effectiveness of three types of sterilization on the contents of sharps
TRANSCRIPT

Intection Control
Effectiveness of three types of sterilization on the contentsof sharps containers
Margie A. Sheldrake*/Crystal Dashawn Majors**/Darla J. Gaities***/Charlcs John Palenik****
The purpose ofthis study was to test the effect of treatment in a gravity steam autoclave,high-vacuum steam autoclave, or an unsatitrated chemical vapor sterilizer on endosporespresent on strips or placed inside of dental anesthetic cartridges held within sharps containers.Strips with 1.7 X /O Bacillus stearothermophilus endospores were tised: the cartridges weresoiled with an equal number of spores or spores mixed with blood, ¡f sterilization was notaccomplished after the initial period, additional exposure time was added. Neither thepresence of blood or anesthetic solution nor the position ofthe container affected the efficiencyof sterilization. Soiled cartridges were much more difficult than strips to sterilize. Intactcartridges could not be sterilized by tM'o runs in a gravit}- steam autoclave or an unsaturatedchemical vapor .sterilizer or one run in a high-vacuum steam autoclave. Sterilization occurredafter iiro runs in the gravity steam atitoclave and unsaturated chemical vapor .sterilizer onlywhen one end of the cartridge was removed prior to processing. Results indicated thatunopened spore-soiled cartridges are not readily sterilized by commonplace office sterilizers,even after extended exposure. (Quintessence Int 1995.26:77i-778.)
Introduction
Many people mistakenly consider the tetms hospitalwaste, medical waste, and infectious waste synony-mous. Hospital waste, like dental office waste orhousehold waste, refers to the total discarded solidwaste generated by all sources within a given location.In a hospital, this would include biologic wastematerials, such as medical, food services, or animal
* Research Associate. Infeelion Control Research and Services,Indiana University. Sctiool of Dentistry. Indianapolis. Indiana.
** Summer Minority Researeti Student, Department of Oral Biology,Indiana Uruversjty. Schuoi ofDentistry, Indianapoiis. Indiana.
*** Research Assistant, Infection Control Räsearch and Services.Indiana LJniversity. School ofDentistry, Indianapolis. Indiana.
**"- Professor of Oral Microbiology. Department of Oral Biology.Indiana University, School of Dentistry. Indianapolis, Indiana.
Repnnt requests: Dr Charles John Palenilt, Professor of Oral Micro-biology, Departmeni of (Irai Biology. Indiana University School ofDentistry. 1121 West Michigan Street. Indianapolis, Indiana 463tl2.
This researcii was supported in part by tiie Nationai Institutes of Heaith,National Center for Research Resources. Minority Higiî School Re-search Apprentice Program, grant No. SOJ RRO 3487-05.
research facility waste, in addition to nonbiologicrefuse, such as clerical paper and plastic items.Medical waste includes materials generated duringpatient diagnosis, treatment, or immunization. Infec-tious waste is a small subset (about 3%) of medicalwaste that has been shown through epidemiologicreview to be capable of transmitting infectious diseas-es. Special handling, storage, and disposal proceduresare required for infectious waste, but not for the vastmajority of medical waste. Infectious waste of primeconcern to dentai offices and clinics includes bloodand blood products, saliva, oral tissues, such as teeth,and used sharps.'-
Sharps are items capable of penetrating intact skin.Dental examples include injection needles, scalpelblades, suture needles, burs, many clitiical instruments,and broken glass. If soiled with bodily fluids and/ortissues, such iletns have the potential to transtnitpathogenic organisms, such as the hepatitis B and Cviruses and human immunodeficiency vims type 1. "*Proper handling of sharps is essential because univer-sal precaution methods, such as the wearing of gloves,will not totally prevent exposure to sharps ("needle-stick accidents" )- "
Quintessence International Volume 26, Number 11/1995 771

Infection Control
In the United States. Occupational Safety andHealth Administration regulations. Centers for Dis-ease Control and Prevention guidelines and AmericanDental Association recommendations indicate thatsharps are to be placed into closable, labeled andcolor-coded, leakproof, puncture-resistant containers(sharps boxes) as soon as possible after generation.''"''The World Health Organization and the FinnishNational Research and Development Centre for Wel-fare and Health have issued strong statements indica-ting the need for prompt isolation of sharps intoimpervious containers.'"'' Sharps boxes should bereadily available in all treatment and instrumentrecycling areas. The overall goal of these efforts is toestablish a system by which sharps can be safelyhandled, stored, treated, and then sent on for finaldisposition.
In some areas of Ihe United States, a waste haulerapproved hy the Environmental Protection Agencymust be contracted for transport, off-site treatment,and disposal of sharps. However, many locations allowfor in-house treatment and then disposal throughregular waste-management schemes. Dentists shouldregularly check on their local regulations concerningmedical waste disposal, including infectious waste.
Waste generators have several choices for in-housetreatment and disposal of filled sharps containers.Incineration not only sterilizes the contents of thecontainers, but also reduces the volume by at least80%.' This process usually renders needles inoper-able. Although incineration is now highly regulated,many communities are reluctant to maintain or ap-prove such burning units. An alternative is moist heatsterilization.'-'^ Both steam autoclaves and unsaturatedchemical vapor sterilizers are commonly found inprivate dental offices. Autoclaving does not reduce thevolume of solids entering the waste stream, nor doesit significantly affect the appearance (or generalusability) of sharps. However, it does not seriouslychallenge air quality and can be easily accomplishedwithin most health care facilities.
OnJy a limited amount of information has beenpublished to help practitioners, especially those inprivate practice situations, to select the most efficientsterilization procedures. The effectiveness of steamautociaving and unsaturated chemical vapor sterili-zation on spore-soiled dental anesthetic needles placedwithin filled sharps containers has been investigated.""''It was reponed that spore-soiled needles are moredifficult to sterilize than commercial spore strips, thatneedle capping or the presence of blood does not affectsterilization efficiency, and that most containers pro-
cessed in an upward position cannot routinely besterilized in a single sterilizer cycle. It was determinedthat quart-sized or smaller containers can be effectivelytreated in one cycle if processed on their sides. Similarstudies have been conducted with spore-soiled tuber-culin syringes (with needles) placed inside of sharpscontainers.™-' The spores in the syringes proved tobe more difficult to kill than those in dental anestheticneedles contaminated in the same manner. The in-creased resistance is thought to be related to thepresence of "mini-vacuums" within the syringes. Tosoil the syringes, spore suspension materiais weredrawn into their lumens by upward movement oftheplungers. Penetrance of steam or chemical vapor couldbe retarded because of the presence of a resistantinternal negative pressure.
A similar situation could exist within dental anes-thetic cartridges. It is possible that body fiuids,including blood, could be aspirated into the cartridgeduring normal use. Soiled cartridges could be thenconsidered potential sharps—items that transform intotrue sharps if broken. Because of their physicalmakeup, cartridges could resist the inward movementof killing steam or chemical vapor.
Therefore, the purpose of this study was to evaluatethe killing effect a steam autoclave (gravity andhigh-vacuum types) or an unsaturated chettiical vaporsterilizer had on bacterial endospores present oncommercial spore strips or deposited within standarddental anesthetic cartridges placed within sharpscontainers.
Method and materials
One type of sharps container ( Sharps-A-Gator, Model4800, Devon Industries) was used. It had a stated 1-qtcapacity. Its three-quarters-filled volume was 550 niL.Previous investigations have indicated that the 1-qt sizeis used by 60% of surveyed offices and produces sterili-zation results representative of all but extremely smallor large containers.''"-'
The microbial challenge used to monitor sterilizereffectiveness was the Baciilus stearothennophihis bac-terial cndospore (SPS Medical). Two forms wereemployed—commercial spore strips (1.7 x 10 sporesper strip) and spore suspensions (diluted to a finalconcentration of 2.0 x 10' spores per 0.2 mL).
The gravity steam autoclave (SA) used was theValidator 10 (Pelton & Crane), a unit used by manyprivate dental and medical offices. The operatingconditions were 129 kPa (1 psi - 6.88 kPa) at 121''C
772 Quintessence International Volume 26, Number 11/1995

Infection Control
for 30 minutes. In some experiments, additional cyclesof 30 minutes were added. No poststerilization dryingcycles were run. Only distilled water was used togenerate steam.
Also used was a large-volume (24 x 36 ¡< 60 inch)high-vacuum steam autoclave (HVA) (Vacamatic Mo-del 3053, AMSCO) commonly found in centralsterilization departments in hospitals or larger clinics.Its operating conditions were 214 kPa at \3\°C for 10minutes with prevacuum and postvacuum cycles of 7minutes each.
An unsaturated chemical vapor sterilizer (UCV)(Harvey Chemiclave model 8000, MDT Biologies)was also used. Operating conditions were 172 kPa at134°C for 20 minutes. The mandatory 10 minutepoststerilization venting cycle was run. In someexperiments, additional runs of 20 minutes wereapplied.
Two phases of experimentation were performed.Experiments included the killing of bacterial endo-spores present on spore strips or deposited withindental anesthetic cartridges (Lidocaine, Novoco! Phar-maceutical), which initially contained 1.8 mL ofsolution. Some cartridges were soiled with spores,while others were contaminated with spores and wholesheep's blood (Colorado Serum). Strips and cartridgeswere processed through the gravity steam and high-vacuum autoclave and the unsaturated chemical vaporsterilizer. All spore challenges were placed withinopen-vent, three-quarters-filled sharps containers.Data were collected only on a qualitative basis—either"kill/no endospore growth" or "no kill/endosporegrowth. '
Phase ¡
Three spore strips were placed inside of three-quarters-filled sharps containers. The containers werefilled with a representative mix of sharps wastematerials, including needles, plastic needle sheaths,suture needles, plastic needle caps, plunger mecha-nisms, and scalpel blades. Equal amounts ( 175 g) offilling material were added so that each container wasthree-quarters full. A slow pouring method was used.No attempt to compact the filling material was made.Three spore strips were added during filling, one onthe bottom, one in the middle, and one on top ofthefull load.
Three containers were placed inside of each sterili-zer in a straight row, front to back. Containers wereput in either an upward or on-side position. Fachcombination was evaluated with the use of 24 contai-
ners. A single spore strip was placed on the outside ofone ofthe containers during each sterilization cycle.These strips served as treated controls. Fvery 25thspore strip was cultured without processing as anuntreated control.
After completion of the sterilization cycle, sporestrips were aseptically removed and placed individ-ually into culture tubes of tr>'pticase soy broth sup-plemented with glucose (TSB-G, Difco Laboratories).Aerobic incubation was at 56°C for 7 days. Resultswere recorded only as "growth" or "no growth."
Phase 2
A single microbially soiled anesthetic cartridge wasplaced during filling into the center of a container's fillload. Cartridges were chosen as test items because they/¡) are common forms of clinical waste; (2) canbecome soiled internally with a patient's bodily fluids,including blood; (3) are often soiled on the exteriorwith fluids from the patient; (4) often are disposed ofby placement in sharps containers; and (5) can be con-sidered potential sharps—contaminated sharps capa-ble of penetration if broken. Cartridges were usedempty and half filled with anesthetic solution. A1.0 mL. tuberculin syringe equipped with a 25-gaugeneedle (Precision Glide, Becton Dickinson) was usedto place 0.2 mL of spore solution into the cartridges.To half of the cartridges, an equal volume of sheep'sblood was also injected.
Containers were sterilized either in an upward or anon-side position with their vents opened. Each combi-nation was initially tested 24 times. Containers wereprocessed in groups of three—one in the back, one inthe middle, and one in front. A single treated controlstrip was placed on one container per cycle. Fvery25th strip and soiled cartridge served as an untreatedcontrol.
After processing, the cartridges were removed andallowed to cool for 15 minutes. Then, air was injectedinto the cartridges with a 1.0 mL tuberculin syringeuntil the rubber stopper (plunger end) moved towardthe end of and then out ofthe cartridge. The stopperand cartridge were placed together into a tube con-taining 10 mL of TSB-G, The tubes containing thespore strips or the anesthetic cartridges and stopperswere incubated in the same manner as described forspore strips in phase 1.
If sterilization of all 24 cartridges in a given testgroup did not occur after one cycle (30 minutes forGSA and 20 minutes for UCV), additional cycle-
Quintessenoe international Voiume 26, Number 11/1995 773
Infection Control
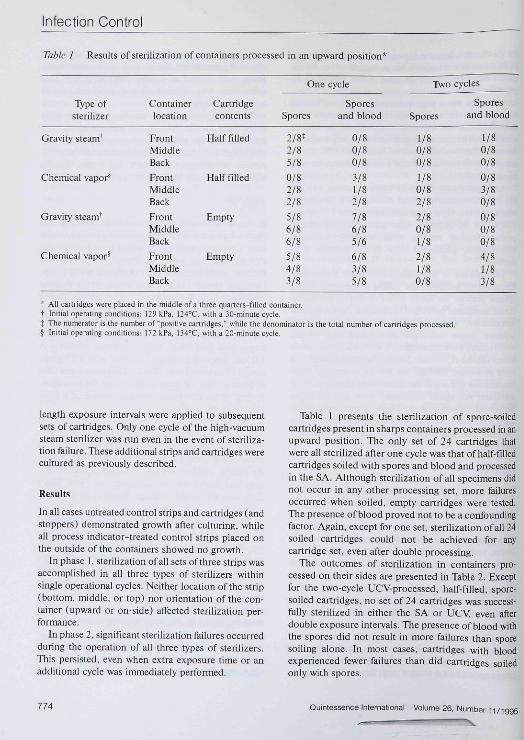
Table 1 Results of sterilization of containers processed in an upward position*
Type ofsterilizer
Gravity steam^
Chemical vapor*
Gravity steam^
Chemical vapoH
Containerlocation
FrontMiddleBack
FrontMiddleBack
FrontMiddleBack
FrontMiddleBack
Cartridgecontents
Half filled
Half filled
Empty
Empty
One cycle
Spores
2/8*2/85/8
0/82/82/8
5/86/86/8
S/84/83/8
Sporesand blood
0/80/80/8
3/81/82/8
7/86/85/6
6/83/85/8
Two cycles
Spores
1/80/80/8
1/80/82/8
2/80/81/8
2/81/80/8
Sporesand blood
1/80/80/8
0/83/80/8
0/80/80/8
4/81/83/8
* All cartridges were placed in the middle of a three-qtiarters-filled container.t Initial operating conditions: 129 kPa. I24''C. with a 30-miTiute cycle.t The numerator is the number of "positive cartridges,"" while Ihe denominator is the total nutnber of cartridges processed.§ Initial operating conditions: 172 kPa. I34''C, with a 2Q-minute cycle.
length exposure intervals were applied to subsequentsets of cartridges. Only one cycle ofthe high-vacuumsteam sterihzer was run even in the event of steriliza-tion failure. These additionai strips and cartridges werecultured as previously described.
Results
In all cases untreated control strips and cartridges (andstoppers) demonstrated growth after culturing, whileall process indicator-treated control strips placed onthe outside ofthe containers showed no growth.
In phase 1, sterilization of all sets of three strips wasaccomplished in all three types of sterilizers withinsingle operational cycles. Neither location ofthe strip(bottom, middle, or top) nor orientation ofthe con-tainer (upward or on-side) affected sterilization per-fonnance.
In phase 2, significant sterilization failures occurredduring the operation of all three types of sterilizers.This persisted, even when extra exposure time or anadditional cycle was ünmediately perfonned.
Table 1 presents the sterilization of spore-soiledcartridges present in sharps containers processed in anupward position. The only set of 24 cartridges thatwere all sterilized after one cycle was that of half-filledcartridges soiled with spores and blood and processedin the SA. Although sterilization of all specimens didnot occur in any other processing set, more failuresoccurred when soiled, empty cartridges were tested.The presence of blood proved not to be a confoundingfactor. Again, except for one set, sterilization of all 24soiled cartridges could not be achieved for anycartridge set, even after double processing.
The outcomes of sterilization in containers pro-cessed on their sides are presented in Table 2. Exceptfor the two-cycle UCV-processed, half-filled, spore-soiled cartridges, no set of 24 cartridges was success-Hilly sterilized in either the SA or UCV, even afterdouble exposure intervals. The presence of blood withthe spores did not result in more failures than sporesoiling alone. In most cases, cartridges with bloodexperienced fewer failures than did cartridges soiledonly with spores.
774 Quintessence International Volume 26, Number 11/1995

Infection Control
Table 2 Results of sterilization of containers processed on their sides*
Type ofsterilizer
Gravity steam*
Chemical vapor^
Gravity steam^
Chemical vapor*
Containerlocation
FrontMiddleBackFrontMiddleBack
FrontMiddleBack
FrontMiddieBack
Canridgecontents
Half filled
Half filled
Empty
Empty
One cycle
Spores
4/8*4/87/8
3/84/87/8
6/85/86/8
6/S5/85/8
Sporesand blood
0/80/81/82/81/82/8
5/81/82/6
3/84/81/8
Two cycles
Spores
0/81/80/80/80/80/8
1/84/81/80/81/81/8
Sporesand blood
0/80/81/8
1/81/80/8
1/80/80/8
1/80/81/8
* All cattridges were placed in the middle of a three-quarters-fil led container,I Initial operating conditions; 129 kPa, 124°C, with a 30-minute cycle.% The numerator is ihe number of "positive cartridges," while the denominator is the total number ofcatiridges processed.S Initial operating conditions; 172 kPa, 134°C, wilh a 20-minutc cycle.
Spore-soiled cartridges were also processed in aHVA. (Table 3). Cartridges that were soiled whilehalf-filied with anesthetic could be sterilized withineither upright or on-side containers in a single cycle.Tlie presence of blood did not affect sterilizationefficiency. In spite of being processed in a large-volume, industrial capacity high-vacuum steam auto-clave, all half-filled and empty cartridges could not besterilized.
Because intact cartridges could not be sterilized byany of the three sterilization processes, even after twocycle-lengths of exposure, the cartridges were pro-cessed white partially disassembled. Empty cartridgeswere soiled with spores only, as previously described.The rubber stopper (plunger end) was removed fromthe cartridge. The two pieces were then piacedtogether in the center ofa three-quarters-filled con-tainer and processed in the SA and the UCV Ail soiledcartridges could be sterilized, but only after two cyclelengths of exposure were run (Table 4).
Discussion
The goal of this investigation was to identifyprocedures that enhance steriiization of bacterial
Table 3 Results of sterilization of containers pro-cessed within a high-vacuum steam autoclave*
Containerodentation
UpwardUpwardUpward
UpwardUpwardUpward
On sideOn sideOn side
On sideOn sideOn side
Containerlocation
FrontMiddleBack
FrontMiddleBack
FrontMiddleBack
FrontMiddleBack
Cartddgecontent s
Half filled
Empty
Half filled
Empty
Spores
0/8*0/80/8
0/a1/81/8
0/80/S0/8
1/82/R2/8
Sporesand blood
0/80/80/8
2/81/82/6
0/80/80/8
1/82/82/8
* A single cycle, operated at 214 kPa, i3rC. for 8 minutes witli7-minute prevacuum and postvacuum steps.
t All cartridges were placed in the middle ofa three-quarters-filledcontainer.
% The numerator is the number of 'positive cartridges." while thedenominator is the total number of cartridges processed.
Quintessence internaticnal Volume 26. Number 11/1995 775

Infection Control
Table 4 Results of sterilization of containers processed in an upward position with cartridgespartially disassembled*
Type ofsterilizer
Gravity steam*
Chemical vapor^
Containerlocation
Front
BackFrontMiddleBack
Cartridgecontents^
Empty
Empty
One cycle
Rubber stopper(plunger end)
0/4"
0/40/41/40/4
Remainder ofcartridge
2/42/4
1/42/43/4
Two cycles
Rubber stopper Remainder of(plunger end) cartridge
0/40/4
0/40/40/4
0/40/40/40/40/4
' Followmg the usual procedure for contamination with spores only, the plunger end of the cartridge was removed and both pieces wereprocessed; then, each piece was cultured separately.
t All cartridges were placed in the middle of a three-quarters-filled containeri Initial operating conditions: 129 kPa, I24°C. with a 30-minute cycle.§ Initial operating conditions: 172 kPa, I34''C, with a 20-nTJnute cycle.II The numerator is the number of "positive cartridges." while the denominator is the total number of cartridges processed.
endospore-contaminated anesthetic cartridges placedwithin average-sized shatps containers. Determinationof affecting factors could help health care facilities tocomply with federal, state, provincial, or local regula-tions and guidelines as to the safer handling, storage,and treatment of filled sharps containers.
Results of phase 1 testing corroborated previousexperimentation, in which cotnmercial spore stripswere used as microbial challenges on and within avariety of differently sized sharps containers.''"^' Inthose studies, all spore strips were readily killed by theSA, UCy and HVA within a single treatment cycle.Orientation ofthe container {processed upward or ontheir sides), position of the container within thesterilizer (front, middle, or back), and location ofthestrip within the container (top, middle, or bottom) didnot negatively affect sterilizer performance.
In phase 2 ofthe present study, anesthetic cartridgeswere internally soiled with bacterial endospores orendospores plus sheep's blood. Contamination levelswere designed to equal those present on commercialspore strips used to test sterilizer effectiveness.
In the SA, UC V, and HVA the soiled cartridges weremuch more difficult to kill than were the spore strips.Also, when cartridges in the present study were pro-cessed in a manner that had resulted in sterilization ofspore-soiled tuberculin syringes or anesthetic needles
in previous experimentation,""-' sterilization of all testspecimens could not be achieved. In those studies,routine sterilization of soiled needles could be achievedin SA and UCV when the holding sharps containerswere treated on their sides for two cycles. The sporeswere killed in the HVA within one cycle, regardless ofcontainer orientation.""-'
In the present study, double cycling, the presence ofblood, the orientation ofthe sharps containers, and thelocation ofthe container within the sterilizer did notinfiuence killing efficiency- However, half-filled car-tridges had lower numbers of sterilization failures thandid soiled cartridges processed without any anestheticsolution present- The increased effectiveness could berelated to the fact that the rubber stoppers (plungerends) of about 40% ofthe half-filled cartridges wereexpelled during processing.
To investigate the effect of the separation of thestoppers from the cartridges, empty cartridges weresoiled as previously described, and then the stopperswere removed. The process was readily accomplishedby holding the glass portion with a pair of forceps andremoving the rubber stopper (plunger end) with anexplorer tip. Both the stoppers and the rest of thecartridges were treated in the SA and UCV withinsharps containers placed on their sides. After proces-sing, both items were recovered and cultured in
776 Quintessence International Volume 26, Number 11/1995

Infection Control
separate tubes. Sterilization of all soiled cartridgecomponents was realized after two sterilizationcycles.
Soiled cartridges proved to be extraordinary sterili-zation challenges. The number of cells used to soil thecartridges probably was not a determining factor,because it was the same as that present on the sporestrips, which were easily sterilized. Also, similar levelsof spores were used previously to contaminate syringesand anesthetic needles, which can be sterilized suc-cessftilly in the SA, UCV, and HVA.' -=' Cartridgesmay resist sterilization because of the presence of asmall internal positive pressure that retards the passageof steam or chemical vapor. Also, the presence ofstoppers on both ends of the cartridge's glass mbenegatively affects movement of steam or gas. This"seal" must be effective, because it was able to resist theHVA's prevacuum cycle, which usually results in therapid and efficient movement of steam throughout thecontents ofthe chamber.-- Lower rates of failure inhalf-filled cartridges can be explained by the "pop-ping" of some rubber stoppers. This wouid betterexpose the adhering spores to killing steam or gas.
The test organisms used in this study were bacterialendospores. Such spores are considered the mostphysically and chemically resistant life forms known.Thus, they presented a most demanding test forsterility. Bloodbome pathogens, such as human immu-nodeficiency virus type 1 and hepatitis B and hepatitisC viruses, are less resistant and thus are more readilykilled. Situations that result in spore death also assurethe killing of such viruses. Unfortunately, sterilizationof all test cartridges could only be achieved after theirpartial disassembly and the running of double steriliza-tion cycles.
This study was performed with the use of singlemodels of SA, UCV, and HVA sterilizers. Performancecan vary among difFerent models and even in the samesterihzer over time. Therefore, the findings may notapply to every type or model of autoclave or unsaturat-ed chemical vapor sterilizer.
Summary
1. Bacterial endospores on commercial spore stripswere readily killed when placed on or within three-quarters-filled sharps containers.
2. Anesthetic cartridges soiled internally with bacte-rial spores ofthe same number as the strips couldnot be routinely sterilized in a gravity steamautoclave or unsaturated chemical vapor sterilizer.
even when the exposure was equal to two normalcycle lengths.
3. Soiled anesthetic cartridges could not be routinelysterilized in a single cycle of a high-vacuum steamautoclave.
4. When the rubber stopper (plunger end) wasremoved from spore-soiled cartridges, sterilizationof all test specimens could be accomplished in thegravity steam autoclave and unsaturated chemicalvapor sterilizer when treatment lasted two cyclelengths.
5. Spore-soiled cartridges, when left intact, proved tobe exceptionally resistant to sterilization modalitiesthat were effective against commercial spore stripsand spore-soiled tuberculin syringes and dentalanesthetic needles.
References1. Miller CH, Palenik CJ. Infection Conliol and Managemenl of
Hazardous Materials for the Dental Team. St Louis; Mosby,1994:210-219.
2. tJS Environmental Protection Agency. 40 CFR Parts 22 and 259:Standards for tlie tracking and management of medical waste.Federal Register 19S9;54:12,326-332,395.
3. OccupalJonal Safety atid Health Admitiistration. Controlling Occu-pational Exposure to Bloodborne Pathogens in Dentistry. Washing-ton, DC: US Dept Labor, 1992:1-17.
4. US Department of Health* Human Services, Puhlic Health Service,Centers for Disease Control and Prevention and Food and DrugAdministration. Practical Infection Control In the Dental Office.Atlanta: US Dept Health & Human Services, 1993:33-34.
5. American Dental Association. Infection Control Recommendationsfor the Denial Office and the Dental Laboratory. Chicago: AmericanDental Association, 1992:1-8.
6. Gerberding ,IL, Littei C, Tarkington A. Risk of exposure of surgicalpersonnel to patients' blood during surgery at San Francisco GeneralHospital N Eng[ J Med I99O;332:I788-I793.
7. Centers for Disease Control and Prevention. Recommended in-fection-control practices for dentistry, 1993. MMWR 1993^41 IRR-8):9-|0.
8. Rubin I. Human immunodeficiency virus (HIV) disinfection andcontrol. In: Block SS (ed] Disinfection, Sterilization and Preser-vation, ed 4. Philadelphia' Lea & Febiger, 1991:472-481.
9. US Department of Labor, Occupational Safety and Health Admini-stration. OSHA Instruction CPL 2-2.44C. Washmgtor, DC: USDept Labor, 1992:1-71,
10. US Department of Labor, Occupational Safety and Health Admini-stration. 29 CFR Pait 1910. Occupational exposure to bloodbornepathogens: Final rule. Federal Register 1991;56:64004-64I82.
11. Centers for Disease Control and Prevention. Universal precautionsfor prevention of transmission of human initnunodeficiency virus,hepatitis B virus, and other blood borne pathogens in healthcaresettings. MMWR 19S8;37:377-382.
12 American Dental Association, Q&A: Infectious Waste Disposal inthe Dental Office. Chicago: American Dental Association, 1989:1-8.
13. World Heatth Organization, Oral Health Programme. Hygiene andInfection Control in Oral Care Clinics. Geneva: World HealtliOrganisation. 1992:9-10.
Quintessence International Volume 26, Number 11/1995 777

Intection Control
14. Finnish National Research and Development Cenlce for Welfare andHealth (STAKES). Hygiene Recommentiülions for Dental Sur-geries. Helsinki: STAKES, 1993:17.
15. US Environmental Prolection Agency. EPA Guide for InfectiousWasle Management (EPA/530-5W-S6-014). Washington, DC: USEnvironmenlal Protection Agency. 1986:1-12.
16. Hughes C. Questions on disposal of sharps containers. 1 HealthcareMaterial Manage 1989:7:92.
17. Palcntk CJ. Adams ML. Miller CH. EEfecliveness of steamsterilization on theconlents of sharps containers. AmJ Dent 1990:3:239-244.
18. Palcnik CJ, Riggen SD, Cells LS, Sheldrake MA, Milier CH.Effectiveness of steam autoclaving on the conlents of sharpscontainers. Clin Prev Dent 1992J4:28-34.
19. Palenik CJ. Golden LC. Effectiveness of two types of sterilizers onthe contents of sharps containers. Am J Deni 1994:7:98-102.
20. Paletiik CJ. Cumberland er NL. Effectiveness of steam autociavingon the contents of sharps containers. Am J Infect Control 1993;21 2S-33-
21. Patenik CJ. Effectiveness of two types of autoclaves on the contentsof sharps containers. Clin Performance Quality Health Care (inpresB].
22. Josyl U . Sterilization by heat. In' Block SS (ed). Disinfection,Sterilization and Preservation, ed 4. Philadelphia: Lea & Febiger,1991:495-526. D
778
An IntroductionPhilip Worthington, Brien R. Lang, and William E. LaVeiie
A concise introduction to the physical andchemical processes of osseointegration and the
practical applications of osseointegrated dentalimplants, this book provides a much-neededoverview ofthe subject. Osseointegration isexamined from its discovery and development toits current, increasingly significant place inrestorative dentistr;'. Practitioners, educators,and students alike will appreciate che hook'slogical organization, straightforward text, andclear illustrations.
CoNTENTS
• Biochemical and hiomechanicalaspectsofosseointegration
• Types of dental implants available• Intraorai and extraoral applications
• Diagnostics and treatment planning• Surgical stages of implant placement• Prosthodontic procedures• Maintenance• Complications and failure
OrderNow Toil free I-80Ü-fi2|-0587Fax 708 682^5288
s/faiKCbook/ Quintessence Publishirit; Co, Inc