effective ways of supporting patients to stop · pdf filefi l smoking cessation 16 prescriber...
TRANSCRIPT
14 ❚ Prescriber February 2017 prescriber.co.uk
■ PRESCRIBING IN PRACTICE
Smoking is the primary cause of preventable illness and pre-mature death in the UK, accounting for 81,400 deaths in
England in 2009.1 Smoking harms nearly every organ of the body and dramatically reduces both quality of life and life expectancy. Smoking causes lung cancer, respiratory disease and heart dis-ease as well as numerous cancers in other organs including lip, mouth, throat, bladder, kidney, stomach, liver and cervix. Adults with mental health problems are at particular risk. People in this group smoke 42% of all tobacco in England2 and die on average 16–25 years sooner than the general popula-tion, largely due to higher rates of respiratory and cardiovascu-lar illness, and poor survival outcomes from smoking-related illnesses like chronic obstructive pulmonary disease (COPD), which is underdiagnosed and undertreated.3 Patients with schizophrenia have a 28% five-year mortality from COPD com-pared with a 12% five-year mortality in an age-adjusted popula-tion,4 in spite of the fact that over 50% of patients with mental health disorders want to stop smoking.5 In all available studies, supporting patients to stop smoking has been shown to be an effective and highly cost-effective long-term intervention for those with smoking-related long-term disease. Table 1 lists some of the benefits of smoking cessa-tion for a wide range of diseases. Though long, even this list is not exhaustive, and suggests that supporting smokers to quit should be embedded as part of core education and treatment in every sphere of healthcare.
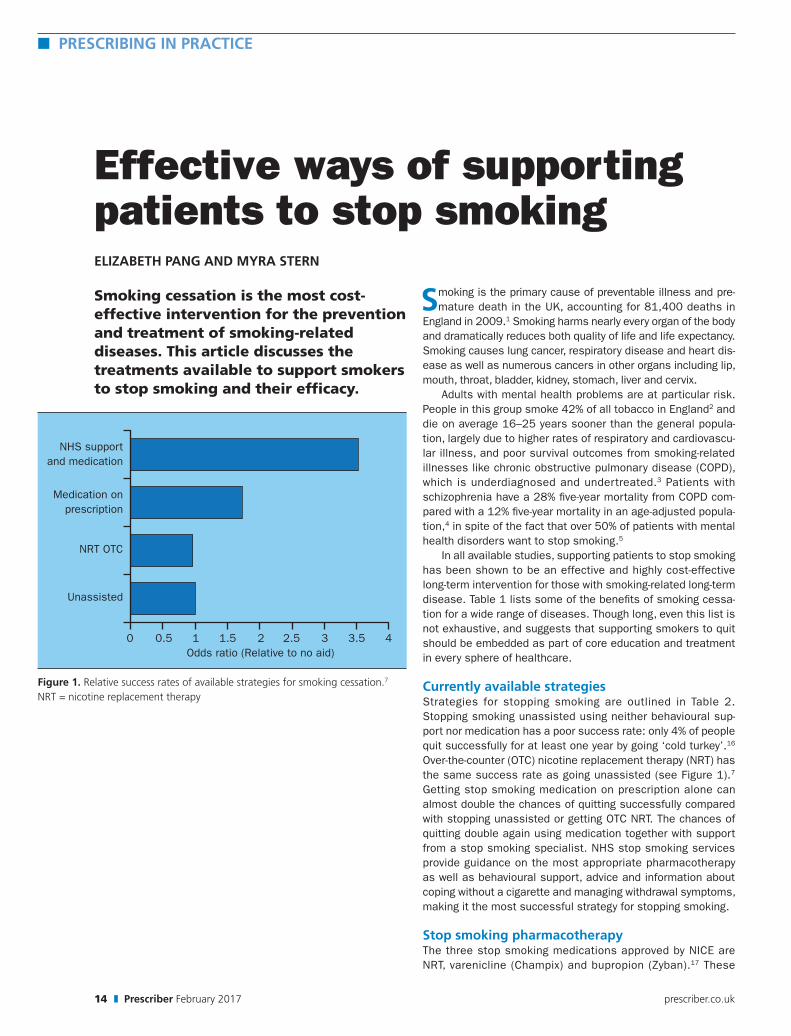
Currently available strategiesStrategies for stopping smoking are outlined in Table 2. Stopping smoking unassisted using neither behavioural sup-port nor medication has a poor success rate: only 4% of people quit successfully for at least one year by going ‘cold turkey’.16 Over-the-counter (OTC) nicotine replacement therapy (NRT) has the same success rate as going unassisted (see Figure 1).7 Getting stop smoking medication on prescription alone can almost double the chances of quitting successfully compared with stopping unassisted or getting OTC NRT. The chances of quitting double again using medication together with support from a stop smoking specialist. NHS stop smoking services provide guidance on the most appropriate pharmacotherapy as well as behavioural support, advice and information about coping without a cigarette and managing withdrawal symptoms, making it the most successful strategy for stopping smoking.
Stop smoking pharmacotherapyThe three stop smoking medications approved by NICE are NRT, varenicline (Champix) and bupropion (Zyban).17 These
Effective ways of supporting patients to stop smokingELIZABETH PANG AND MYRA STERN
Smoking cessation is the most cost-effective intervention for the prevention and treatment of smoking-related diseases. This article discusses the treatments available to support smokers to stop smoking and their efficacy.
Figure 1. Relative success rates of available strategies for smoking cessation.7
NRT = nicotine replacement therapy
NHS support and medication
Medication on prescription
NRT OTC
Unassisted
0 0.5 1 1.5 2 2.5 3 3.5 4Odds ratio (Relative to no aid)

Prescriber February 2017 ❚ 15prescriber.co.uk
Smoking cessation l PRESCRIBING IN PRACTICE ■
are extremely cost effective and all three medications should be offered as first-line products to smokers who want to stop smoking. None of these medications should be favoured over another unless there are specific contraindications.18
Although NRT can be bought OTC, varenicline and bupropion are prescription-only medications. All three medications should only be prescribed as part of an abstinent contingent treatment in which the smoker sets a quit date and commits to stopping smoking. Only two weeks of medication should be prescribed and further prescriptions should only be given to people who have shown on reassessment that they have remained absti-nent or if the clinician and client feel there is a high chance that abstinence will be achieved. Abstinence can be validated either by self-report or by measuring a person’s carbon monox-ide level.
NRTNRT is available as a patch (16 hours and 24 hours duration), mouth spray, chewing gum, lozenges and mini lozenges, inha-lator, nasal spray and microtabs (see Table 3). They all come in different strengths and are safe and effective. There are very few contraindications to NRT as it delivers nicotine in a safe form instead of in a cigarette, which delivers nicotine plus tar, carbon monoxide and more than 4000 toxic chemicals, many known to be carcinogenic. Risks and benefits of using NRT should be discussed with pregnant and breastfeeding women and young people under the age of 18 years old. The odds ratio (OR) of maintaining long-term abstinence with NRT compared with placebo is 1.84.19 There is little signif-icant difference in the effectiveness of each NRT product. The effectiveness of each product is based on individual prefer-ence. However, there is good evidence that using a combination of NRT, preferably a combination of slow-release (eg a patch) and fast-acting (eg an inhalator or mouth spray) products, is more effective than using just single NRT.19
The most common reason for poor efficacy and relapse is that an inadequate amount of NRT has been used. NRT delivers approximately half the amount of nicotine that a cigarette would deliver, therefore it is important for people to use the product frequently (on an hourly basis) and to use the maximum dose in order to maintain blood nicotine levels to make their quit attempt more comfortable and minimise withdrawal symptoms. Withdrawal from nicotine can be profoundly unpleasant, com-ing on two to three hours after the last cigarette and peaking two to three days later. Symptoms include an intense craving for nic-otine, coupled with any or all of the following: anxiety, depression, drowsiness or trouble sleeping, bad dreams and nightmares, feeling tense, restless or frustrated, headaches, increased appe-tite and weight gain, and problems concentrating. Poor technique and incorrect usage of NRT is another com-mon reason for failure. Nicotine gum, for example, is taken by chewing the gum, then resting the pellet between gum and cheek and then chewing again when the taste has faded. Resting the gum allows the nicotine to be absorbed through the lining of the mouth. If the gum is continuously chewed, the nicotine is released too quickly and is then just swallowed, providing only
minimal therapeutic effect. It is therefore highly important for people to seek advice and support with an NHS stop smoking service, which can advise them on the best ways of maximising the use of their NRT. Providing smokers with a choice of phar-macotherapy by demonstrating the actual products available facilitates better uptake of treatment by empowering smokers to decide what would work best for them (see Figure 2).
• Over a lifetime, the incremental costs per year of life gained by smoking cessation in patients with coronary artery disease were approximately 1/25 the cost of both statins in low-risk patients and ACE inhibitors in high-risk patients6
• Stop smoking support has been shown to be highly cost-effective – around £2000 per quality-adjusted life year (QALY) gained – and an effective long-term intervention for people with COPD, as long as the support is evidence based and manages the higher relapse rate and the time needed (90 minutes)7
• Evidence from a study that modelled the relative value of different COPD interventions8 demonstrated that stop smoking interventions provided great value in both diagnosed and undiagnosed populations and should be commissioned as a treatment for COPD
• Stopping smoking has been associated with a decreased risk of COPD exacerbations, with the size of the risk reduction increasing with duration of smoking abstinence9
• Stopping smoking dramatically reduces the risk of a stroke occurring; within two years of stopping smoking, a former smoker’s risk of stroke is reduced to that of a nonsmoker10
• Stopping smoking reduces all-cause mortality by 36% after an MI11 and by 21% in heart failure12
• Stopping smoking early in rheumatoid arthritis may prevent the development of high disease activity and severe extra-articular manifestations13
• Stopping smoking improves exercise tolerance in peripheral vascular disease14
• 15% of pulmonary tuberculosis (TB) diagnosed each year may be attributable to smoking alone and smoking cessation reduces the risk of premature death from TB by 50%, reduces the risk of infection in contacts and reduces the risk of relapse15
Table 1. Examples of where stop smoking support has been shown to be highly cost-effective and an effective long-term intervention for people with smoking-related long-term disease
• Self-managed quitting or reduction, eg: - ‘cold turkey’, ie an unassisted immediate quit - nicotine replacement therapy (NRT) bought over the counter - self-help literature - e-cigarettes
• Health professional-assisted evidence-based interventions using stop smoking medication provided on prescription and an NHS stop smoking service
• Alternative strategies such as acupuncture, hypnosis, homoeopathy, herbal remedies or reflexology, which can be useful for some smokers but are not evidence-based strategies
Table 2. Strategies used for stopping smoking

■ PRESCRIBING IN PRACTICE l Smoking cessation
16 ❚ Prescriber February 2017 prescriber.co.uk
Product What it does Who should use What to prescribe
Pros Cons Contraindications Side-effects
NRT
Patch Steady flow of nicotine into the blood stream
Any daily smoker 25mg/16hrs (day smokers); 21mg/24hrs (night smoking)
Easy to use, widely tolerated, steady blood levels of nicotine
Cannot titrate dose; offers no replacement activity for smoking
Skin problems (eg eczema); excessive sweating; previous allergic reaction
Possible slight skin marking/irritation
Gum Nicotine absorbed through the lining of the mouth when gum ‘parked’ after chewing
Any smoker as dual combination therapy; main item for occasional smokers
4mg when required, up to 15 pieces daily
Can titrate to needs; offers replacement for smoking
Avoid acidic drinks within 15 minutes of using
Under 12 year olds; poor dentition; caution in peptic ulcer disease
Can cause indigestion, hiccups, nausea
Lozenge Nicotine absorbed through lining of the mouth when ‘parked’ in cheek
Any smoker as dual combination therapy; main item for occasional smokers
4mg when required, up to 15 lozenges daily
Can titrate to nicotine needs; offers replacement for smoking
Caution advised for those on low sodium diet; avoid acidic drinks within 15 minutes of using
Under 12 year olds; caution in peptic ulcer disease and hypertension
Can cause indigestion and hiccups
Sublingual tablets
Nicotine absorbed through lining of the mouth/tongue
Any smoker as dual combination therapy; main item for occasional smokers
2mg when required, up to 40 tablets daily
Discrete; can titrate to needs
Tastes unpleasant; avoid acidic drinks within 15 minutes of using
Caution in peptic ulcer disease
GI discomfort, hiccups, sore mouth/throat, mouth dryness
Nasal spray
Nicotine absorbed through the lining of the nose
Any smoker as dual combination therapy; main item for occasional smokers
500µg when required, up to 64 sprays daily
Can titrate to nicotine needs; gives rapid rise in blood levels closest to cigarette effect
Difficult to use at start: sneezing, eyes watering; avoid acidic drinks within 15 minutes of using
Under 12 year olds; people with hyper-reactive airways; sinusitis
Nasal irritation (temporary)
Inhalator Nicotine absorbed directly through the lining of the mouth
Any smoker as dual combination therapy; main item for occasional smokers
15mg cartridge when required, up to 6 cartridges daily
Replacement activity for smoking; can titrate to nicotine needs
Cartridge loading can be difficult
Under 12 year olds
Throat and mouth irritation
Oral spray Absorbed through lining of the mouth
Any smoker as dual combination therapy; main item for occasional smokers
1mg/spray when required. Up to 64 sprays/day in side of mouth
Rapidly absorbed within 60 seconds
Canister difficult to open; needs to be primed before use; strong taste
Under 12 year olds; peptic ulcer disease
Dyspepsia, hiccups
Varenicline and bupropion
Varenicline Partial agonist to nicotine receptors
Long-term/highly dependent smokers
Day 1-3 0.5mg daily; day 4-7 0.5mg BD; day 8 onward 1mg BD for 11 weeks
Very effective when combined with support; can smoke for first week
Counselling on dosage essential
Under 18, pregnant/lactating women, non-daily smokers, end-stage renal disease, epilepsy
Nausea, headaches, insomnia, nasopharyngitis, abdominal pain
Bupropion Selective noradrenaline and dopamine reuptake inhibitor
Nicotine-dependent adults in combination with motivational support
150mg daily for 6 days, increasing on day 7 to 150mg twice daily
Nicotine-free but can reduce cravings and withdrawal symptoms
May impair performance of skilled tasks, eg driving
Under 18s, pregnant/lactating women, history of seizures, bulimia, anorexia nervosa, bipolar disorder, severe cirrhosis
Agitation, anxiety, seizures depression, dizziness, dry mouth, fever, headache, insomnia, rash
Table 3. Types of stop smoking pharmacotherapy, including nicotine replacement therapy (NRT), varenicline and bupropion, and their properties

■ PRESCRIBING IN PRACTICE l Smoking cessation
18 ❚ Prescriber February 2017 prescriber.co.uk
VareniclineVarenicline is a nicotinic-receptor partial agonist that helps people to stop smoking by binding the alpha4beta2 subtype of nicotinic acetylcholine receptors, blocking the ability of nicotine to bind (reducing smoking satisfaction) and stimulating the mesolimbic dopamine system (maintaining moderate levels of dopamine to counteract withdrawal symptoms). Varenicline is indicated for smoking cessation in people over 18 years old, not pregnant and not in renal failure. It is unknown whether varenicline is secreted in human breast milk therefore caution and clinical judgement needs to be taken with pregnant and breastfeeding women. Every smoker who takes varenicline should also receive behavioural support. A recent study found patients taking varenicline showed statistically superior continuous abstinence rates at weeks 9–12 and 9–24 compared with patients treated with placebo, bupropion or nicotine patch.20
The most common side-effect reported from the use of varenicline is nausea (28.6%). In the majority of cases, the nausea is mild to moderate in severity and generally subsides over time.21
There have been media reports to suggest that varenicline can increase the risk of cardiovascular events and of suicide and is therefore unsafe to be used with people with mental health problems. These reports have, however, been refuted in a meta-analysis, which demonstrated that there was no evidence of an increased risk of suicidal behaviour in patients prescribed varenicline compared with those prescribed NRT.22 In addition, a recent large study demonstrated that the use of varenicline in patients with or without a history of psychiatric disorder is not associated with a significantly increased risk of serious neu-ropsychiatric adverse events compared with placebo.20
BupropionBupropion is a selective noradrenaline and dopamine reuptake inhibitor. It has antidepressant properties and is indicated as
a stop smoking medication for smokers in combination with behavioural support. The odds ratio of bupropion achieving long-term abstinence compared with placebo is 1.82.19 Its effi-cacy is comparable with single NRT but it has been shown to be less effective than varenicline. Bupropion is contraindicated in people with seizures or cen-tral nervous system tumour, in those who are under 18 years old, pregnant or breastfeeding, those with a previous diagnosis of bulimia or anorexia nervosa, in severe hepatic cirrhosis, bipo-lar disorder and in people using monoamine oxidase inhibitors (MAOIs). Side-effects of bupropion can include rash, seizures (0.1%) and increased anxiety and depression. It also has a number of drug interactions and interactions with clinical conditions, therefore caution should be taken before recommending to a smoker.
Electronic cigarettesThe electronic cigarette (e-cigarette) is a battery-powered electronic nicotine delivery device (ENDD) designed for the purpose of providing inhaled doses of nicotine by way of a vaporised solution to the respiratory system. E-cigarettes pro-vide a flavour and physical sensation similar to that of inhaled tobacco smoke, with no smoke or combustion actually involved, although some vapour is released into the air when the smoker exhales. Propylene glycol is typically used to produce the nico-tine-carrying vapour. There are three main types of e-cigarettes or vaporisers (see Figure 3):• ‘Cig-a-like’ products This first generation of e-cigarettes was designed to resemble tobacco cigarettes. They sometimes have a light at the end that glows when the user draws on the device to resemble a lit cigarette. They are available either as nonrechargeable disposable models or as an e-cigarette kit that is rechargeable and includes replaceable prefilled cartridges.• ‘Tank’ models (also known as ‘vape’ pens) An e-cigarette that is rechargeable and has a tank or reservoir that has to be filled with liquid nicotine. • ‘Mods’ (or advanced personal vaporisers) This is a more com-plex tank model, which can be manually customised by, for example, adjusting the voltage on the device.
An estimated 2.6 million adults in the UK currently use e-ciga-rettes (‘vape’).23 E-cigarettes may be used:24–25 • To help quit smoking or avoid relapsing• To reduce cigarette consumption• To relieve tobacco withdrawal symptoms in places where there are smoking restrictions• In order not to disturb other people with smoke• To continue having a ‘smoking’ experience with reduced health risks• Because it is cheaper than smoking.
Benefits include the positive effects of abstinence from smok-ing (less coughing, improved breathing, better physical fitness),
Figure 2. Example of a patient choice box to assist smokers to choose the pharmacotherapy that would best suit them. The box is filled with dummy stop smoking products and a guideline for prescribing is included at the bottom of the box

Prescriber February 2017 ❚ 19prescriber.co.uk
Smoking cessation l PRESCRIBING IN PRACTICE ■
enjoyment of the flavour and the sensation of inhalation. Side-effects include dryness of the mouth and throat.26 Evidence on the safety of e-cigarettes is limited, and there is, as yet, no definite evidence regarding the health effects of long-term use. However, numerous studies27 now demonstrate that compared with tobacco products, e-cigarettes are signifi-cantly safer for both users and bystanders, there is no excess take up of smoking following their use, and that e-cigarettes can help people to quit smoking and may be contributing to the decline in smoking prevalence. This is important, as the public and smokers are increasingly failing to recognise that e-ciga-rettes are less harmful than smoking, suggesting that public education on this front still needs addressing. E-cigarettes were previously regulated as general consumer products, and inconsistencies in product contents and labelling have been of great concern.28 In June 2013, the Medicines and Healthcare products Regulatory Agency (MHRA) announced its intention to regulate e-cigarettes as medicines and under the EU Tobacco Products Directive (TPD), which came into effect from May 2016,29 e-cigarettes containing up to 20mg/ml of nic-otine are regulated by the TPD. Levels of 18mg/ml are reported on user websites as suitable for typical smokers.30 NHS stop smoking advisers have still been advised not to recommend that smokers wishing to quit should use e-cigarettes in favour of NHS approved smoking cessation treatments to have the best chances to quit successfully. However, for those smokers who have successfully switched to e-cigarettes, the priority should be staying off conventional cigarettes, rather than quitting e-cig-arettes.31
In summary, the role and impact of e-cigarettes has been one of the great debates in public health in recent years. Public Health England (PHE) commissioned an independent review27 of the all the latest evidence to ensure that practitioners, policy makers and, most importantly of all, the public have the best evidence available. From this review, best estimates show that e-cigarettes are 95% less harmful to health than normal ciga-rettes and, when supported by a smoking cessation service, help most smokers to quit tobacco altogether. Furthermore, the review comprehensively explains the relative risks and ben-
efits of e-cigarettes in terms of harm reduction when compared with cigarettes and as an aid to quitting.
ConclusionSmoking cessation is the most cost-effective intervention for the prevention of smoking-related disease and treatment for smokers who have smoking-related disease(s). A range of evi-dence-based treatments exists to support smokers facing the difficulty of behaviour change and breaking nicotine addiction. Supporting smokers to quit, knowing and using these interven-tions, is every clinician’s business.
References 1. HM Government. Healthy lives, healthy people: A tobacco control plan for England. March 2011. www.gov.uk/government/publications/the-tobacco-control-plan-for-england2. HM Government. No health without mental health: a cross-government mental health outcomes strategy for people of all ages. February 2011. www.gov.uk/government/publications/the-mental-health-strategy-for-england
Figure 3. Types of e-cigarette. (a) A ‘cig-a-like’ product – a first-generation e-cigarette designed to resemble tobacco cigarettes with a light at the end that glows. (b) ‘Tank’ model (also known as ‘vape’ pen) – a rechargeable device with a tank or reservoir that has to be filled with liquid nicotine. (c) ‘Mods’ (or advanced personal vaporisers) are complex tank models that can be manually customised, eg by changing the voltage on the device
Available support and resources for clinicians and smokers
NHS Smokefree is a free resource for advice to help people stop smoking. Millions have used Smokefree support to help them stop smoking. Choose from an app, Quit Kit, email, SMS and face-to-face guidance. www.nhs.uk/smokefreeShared Decision Making is a patient decision aid to help patients make an informed choice about the best route for them to stop smoking. http://sdm.rightcare.nhs.uk/pda/smoking-cessation/Action on Smoking and Health (ASH) is a campaigning public health charity that works to eliminate the harm caused by tobacco. It has useful resources for both patients who want to stop smoking or health professionals wanting to help people stop smoking. www.ash.org.ukThe National Centre for Smoking Cessation and Training (NCSCT) has lots of useful resources for healthcare professionals wanting to help people stop smoking. The NCSCT has developed a range of training, assessment and certification programmes to enable people to become more skilled stop smoking practitioners. www.ncsct.co.uk
a b cSPL
SPL

■ PRESCRIBING IN PRACTICE l Smoking cessation
20 ❚ Prescriber February 2017 prescriber.co.uk
3. Health Development Agency. Smoking and patients with mental health problems. April 2004. http://www.webarchive.org.uk/wayback/archive/20140616174051/http://nice.org.uk/nicemedia/documents/smoking_mentalhealth.pdf4. Jones DR, et al. Prevalence, severity and co-occurrence of chronic physical health problems of persons with serious mental illness. Psychiatric Services 2004;55:1250–7.5. Jochelson K, Majrowski B. Clearing the air: debating smoke free poli-cies in psychiatric units. Kings Fund. July 2006. www.kingsfund.org.uk/publications/clearing-air6. Critchley JA, et al. Life-years gained from coronary heart disease mor-tality reduction in Scotland: prevention or treatment? J Clin Epidemiol 2003;56:583–90.7. Hoogendern M, et al. Long-term effectiveness and cost-effective-ness of smoking cessation interventions in patients with COPD. Thorax 2010;65(8):711–8.8. IMPRESS. Guide to the relative value of interventions for people with COPD. 2012.9. Au DH, et al. The effect of smoking cessation on the risk of chronic obstructive pulmonary disease exacerbations. J Gen Int Med 2009;24:457.10. Kawachi I, et al. Smoking cessation and decreased risk of stroke in women. JAMA 1993;269:232–6.11. Critchley JA, Capewell S. Smoking cessation for the secondary prevention of coronary heart disease. Cochrane Database of Systemic Reviews 2003;4:CD003041.12. Suskin NS, et al. Relationship of current and past smoking to mor-tality and morbidity in patients with left ventricular dysfunction. J Am Coll Cardiol 2001;37(6):1677.13. Nyhäll-Wålin BM, et al. High disease activity disability burden and smoking predict severe extra articular manifestations in early rheuma-toid arthritis. Rheumatology 2009;48(4):416–20.14. Quick CRG, Cotton LT. The measured effect of stopping smoking on intermittent claudication. Br J Surgery 2005;69(S6):24–6.15. Dogar O, et al. Smoking cessation and respiratory disease in low- income and middle-income countries. Lancet Respir Med 2013; 1(5):e23–4.16. Hughes JR, et al. Shape of the relapse curve and long-term absti-nence among untreated smokers. Addiction 2004;99:29–38.17. West R, Brown J. Smoking and smoking cessation in England 2011. April 2012. www.smokinginengland.info 18. National Institute for Health and Care Excellence. Stop smoking services. PH10. February 2008 (updated November 2013). www.nice.org.uk/guidance/ph10
19. Cahill K, et al. Pharmacological interventions for smoking cessa-tion: an overview and network meta-analysis. Cochrane Database of Systematic Reviews 2013;5:CD009329. 20. Anthenelli RM, et al. Neuropsychiatric safety and efficacy of varen-icline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomized, place-bo-controlled clinical trial. Lancet 2016;387(10037):2507–20.21. Cahill K, et al. Nicotine receptor partial agonists for smoking ces-sation. Cochrane Database of Systematic Reviews 2011;2:CD006103.22. Thomas KH. Smoking cessation treatment and risk of depression, suicide, and self harm in the Clinical Practice Research Datalink: a prospective cohort study. BMJ 2013;347:f5704.23. ASH. Electronic cigarettes (also known as vapourisers). February 2016 http://ash.org.uk/stopping-smoking/ash-briefing-on-electronic- cigarettes-2/24. Etter JF, Bullen C. Electronic cigarette: users profile, utilization, satisfaction and perceived efficacy. Addiction 2011;106(11):2017–28. 25. Caponnetto P, et al. The emerging phenomenon of electronic ciga-rettes. Expert Rev Respir Med 2012;6(1):63–74.26. Etter JF. Electronic cigarettes: a survey of users. BMC Public Health 2010;10:231.27. McNeill A, et al. E-cigarettes: an evidence update. A report commis-sioned by Public Health England. August 2015. https://www.gov.uk/government/publications/e-cigarettes-an-evidence-update28. ASH Scotland. E-cigarettes. August 2010. http://www.ashscotland.org.uk/29. European Commission. Revision of the tobacco products direc-tive. March 2014. http://ec.europa.eu/health/tobacco/products/revision_en30. See for example: www.learn.eversmoke.com/nicotine-strength.html; www.vapertrain.com/page/hdics; www.vapehit.co.uk/info.php?articles&articles_id=2231. Foulds J, et al. Electronic cigarettes (e-cigs): views of aficio-nados and clinical/public health perspectives. Int J Clin Prac 2011;65(10):1037–42.
Declaration of interests None to declare.
Elizabeth Pang is stop smoking specialist and self-management support and behaviour change manager and Myra Stern is a consultant respiratory physician, Whittington Health, London
Visit the new-look Prescriber online at www.prescriber.co.ukThe Prescriber website has all the latest news, up-to-date features and free access to all articles published since 2006.
www.prescriber.co.uk