effects of immediate postoperative physical therapy on
TRANSCRIPT
Central Annals of Sports Medicine and Research
Cite this article: Sun G, Gundle K, Arnold K, Contag A, Crawford D (2020) Effects of Immediate Postoperative Physical Therapy on Negative Events following Ambulatory Orthopaedic Surgery. Ann Sports Med Res 7(3): 1154.
*Corresponding authorDennis C. Crawford, Department of Orthopaedics and Rehabilitation, Oregon Health and Science University, 3181 SW Sam Jackson Park Road, mail code OP31, Portland, OR 97239, USA, Tel: 503-494-5327; Fax: 503-494-5050; Email: [email protected]
Submitted: 24 June 2020
Accepted: 08 July 2020
Published: 10 July 2020
ISSN: 2379-0571
Copyright© 2020 Sun G, et al.
OPEN ACCESS
Keywords•Sports medicine; Satisfaction; Survey; Phone
Abstract
Study Design: Cohort.
Background: Postoperative physical therapy on the day of surgery (SDPT) for inpatient orthopaedic patients is known to improve function and reduce hospital length of stay. However, as far as we know, this has not been examined in the outpatient surgical setting.
Objectives: We examined whether negative event rates (triage phone calls, ER (emergency room) visits) and Press Ganey satisfaction scores were different in patients receiving SDPT compared to those that did not.
Methods: One surgeon performed 590 ambulatory shoulder or knee procedures. Patients who had significant postoperative activity restrictions and underwent surgery on Thursdays received SDPT; those undergoing surgery on Fridays did not. To determine if there was a hidden day-of-week bias, two control groups without postoperative activity restrictions also underwent surgery on Thursday or Friday.
Results: Negative event rates did not differ based on SDPT in those with postoperative activity restrictions (0.86 vs. 0.69, respectively, p=0.29) or in those with no activity restrictions (0.40 vs 0.26, respectively, p=0.12). Press Ganey scores similarly did not differ significantly based on SDPT, with mean scores of 9.2 and 9.0, of 10, in those with postoperative activity restrictions (p=0.53).
Conclusion: SDPT did not affect negative event rates or Press Ganey scores in patients with or without postoperative activity restrictions. This may reflect a ceiling effect, given the high baseline level of satisfaction associated with these procedures. A larger cohort and different metrics could be additional elements to identify the impact of this complementary educational method in the post-operative ambulatory setting.
Level of Evidence: III.
Research Article
Effects of Immediate Postoperative Physical Therapy on Negative Events following Ambulatory Orthopaedic SurgeryGrant Sun, Kenneth Gundle, Kaytee Arnold, Alec Contag, and Dennis Crawford*
Department of Orthopaedics and Rehabilitation, Oregon Health and Science University, USA
ABBREVIATIONSSDPT: Same Day Physical Therapy; ER: Emergency Room;
CPT: Current Procedural Terminology; N: Number; SD: Standard Deviation
INTRODUCTIONPhysical therapy is a crucial component of postoperative
rehabilitation following orthopaedic surgery. However, to our knowledge, no literature exists regarding physical therapy on the day of surgery in the ambulatory surgical setting. By contrast, there seems to be a wealth of supportive literature in the inpatient setting. For total hip and knee arthroplasty performed in the in-hospital setting, favorable outcomes and effects are reported. Chen et al. found significantly shorter length of hospital stays in patients with same day physical therapy (3.7 versus 2.8 days, p=0.02) without an increase in pain scores [1]. Larsen et al. also found significantly shorter hospital stays (8 to 5 days, p<0.001) and by extension, reductions in overall cost for patients
with same day physical therapy [2]. Labraca et al. found shorter hospital stays (2.09 days p<0.001) as well as reduced pain (2.36 on 0-10 scale p<0.027), greater range of motion (16 degree increase in flexion p<0.012), improved strength, and higher gait and balance scores, as a result of starting rehabilitation within 24 hours of total knee arthroplasty [3]. We have found no reports of accelerated or same day physical therapy (SDPT) in ambulatory orthopaedic sports medicine patients. To evaluate SDPT in the ambulatory setting, a pilot program was established to assess patients who had significant postoperative activity restrictions after their orthopaedic surgery. As an extension of this program, data was collected to capture the effect of this intervention on “negative” events, specifically postoperative triage phone calls and emergency room (ER) visits.
Postoperative triage phone calls and ER visits are costly burdens for orthopaedic practices [4,5]. Our first aim was to determine if SDPT affects the number of negative events in an orthopaedic sports medicine practice. We hypothesized that

Central
Sun G, et al. (2020)
Ann Sports Med Res 7(3): 1154 (2020) 2/4
there would be a decrease in negative events with the addition of SDPT.
Our second aim was to determine if SDPT affected patient satisfaction. Patient satisfaction scores are an increasingly ubiquitous metric for self-assessment and have even been used for care provider compensation formulas [6]. Etier et al., evaluated factors that affected Press Ganey patient satisfaction scores in an orthopaedic spine clinic and found that the most important factor was the patients’ feelings of adequate time spent with the provider [7]. SDPT increases the time each patient spends with a medical provider, and anecdotally is well liked by our patients. The hypothesis of our second aim was that there would be an increase in Press Ganey scores in those who received SDPT.
MATERIALS AND METHODSOur institution’s IRB (the OHSU Institutional Review Board)
granted approval for this retrospective cohort study. Patients were included in the study if they were at least 18 years of age and were undergoing same day ambulatory shoulder or knee surgery on a Thursday or Friday. Exclusion criteria were patients enrolled in ongoing premarket FDA regulated trials. All patients enrolled in the study underwent surgery by a single Sport Medicine and Orthopedic Trauma fellowship-trained orthopaedic surgeon between October, 2015 and August, 2017.
Demographic data collected were age, gender, and insurance type (private or government sponsored). Data for ER visits and phone calls was collected through our institutions electronic medical record. Between the time of operation and first postoperative clinic visit, we collected data on the number of ER visits and postoperative phone calls, collectively defined as negative events. Surgery type was collected by principal CPT (current procedural terminology) code and categorized into those with significant postoperative activity restrictions and those without. After subject numbers were known, a pre-hoc power analysis was performed based on a difference of proportion for a binomial distribution with an alpha of 0.05. Our known difference in group size (271 vs 144 for primary outcome), and with a goal power of 0.8, would identify a modest effect size (h=0.3).
Press Ganey scores were collected from our institution’s Patient Experience Office. These were mailed to our patients from the office, typically a few weeks after their surgery. They were then filled out by the patient and mailed back in. Some questions are specific to clinical care, however, the score we collected and kept simply asked how satisfied the patient was with the overall health care experience surrounding the surgery.
Patients with postoperative activity restrictions
Physical therapists were available on Thursdays only to provide SDPT to postoperative patients. Thus, physical therapists visited patients just prior to discharge on Thursdays only and provided SDPT; they reviewed postoperative instructions, and demonstrated exercises to those with postoperative activity restrictions. Activity restrictions were defined as any range of motion or weight bearing restrictions. Conversely, patients who had their operations on Fridays with postoperative activity restrictions did not receive SDPT; discharge nurses simply
reviewed activity restrictions and orders with the patient, as historically routine.
Patients with no postoperative activity restrictions
To determine if there was a hidden day-of-week bias between those patients undergoing surgery on Thursdays compared to Fridays, two control groups were also included in the study that did not have postoperative activity restrictions. One control group underwent surgery on Thursday and one control group underwent surgery on Friday.
Finally, data regarding Press Ganey scores was collected through our Patient Experience Office. We collected a single data point from this questionnaire that asked, on a 0-10 scale, how satisfied the patient was with their surgery experience at our hospital (0 worst, 10 best). Scores were averaged and compared for significance using both a Wilcoxon rank sum test and Pearson’s chi-squared test. Surgeries with Press Ganey scores that had negative events were also compared against those without these scores, to determine if there was a significant difference by Fisher’s Exact test.
Statistical analysis
Gender and insurance type between groups were compared using Pearson’s chi-squared test. Group differences in age were determined using analysis of variance. Differences were considered statistically significant at p<0.05.
RESULTSDuring the study period, 590 surgeries were performed on
483 patients. Demographic variables for each group are shown in Table 1. The four groups did not differ significantly in gender (p=0.64), insurance type (p=0.46) or age (p=0.96). Surgery
Table 1: Demographic variables based on patients who underwent surgery on Thursday (received SDPT) and patients who underwent surgery on Friday (did not receive SDPT).
Thursday - SDPT Friday - No SDPTPostoperative activity restrictions N=271 N=144
Age, years; mean (SD) 39 (14) 40 (13)
% Female (N) 44% (119) 47% (67)
Private insurance, % (N) 71% (193) 75% (108)Government sponsored insurance, % (N) 21% (56) 19% (28)
No postoperative activity restrictions N=87 N=88
Age, years; mean (SD) 40 (14) 39 (14)
Female, % (N) 39% (33) 40% (34)
Private insurance, % (N) 71% (60) 83% (71) Government sponsored insurance, % (N) 23% (19) 14% (12)
Abbreviations: SDPT: Same Day Physical Therapy; N: Number; SD: Standard DeviationBy Pearson’s Chi-squared test, there was no significant difference between groups by gender or type of insurance (private versus government sponsored) (p=0.64, p=0.46 respectively). There was also no difference between the four groups by age (ANOVA p=0.96).
Central
Sun G, et al. (2020)
Ann Sports Med Res 7(3): 1154 (2020) 3/4
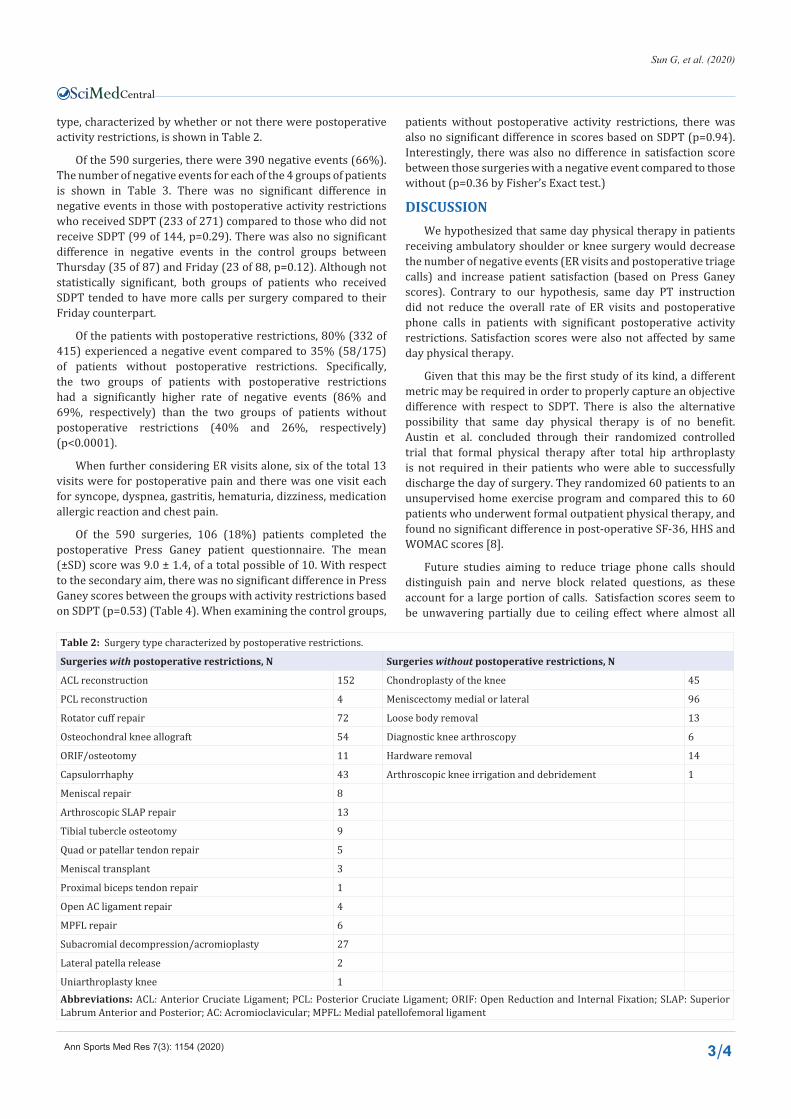
type, characterized by whether or not there were postoperative activity restrictions, is shown in Table 2.
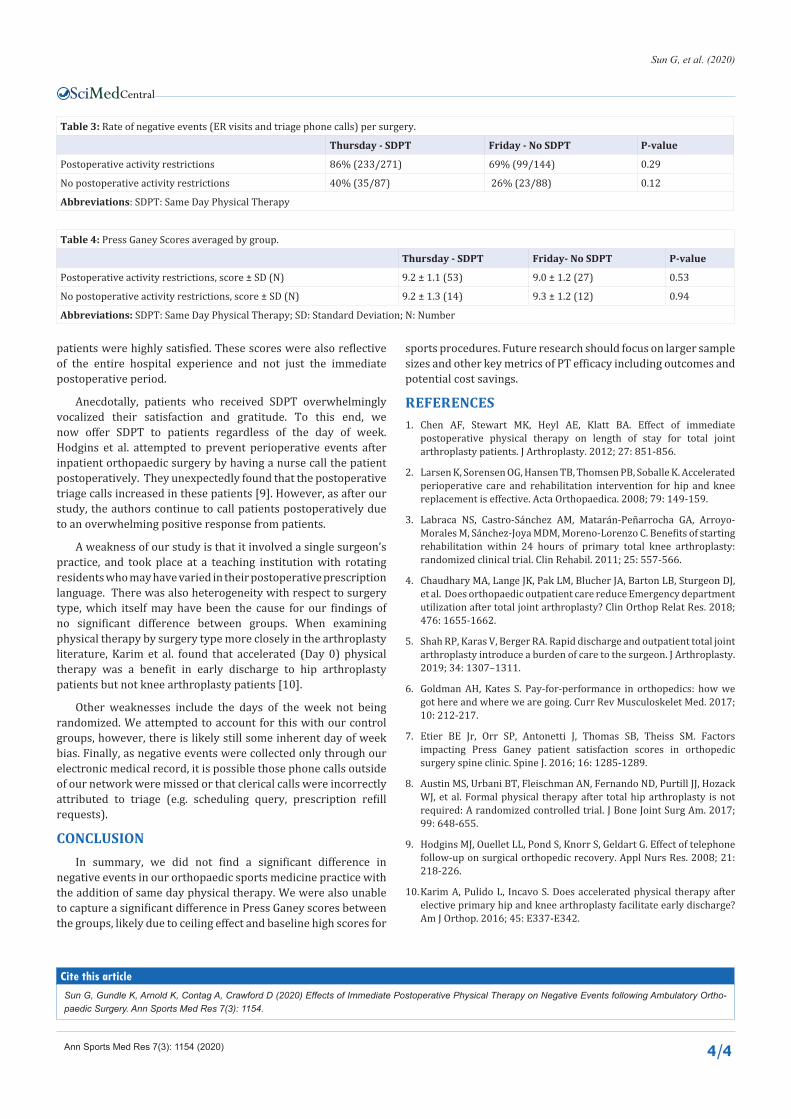
Of the 590 surgeries, there were 390 negative events (66%). The number of negative events for each of the 4 groups of patients is shown in Table 3. There was no significant difference in negative events in those with postoperative activity restrictions who received SDPT (233 of 271) compared to those who did not receive SDPT (99 of 144, p=0.29). There was also no significant difference in negative events in the control groups between Thursday (35 of 87) and Friday (23 of 88, p=0.12). Although not statistically significant, both groups of patients who received SDPT tended to have more calls per surgery compared to their Friday counterpart.
Of the patients with postoperative restrictions, 80% (332 of 415) experienced a negative event compared to 35% (58/175) of patients without postoperative restrictions. Specifically, the two groups of patients with postoperative restrictions had a significantly higher rate of negative events (86% and 69%, respectively) than the two groups of patients without postoperative restrictions (40% and 26%, respectively) (p<0.0001).
When further considering ER visits alone, six of the total 13 visits were for postoperative pain and there was one visit each for syncope, dyspnea, gastritis, hematuria, dizziness, medication allergic reaction and chest pain.
Of the 590 surgeries, 106 (18%) patients completed the postoperative Press Ganey patient questionnaire. The mean (±SD) score was 9.0 ± 1.4, of a total possible of 10. With respect to the secondary aim, there was no significant difference in Press Ganey scores between the groups with activity restrictions based on SDPT (p=0.53) (Table 4). When examining the control groups,
patients without postoperative activity restrictions, there was also no significant difference in scores based on SDPT (p=0.94). Interestingly, there was also no difference in satisfaction score between those surgeries with a negative event compared to those without (p=0.36 by Fisher’s Exact test.)
DISCUSSIONWe hypothesized that same day physical therapy in patients
receiving ambulatory shoulder or knee surgery would decrease the number of negative events (ER visits and postoperative triage calls) and increase patient satisfaction (based on Press Ganey scores). Contrary to our hypothesis, same day PT instruction did not reduce the overall rate of ER visits and postoperative phone calls in patients with significant postoperative activity restrictions. Satisfaction scores were also not affected by same day physical therapy.
Given that this may be the first study of its kind, a different metric may be required in order to properly capture an objective difference with respect to SDPT. There is also the alternative possibility that same day physical therapy is of no benefit. Austin et al. concluded through their randomized controlled trial that formal physical therapy after total hip arthroplasty is not required in their patients who were able to successfully discharge the day of surgery. They randomized 60 patients to an unsupervised home exercise program and compared this to 60 patients who underwent formal outpatient physical therapy, and found no significant difference in post-operative SF-36, HHS and WOMAC scores [8].
Future studies aiming to reduce triage phone calls should distinguish pain and nerve block related questions, as these account for a large portion of calls. Satisfaction scores seem to be unwavering partially due to ceiling effect where almost all
Table 2: Surgery type characterized by postoperative restrictions.
Surgeries with postoperative restrictions, N Surgeries without postoperative restrictions, N
ACL reconstruction 152 Chondroplasty of the knee 45
PCL reconstruction 4 Meniscectomy medial or lateral 96
Rotator cuff repair 72 Loose body removal 13
Osteochondral knee allograft 54 Diagnostic knee arthroscopy 6
ORIF/osteotomy 11 Hardware removal 14
Capsulorrhaphy 43 Arthroscopic knee irrigation and debridement 1
Meniscal repair 8
Arthroscopic SLAP repair 13
Tibial tubercle osteotomy 9
Quad or patellar tendon repair 5
Meniscal transplant 3
Proximal biceps tendon repair 1
Open AC ligament repair 4
MPFL repair 6
Subacromial decompression/acromioplasty 27
Lateral patella release 2
Uniarthroplasty knee 1Abbreviations: ACL: Anterior Cruciate Ligament; PCL: Posterior Cruciate Ligament; ORIF: Open Reduction and Internal Fixation; SLAP: Superior Labrum Anterior and Posterior; AC: Acromioclavicular; MPFL: Medial patellofemoral ligament
Central
Sun G, et al. (2020)
Ann Sports Med Res 7(3): 1154 (2020) 4/4
patients were highly satisfied. These scores were also reflective of the entire hospital experience and not just the immediate postoperative period.
Anecdotally, patients who received SDPT overwhelmingly vocalized their satisfaction and gratitude. To this end, we now offer SDPT to patients regardless of the day of week. Hodgins et al. attempted to prevent perioperative events after inpatient orthopaedic surgery by having a nurse call the patient postoperatively. They unexpectedly found that the postoperative triage calls increased in these patients [9]. However, as after our study, the authors continue to call patients postoperatively due to an overwhelming positive response from patients.
A weakness of our study is that it involved a single surgeon’s practice, and took place at a teaching institution with rotating residents who may have varied in their postoperative prescription language. There was also heterogeneity with respect to surgery type, which itself may have been the cause for our findings of no significant difference between groups. When examining physical therapy by surgery type more closely in the arthroplasty literature, Karim et al. found that accelerated (Day 0) physical therapy was a benefit in early discharge to hip arthroplasty patients but not knee arthroplasty patients [10].
Other weaknesses include the days of the week not being randomized. We attempted to account for this with our control groups, however, there is likely still some inherent day of week bias. Finally, as negative events were collected only through our electronic medical record, it is possible those phone calls outside of our network were missed or that clerical calls were incorrectly attributed to triage (e.g. scheduling query, prescription refill requests).
CONCLUSIONIn summary, we did not find a significant difference in
negative events in our orthopaedic sports medicine practice with the addition of same day physical therapy. We were also unable to capture a significant difference in Press Ganey scores between the groups, likely due to ceiling effect and baseline high scores for
Table 3: Rate of negative events (ER visits and triage phone calls) per surgery.
Thursday - SDPT Friday - No SDPT P-value
Postoperative activity restrictions 86% (233/271) 69% (99/144) 0.29
No postoperative activity restrictions 40% (35/87) 26% (23/88) 0.12
Abbreviations: SDPT: Same Day Physical Therapy
Table 4: Press Ganey Scores averaged by group.
Thursday - SDPT Friday- No SDPT P-value
Postoperative activity restrictions, score ± SD (N) 9.2 ± 1.1 (53) 9.0 ± 1.2 (27) 0.53
No postoperative activity restrictions, score ± SD (N) 9.2 ± 1.3 (14) 9.3 ± 1.2 (12) 0.94
Abbreviations: SDPT: Same Day Physical Therapy; SD: Standard Deviation; N: Number
sports procedures. Future research should focus on larger sample sizes and other key metrics of PT efficacy including outcomes and potential cost savings.
REFERENCES1. Chen AF, Stewart MK, Heyl AE, Klatt BA. Effect of immediate
postoperative physical therapy on length of stay for total joint arthroplasty patients. J Arthroplasty. 2012; 27: 851-856.
2. Larsen K, Sorensen OG, Hansen TB, Thomsen PB, Soballe K. Accelerated perioperative care and rehabilitation intervention for hip and knee replacement is effective. Acta Orthopaedica. 2008; 79: 149-159.
3. Labraca NS, Castro-Sánchez AM, Matarán-Peñarrocha GA, Arroyo-Morales M, Sánchez-Joya MDM, Moreno-Lorenzo C. Benefits of starting rehabilitation within 24 hours of primary total knee arthroplasty: randomized clinical trial. Clin Rehabil. 2011; 25: 557-566.
4. Chaudhary MA, Lange JK, Pak LM, Blucher JA, Barton LB, Sturgeon DJ, et al. Does orthopaedic outpatient care reduce Emergency department utilization after total joint arthroplasty? Clin Orthop Relat Res. 2018; 476: 1655-1662.
5. Shah RP, Karas V, Berger RA. Rapid discharge and outpatient total joint arthroplasty introduce a burden of care to the surgeon. J Arthroplasty. 2019; 34: 1307–1311.
6. Goldman AH, Kates S. Pay-for-performance in orthopedics: how we got here and where we are going. Curr Rev Musculoskelet Med. 2017; 10: 212-217.
7. Etier BE Jr, Orr SP, Antonetti J, Thomas SB, Theiss SM. Factors impacting Press Ganey patient satisfaction scores in orthopedic surgery spine clinic. Spine J. 2016; 16: 1285-1289.
8. Austin MS, Urbani BT, Fleischman AN, Fernando ND, Purtill JJ, Hozack WJ, et al. Formal physical therapy after total hip arthroplasty is not required: A randomized controlled trial. J Bone Joint Surg Am. 2017; 99: 648-655.
9. Hodgins MJ, Ouellet LL, Pond S, Knorr S, Geldart G. Effect of telephone follow-up on surgical orthopedic recovery. Appl Nurs Res. 2008; 21: 218-226.
10. Karim A, Pulido L, Incavo S. Does accelerated physical therapy after elective primary hip and knee arthroplasty facilitate early discharge? Am J Orthop. 2016; 45: E337-E342.
Sun G, Gundle K, Arnold K, Contag A, Crawford D (2020) Effects of Immediate Postoperative Physical Therapy on Negative Events following Ambulatory Ortho-paedic Surgery. Ann Sports Med Res 7(3): 1154.
Cite this article