such studies will be completed in the near future. We therefore set a more modest goal of studying the effect that a short course of monotherapy with a sustained-release (SR) preparation of verapamil* might have on the lipid profile, renal function, glucose toler- ance, and well-being of older patients with mild to moderate hypertension.
The stringently enforced protocols necessary for assessing the safety and efficacy of a drug during the drug approval process, although invalu- able, may not provide the clinician with entirely useful information. Pa- tients having many of the conditions excluded in premarketing tr ials-- such as preexisting or concomitant disease and/or therapy--comprise the greatest percentage of study populations in large-scale postmarketing studies, which have the goal of evaluating the various aspects of treatment generally not assessed during earlier research. These large-scale evalua- tions contribute to our knowledge base for optimizing drug therapy in actual clinical situations.
As mentioned, the present study discusses only one drug treatment group, and there are no inherent guidelines for comparison. Study results, however, corroborate those found in randomized clinical trials conducted elsewhere and may be extended to represent a more heterogeneous patient population. Of course, the current patient population is representative of patient types normally found in clinical practice.
The primary objective of these four clinical trials was to assess the antihypertensive effectiveness and tolerability of monotherapy with SR verapamil over the course of 6 weeks. A specific secondary objective of each clinical trial was to study the effect of SR verapamil on lipid levels, renal function, glycemic control in diabetic patients, and patient well-being.
P A T I E N T S AND M E T H O D S
Newly diagnosed patients (n = 128) and previously treated patients (n = 376; 3 not reported) thought to require a change in antihypertensive ther- apy were eligible for the study. (The case report form did not request information on the duration of hypertension from those being switched from other medications.) Patients 50 years of age or older with documented mild to moderate hypertension were recruited. Blood pressure criteria for inclusion were defined as a sitting or lying diastolic blood pressure (DBP)
* Trademark: Isoptin ® SR (Searle Canada Inc., Oakville, Ontario, Canada).
128

C. BARNESET AL.
of 90 to 114 mmHg. Severity of hypertension was defined as diastolic blood pressure of 95 to 104 mmHg (mild), 105 to 115 mmHg (moderate), >115 mmHg (severe), and <95 mmHg (other). Pat ients with any of the contrain- dications described in the Isoptin ® SR product monograph, as well as pa- t ients requiring more than one antihypertensive agent, were excluded.
Of the 507 patients enrolled, 51 were under 50 years of age; 7 were not reported. A total of 10 patients (four under 50 years of age) had severe hypertension and represent protocol violations. None of the patients were reported as receiving combination therapy.
The individual studies had additional inclusion and exclusion criteria. For the lipid study, patients who required antihyperlipidemic therapy or a change in diet were excluded. In the renal function study, patients who required a change in current concomitant renal therapy or diet were ex- cluded. In the diabetes study, pat ients with well-controlled insulin- dependent or non-insul in-dependent diabetes melli tus were eligible to participate in the study; however, patients requiring a change in diabetic therapy or diet were excluded. Newly diagnosed patients or those requir- ing a change of antihypertensive therapy were eligible for the well-being study. Pat ients who lived alone were excluded, because a live-in par tner was necessary for completion of the partner questionnaires.
Five hundred physicians throughout Canada, mostly family practitio- ners, were invited to participate in this study. Each was asked to enroll one patient in each of the four studies. At the initial visit, patients were screened and, if eligible, gave their consent to participate. At this visit, patients provided a medical history, underwent a physical examination, and had their blood pressure measured.
Pat ients were reexamined by their physician after 2 and 6 weeks. At each visit, the physical examination and blood pressure measurements were repeated. The physician was requested to indicate adverse events in the withdrawal section of the case report forms. A global evaluation was performed at week 6. The goal of therapy was a DBP ~<90 mmHg or a decrease of i>10 mmHg at the final study visit. The final study visit was the week-2 visit if data were not given for week 6. This affected 10% of patients; 90% completed the study.
No data concerning Korotkoff sounds were available or recorded. Blood tests were required on admission and at week 6, as follows: lipid
study: total cholesterol, high-density lipoproteins (HDL), low-density li- poproteins (LDL), and triglycerides; renal function study: creatinine and blood urea nitrogen; and diabetes study: glycosylated hemoglobin.
At admission and at week 6, patients in the well-being study and their live-in partners were required to complete a well-being questionnaire. The patient questionnaire was completed at the physician's office, but the live- in par tner questionnaire was completed at the patient 's home and mailed directly to Searle Canada Inc.
129

BP, LIPID, RENAL, GLYCEMIC, AND QOL EFFECTS OF SR VERAPAMIL
On study entry, patients discontinued all currently administered an- t ihypertensive medications and began receiving SR verapamil 240 mg once daily in the morning with food. If necessary, dosage was increased by half-tablet increments in the evening, to a maximum of 480 mg/day.
Data entry and statistical analysis were completed by Innovus Inc. (Hamilton, Ontario, Canada). Data analysis was performed using SAS version 6.03 and BMDP-UX (1987) software packages. Results include an intent-to-treat analysis. Descriptive analysis was conducted on all para- metric variables using the mean -+ standard deviation. The number of pat ients on which the values of certain parameters are based differs slightly from the total number because complete data were not available for all patients. Pat ients with missing values were excluded from the cal- culation of percentages.
RESULTS
Efficacy
A total of 507 patients (251 men, 251 women, 5 not reported) were enrolled in the four trials and were assessable for efficacy and safety. Of these, 457 (90%) patients completed the 6-week study; 50 (10%) patients withdrew prematurely, 37 (7%) because of side effects.
The mean age of study participants was 60 years (range, 31 to 89 years). The age distribution of patients was as follows: 10.1% younger than age 50, 58.2% between ages 50 and 64, and 30.4% older than age 64. Fifty-one patients younger than age 50 were enrolled in the study, even though this was an exclusion criterion. Data from these patients were included in all analyses. This was a protocol violation. The critical param- eters of a t ta inment of blood pressure goal by severity were broken out by age groups to ensure that the younger patients had no effect on the results. Renal function, diabetes, and well-being showed no impact. Age was not a covariate in the lipid analysis.
Approximately 75% of patients had been treated previously for hyper- tension. Fifty-five percent had been previously t reated with monotherapy, primarily beta blockers (20%) or diuretics (15%). Twenty-one percent had previously received combination therapy, principally beta blockers com- bined with diuretics (9%).
Almost half (48%) of the patients had been diagnosed as having mild hypertension on entry; 22% and 2% of patients had moderate and severe hypertension, respectively. Twenty-eight percent had a DBP <95 mmHg, presumably because they either had borderline hypertension or were being t reated with another antihypertensive agent immediately before entering the study.
The greatest decreases in blood pressure were seen between baseline and week 2. Blood pressure fell from 163 -+ 20 mmHg systolic (SBP)/98 -+
130

C. BARNESET AL.
9 mmHg DBP to 149 -+ 17 mmHg SBP/88 - 9 mmHg DBP after 2 weeks of treatment and to 147 -+ 17 mmHg SBP/86 + 9 mmHg DBP after 6 weeks of treatment. The mean percentage decrease in blood pressure by week 6 was 9.24% for SBP and 12.21% for DBP.
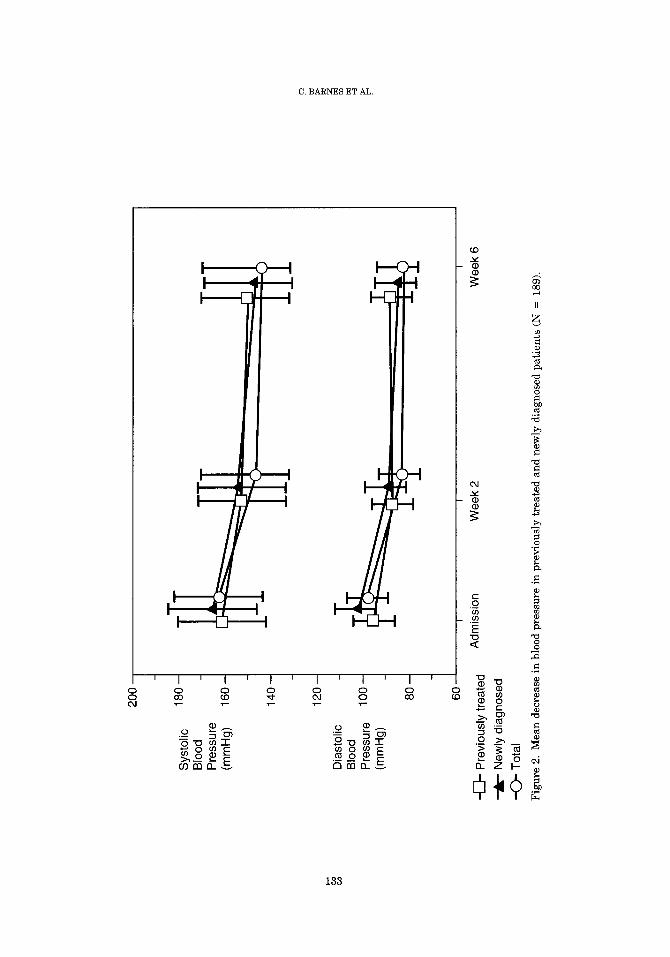
Blood pressure decreased in all age groups during the 6-week study, with patients younger than age 50 having the greatest overall decrease (Figure 1). Patients older than age 64 had the largest decrease in blood pressure between baseline and week 2. Blood pressure fell in both previ- ously treated and newly diagnosed patients (N = 189) during the 6-week trial. The reduction was more pronounced in the newly diagnosed patients because they had higher blood pressures at admission. At week 6, the blood pressures in both groups were similar (Figure 2).
A subgroup analysis of 84 patients previously treated with at least two antihypertensive medications who switched to SR verapamil monotherapy indicated a change in blood pressure from 161 + 20 mmHg SBP/96 -+ 11 mmHg DBP at admission to 151 -+ 17 mmHg SBP/87 +- 10 mmHg DBP at week 2, to 150 -+ 21 mmHg SBP/86 -+ 9 mmHg DBP by week 6. The mean percentage decrease in blood pressure in this group was 5.48% for SBP and 9.95% for DBP.
Overall, 85% of study patients attained goal blood pressure (Table I). Eighty percent of patients with mild hypertension and 87% of those with moderate hypertension a t baseline attained the goal. The percentage of patients attaining the goal rose with both increasing age and severity of hypertensive disease. The trend toward greater drug effectiveness with increasing age was most pronounced in patients with DBP < 104 mmHg at baseline.
Data describing the patient subgroup newly diagnosed for hyperten- sion are shown in Table II. Overall, a similar percentage (83%) of these patients attained goal blood pressure. In this subgroup, the percentage of patients who attained the goal increased with severity of hypertension, but not with age. Age may be a surrogate measure of history of disease; how- ever, data on duration of hypertension were not collected in this study.
As shown in Figure 3, patient acceptance of SR verapamil was good or excellent in 90% of patients.
Physician assessments of drug efficacy were recorded as good or ex- cellent for 89% of patients (Figure 4), ranging from 79% for the youngest age group, to 87% for the middle age group, to 93% for the oldest age group. Eighty-eight percent of patients were reported to be continuing SR ve- rapamil treatment after trial completion.
Lipid Study
A total of 192 patients were enrolled in the lipid study; 52 (28%) were newly diagnosed hypertensive patients and 137 (72%) had been treated previously. Three patients with missing values were excluded from
131

200
b~
Sys
tolic
B
lood
P
ress
ure
(mm
Hg)
Dia
stol
ic
Blo
od
Pre
ssur
e (m
mH
g)
< 50
yr
50-6
4 yr
-C
)"
> 64
yr
180
-
160
-
140
120
100 80
-
60
I I
Adm
issi
on
Wee
k 2
I
Wee
k 6
Fig
ure
1. M
ean
decr
ease
in
bloo
d pr
essu
re,
by a
ge.
== ~3
0 ©
<
200
O3
Sys
tolic
18
0 -
Blo
od
Pre
ssur
e (m
mH
g)
160
-
140
-
12
0-
Dia
stol
ic
Blo
od
Pre
ssur
e lO
0-
(mm
Hg)
80
-
60
Pre
viou
sly
trea
ted
New
ly d
iagn
osed
-O-
Tot
al
I I
I
Adm
issi
on
Wee
k 2
Wee
k 6
Fig
ure
2.
Mea
n d
ecre
ase
in b
lood
pre
ssur
e in
pre
viou
sly
trea
ted
and
new
ly d
iagn
osed
pat
ien
ts (
N =
18
9).

BP, LIPID, RENAL, GLYCEMIC, AND QOL EFFECTS OF SR VERAPAMIL
Table I. Overall attainment of goal* blood pressure: Intention to treat by severity of hyper- tension at baselinet frequencies:
Age (yr)
<50 50 to 64 >64 Total N (%) N (%) N (%) N (%)
Total:l: 51 295 154 507 Total controlled 38 (75) 253 (86) 138 (90) 429 (85)
Severity at baseline Mild
Total controlled 20/29 (69) 115/142 (81) 53/64 (83) 193/241 (80) Moderate
Total controlled 9/11 (82) 61/71 (86) 27/30 (90) 97/112 (87) Severe
Total controlled 4/4 (100) 6/6 (100) 0/0 10/10 (100) Other
Total controlled 5/7 (71) 71/76 (93) 58/60 (97) 135/144 (94)
* Attainment of goal was defined as diastolic blood pressure (DBP) ~<90 mmHg or a drop of >110 mmHg in DBP. t Severity of hypertension was defined as DBP of 95 to t04 mmHg (mild), 105 to 115 mmHg (moderate), >115 mmHg (severe), and <95 mmHg (other). :1: Age was not reported for 7 patients.
the calculation. All lipid evaluations were conducted over the 6 weeks of study.
The mean changes in lipid profile for the newly diagnosed patients as compared with those for the total patient population (N = 186) are out- lined in Table III. Changes in total cholesterol and triglycerides were statistically significant in both the total population group (P = 0.001 and P = 0.001, respectively) and the subgroup of newly diagnosed patients (P
Table II. Attainment of goal* blood pressure in patients newly diagnosed for hypertension: Intention to treat by severity of hypertension at baseline# frequencies.
Age (yr)
<50 50 to 64 >64 Total N (%) N (%) N (%) N (%)
Total 16 100 84 100 28 100 128 100 Severity at baseline 12 75 72 86 22 79 106 83 Mild
Total controlled 4/7 57 35/45 78 7/10 70 46/62 74 Moderate
Total controlled 6/6 1 O0 25/27 93 11/13 85 42/46 91 Severe
Total controlled 2/2 100 3/3 100 0/0 0 5/5 100 Other
Total controlled 0/1 0 9/9 100 4/5 80 13/15 87
* Attainment of goal was defined as diastolic blood pressure (DBP) ~<90 mmHg or in DBP. 1 Severity of hypertension was defined as DBP of 95 to 104 mmHg (mild), 105 to 1 >115 mmHg (severe), and <95 mmHg (other).
a drop of/>10 mmHg
15 mmHg (moderate),
134

C. BARNESET AL.
Excellent (
Fair (3%)
(7%)
Figure 3. Patient acceptance of SR verapamil by the 507 study participants.
= 0.009 and P = 0.007, respectively). Changes in high-density lipoprotein (HDL) and low-density lipoprotein (LDL) were not statistically significant in either group.
Renal Function Study
A total of 142 patients participated in the renal function study. No changes were found in mean values for creatinine, blood urea nitrogen, or creatinine clearance between admission and week 6.
Diabetes Study
Seventy-seven patients were enrolled in the diabetes study. A mean decrease in glycosylated hemoglobin of 0.01% was observed between ad- mission and week 6. No patients reported difficulties with diabetic control.
Well-Being Study
A total of 96 patients entered the well-being study. As shown in Figure 5, scores on all i tems in the patient questionnaire improved between ad- mission and week 6, in most cases by one to two points on a scale of 0 to 10, with 10 indicating maximal well-being. An increase in scores was also
135

BP, LIPID, RENAL, GLYCEMIC, AND QOL EFFECTS OF SR VERAPAMIL
Excellent (56%)
Poor (3%)
tir (8%)
Good (33%)
Figure 4. Physician assessment of efficacy of SR verapamil in the 507 study participants.
observed in responses to the partner questionnaire. No differences were noted between the previously treated patients (N = 62) and the total population in terms of changes in quality of life at week 6.
Safety
A total of 179 side effects were r epor t edby 114 (22.5%) patients. All
Table III. Mean changes in lipid profile.
Total Patient Population (N = 189)
Newly Diagnosed Patients (N = 52)
Mean Change Mean Change Lipid (mmol/L) P Value (mmol/L) P Value
Total cholesterol - 0.20 0.001 - 0.26 0.009 Triglycerides - 0.21 0.001 - 0.32 0.007 High-density lipoprotein + 0.05 0.225 + 0.12 0.434 Low-density lipoprotein -0 .10 0.141 -0 .16 0.126
136

2o t D
P
atie
nt
, P
artn
er
09
1.5
1.0
0.5
Sle
epin
g E
nerg
y D
ays G
o B
y G
ettin
g Alo
ng
F
eelin
g Q
uick
ly
With
Oth
ers
R
elax
ed
Wel
l-Bei
ng M
easu
res
Fig
ure
5.
Cha
nges
in
wel
l-be
ing
mea
sure
s ov
er t
he s
tudy
per
iod.
Feel
ing
Che
erfu
l A
lert
ness
E
nerg
y Dur
ing
On
Wak
ing
Up
Dai
ly A
ctiv
ity

BP, LIPID, RENAL, GLYCEMIC, AND QOL EFFECTS OF SR VERAPAMIL
adverse events, whether or not related to SR verapamil, were included in the statistical analysis. The most common side effects were constipation (10.7%), edema (3.2%), dizziness (2.6%), asthenia (2.2%), nausea (1.4%), flushing (1.2%), and headache (1.2%). All other side effects were reported by fewer than 1% of the patients. Cardiac side effects were reported by 10 (2%) patients: 2 (0.4%) patients experienced bradycardia between 50 and 60 beats/min, 2 (0.4%) patients experienced tachycardia, 2 (0.4%) had car- diac palpitations, 3 (0.6%) had congestive heart failure, and 1 (0.2%) pa- tient was thought to have transitory cerebral ischemia.
The most common adverse events causing patients to withdraw from the study were constipation (1.8%), asthenia (1.2%), nausea (1.2%), edema (1%), dizziness (1%), and flushing (1%). Six (1.2%) patients were with- drawn from the study because of cardiac events: congestive heart failure in 3 (0.6%), cardiac palpitations in 1 (0.2%), and tachycardia in 2 (0.4%) patients (one after discontinuing beta-blockers).
Some adverse events, such as constipation, edema, and dizziness, were reported more frequently by patients older than age 64 (Table IV).
DISCUSSION
One of the principal objectives of multicenter open trials is to evaluate the effects of a drug under real-life conditions. In this context, our study is of particular interest because it was conducted in general practice using more than 500 patients with mild to moderate hypertension.
SR verapamil was found to be an effective and well-tolerated antihy- pertensive medication. Blood pressure was controlled in 85% of patients, closely paralleling results of other studies of SR verapamil in general practice. ~-s Patient satisfaction with treatment and physician assessment of t reatment efficacy reflect the results reported in the literature. ~-9 Ninety percent of patients and 89% of physicians rated treatment as either good or excellent.
In this study, monotherapy with SR verapamil produced a mean re-
Table IV. Incidence (%), by age, of the most common adverse events reported by 114 study patients.
Age
Event ~<64 yr >64 yr Total
Constipation 7.2 18.2 10.7 Edema 2.0 5.2 3.2 Dizziness 1.7 4.5 2.6 Asthenia 2.0 2.6 2.2 Nausea 1.2 1.9 1.4 Flushing 1.2 1.3 1.2 Headache 1.2 1.3 1.2
138

C. BARNES ET AL.
duction in blood pressure of 16 mmHg SBP and 12 mmHg DBP. Similar results were reported in another trial with SR verapamil, in which a mean reduction of 17 mmHg SBP and 12 mmHg DBP was seen during 8 weeks of therapy, s
We observed an early onset of efficacy, with the greatest decrease in blood pressure occurring between baseline and week 2 (14 mmHg SBP and 10 mmHg DBP). In a similar trial with nifedipine, the greatest mean decrease in blood pressure was likewise seen within the first 2 weeks of therapy. 9
SR verapamil was found to be as efficacious in elderly patients as in younger patients. No significant difference in blood pressure response was observed when patients were stratified by age.
Recent literature suggests that SR verapamil is lipid neutral1°-13; however, our results showed a statistically significant improvement in total cholesterol and triglyceride levels in both previously treated and newly diagnosed patients. In addition, a mild beneficial effect on LDL and HDL levels was noted, although this was not statistically significant. Thus SR verapamil was effective in improving lipid profiles even in patients whose lipid levels had not been compromised by previous antihypertensive treatment. Although this finding is of interest, our study reflects only short-term treatment. Further research is needed to confirm the long-term effect of SR verapamil on lipid profiles.
Although some investigators suggest that SR verapamil exerts a reno- protective effect independent of its effect on blood pressure in experimental models, 14 we found no change in renal function, as measured by creatinine clearance in patients considered at risk. Our study probably was not of long enough duration to detect a favorable effect.
As demonstrated in several studies, 1~J6 treatment with SR verapamil does not alter blood glucose levels. SR verapamil had no negative effects on the metabolic factors examined in our study, indicating that it may be a good choice for monotherapy in patients with concomitant diseases.
Patient quality of life was found to improve over the 6 weeks, with partner responses closely reflecting those of the patients. Although we anticipated that patients previously treated with other antihypertensive medications (particularly beta-blockers and diuretics) might show a greater improvement in quality of life than the total patient population, this effect was not observed. Our ability to assess changes in quality of life, however, was somewhat limited, because of limited study length and lack of a validated questionnaire. Future studies should address changes in patient well-being over a longer period of time.
The frequency of adverse events reported in this study (22.5%) is higher than that reported in the literature6-S; however, this percentage includes all events, whether related or not to SR verapamil, and all neg- ative comments noted on the case report forms. Also, because this study did
139

BP, LIPID, RENAL, GLYCEMIC, AND QOL EFFECTS OF SR VERAPAMIL
not incorporate a placebo phase for washout of previous antihypertensive medications, withdrawal symptoms were probably recorded as side effects for patients switched from other medications. Dropout rate because of side effects (7%) compares favorably with that in other, similar studies. 6-9 Frequency of cardiac adverse events was extremely low (2%).
The most common side effect was constipation, reported by 10.7% of patients. Severity of constipation appeared to be mild, however, and the withdrawal rate due to constipation was low (1.8%). Constipation fre- quency increased with age. This effect can be minimized by a diet rich in roughage, increased fluid intake, regular exercise, and taking SR vera- pamil with meals. In elderly patients, a starting dose of 120 mg might also reduce constipation frequency and severity.
In conclusion, results of this study indicate that SR verapamil is safe and effective in the treatment of hypertension. Monotherapy with SR ve- rapamil was found to be as efficacious in older patients (those over age 64) as in younger patients. In addition, SR verapamil had a positive effect on lipid levels and patient well-being, with no deleterious effects on renal function or diabetic control.
Acknowledgment
This study was supported by a grant from Searle Canada Inc., Oakville, Ontario, Canada.
References:
1. 1988 Joint National Committee. The 1988 report of the Joint National Committee on detection, evaluation and treatment of high blood pressure (JNC IV). Arch Intern Med 1988; 148:1023-1038.
2. Halperin AK, Cubeddu LX. The role of calcium channel blockers in the treatment of hypertension. Am Heart J 1986; 3:363-382.
3. Opie LH. Calcium channel antagonists: Use and comparative efficacy in hypertension and supraventricular arrhythmias. In: Opie LH, ed. Clinical use of calcium channel antagonist drugs. 2nd ed. Boston: Kluwer Academic Publishers, 1989:131-192.
4. Halperin AK, Gross KM, Rogers JF, Cubeddu LX. Verapamil and propranolol in essen- tial hypertension. Clin Pharmacol Ther 1984; 36:750-758.
5. Naylor WG. Calcium antagonists and the treatment of hypertension. In: Naylor WG, ed. Calcium antagonists. London: Academic Press, 1988:209-233.
6. EVEREST'H (Evaluation of Verapamil for Efficacy, Safety and Tolerability in the Man- agement of Hypertension). Multicentre trial of the antihypertensive efficacy and safety of Isoptin ® SR. Acta Med Int 1990; 2:3-7.
7. Speders S, Sosna J, Schumacher A, Pfennigsdorf G. Efficacy and tolerability of Isoptin SR in essential hypertension--Results of a phase IV study under practice conditions. Hoch- druck 1988; 8:3-14.
140

c. BARNES ET AL.
8. Hamel D. An open-label multicentre study of Isoptin SR in the therapeutic management of patients with mild to moderate hypertension. Data on file, Searle Canada, Oakville, Ontario, Canada, 1992.
9. The Canadian Adalat Profile Assessment Group. Effectiveness of nifedipine 20 mg pro- longed action tablet (Adalat PA20) in the management of hypertension in general prac- tice. Drug Invest 1989; 1:24-28.
10. Rouleau JL, Parmley WW, Stevens J, et al. Verapamil suppresses atherosclerosis in cholesterol fed rabbits. J Am Coll Cardiol 1983; 1:1453-1460.
11. Lewis GRJ. Long term results with verapamil in essential hypertension and its influence on serum lipids. Am J Cardiol 1986; 57(Suppl):35D-38D.
12. Lewis GRJ, Steward DJ, Lewis BM, et al. The antihypertensive effect of oral verapamil-- Acute and long term administration and its effects on the high-density lipoprotein values in plasma. In: Zanchetti A, Krikler DM. Calcium antagonism in cardiovascular therapy: Experience with verapamil. Amsterdam: Excerpta Medica, 1981:270-277.
13. Stadler P, Leonardi L, Riesen W, et al. Cardiovascular effects of verapamil in essential hypertension. Clin Pharmacol Ther 1987; 42:485-492.
14. Harris DCH, Hammond WS, Burke TJ, Schrier R. Verapamil protects against progres- sion of experimental chronic renal failure. Kidney Int 1987; 31:41-46.
15. Houston MC. Treatment of hypertension in diabetes mellitus. Am Heart J 1989; 118: 819-829.
16. Chellingsworth MC, Kendall MJ, Wright AD, et al. The effects of verapamil, diltiazem, nifedipine and propranolol on metabolic control in hypertensives with non-insulin de- pendent diabetes mellitus. J Human Hypertens 1989; 3:35-39.
141