effective strategies for promoting attachment between...
TRANSCRIPT

NZHTA TECHNICAL BRIEF March 2007 Volume 6 Number 2
Effective strategies for promoting
attachment between young children and their parents
Carolyn Doughty
New Zealand Health Technology Assessment
Department of Public Health and General Practice
Christchurch School of Medicine and Health Sciences Christchurch, New Zealand

NEW ZEALAND HEALTH TECHNOLOGY ASSESSMENT (NZHTA) Department of Public Health and General Practice Christchurch School of Medicine and Health Sciences Christchurch, New Zealand
Effective strategies for promoting attachment between young children and their parents Carolyn Doughty
NZHTA TECHNICAL BRIEF March 2007 Volume 6 Number 2

This report should be referenced as follows: Doughty, C. J. Effective strategies for promoting attachment between young children and their parents. NZHTA Technical Brief 2005; 6(2) Titles in this Series can be found on the NZHTA website: http://nzhta.chmeds.ac.nz/attachment_interventions.pdf 2007 New Zealand Health Technology Assessment (NZHTA) ISBN 1-877235-96-2 (Print)
1-877235-97-0 (Web) ISSN 1175-7884

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
i
CONTRIBUTIONS BY AUTHORS
It was authored by Dr Carolyn Doughty (Research Fellow), who conducted the critical appraisals, prepared the report and coordinated the project.
ACKNOWLEDGEMENTS
This Technical Brief was commissioned by the New Zealand Ministry of Health.
The literature search strategy was developed and undertaken by Ms Susan Bidwell (Information Specialist Manager). Ms Cath Turnbull (Administrator) provided document formatting. Internal peer review was provided by Dr Robert Weir (Director).
DISCLAIMER
NZHTA takes great care to ensure the accuracy of the information supplied within the project timeframe, but neither NZHTA nor the University of Otago can accept responsibility for any errors or omissions that may occur. NZHTA and the University of Otago along with their employees accept no liability for any loss of whatever kind, or damage, arising from the reliance in whole or part, by any person, corporate or natural, on the contents of this paper. This document is not intended to be used as personal health advice; people seeking individual medical advice are referred to their physician. The views expressed in this report are those of NZHTA and do not necessarily represent those of the University of Otago, or the New Zealand Ministry of Health.
COPYRIGHT
This work is copyright. Apart from any use as permitted under the Copyright Act 1994 no part may be reproduced by any process without written permission from New Zealand Health Technology Assessment. Requests and inquiries concerning reproduction and rights should be directed to the Director, New Zealand Health Technology Assessment, Christchurch School of Medicine and Health Sciences, P O Box 4345, Christchurch, New Zealand.
CONTACT DETAILS New Zealand Health Technology Assessment (NZHTA) Department of Public Health and General Practice Christchurch School of Medicine and Health Sciences PO Box 4345 Christchurch New Zealand Tel: +64 3 364 3696 Fax: +64 3 364 3697 Email: [email protected] Website: http://nzhta.chmeds.ac.nz

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
ii
LEVEL OF EVIDENCE CONSIDERED IN TECHNICAL BRIEFS
Technical Briefs are rapidly produced assessments of the best available evidence for a topic of highly limited scope. They are less rigorous than systematic reviews. Best evidence is indicated by research designs which are least susceptible to bias according to the National Health and Medical Research Council’s (NHMRC) criteria (see Appendix 1) Where methodologically acceptable and applicable, appraised evidence is limited to systematic reviews, meta-analyses, evidence based clinical practice guidelines, health technology assessments and randomised controlled trials (RCTs). Where not available, poorer quality evidence may be considered.
CONFLICT OF INTEREST
None.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
iii
EXECUTIVE SUMMARY
Objective To systematically identify and appraise international evidence on the effectiveness of specific interventions for promoting attachment between young children and their parents.
Data sources
The literature was searched using the following databases: Medline, Embase, Cinahl, Current Contents, Science/Social Science Citation Index, Cochrane Central Register of Controlled Trials, Index New Zealand and Te Puna-New Zealand Bibliographic Database. Other electronic and library catalogue sources searched included the Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effectiveness, the NHS Economic Evaluation Database, Health Technology Assessment Database and the ACP Journal Club. Wider searches of the Internet, hand searching of journals and contacting of authors for unpublished research were not undertaken.
Searches were limited to English language material and published between January 1999 and December 2006 inclusive.
Study selection
Studies were included if they investigated the effectiveness of an early intervention or intervention strategy which aimed to promote the development of positive, trusting parent-child relationships. Clinical and home-based interventions including group-based parent training programmes, other types of parent training or education, home visiting programmes with a clearly identified parent training component and relationship-based interventions were considered. Key socio-emotional outcomes, usually relating to the relationship with the maternal parent must have been reported for either parental sensitivity or responsiveness to infant needs and/or infant-parent attachment security. Only relevant systematic reviews, meta-analyses and randomised controlled trials within the timeframe were eligible for appraisal.
Excluded studies included those that reported on outcomes for specific populations including adoptees, pre-term infants, and children with severe existing behavioural problems. Children with other serious mental health issues or developmental problems and mothers with drug dependency were also excluded. Interventions for preventing family violence, child abuse and neglect including interventions that target parental attitudes and behaviours around violence were not examined. Studies that focused on a primary outcome related to child physical health (breastfeeding and nutrition, intention to vaccinate, sudden infant death, accidental injury, use of medical services), brief postnatal interventions with the Brazelton Neonatal Behavioural Assessment Scale and early skin-to-skin contact or infant massage for mothers and infants were not eligible.
Data extraction and synthesis
A systematic method of literature searching, selection and appraisal was employed in the preparation of this report.
Of more than 517 potentially relevant articles/abstracts identified, 105 articles were retrieved as full text from which a final group of 20 studies were selected. Of these, two systematic reviews, 18 randomised controlled trials (represented by 24 articles) were identified as eligible for inclusion in this Technical Brief.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
iv
Key results and conclusions
Changes reported in attachment security were generally in a direction consistent with attachment theory; however effect sizes were relatively modest. Less broad interventions that target sensitive maternal behaviour are among those that are the most successful both at improving insensitive parenting and promoting better infant attachment security.
Results suggest that the most effective interventions do not always use a large number of sessions with families, in fact fewer contacts may be more effective. There is good evidence supporting the use of behaviourally focused interventions and these types of interventions, with or without video feedback are effective regardless of the presence or absence of multiple problems in the family. Highly intensive interventions with numerous sessions focusing on sensitivity, representation and support may not be as effective as less intensive approaches.
Overall, evidence from primary and secondary research shows that a variety of types of intervention for enhancing maternal sensitivity and to a lesser extent attachment security are effective, with nearly all of the studies appraised in this review involving the use of some form of home visiting to deliver the intervention.
Limitations of this report
The size of included studies ranged from very small pilot trials to larger multi-site studies. Some of the smaller studies may not be of adequate size to detect an intervention effect, if there is one, whereas the larger studies that used broader approaches although sufficiently powered may have not resulted in significant effects for a number of reasons. These types of more general home visiting programmes may be more likely to show patterns of small pervasive benefits than large effect sizes for specific outcomes.
Differential attrition may present an issue for these longer term interventions as it may be difficult for the control group to remain motivated to participate in the face of problems but no active support from the programme. For studies in which specific populations were targeted, treatment effects found may hold only for the participants of that specific sample and results may not be generalisable to other groups. All of the studies considered focused on exclusively mother-infant interaction rather than father or parent-child interaction which are consistent with previous reviews that have only noted several such studies.
Within individual studies the aim or objective was often described but without reference to the specific individual components of the intervention or the process by which intervention goals were achieved. Although research only trials were in theory excluded from this review, in the absence of predetermined criteria to ascertain what this meant in practice (eg. laboratory versus community setting) a small minority of the included studies may be nearer to being efficacy than effectiveness trials. Efficacy studies may not truly reflect how a therapeutic intervention might be more flexibly applied in a real world setting as opposed to the research setting but remain informative for considering what interventions demonstrate potential and therefore what future research might be indicated.
MeSH headings
parent-child relations, object attachment, child-preschool, infant, early intervention (education), family therapy, intervention studies, prevention
Additional key words
Attachment, resilience, wellbeing, well being, wellness, early intervention, parent$ program$, parent$ train$, parent$, educat$, home visit$, domiciliary visit$, family visit$, multisystemic therapy, healthy steps, healthy start, early start, healthy famil$, (promot$ and wellbeing or wellness or attachment or well being).

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
v
TABLE OF CONTENTS
CONTRIBUTIONS BY AUTHORS.................................................................................................................... I ACKNOWLEDGEMENTS............................................................................................................................... I DISCLAIMER............................................................................................................................................... I COPYRIGHT ................................................................................................................................................ I CONTACT DETAILS ..................................................................................................................................... I LEVEL OF EVIDENCE CONSIDERED IN TECHNICAL BRIEFS .......................................................................... II CONFLICT OF INTEREST ............................................................................................................................. II EXECUTIVE SUMMARY .............................................................................................................................III Objective .................................................................................................................................................................. iii Data sources ............................................................................................................................................................ iii Study selection ......................................................................................................................................................... iii Data extraction and synthesis .................................................................................................................................. iii Key results and conclusions ...................................................................................................................................... iv Limitations of this report........................................................................................................................................... iv MeSH headings ......................................................................................................................................................... iv Additional key words................................................................................................................................................. iv TABLE OF CONTENTS.................................................................................................................................V LIST OF TABLES........................................................................................................................................VI BACKGROUND...........................................................................................................................................1 SELECTION CRITERIA.................................................................................................................................3 Study inclusion criteria ..............................................................................................................................................3 Study exclusion criteria..............................................................................................................................................4 MAIN SEARCH TERMS................................................................................................................................4 Principal sources of information................................................................................................................................4 SEARCH SOURCES......................................................................................................................................5 Search methodology...................................................................................................................................................5 APPRAISAL METHODOLOGY ......................................................................................................................5 RESULTS ...................................................................................................................................................5 OVERVIEW ..............................................................................................................................................39 Overall quality of evidence ......................................................................................................................................39 Summary of evidence for the effectiveness of interventions promoting attachment between young children and their parents............................................................................................................................................................39 Discussion................................................................................................................................................................44 Conclusions..............................................................................................................................................................47 REFERENCES ...........................................................................................................................................48 APPENDIX 1: LEVELS OF EVIDENCE.........................................................................................................52 APPENDIX 2: SEARCH STRATEGY ............................................................................................................54 APPENDIX 3A: EXCLUDED RETRIEVED PAPERS........................................................................................58 APPENDIX 3B: APPRAISED RETRIEVED PAPERS (EXCLUDED) ...................................................................68 APPENDIX 4: APPRAISED RETRIEVED PAPERS..........................................................................................70

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
vi
LIST OF TABLES
Table 1. Typology of child attachment patterns or responses to the “strange situation”.......... 1 Table 2. Evidence table of a secondary research appraised relating to effective strategies
for promoting attachment between young children and their parents......................... 7 Table 3. Evidence table of primary research appraised relating to effective strategies
for promoting attachment between young children and their parents....................... 11 Table 4. Summary of aim, mode of delivery, settings and theoretical basis of interventions
appraised in primary studies ..................................................................................... 41 Table 5. Summary of direction of observed effect in intervention group by outcome and
the statistical significance/size of the effect ............................................................. 45

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
1
BACKGROUND
This Technical Brief was requested by Dr Pat Tuohy, Chief Advisor of Child and Youth Health, New Zealand Ministry of Health and aimed to critically appraise the evidence for effectiveness of a range of early intervention strategies seeking to promote attachment between young children and their parents.
The scope of this report reflects the Ministry of Health’s priority to understand what actions can be taken or future services developed to ensure healthy socio-emotional development, including secure attachment in young children before they start school. Healthy child development has been identified as one of the key determinants of health and resiliency in adulthood. Therefore parent support interventions aimed at improving the parent-child relationship are indirectly targeting the future resilience capacity of children for whom healthy development may be at risk.
Research indicates that the quality of the parent-infant relationship creates conditions for establishing healthy patterns of functioning throughout childhood and adulthood. Early secure attachments with parents provide a firm basis for secure attachments later in life. Furthermore, insecure attachment prior to the age of 2 years is associated with a range of poor outcomes that includes conduct problems, low sociability, poor peer relations, anger, and poor behavioural self-control during the preschool years (Barlow and Parsons 2006) and beyond. In a classic treatise on attachment Ainsworth and colleagues (1978) described a method of categorising infants’ responses using the “strange situation”. The categories that result from this procedure are based on the child’s behaviours when the child and mother are alone in the playroom together, when the mother leaves the room, when a strange women offers comfort, and when the mother returns.
Table 1. Typology of child attachment patterns or responses to the “strange situation”
Anxious/Avoidant mother and child are left alone together in playroom
the child is more or less indifferent to where their mother is sitting
may or may not cry when their mothers leave the room
if the child becomes distressed, strangers are likely to be as effective as comforting them as their mothers
when the mother returns these children may turn or look away from her instead of seeking closeness or comfort.
Securely Attached if the mother is present, the child plays comfortably with the toys in the playroom and reacts positively to the stranger
the child become visibly and vocally upset when their mothers leave
the child is unlikely to be consoled by a stranger
when the mother reappears, the child climbs into her arms, quickly calms down and resumes playing
Anxious/Resistant these children have trouble from the start in the strange situation
the child stays close to their mother and appears anxious even when their mother is near
the child becomes very upset when their mother leaves, but is not comforted by her return
the child may seek renewed contact with their mother and resist her efforts to comfort them
the child may cry angrily to be picked up with their arms outstretched, but will struggle to climb down once they are in their mother’s arms
these children do not readily assume playing after their mother returns, instead they keep a wary eye on her.
After (Ainsworth et al. 1978; Cole and Cole 1997)
Further to this typology, some child-parent attachment relationships appear to be characterised by the absence or breakdown of an organised strategy, for dealing with the stresses of separations, illness, and other life threatening events. This has been described as disorganised attachment (Juffer et al. 2005). The rates of disorganised attachment in low-risk families are about 15% compared to high-risk samples where elevated rates (up to 80%) have been found. Disorganised attachment in infancy has been shown to predict problems with stress management, increased externalising behaviour and dissociative behaviour in adolescence (Juffer et al. 2005b). It is considered to be of clinical importance as it is also predictive of later psychopathology. It highlights the need to search for determinants of attachment disorganisation with the goal of developing effective child-parent interventions to mitigate its effect on normal child development.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
2
This Technical Brief focuses on identifying studies that have experimentally evaluated attachment-based interventions. Experimental intervention studies that aim at changing parental behaviour or children’s development are important partly because of the dominance of non-experimental research in the field of parenting and child development. Descriptive, cross-sectional or longitudinal designs are far more common than experimental studies but a moderate number of experimental studies have been conducted. Of these, only a minority of studies target low risk parents with healthy children with more studies being concerned with interventions designed for infants at risk for problematic socio-emotional development, for parents in adverse circumstances, or for families with both parents and children at-risk. Studies frequently examine special groups of children including families with premature infants (Brisch et al. 2003), clinically referred children (Cohen et al. 1999) or mothers (Field et al. 1998; Suchman et al. 2004), children with developmental disabilities, anxious-withdrawn preschoolers (LaFreniere and Capuano 1997), or internationally adopted infants (Juffer et al. 1997) but these particular studies were outside the scope of this report.
Dunst et al. (2004) noted that parental sensitivity has been implicated as a factor influencing and contributing to variations in child developmental outcomes. Ainsworth (1978) defined sensitivity as the ability to perceive the child’s signals correctly and react to these signals promptly and adequately. Sensitivity has been proposed to have a causal role in shaping attachment. For this reason, many interventions that have the goal of promoting children’s emotional and social development, especially their attachment security attempt to do so by enhancing maternal sensitivity or responsiveness. In these types of intervention the parent’s behaviour toward the child is the focus of the intervention. Attachment-based interventions start at the most basic level of sensitivity and aim to make parents better perceivers of their child’s needs by teaching them observational skills. Intervenors may also encourage and train parents to perceive their child’s behaviour in a more objective way, by explaining salient issues around child development.
The primary focus of this Technical Brief was to review recent evidence from systematic reviews and randomised controlled trials about a range of early intervention strategies that seek to promote attachment between young children and their parents.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
3
SELECTION CRITERIA
Study inclusion criteria
Publication type
Studies published between January 1999 and December 2006 inclusive in the English language, including primary (original) research (published as full original reports) and secondary research (systematic reviews and meta-analyses) appearing in the published literature.
Context
Studies reporting on effective strategies for promoting attachment between young children and their parents
Population of interest
Infants and young children aged 0 to 4 years, inclusive. Parent/s or primary caregivers of sample children.
Setting
Community (home or clinic)
Intervention
Studies that investigate the effectiveness of an early intervention or strategy which aims to promote the development of positive, trusting parent-child relationships.
Clinical and home-based interventions may be universal or selective and include
group-based parent training programmes other parent training or education programmes home visiting programmes with a clearly identified parent training component relationship-based interventions
Outcomes
Key socio-emotional outcomes, usually relating to the relationship with the maternal parent must have been reported in either of the following categories:
parental sensitivity or responsiveness to infant needs infant-parent attachment security
Outcomes measures directly addressing sensitivity and attachment including but not limited to the:
Ainsworth sensitivity rating scales (e.g. strange situation) Home Observation for Measurement of the Environment (HOME) Erickson rating scales for maternal sensitivity and supportiveness Nursing Child Assessment Feeding (NCAFS) and Teaching Scales (NCATS)
Study design
Systematic review or meta-analysis Randomised controlled trials
Sample size
Studies with samples of at least 10 participants.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
4
Study exclusion criteria
Studies were excluded if they:
were non-systematic reviews, letters, editorials, expert opinion articles, comments, book chapters, articles published in abstract form, and studies on animal subjects,
were not published work or were non-English language articles, were evidence obtained from comparative studies, case series, either post-test or pre-test/post-test,
(Level III and IV intervention evidence). reported on programmes that focused on settings where 50% or more of the sample had a mean
age > 5 years reported only outcomes for specific populations where 50% or more of the sample were
adoptees, pre-term infants, children with severe existing behavioural problems, children with other serious mental health issues or developmental problems or mothers with drug dependency
other multi-component or comprehensive programmes except where specific outcomes of interest were clearly reported
focused on specific interventions for preventing family violence, child abuse and neglect including interventions that target parental attitudes and behaviours around violence
did not clearly describe the methods and results, or where there were significant discrepancies were implemented only in a research setting focused on a primary outcome related to child physical health (breastfeeding and nutrition,
intention to vaccinate, sudden infant death, accidental injury, use of medical services) were on brief postnatal interventions with the Brazelton Neonatal Behavioural Assessment Scale were on early skin-to-skin contact or infant massage for mothers and infants were on parental satisfaction with services or programmes evaluated the process of the early intervention (e.g. uptake of programme) rather than eligible
outcomes
MAIN SEARCH TERMS
MeSH headings (Medline subject headings): parent-child relations, object attachment, child-preschool, exp infant, “early intervention (education)”, family therapy, intervention studies, pc.fs (prevention & control as floated subheading)
Embase subject headings (where different from Medline): emotional attachment
PsychInfo subject headings (where different from Medline): attachment behavior, early intervention, parent training, family intervention, exp multimodal treatment approach, treatment effectiveness evaluation
Additional free text (used in all databases): attachment, resilience, wellbeing, well being, wellness, early intervention, (parent$ adj3 program$), (parent$ adj3 (train$ or educat$)), (home adj2 visit$), domiciliary visit$, (family adj2 visit$), multisystemic therapy, healthy steps, healthy start, early start, healthy famil$, (promot$ and (wellbeing or wellness or attachment or well being))
Correspondence was excluded from the search and references with vaccination, immunisation or breastfeeding (or variant forms) in the title of the article were excluded in all databases.
Full details of the search strategies are presented in Appendix 2.
Principal sources of information Bibliographic databases Medline PubMed (last 90 days) Embase
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
5
Cinahl Psychinfo Current Contents Cochrane Central Register of Controlled Trials Review databases Cochrane Database of Systematic Reviews DARE database NHS Economic Evaluation Database Health Technology Assessment Database ACP Journal Club
References of all retrieved papers were scanned for further relevant studies.
Extended searching of internet websites, meeting abstracts, hand searching of journals, and contacting of authors for unpublished data was not undertaken for this Technical Brief.
SEARCH SOURCES
Search methodology
Searches were for material in English published from 1999 onwards. Searches of Medline and PsychInfo were carried out on 12 October 2006. Other databases were searched on 8 January 2007. A follow-up search for additional material on home visiting was carried on 26 January 2007 and an update of the Medline and PsychInfo databases on 8 February 2007.
APPRAISAL METHODOLOGY
Summaries of appraisal results are shown in tabular form (known as Evidence Tables) which detail study design, study setting, sample, methods, results, reported conclusions and NZHTA reviewer conclusions/comments based on the limitations and validity of the study. The spelling of the original article is retained in the Evidence Tables.
The evidence presented in the selected studies were assessed and classified according to the NHMRC’s revised hierarchy of evidence (Appendix 1).
RESULTS
From the above search strategy we identified 517 potentially relevant articles/abstracts of which 108 were retrieved. Of these retrieved articles, 81 were excluded. These papers, annotated with the reason for exclusion, are presented in Appendix 3a.
primary outcomes of interest were not evaluated at all (n=18) narrative review or background article (n=17) attachment interventions and related outcome were not the focus of primary or secondary study
(n=15) population outside scope (n=10) descriptive or cross sectional study (n=8) they focused on home environment (HOME) only and did not examine any other relevant
outcomes (n=6) case study or pretest/post-test study (n=3) editorial, commentary or book chapter (n=2) letter to the editor or conference abstract (n=1) research focus only (n=1)

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
6
Two secondary studies and 18 primary studies (from a total of 24 articles) were critically appraised (listed in Appendix 4). The included papers are presented in the evidence tables on the following pages. Two systematic reviews that were directly relevant to the present review were identified, although it is noted that neither of these were exclusively reviews of controlled trials. However the review by Bakermans-Kranenburg et al. (2003) did establish a core set of randomised controlled trials on which their principal analyses were based. All of the primary studies selected for inclusion were level II according to NHMRC’s hierarchy of intervention evidence (NHMRC 2005).
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
7
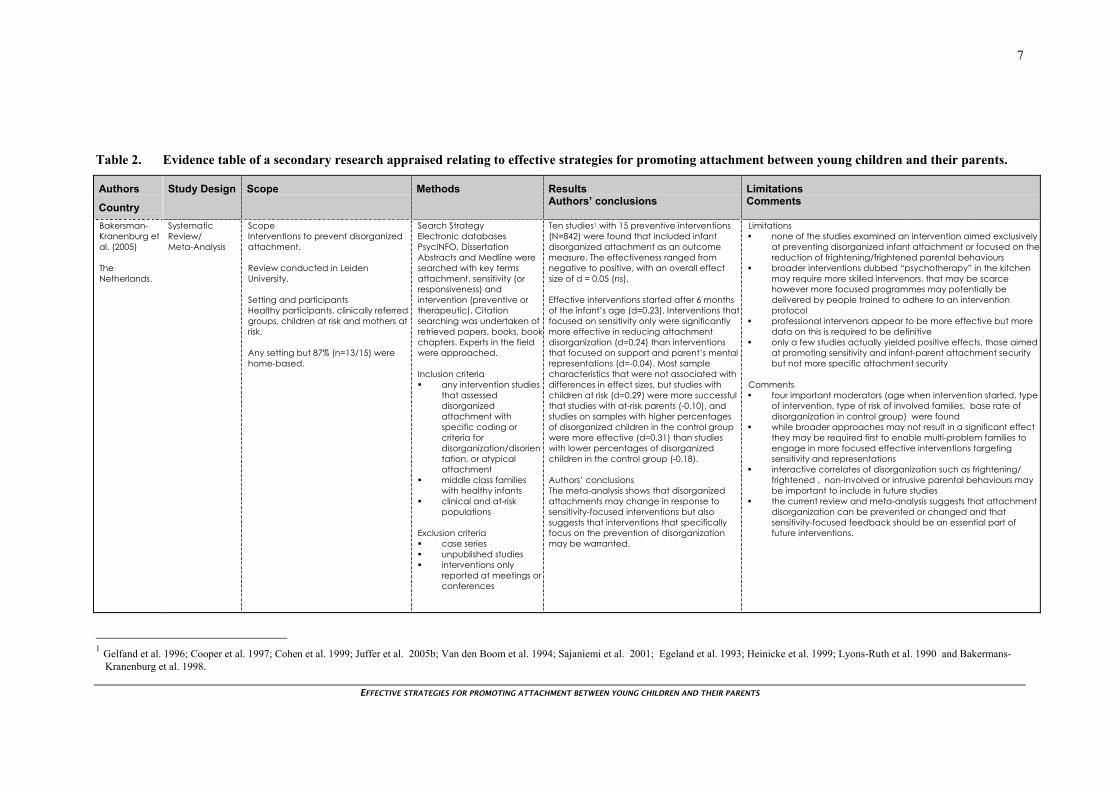
Table 2. Evidence table of a secondary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors
Country
Study Design Scope Methods Results Authors’ conclusions
Limitations Comments
Bakersman-Kranenburg et al. (2005) The Netherlands.
Systematic Review/ Meta-Analysis
Scope Interventions to prevent disorganized attachment. Review conducted in Leiden University. Setting and participants Healthy participants, clinically referred groups, children at risk and mothers at risk. Any setting but 87% (n=13/15) were home-based.
Search Strategy Electronic databases PsycINFO, Dissertation Abstracts and Medline were searched with key terms attachment, sensitivity (or responsiveness) and intervention (preventive or therapeutic). Citation searching was undertaken of retrieved papers, books, bookchapters. Experts in the field were approached. Inclusion criteria any intervention studies
that assessed disorganized attachment with specific coding or criteria for disorganization/disorientation, or atypical attachment
middle class families with healthy infants
clinical and at-risk populations
Exclusion criteria case series unpublished studies interventions only
reported at meetings or conferences
Ten studies1 with 15 preventive interventions (N=842) were found that included infant disorganized attachment as an outcome measure. The effectiveness ranged from negative to positive, with an overall effect size of d = 0.05 (ns). Effective interventions started after 6 months of the infant’s age (d=0.23). Interventions that focused on sensitivity only were significantly more effective in reducing attachment disorganization (d=0.24) than interventions that focused on support and parent’s mental representations (d=-0.04). Most sample characteristics that were not associated with differences in effect sizes, but studies with children at risk (d=0.29) were more successful that studies with at-risk parents (-0.10), and studies on samples with higher percentages of disorganized children in the control group were more effective (d=0.31) than studies with lower percentages of disorganized children in the control group (-0.18). Authors’ conclusions The meta-analysis shows that disorganized attachments may change in response to sensitivity-focused interventions but also suggests that interventions that specifically focus on the prevention of disorganization may be warranted.
Limitations none of the studies examined an intervention aimed exclusively
at preventing disorganized infant attachment or focused on thereduction of frightening/frightened parental behaviours
broader interventions dubbed “psychotherapy” in the kitchen may require more skilled intervenors, that may be scarce however more focused programmes may potentially be delivered by people trained to adhere to an intervention protocol
professional intervenors appear to be more effective but more data on this is required to be definitive
only a few studies actually yielded positive effects, those aimed at promoting sensitivity and infant-parent attachment security but not more specific attachment security
Comments four important moderators (age when intervention started, type
of intervention, type of risk of involved families, base rate of disorganization in control group) were found
while broader approaches may not result in a significant effect they may be required first to enable multi-problem families to engage in more focused effective interventions targeting sensitivity and representations
interactive correlates of disorganization such as frightening/ frightened , non-involved or intrusive parental behaviours may be important to include in future studies
the current review and meta-analysis suggests that attachment disorganization can be prevented or changed and that sensitivity-focused feedback should be an essential part of future interventions.
1 Gelfand et al. 1996; Cooper et al. 1997; Cohen et al. 1999; Juffer et al. 2005b; Van den Boom et al. 1994; Sajaniemi et al. 2001; Egeland et al. 1993; Heinicke et al. 1999; Lyons-Ruth et al. 1990 and Bakermans-
Kranenburg et al. 1998.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
8
Table 2. Evidence table of secondary research appraised relating to the effectiveness of interventions to promote attachment
Authors
Country
Study Design Scope Methods Results Authors’ conclusions
Limitations Comments
Bakersman-Kranenburg et al. (2005) The Netherlands. Continued
A detailed coding system was used to rate every intervention study on design, sample and intervention characteristics. Studies were coded independently by two raters and intercoder reliability established.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
9
Table 2. Evidence table of secondary research appraised relating to the effectiveness of interventions to promote attachment
Authors
Country
Study Design Scope Methods Results Authors’ conclusions
Limitations Comments
Bakersman-Kranenburg et al. (2003) The Netherlands.
Systematic Review/ Meta-Analysis
Scope Interventions to enhance parental sensitivity and infant attachment security. Review conducted in Leiden University. Setting and participants Healthy participants, clinically referred groups, children at risk and mothers at risk. Any setting but 78% (n=40/51) were home-based.
Search Strategy Electronic databases PsycINFO, Dissertation Abstracts and Medline were searched with key terms attachment, sensitivity (or responsiveness) and intervention (preventive or therapeutic). Citation searching was undertaken of retrieved papers, books, bookchapters. Experts in the field were approached. Inclusion criteria interventions starting
before children’s mean age of 54 months
studies using classic Ainsworth sensitivity rating scales
studies with posttests based on the Home Observation for Measurement of the Environment (HOME)
studies using the NursingChild Assessment Teaching Scale (NCATS)
Erickson rating scales forsensitivity and supportiveness
Exclusion criteria case series unpublished studies interventions only
reported at meetings or conferences
Seventy studies were traced including 88 interventions. Data on 9957 children and theirparents were reported. A total of 88 intervention effects on sensitivity (n=7636) and/or attachment (n=1503) were produced. To estimate the combined effect size in the set of studies with the strongest designs only the intervention studies with randomized control group design were selected. A core set of 51 RCTs was established (6282 mothers with their children). Interventions were moderately effective in enhancing maternal sensitivity (d=0.33, p<0.001). Random studies were less effective than other studies (d=0.61, p<0.001). Interventions focusing on sensitivity only (d=0.45, p<.001), combined sensitivity and support (d=0.27, p<0.001), combined representation, sensitivity and support (d=0.46, P<0.001) showed substantial effect sizes. Interventions focusing on sensitivity only were more effective (d=.45) than all other types of interventions combined (d=0.27, p=0.03). Interventions with video feedback were more effective (d=0.44) than interventions without this method (d=0.31, p=0.04). Interventions with fewer than five sessions were as effectives (d=0.42) as interventions with 5 to 16 sessions (d=0.38) but interventions with more than 16 sessions were less effective (d=0.21) than interventions with a smaller number of sessions (p<0.001). Interventions starting later (d=0.44) were more effective than interventions starting prenatally(d=0.32) or in the first 6 months of life (d=0.28, p=0.04).
Limitations in general attachment security may be more difficult to change
than maternal insensitivity small samples may lack power to detect a moderate
intervention effect randomization with a small number of participants may result in
systematic differences between control and experimental groups
there may be a ceiling effect when relatively high scores in the control group prevent any intervention effects from being detected
sleeper effects (time lag between changes in sensitivity and attachment) may make it difficult to evaluate program effectiveness as only long-term effects on deeply rooted relational or representational characteristics are to be expected
analyses were limited to maternal sensitivity Comments some studies with outlying effect sizes were identified and
excluded from further analysis (Van den Boom 1994 and a subsample of Zahr 2000)
to avoid excessive influence of the large multisite intervention study (St Pierre and Layzer) analyses for this study were based in the windsorized number
only a small number of the interventions were aimed at both mothers and fathers (three studies in total)
fail-safe n=913, that is it would take more than 900 unpublished studies without intervention effects to cancel out combined effect size of randomized studies

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
10
Table 2. Evidence table of secondary research appraised relating to the effectiveness of interventions to promote attachment
Authors
Country
Study Design Scope Methods Results Authors’ conclusions
Limitations Comments
Bakersman-Kranenburg et al. (2003) The Netherlands Continued.
brief postnatal interventions with the Brazelton Neonatal Behavioral Assessment Scale
A detailed coding system was used to rate every intervention study on design, sample and intervention characteristics. Studies were coded independently by two raters and intercoder reliability established. Disagreements were discussed to consensus.
Authors’ conclusions The current meta-analytic data suggest that interventions with a clear focus and a modest number of sessions are preferable. Interventions with an exclusively behavioural focus on maternal sensitivity appear to be themost effective not only in enhancing maternal sensitivity but also in promoting children’s attachment security.
four studies that did not use personal contact as a means of intervening (d=0.62, p<.05) had largest effect sizes. These studiesrelied on holding infant close (soft baby carriers, snugglies, kangaroo method etc). It is paradoxical that interventions with the smallest investment in terms of time and money tended to be more effective than more elaborate interventions but this difference was not significant and its important to note the precision of the estimate was low and the subset of studies small.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
11
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Ammaniti et al. (2006) Italy
Interventions Home Visiting Program (HV) Control Scheduled visits for data collection only
Participant families were recruited from maternity and child health services in the second trimester of pregnancy. Home Visiting (HV), n=47 Control (nHV), n=44 Three groups of participants were selected for inclusion on the basis of a psychosocial risk interview and the Center for Epidemiological Studies-Depression Scale (CES-D) Inclusion criteria (1) depressive risk (DR) women with one or no psychosocial risk factors (CES-D 20, Psychosocial risk variable 0-1) (2) a group of psychosocial risk women (PR) who reported low levels of depressive symptoms (CES-D 10, Psychosocial risk variable 3) (3) low risk women (LR) with one or no psychosocial risk factor and low levels of depressive symptoms (CES-D 10, Psychosocial risk variable 0-1) Exclusion criteria None stated. No significant baseline differences in depression scores and risk variables between intervention and control groups were reported. DR (n=30), PR (n=28) and LR (n=33) mothers were equally distributed across the intervention and control conditions.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline and at 3, 6 and 12-month follow-up. Attrition n=19 mothers (17.2% of women who agreed) dropped out in the first three months of the program Assessment and outcome measures Semi-structured interview about mental representations and changes in these (IRMAG and IRMAN respectively) Adult attachment interview (AAI) Scales of Mother-Infant Interactional System CES-D Strange Situation Procedure (SSP)
Selected observations of maternal and infant behavior: 6 months nHV HV p n=33 n=36 Sensitivity 6.89 (1.20) 7.70 (0.77) 0.002 Cooperation 7.77 (1.17) 8.25 (0.67 0.04 Interference 2.12 (1.32) 1.55 (0.72) 0.03 Affective state of mother 1.53 (0.74) 1.08 (0.28) 0.003 Self regulation 4.52 (1.68) 4.16 (2.22) n.s. 12 months nHV HV p n=37 n=45 Sensitivity 6.67 (1.31) 7.25 (1.06) 0.03 Cooperation 7.67 (1.19) 8.11 (0.94) 0.06 Interference 1.52 (0.80) 1.36 (0.81) n.s. Affective state of mother 1.39 (0.66) 1.15 (0.44) 0.06 Self regulation 1.96 (0.99) 1.92 (0.95) n.s. Effects of the home visiting program on mother-infant interaction tended to persist until 12 months, although to a lesser degree. Mothers in the HV group tended to show more sensitivity (p<.03) and more cooperation (p<.06) when interacting with the infant, and their affective state was inclined to be more positive (p<.06). No significant differences were found between the DR and LR groups but mothers in the PR group who were home visited showed lower rates on interference (p<.07), and negative affective state (p<.03). These mothers showed lower interference behaviors and a more positive mood than did the nHV mothers.
Limitations the process of allocation was not clearly stated though it
was described as being “randomly spilt into two subgroups” the authors suggest that compared to the US or UK, home
visiting in Italy is in a very early stage of development and women are less prone to welcome strangers into their houses, even if they are health visitors. Program was very intensive both for the number of visits in the first year and for the kinds of assessments carried out through interviews and videotaped observations.
dropouts could also be due to difficulty keeping engagement they experienced as demanding and potentially judging
the efficacy of the intervention could be less evident due to the inverted-U shaped association between the number of risk factors and efficacy of prevention, where intervention effects in samples with too-few risk factors, as per this sample, could be less clear
possibility exists that both groups are biased as the rate of women who refused to join the program was relatively high
the distribution of mothers in the sample with secure attachment (65-85%) was higher than previously reported in clinical samples (55%)
Comments
the primary goal of the study was to investigate whether the home visiting program would be effective in enhancing the quality of mother-infant interaction in psychosocial and depressive risk samples, specifically to enhance the mothers capacity to read and interpret the signals and behaviours of the child
intervention was designed specifically to promote child development, improve parenting practices, and facilitate positive parent-child relationships and was theoretically based on attachment theory
it may be that the efficacy of the intervention changes at a developmental stage of the child during which the mother faces new developmental tasks of the child that are linked to autonomy and self-assertion

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
12
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Ammaniti et al. (2006) Italy Continued
Authors’ conclusions The study found that the home visiting intervention was effective in improving sensitive maternal behaviors toward the child after 6 months of intervention.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
13
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
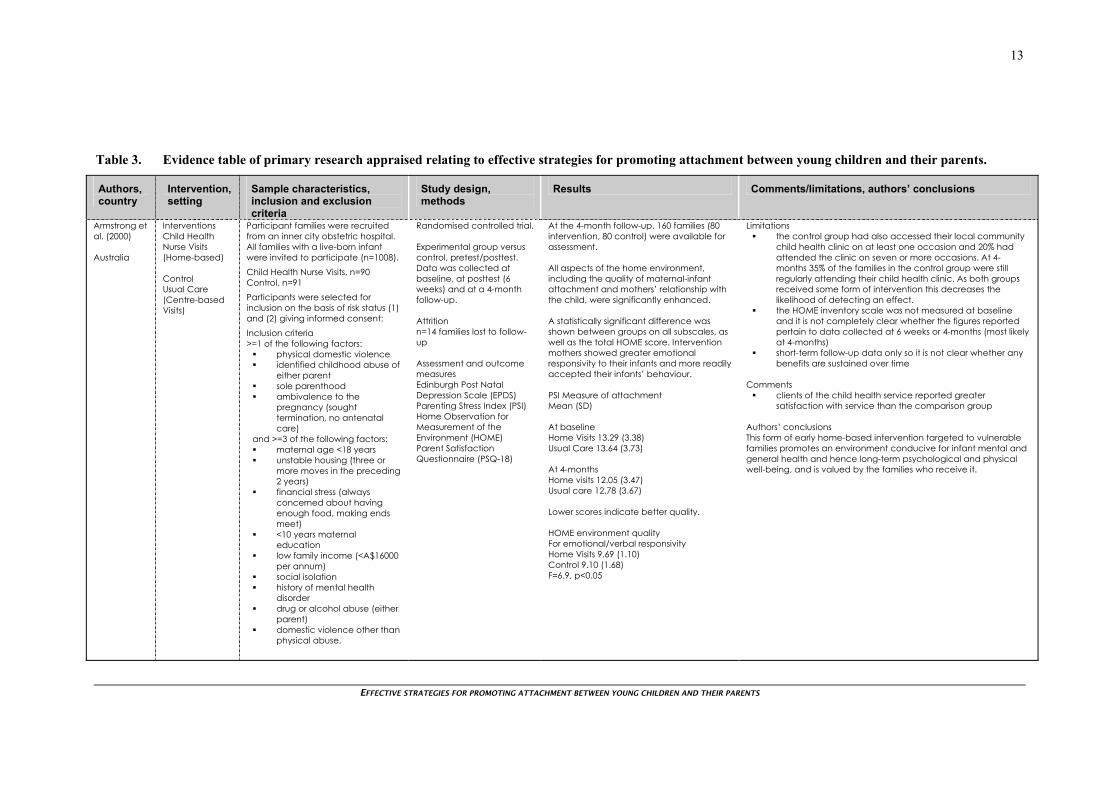
Armstrong et al. (2000) Australia
Interventions Child Health Nurse Visits (Home-based) Control Usual Care (Centre-based Visits)
Participant families were recruited from an inner city obstetric hospital. All families with a live-born infant were invited to participate (n=1008). Child Health Nurse Visits, n=90 Control, n=91 Participants were selected for inclusion on the basis of risk status (1) and (2) giving informed consent: Inclusion criteria >=1 of the following factors:
physical domestic violence identified childhood abuse of
either parent sole parenthood ambivalence to the
pregnancy (sought termination, no antenatal care)
and >=3 of the following factors: maternal age <18 years unstable housing (three or
more moves in the preceding 2 years)
financial stress (always concerned about having enough food, making ends meet)
<10 years maternal education
low family income (<A$16000 per annum)
social isolation history of mental health
disorder drug or alcohol abuse (either
parent) domestic violence other than
physical abuse.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data was collected at baseline, at posttest (6 weeks) and at a 4-month follow-up. Attrition n=14 families lost to follow-up Assessment and outcome measures Edinburgh Post Natal Depression Scale (EPDS) Parenting Stress Index (PSI) Home Observation for Measurement of the Environment (HOME) Parent Satisfaction Questionnaire (PSQ-18)
At the 4-month follow-up, 160 families (80 intervention, 80 control) were available for assessment. All aspects of the home environment, including the quality of maternal-infant attachment and mothers’ relationship with the child, were significantly enhanced. A statistically significant difference was shown between groups on all subscales, as well as the total HOME score. Intervention mothers showed greater emotional responsivity to their infants and more readily accepted their infants’ behaviour. PSI Measure of attachment Mean (SD) At baseline Home Visits 13.29 (3.38) Usual Care 13.64 (3.73) At 4-months Home visits 12.05 (3.47) Usual care 12.78 (3.67) Lower scores indicate better quality. HOME environment quality For emotional/verbal responsivity Home Visits 9.69 (1.10) Control 9.10 (1.68) F=6.9, p<0.05
Limitations the control group had also accessed their local community
child health clinic on at least one occasion and 20% had attended the clinic on seven or more occasions. At 4-months 35% of the families in the control group were still regularly attending their child health clinic. As both groups received some form of intervention this decreases the likelihood of detecting an effect.
the HOME inventory scale was not measured at baseline and it is not completely clear whether the figures reported pertain to data collected at 6 weeks or 4-months (most likely at 4-months)
short-term follow-up data only so it is not clear whether any benefits are sustained over time
Comments
clients of the child health service reported greater satisfaction with service than the comparison group
Authors’ conclusions This form of early home-based intervention targeted to vulnerable families promotes an environment conducive for infant mental and general health and hence long-term psychological and physical well-being, and is valued by the families who receive it.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
14
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Armstrong et al. (2000) Australia Continued
Exclusion criteria None stated. No significant baseline differences between intervention and control groups were reported.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
15
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Caughy et al. (2004) USA
Interventions Healthy Steps (Pediatric office visits plus home visits). Control Usual care
Eligible families were identified and enrolled either at the hospital following the birth of their child or at the pediatric practice following the birth of their child A total of 758 families enrolled in the National Evaluation at the two selected sites. Of these 658 Healthy Steps, n=337 Control, n=321 Were selected to participate in the direct observation study. Inclusion criteria
child born within the study duration
must speak English or Spanish fluently
planning to live in the same area and use same paediatric care for next 6 months or more
Exclusion criteria
their child was to be put up for adoption or placed in foster care
their child was too ill to make an office visit within the first 28 days of life
if the child died if the study child no longer
lived with the biological mother
if the family withdrew from the study, moved out of the study range (more than 1 hour car travel)
if the child never made a visit to the paediatric practice
Randomised controlled trial with cross sectional and longitudinal analysis. Experimental group versus control. Observational data were collected at two time points Time 1 (T1,16-18 months) and Time 2 (T2, 34-37 months). Attrition A total of 378 of the eligible families (57%) completed at least first part of home observation. At time 2, 604 families were eligible and of these 233 (39%) completed at least part of the second home observation. Assessment and outcome measures The Teaching Scale Score of the Nursing Child Assessment by Satellite Training (NCAST) The Parent/Caregiver Involvement Scale (P/CIS) Home Observation for Measurement of the Environment, Infant/Toddlers (HOME) The Attachment Q-Sort Child Behavior Checklist/2-3 (CBCL)Toddler Behavior Assessment Questionnaire (TBAQ)
Results indicated that mothers participating in Healthy Steps were more likely to interact sensitively and appropriately than mothers in the comparison group at the second assessment point (age 34-37 months) but not at the first assessment point (age 16-18 months). There were no differences in child outcomes at either time point when the cross sectional data were analysed. The results of the longitudinal analysis that included families who participated in the home observations at both time 1 and time 2 indicated that Healthy Steps participation was associated with greater security of attachment and fewer child behavior problems Mean treatment differences (n=179) were adjusted by maternal age, race, maternal education, insurance status during pregnancy, and marital status. Post-hoc comparisons indicated mothers in Healthy Steps group had significantly higher NCAST total scores, F(1132)=4.70, p<.05, ES=0.18 and children who participated in Healthy Steps were more securely attached to their mothers, F(1126)=6.91,p<.01, ES=0.23. The maternal behaviors in which differences between treatment and comparison group were found indicated that mothers participating in Healthy Steps were more likely to interact sensitively and appropriately than mothers in the comparison group in that they were more likely to match their interaction to the needs of the child. Differences in maternal sensitivity were observed both in a structured teaching task as well as during free play activity.
Limitations of fifteen participating sites six utilised a randomized design
and nine featured a quasi-experimental design high rates of attrition in the sample with only 179 mothers of
the original 658 (27%) completing both home observations effect sizes (ES) were relatively small program was less intensive than many other intervention
programs in that fewer office and home visits were provided and center-base care not included as part of the program
low risk sample so results may not generalize to at-risk families Comments
this analysis presents observational data from two of the sites that used a randomized treatment design
Healthy Steps is a package of services comprising enhanced well child visits, home visits, telephone support for developmental and behavioural concerns, child development and family health check-ups, written informational materials for parents (including a child health and development record), parent groups, and links to community resources (9 paediatric office visits plus 6 home visits)
data collected for the study came from a structured interview with the mother and direct observation of mother and child
program effects start to emerge and become evident at later time points which is consistent from a developmental perspective
Authors’ conclusions Findings indicate that child development services can be offered through pediatric (primary care) practices. Services delivered in this way can lead to positive changes in mothers’ interactions with their young children and are associated with greater security of attachment and fewer behavioral problems in children in families characterized as low risk.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
16
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Caughy et al. (2004) USA Continued
There were no significant differences between intervention and control groups who completed both observations assessed at time 1. At time 2, treatment families were more likely to have used health insurance to pay for pregnancy and delivery.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
17
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
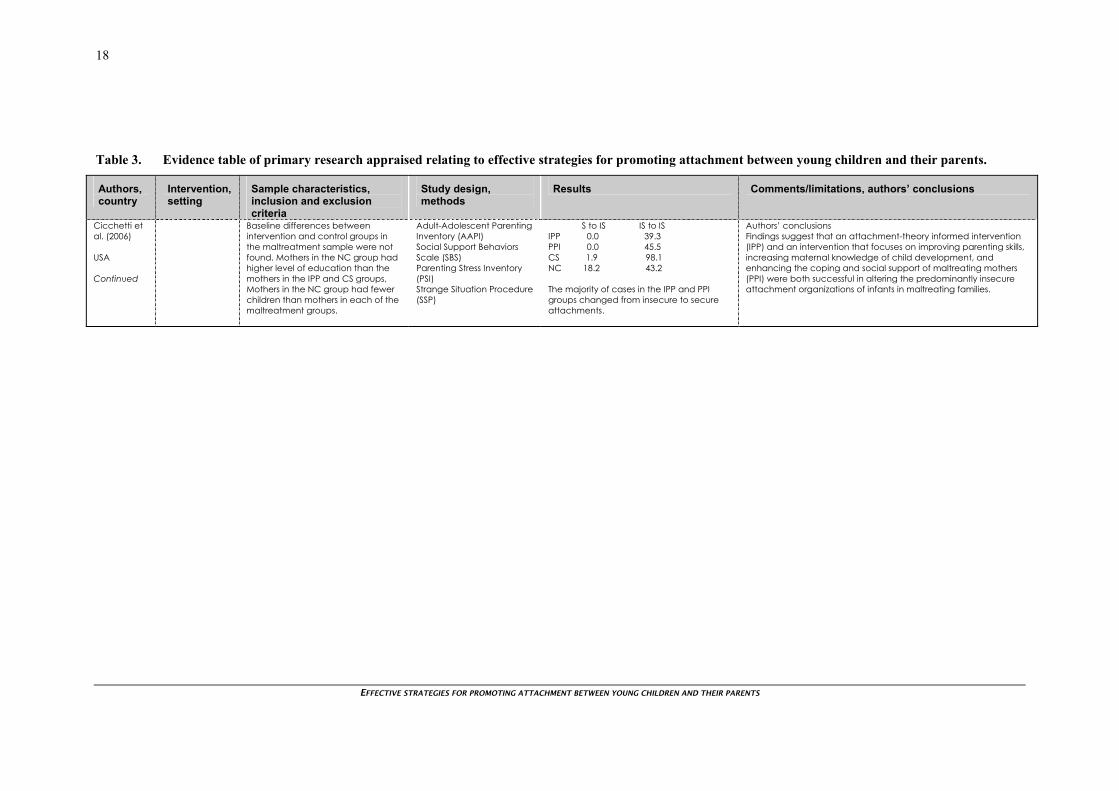
Cicchetti et al. (2006) USA
Intervention Infant parent psychotherapy (IPP) Psychoeducational parenting intervention (PPI) Control/s Community Standard (CS) Normative Comparison (NC) (from non-maltreating families)
Infants in maltreating families and their mothers were recruited for a study of the effects of child maltreatment on infant development and for an evaluation study of the efficacy of two preventive interventions designed to optimize mother-infant relationships and improve parenting. Maltreated, n=137 infants (60 boys, 77 girls) and their mothers. Nonmaltreated, n=52 IPP, n=53 PPI, n=49 CS, n=35 NC, n=52 During initial assessment Infant age (SD) = 13.31 (0.81) months Mothers mean age (SD) = 26.8 (5.88) years 74% were of minority race/ethnicity Inclusion criteria
all infants known to have been maltreated and/or who were living in maltreating families with their biological mothers
Exclusion criteria
infants who had been placed in foster care who had limited contact with their mothers
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline, during the course of the intervention and at a one-year follow-up (when the infants were approximately 26 months old). Attrition 41 families (21.7%) did not complete post-intervention assessments. Assessment and outcome measures Child Trauma Questionnaire (CTQ) Perceptions of Adult Attachment Scale (PAAS) Maternal Behaviour Q-Set (MBQ)
Follow-up contrasts indicated that no significant differences existed among the IPP, PPI and CS groups in their respective distributions of attachment classifications but each maltreatment group differed significantly from the NC group. Post intervention, all mother-child dyads were reassessed in the Strange Situation and significant differences were found that showed the pattern of differences had changed, indicating substantial intervention effects. Strange Situation attachment post intervention (%) Avoidant Secure IPP 7.1 60.7 PPI 0.0 54.5 CS 18.5 1.9 NC 13.6 38.6 Resistant Disorganised IPP 0.0 32.1 PPI 0.0 45.5 CS 1.9 77.8 NC 4.5 43.2 Pre-post intervention change pattern between secure (S) and insecure (IS) attachment S to S IS to S IPP 3.6 57.1 PPI 0.0 54.5 CS 0.0 1.9 NC 20.5 18.2
Limitations cases randomly assigned to IPP and PPI did not always
comply with the assignment, declining to be involved in the interventions. As a result those who completed the interventions are partially self-selected
changes were not found for the constructs hypothesized to serve as potential mediators of intervention efficacy
the extent to which some mothers did not engage in interventions, despite active outreach efforts indicating that additional strategies are necessary to facilitate active participation
the rates of refusal are problematic for intent-to-treat analyses because lack of participation could overwhelm treatment effects
Comments
intent-to-treat analyses examined the group composition irrespective of whether mothers actually participated. These indicated that even with cases declining intervention included in the IPP and PPI groups treatment effects were nonetheless found.
during baseline both home and center-based sessions were conducted with mothers and infants
IPP assumes that difficulties in the parent-infant relationship do not result from deficits in parenting knowledge alone but that the problems that maltreating mothers have in relating sensitively and responsively to their infants stem from insecure representational models evolved in response to the mother’s own experiences in childhood. In IPP the intervention target is not the mother or the infant but the relationship between the two
PPI model is based on the work of Olds et al. involving nurse home visitation. Supplemental cognitive and behavioural techniques were introduced to address parenting skill deficits and social-ecological factors
both interventions were manualized with central components. Therapists participated in weekly group and individual supervision. Fidelity checks were performed throughout the course of the intervention.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
18
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Cicchetti et al. (2006) USA Continued
Baseline differences between intervention and control groups in the maltreatment sample were not found. Mothers in the NC group had higher level of education than the mothers in the IPP and CS groups, Mothers in the NC group had fewer children than mothers in each of the maltreatment groups.
Adult-Adolescent Parenting Inventory (AAPI) Social Support Behaviors Scale (SBS) Parenting Stress Inventory (PSI) Strange Situation Procedure (SSP)
S to IS IS to IS IPP 0.0 39.3 PPI 0.0 45.5 CS 1.9 98.1 NC 18.2 43.2 The majority of cases in the IPP and PPI groups changed from insecure to secure attachments.
Authors’ conclusions Findings suggest that an attachment-theory informed intervention (IPP) and an intervention that focuses on improving parenting skills, increasing maternal knowledge of child development, and enhancing the coping and social support of maltreating mothers (PPI) were both successful in altering the predominantly insecure attachment organizations of infants in maltreating families.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
19
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
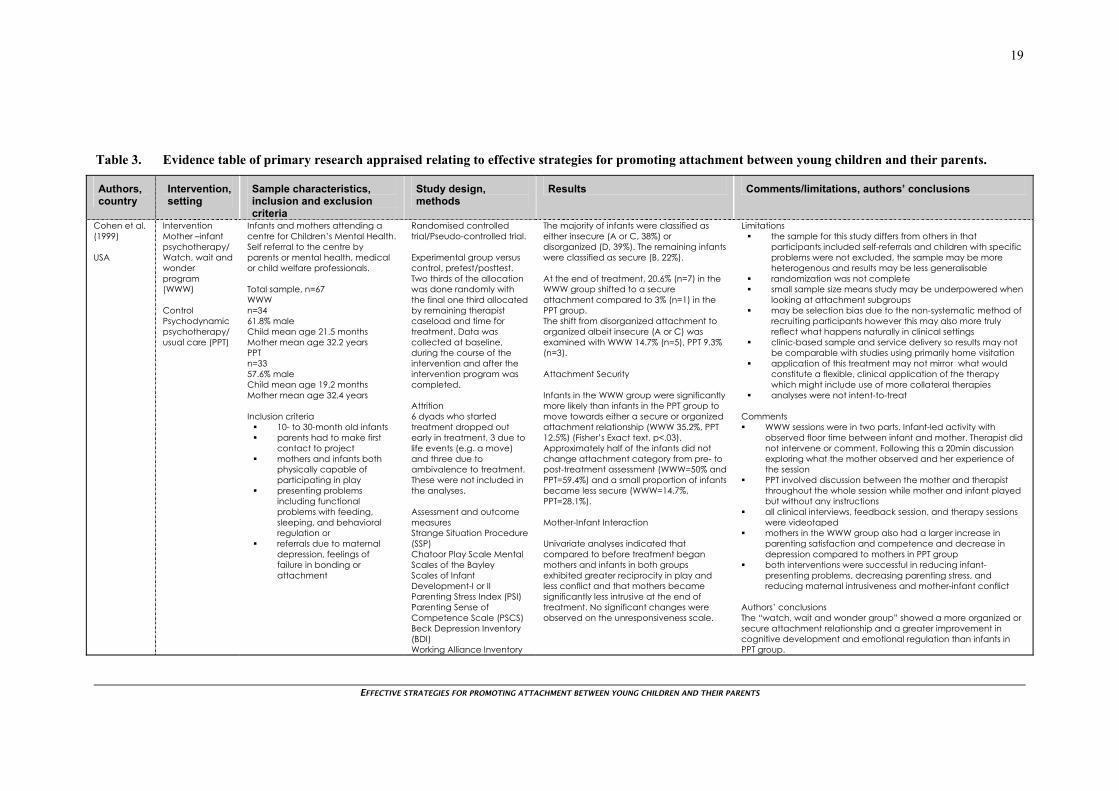
Cohen et al. (1999) USA
Intervention Mother –infant psychotherapy/ Watch, wait and wonder program (WWW) Control Psychodynamic psychotherapy/ usual care (PPT)
Infants and mothers attending a centre for Children’s Mental Health. Self referral to the centre by parents or mental health, medical or child welfare professionals. Total sample, n=67 WWW n=34 61.8% male Child mean age 21.5 months Mother mean age 32.2 years PPT n=33 57.6% male Child mean age 19.2 months Mother mean age 32.4 years Inclusion criteria
10- to 30-month old infants parents had to make first
contact to project mothers and infants both
physically capable of participating in play
presenting problems including functional problems with feeding, sleeping, and behavioral regulation or
referrals due to maternal depression, feelings of failure in bonding or attachment
Randomised controlled trial/Pseudo-controlled trial. Experimental group versus control, pretest/posttest. Two thirds of the allocation was done randomly with the final one third allocated by remaining therapist caseload and time for treatment. Data was collected at baseline, during the course of the intervention and after the intervention program was completed. Attrition 6 dyads who started treatment dropped out early in treatment, 3 due to life events (e.g. a move) and three due to ambivalence to treatment. These were not included in the analyses. Assessment and outcome measures Strange Situation Procedure (SSP) Chatoor Play Scale Mental Scales of the Bayley Scales of Infant Development-I or II Parenting Stress Index (PSI) Parenting Sense of Competence Scale (PSCS) Beck Depression Inventory (BDI) Working Alliance Inventory
The majority of infants were classified as either insecure (A or C, 38%) or disorganized (D, 39%). The remaining infants were classified as secure (B, 22%). At the end of treatment, 20.6% (n=7) in the WWW group shifted to a secure attachment compared to 3% (n=1) in the PPT group. The shift from disorganized attachment to organized albeit insecure (A or C) was examined with WWW 14.7% (n=5), PPT 9.3% (n=3). Attachment Security Infants in the WWW group were significantly more likely than infants in the PPT group to move towards either a secure or organized attachment relationship (WWW 35.2%, PPT 12.5%) (Fisher’s Exact text, p<.03). Approximately half of the infants did not change attachment category from pre- to post-treatment assessment (WWW=50% and PPT=59.4%) and a small proportion of infants became less secure (WWW=14.7%, PPT=28.1%). Mother-Infant Interaction Univariate analyses indicated that compared to before treatment began mothers and infants in both groups exhibited greater reciprocity in play and less conflict and that mothers became significantly less intrusive at the end of treatment. No significant changes were observed on the unresponsiveness scale.
Limitations the sample for this study differs from others in that
participants included self-referrals and children with specific problems were not excluded, the sample may be more heterogenous and results may be less generalisable
randomization was not complete small sample size means study may be underpowered when
looking at attachment subgroups may be selection bias due to the non-systematic method of
recruiting participants however this may also more truly reflect what happens naturally in clinical settings
clinic-based sample and service delivery so results may not be comparable with studies using primarily home visitation
application of this treatment may not mirror what would constitute a flexible, clinical application of the therapy which might include use of more collateral therapies
analyses were not intent-to-treat Comments WWW sessions were in two parts. Infant-led activity with
observed floor time between infant and mother. Therapist did not intervene or comment. Following this a 20min discussion exploring what the mother observed and her experience of the session
PPT involved discussion between the mother and therapist throughout the whole session while mother and infant played but without any instructions
all clinical interviews, feedback session, and therapy sessions were videotaped
mothers in the WWW group also had a larger increase in parenting satisfaction and competence and decrease in depression compared to mothers in PPT group
both interventions were successful in reducing infant-presenting problems, decreasing parenting stress, and reducing maternal intrusiveness and mother-infant conflict
Authors’ conclusions The “watch, wait and wonder group” showed a more organized or secure attachment relationship and a greater improvement in cognitive development and emotional regulation than infants in PPT group.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
20
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Cohen et al. (1999) USA Continued
Exclusion criteria None stated. There were no significant baseline differences between intervention and control groups on pre-assessment measures, demographics, presenting symptoms or the distribution of attachment categories.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
21
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Constantino et al. (2001) USA
Intervention Socioemotional development education programme Cohort 1 Families already involved in home visitation (Parents as Teachers) Cohort 2 Families not previously enrolled in home visitation Control No education programme.
Participant families were recruited from the waiting rooms of health clinics (pediatrics, family practice, and obstetrics and gynecology). Once enrolled families were randomized into intervention or control groups (3:2 ratio for Cohort 1 and 2:1 ratio for Cohort 2). Cohort 1 Recruited, n=190 Enrolled, n=95 Mean age (SD) mother, 26.1 (7.2) years Mean age (SD) infant, 8.3 (5.7) months Intervention (completed), n=51 (24) Control (completed), n= 34 (21) Cohort 2 Recruited, n=164 Enrolled , n=63 Mean age (SD) mother, 26.3 (6.6) years Mean age (SD) infant, 9.3 (6.0) months Intervention (completed), n=42 (28) Control (completed), n= 21 (18) Inclusion criteria
women with 3 to 18 month infants
resident in St Louis (with zip code of 63104 or 63118).
Exclusion criteria not willing to participate in
programme that would be allocated by “lottery”
Baseline differences between intervention and control groups were not reported.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data was collected at baseline and at a 6-month follow-up. Attrition Cohort 1 n=27 (53%) intervention n=13 (38%) control Cohort 1 n=14 (33%) intervention n=3 (14%) control Assessment and outcome measures IFEEL Pictures (standardized set of 30 pictures of infants with ambiguous facial expression) Adult Play Scale Child Behavior Checklist
Cohort 1 (Home visitation) Parents in intervention group made greater gains in the number of categories of emotion for which the number of IFEEL picture cards attributed fell with 1 SD from population mean (p=.08). This suggests an increase in the appropriateness of their emotional cues communicated by infants’ facial expression. None of the specific changes reached statistical significance. Cohort 2 (No previous home visitation) Six months following the intervention period, 14 mothers in the intervention group were enrolled and actively participating in a home visitation program. There was a trend for improvement in parents’ ability to interpret infant’s emotional cues but no clear evidence that the group intervention itself positively influences children’s development independent of the increase in participation in home visitation.
Limitations in both cohorts, those with higher levels of education and
income were more likely to complete the study high attrition rates were a significant problem in all aspects of the intervention including recruitment, enrolment, treatment and follow-up. These rates were inversely associated with parental income and level of income
the magnitude of attrition may have compromised the ability of the study to detect an effect
Comments the geographical areas represented by specific zip codes
represent an ethnically heterogenous stressed, disadvantaged urban population with elevated rates of child abuse and neglect and crime
completed study was deemed to be the number of subjects who completed at least 7 intervention sessions and the 6 month follow-up research assessment (for intervention group) and the number of subjects who completed the 6 month follow-up research assessment (for the control group)
analyses for Cohort 1 were controlled for maternal education level and infant age at follow-up
the intervention was a 10-session curriculum (completed over 10 weeks for Cohort 1 and 20 weeks for Cohort 2. It sought to provide parents with practical experience of interactive play and provide support for young adults in their role as parents. Structured 40min sessions were run with infants present. Sessions included free play, brief review of topic, mentored practice of play techniques and group discussion
availability of a registry for enrolment in the statutory home visitation program allowed participation or nonparticipation in home visitation to be ascertained for every participant
Authors’ conclusions Group meetings designed to promote parents’ practical understanding of children’s earliest social relationships may be an effective means of engaging hard-to-reach families in home visitation.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
22
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Fraser et al. (2000) Australia
Intervention Home visitor program Control Usual care comparison (see comments section for further detail)
Intervention, n=90 Comparison, n=91 Women in the immediate postnatal period were selected on the basis of two criteria sets listed below. Inclusion criteria
they had at least one live born infant
were literate and able to complete questionnaires in English with some assistance
planned to reside in Brisbane’s northern suburbs
respondent reporting one or more of the following four risk factors
sole parenthood ambivalence to pregnancy
(sought termination, no antenatal care)
physical forms of domestic violence
child abuse of either parent respondents reporting three
or more of the following risk factors:
maternal age < 18 years instable housing (three or
more moves in 2 years, homelessness)
financial stress (often concerned about enough food or making ends meet)
<10 years of maternal education
low family income (<A$16000 per annum)
social isolation history of mental health
disorder (either parent)
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline and post intervention at a 12-months and an 18-month follow-up. Attrition Between recruitment to the trial and 12-month follow-up over three-quarters (76.24%) of the sample was retained. Of the home visiting group (75.5%) compared to the comparison group (76.9%). Retained to 12-months Intervention, n=68 Comparison, n=70 Assessment and outcome measures Edinburgh Postnatal Depression Scale (EPDS) Home Observation for Measurement of the Environment (HOME) Child Abuse Potential Inventory Parenting Stress Inventory
Maternal interactions, stimulation and home safety standards were observed and measured in participating family homes where natural behavior between parent and infant could be observed. In this study, inter-rater reliability of the HOME Inventory was checked by having two research assistants visit 23% of the homes at the same time at 12 months. Each made an independent assessment. A correlation between observers of 0.79 for assessing emotional and verbal responsivity to infant was obtained.
Maternal-infant interactions were more likely to be positive, with significantly higher (better) scores in aspects of the home environment related to optimal development in children, particularly maternal-infant attachment in the intervention group.
Parent attachment in intervention group, mean (SD)
Primiparas Multiparae Baseline 14.00 (3.23) 12.96 (3.47) 6-week 12.45 (3.71) 12.00 (3.40) 12-month 12.14 (3.68) 11.96 (2.88)
Parent attachment in comparison
group, mean (SD)
Primiparas Multiparae Baseline 14.35 (3.39) 13.66 (4.02) 6-week 13.20 (3.65) 13.64 (3.84) 12-month 11.50 (2.95) 13.33 (4.08) There was a significant main effect for time for parent-infant attachment (p<.05) but no statistically significant group effect for this subscale.
Limitations limited evaluation of infant attachment status (Strange
Situation Procedure) as an outcome although this may be addressed if subsequent follow-ups are conducted when the infants are older
teenage mothers and mothers with insecure housing were more likely to withdraw from the study in first 12-months
short-term outcomes reported and longer follow-up may be required to program (“sleeper”) effects that present much later.
Comments
this article had more of an emphasis on prevention of child abuse and neglect but attachment outcome was reported
the home visiting programme was designed to establish a relationship of trust between the professional home visitors and the family; to promote maternal-infant attachment; to improve parental adoption of health promoting behaviours; promote positive parenting practices; reduce parental stress and improve maternal mood; reduce child abuse potential, and promote the use of community and neighbourhood support systems to assist families
families allocated to comparison received information about community child health services as part of routine discharge planning at the recruiting hospital. Standard community child health care services involve the choice of one home visit by the local child health nurse with more extensive home visiting provided to those with specific problems.
Authors’ conclusions The evaluation did not demonstrate a sustained positive impact on the quality of the home environment which included measures of parent-child interaction.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
23
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Fraser et al. (2000) Australia Continued
alcohol or drug abuse domestic violence other than
physical abuse Exclusion criteria None stated. Baseline differences between intervention and control groups were rigorously assessed and adjusted for where appropriate.
The schedule of visiting included weekly visits until the infant was 6 weeks old, fortnightly visits until 3 months, then monthly visits until the age of 12 months. The minimum number of nurse-visits per family was 18.
No overall intervention effect was demonstrated at 12 or 18-month follow-up with no significant differences between intervention and comparison groups.
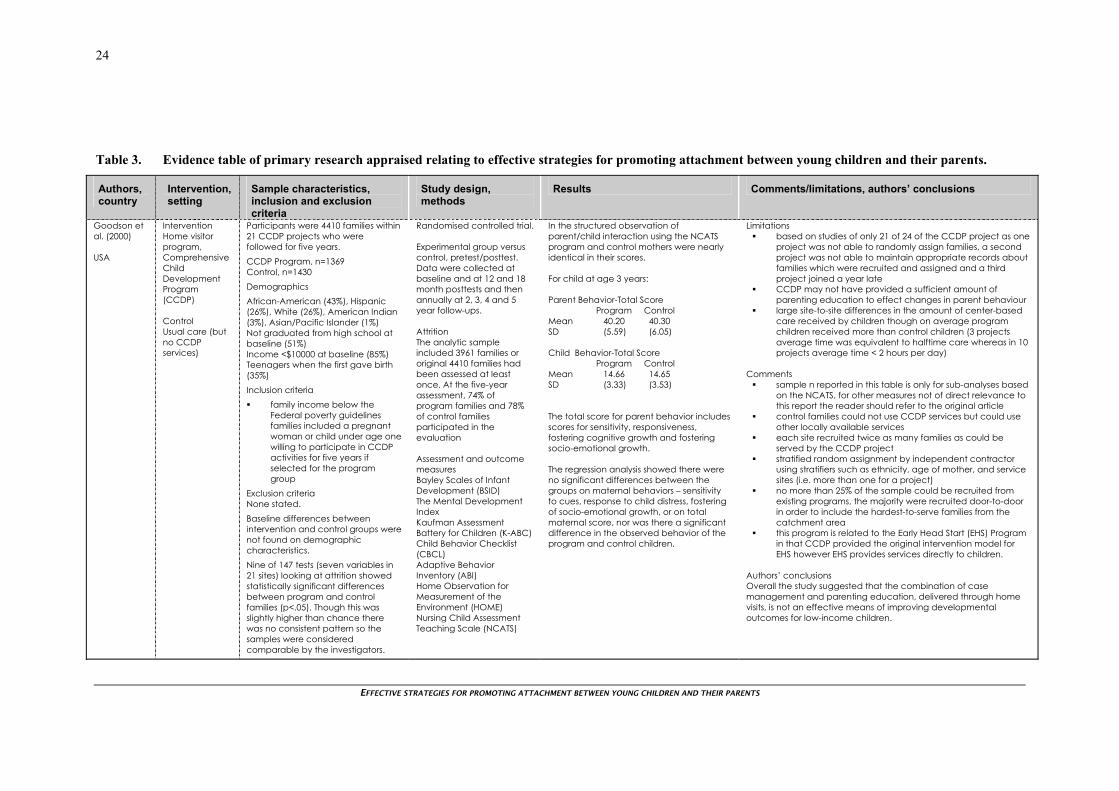
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
24
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Goodson et al. (2000) USA
Intervention Home visitor program, Comprehensive Child Development Program (CCDP) Control Usual care (but no CCDP services)
Participants were 4410 families within 21 CCDP projects who were followed for five years. CCDP Program, n=1369 Control, n=1430 Demographics African-American (43%), Hispanic (26%), White (26%), American Indian (3%), Asian/Pacific Islander (1%) Not graduated from high school at baseline (51%) Income <$10000 at baseline (85%) Teenagers when the first gave birth (35%) Inclusion criteria family income below the
Federal poverty guidelines families included a pregnant woman or child under age one willing to participate in CCDP activities for five years if selected for the program group
Exclusion criteria None stated. Baseline differences between intervention and control groups were not found on demographic characteristics. Nine of 147 tests (seven variables in 21 sites) looking at attrition showed statistically significant differences between program and control families (p<.05). Though this was slightly higher than chance there was no consistent pattern so the samples were considered comparable by the investigators.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline and at 12 and 18 month posttests and then annually at 2, 3, 4 and 5 year follow-ups. Attrition The analytic sample included 3961 families or original 4410 families had been assessed at least once. At the five-year assessment, 74% of program families and 78% of control families participated in the evaluation Assessment and outcome measures Bayley Scales of Infant Development (BSID) The Mental Development Index Kaufman Assessment Battery for Children (K-ABC) Child Behavior Checklist (CBCL) Adaptive Behavior Inventory (ABI) Home Observation for Measurement of the Environment (HOME) Nursing Child Assessment Teaching Scale (NCATS)
In the structured observation of parent/child interaction using the NCATS program and control mothers were nearly identical in their scores. For child at age 3 years: Parent Behavior-Total Score Program Control Mean 40.20 40.30 SD (5.59) (6.05) Child Behavior-Total Score Program Control Mean 14.66 14.65 SD (3.33) (3.53) The total score for parent behavior includes scores for sensitivity, responsiveness, fostering cognitive growth and fostering socio-emotional growth. The regression analysis showed there were no significant differences between the groups on maternal behaviors – sensitivity to cues, response to child distress, fostering of socio-emotional growth, or on total maternal score, nor was there a significant difference in the observed behavior of the program and control children.
Limitations based on studies of only 21 of 24 of the CCDP project as one
project was not able to randomly assign families, a second project was not able to maintain appropriate records about families which were recruited and assigned and a third project joined a year late
CCDP may not have provided a sufficient amount of parenting education to effect changes in parent behaviour
large site-to-site differences in the amount of center-based care received by children though on average program children received more than control children (3 projects average time was equivalent to halftime care whereas in 10 projects average time < 2 hours per day)
Comments
sample n reported in this table is only for sub-analyses based on the NCATS, for other measures not of direct relevance to this report the reader should refer to the original article
control families could not use CCDP services but could use other locally available services
each site recruited twice as many families as could be served by the CCDP project
stratified random assignment by independent contractor using stratifiers such as ethnicity, age of mother, and service sites (i.e. more than one for a project)
no more than 25% of the sample could be recruited from existing programs, the majority were recruited door-to-door in order to include the hardest-to-serve families from the catchment area
this program is related to the Early Head Start (EHS) Program in that CCDP provided the original intervention model for EHS however EHS provides services directly to children.
Authors’ conclusions Overall the study suggested that the combination of case management and parenting education, delivered through home visits, is not an effective means of improving developmental outcomes for low-income children.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
25
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Heinicke et al. (1999, 2000 and 2001) USA
Intervention Home visiting, relationship based program (UCLA Family Development Project) Control Pediatric follow-up
All families receiving prenatal care at the UCLA Ob/Gyn and pediatric clinics. In total 70 families were recruited to the study. Home-visited (HV), n=31 (52% girls) Pediatric follow-up (PF), n=33 (48% girls) Mean age mother (bothgroups) = 24 years Inclusion criteria
having first child live within a 20-min drive of
the hospital families who had four or more
risk factors from social interview
mother is poor and receiving aid
mother lacks support (partner, family, friends)
pregnancy not wanted mother victim of childhood
physical or sexual or emotional abuse
mother victim of childhood rape or violence
mother experienced suicidal thoughts in the past
mother referred for mental/health counselling in the past
mother treated for drug and/or alcohol addiction in the past, and
mother homeless
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline and at 12- and 24- month follow-ups. Attrition at 12-month follow-up 4/70 intervention families and 2/70 non-intervention families Assessment and outcome measures Wechsler Adult Intelligence Scale Maternal Support Interview Beck Depression Inventory Cutrona Support Inventory Spielberger Anxiety Inventory Locke-Wallace Marital Inventory Parent-Child and Child Global Ratings Caldwell HOME Scales Bayley Scales of Infant Development/Bayley Scale Test Situation Attachment Q-set Strange Situation Procedure (SSP)
Mother responsiveness and child security of attachment were assessed at 6, 12 and 24 months. Impact of intervention on mother responsiveness to need and indices of child security (mean value shown on a seven point rating scale) other responsive to need 6Mos 12Mos 24Mos HV 4.29 5.22 5.29 PF 4.90 4.30 4.00 Effect size -.42 .97 1.63 p-value .03 .0003 .0001 Mother affectionate response to reunion 6Mos 12Mos 24Mos HV 3.45 3.90 3.81 PF 3.57 3.45 2.88 Effect size -.11 .47 1.00 p-value .65 .07 .0003 Mother positive affect 6Mos 12Mos 24Mos HV 4.32 4.90 4.87 PF 4.64 4.30 4.18 Effect size -.19 .54 .58 p-value .30 .03 .02 Secure response to separation 6Mos 12Mos 24Mos HV 5.10 6.32 6.10 PF 6.06 4.61 4.21 Effect size -.61 1.30 1.31 p-value .02 .0001 .0001
Limitations on the basis of trends seen at 12 months it was anticipated
that intervention families would show further differential gains in adaptation however this was not realized
may lack generalisability due to the detailed inclusion and exclusion criteria
inadequate resources prevented completion of the three and 4-year follow-up
Comments
this table combines results from three articles, two of which reported outcomes after the first and second year of life
three socio-emotional transactions were focused on as key outcomes (1) parental responsiveness to the needs of her infant as related to the development of his or her security of attachment; (2) parental encouragement of infant autonomy and (3) parental encouragement of her child’s task involvement as related to the development of her task orientation. This evidence table focuses on (1).
the primary goal of the intervention is to offer the mother experience of a stable trustworthy relationship that conveys understanding of the situation, and that promotes her sense of self efficacy through specific interventions
specific intervention included enhancing the mothers communication and personal adaptation, providing alternative approaches for relating to her child, direct affirmation and support
Authors’ conclusions Findings suggest that the intervention made a significant impact on three critical socio-emotional mother-infant transactions in the first year of life. Children receiving the intervention were more secure and their mothers more responsive to their needs in the first and second year of life.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
26
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Heinicke et al. (1999, 2000 and 2001) USA Continued
Exclusion criteria any DSM-IV Axis I diagnosis currently using drugs do not speak English any member of the family
suffering from serious health complications
No statistically significant differences in demographic characteristics including IQ between intervention and control groups were reported at baseline.
Child positive affect 6Mos 12Mos 24Mos HV 3.77 4.58 4.87 PF 3.91 4.33 3.91 Effect size -.11 .21 .74 p-value .66 .41 .004 For standard deviations (SD) refer to original article.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
27
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Letourneau et al. (2001a and 2001b) USA
Study 1 Interventions Keys to Caregiving program Control Home visits with nurse social support
Two studies were conducted on two different interventions both with a focus on parent and infant interactive behavior. Study 1 is reported here. Study 1 n=15 (time 1), n=16 (time 2) Mothers mean age=18 years (SD=1) 50% partners Inclusion criteria
adolescent parents at risk due to low income,
educational attainment and single parent status
Exclusion criteria None stated. Baseline differences between intervention and control groups were not found for any of the demographic or descriptive variables examined, including gestational age, birth weight, educational level, age, partner status, ethnicity, socioeconomic status, depression or life stress. No significant differences could be found between those who completed and those who dropped out though only limited data were available.
Randomised controlled trial. Experimental group versus control, two posttests only. Interactive behavior was assessed at the baseline pretest and 6 months posttest. Data were collected and mother-child interactions videotaped posttest only, at 7 to 9 (time 1) weeks and at follow-up, 11 to 13 (time 2) weeks old. Attrition Study 1 Of 24 mothers recruited 18 completed two follow-ups (75%), only 13 of 24 completed all of the intervention and outcome measurement. Assessment and outcome measures Nursing Child Assessment Feeding (NCAFS) and Teaching Scales (NCATS) Preschool-Parent Interactive Behavior (PPIB) Coding System
Feeding Scale Effects Parent time 1 time 2 Sensitivity to cues 1.07 0.87 Response to distress 0.86 0.61 Socioemotional growth 1.09 1.08 Cognitive Growth 0.86 1.19 Infant Clarity of cues 0.38 - Responsiveness 0.69 - Teaching Scale Effects Parent time 1 time 2 Sensitivity to cues 1.02 0.47 Response to distress 0.66 0.45 Socioemotional growth 0.88 0.32 Cognitive Growth 0.35 1.03 Infant Clarity of cues - 1.24 Responsiveness 0.21 0.63 Larger effect sizes greater than 0.8 are noted for 11 of 16 comparisons in the subscales relating to parental behavior change suggesting mean change scores approaching 1 standard deviation were achieved for most subscale measures. Anovas were computed by using those participants who completed all measures of NCAFS and NCATS. For NCAFS, there was a significant main effect (p=.028) and for NCATS on the total score (p=.027) and parent subscale (p=.036).Further tests were conducted that are not reported here. Group differences were observed in the overall quality of the interaction, the parents’ contributions to the interaction, and the proportion of contingently responsive parent-infant interactions.
Limitations pilot study (study 1), very small sample size problematic for
statistical analysis however effect size calculation were presented, a separate article presents some analyses
support processes were not documented as per intervention Comments
the Keys to Caregiving program delivered via six home visits introduces five key concepts 1) infant states, 2) infant behaviour, 3) infant cues, 4) how to modulate states, and 5) interacting during feeding
social support for the control group included informational resources, affirmation or reinforcement of parents perspectives or behaviours, and listening and responding to parents (emotional support)
a second trial was reported in the same article however this is not reported here as to qualify for inclusion children had to have exhibited a 6-month developmental delay in two or more areas
mean intrarater reliability of 95% for the feeding scale and 94% for the teaching scale were achieved
intervention integrity was monitored through regular debriefing sessions, field not taking, and selected audio recordings of intervention sessions
Authors’ conclusions Results suggested that parent-child relationships were enhanced.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
28
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Klein and Rye. (2004) Israel
Intervention Mediational Intervention for Sensitising Caregivers/More Intelligent and Sensitive Children (MISC) Control Home visits from community workers who focused on basic health and nutrition issues with a general focus on child development
Families with infants and very young children living in two of the poorest communities in Addis Ababa, Ethiopia participated in the study. 49 out of 893 families from Kebele 18 and 47 of 1997 families from Kebele 15 were randomly selected for the intervention and comparison groups respectively. MISC, n= 49 Control, n=47 Inclusion criteria
children aged from 1 to 3 years
resident in the Kechene community (Kebelle 15 and Kebele 18)
Exclusion criteria None stated. Baseline differences between groups not reported.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline (6 months) and within 3 months of termination of the programme at 12-month and 6- year follow-ups. Attrition Of the 96 children who were initially selected as participants 84 (87.5%, 42 from each group) participated in the 6-year follow-up. Assessment and outcome measures The Rutter Scale of Emotional and Social Development Observing Mediational Interaction (semi-structured questionnaire for parents) The MacArthur Communicative Development Inventory
The effects of the intervention on the participating mothers and their children were assessed and findings were consistent with stable effects of the intervention over time. A clear improvement in the quality of mother-child interactions was noted following the MISC intervention. These findings persisted over time and were noted in the 6-year follow-up study. The change in the interactive behavior of the intervention group mothers and their children was clearly apparent in comparison to their own behavior prior to the intervention as well as in comparison to the behavior of mothers in the comparison group. A clear increase in frequency of parental mediation was found and included interaction initiated by mothers and by children. The latter was rare at outset and remained rare in comparison group. Mothers and children initiated more eye contact as well as physical contact, responded more fully to each other’s communicative signals and had more and longer shared attention episodes. The emotional climate of the parent-child interactions became more positive in the intervention group, with high frequencies of positive affect and turn taking in the intervention group and nearly none in the comparison group.
Limitations study conducted in a very specific population so may not
be generalisable to other populations statistical analyses although performed were not explicitly
reported but are reported elsewhere in a unpublished doctoral dissertation and a book chapter2
Comments
the intervention with the families was carried out by 21 paraprofessionals, selected from the site of the project as well as from neighbouring communities, all of them were already employed by the community as health and social workers and other positions
this community was among the poorest and most congested urban slum areas in the city with little or no sanitation and extreme poverty
training materials were adapted for use in Ethiopia in a pilot study constructed a year prior to the current intervention study
home-based and institution-based intervention however this article focuses on the home-based intervention (5 individual meetings of 1-1.5hours and 5 group meetings of 2-3 hours)
parent-child interactions were videotaped and analyzed this program has been evaluated cross culturally in other
settings Authors’ conclusions One year following the intervention, mothers in the intervention group were more sensitive, more responsive, and optimistic about their potential to affect their child’s development than were mothers in the comparison group. Six years later significant changes were still noted in the quality of the adult-child interactions and developmental measures of the children.
2 Melese, F. (2001) Early psychosocial intervention in Ethiopia [Doctoral Dissertation]. Norway: University of Bergen; Melese, F. (2001) The More Intelligent and Sensitive Child (MISC). In P.S. Klein (Ed.), Seeds of hope: Twelve years of early intervention in Africa (pp. 131-158). Oslo: University of Oslo, Unipub, Forlag. Neither of these were retrieved for the current Technical Brief.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
29
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Klein and Rye. (2004) Israel
Although no statistically significant intervention effects were found for childrens’ socioemotional development, there was a consistent trend showing that more children in the intervention group reached developmentally higher landmarks of socioemotional development compared to others.
Findings confirmed that the intervention resulted in an increase in age-appropriate, sensitive and affective interactions had a positive effect on childrens’ cognitive and socioemotional development.
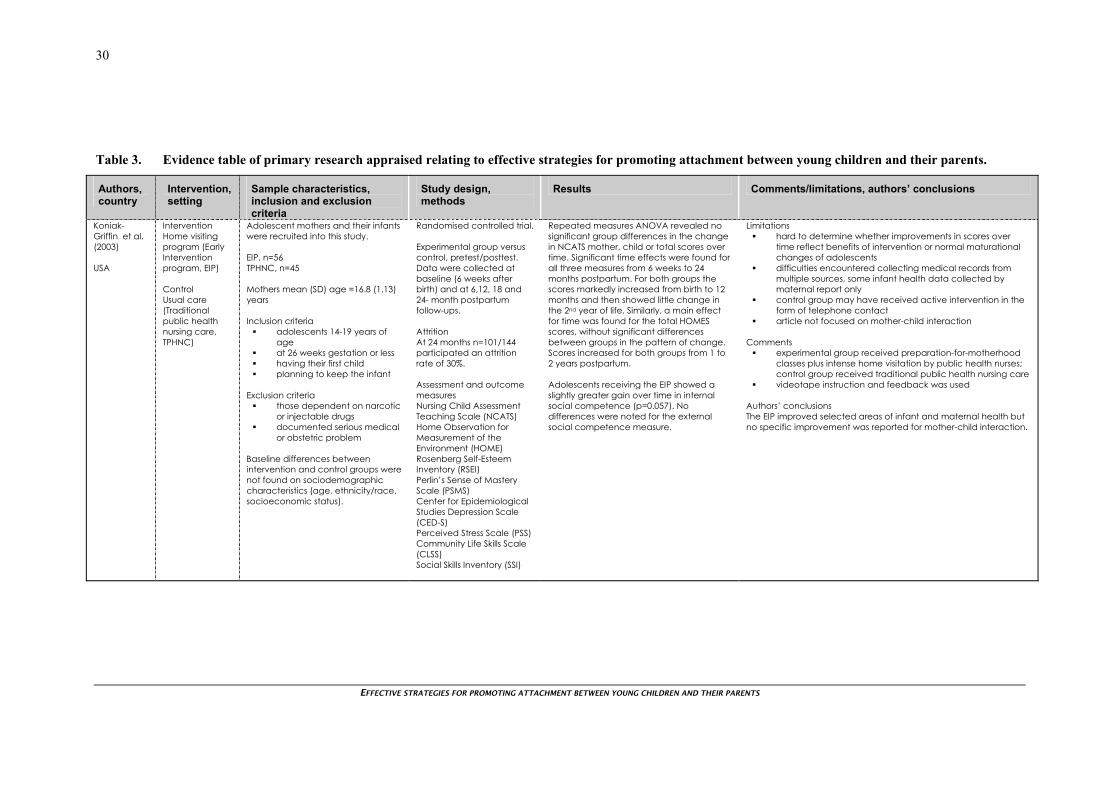
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
30
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Koniak-Griffin et al. (2003) USA
Intervention Home visiting program (Early Intervention program, EIP) Control Usual care (Traditional public health nursing care, TPHNC)
Adolescent mothers and their infants were recruited into this study. EIP, n=56 TPHNC, n=45 Mothers mean (SD) age =16.8 (1.13) years Inclusion criteria
adolescents 14-19 years of age
at 26 weeks gestation or less having their first child planning to keep the infant
Exclusion criteria
those dependent on narcotic or injectable drugs
documented serious medical or obstetric problem
Baseline differences between intervention and control groups were not found on sociodemographic characteristics (age, ethnicity/race, socioeconomic status).
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline (6 weeks after birth) and at 6,12, 18 and 24- month postpartum follow-ups. Attrition At 24 months n=101/144 participated an attrition rate of 30%. Assessment and outcome measures Nursing Child Assessment Teaching Scale (NCATS) Home Observation for Measurement of the Environment (HOME) Rosenberg Self-Esteem Inventory (RSEI) Perlin’s Sense of Mastery Scale (PSMS) Center for Epidemiological Studies Depression Scale (CED-S) Perceived Stress Scale (PSS) Community Life Skills Scale (CLSS) Social Skills Inventory (SSI)
Repeated measures ANOVA revealed no significant group differences in the change in NCATS mother, child or total scores over time. Significant time effects were found for all three measures from 6 weeks to 24 months postpartum. For both groups the scores markedly increased from birth to 12 months and then showed little change in the 2nd year of life. Similarly, a main effect for time was found for the total HOMES scores, without significant differences between groups in the pattern of change. Scores increased for both groups from 1 to 2 years postpartum. Adolescents receiving the EIP showed a slightly greater gain over time in internal social competence (p=0.057). No differences were noted for the external social competence measure.
Limitations hard to determine whether improvements in scores over
time reflect benefits of intervention or normal maturational changes of adolescents
difficulties encountered collecting medical records from multiple sources, some infant health data collected by maternal report only
control group may have received active intervention in the form of telephone contact
article not focused on mother-child interaction Comments
experimental group received preparation-for-motherhood classes plus intense home visitation by public health nurses; control group received traditional public health nursing care
videotape instruction and feedback was used Authors’ conclusions The EIP improved selected areas of infant and maternal health but no specific improvement was reported for mother-child interaction.
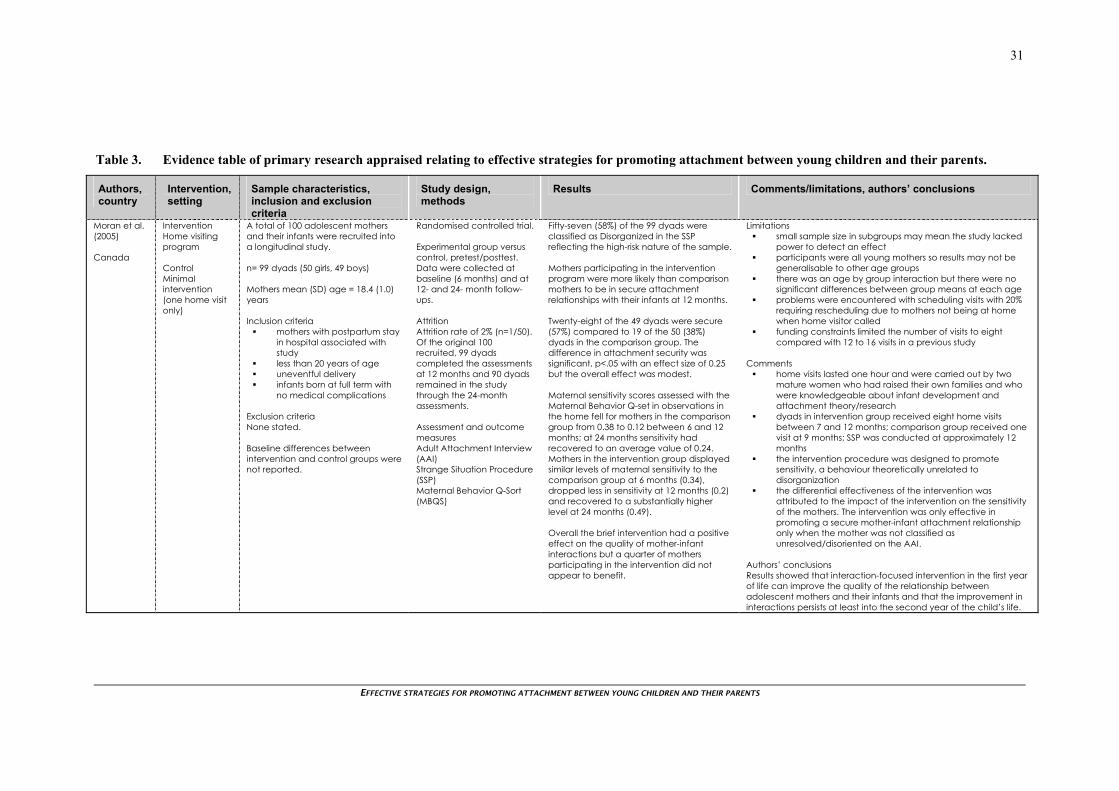
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
31
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Moran et al. (2005) Canada
Intervention Home visiting program Control Minimal intervention (one home visit only)
A total of 100 adolescent mothers and their infants were recruited into a longitudinal study. n= 99 dyads (50 girls, 49 boys) Mothers mean (SD) age = 18.4 (1.0) years Inclusion criteria
mothers with postpartum stay in hospital associated with study
less than 20 years of age uneventful delivery infants born at full term with
no medical complications Exclusion criteria None stated. Baseline differences between intervention and control groups were not reported.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data were collected at baseline (6 months) and at 12- and 24- month follow-ups. Attrition Attrition rate of 2% (n=1/50). Of the original 100 recruited, 99 dyads completed the assessments at 12 months and 90 dyads remained in the study through the 24-month assessments. Assessment and outcome measures Adult Attachment Interview (AAI) Strange Situation Procedure (SSP) Maternal Behavior Q-Sort (MBQS)
Fifty-seven (58%) of the 99 dyads were classified as Disorganized in the SSP reflecting the high-risk nature of the sample. Mothers participating in the intervention program were more likely than comparison mothers to be in secure attachment relationships with their infants at 12 months. Twenty-eight of the 49 dyads were secure (57%) compared to 19 of the 50 (38%) dyads in the comparison group. The difference in attachment security was significant, p<.05 with an effect size of 0.25 but the overall effect was modest. Maternal sensitivity scores assessed with the Maternal Behavior Q-set in observations in the home fell for mothers in the comparison group from 0.38 to 0.12 between 6 and 12 months; at 24 months sensitivity had recovered to an average value of 0.24. Mothers in the intervention group displayed similar levels of maternal sensitivity to the comparison group at 6 months (0.34), dropped less in sensitivity at 12 months (0.2) and recovered to a substantially higher level at 24 months (0.49). Overall the brief intervention had a positive effect on the quality of mother-infant interactions but a quarter of mothers participating in the intervention did not appear to benefit.
Limitations small sample size in subgroups may mean the study lacked
power to detect an effect participants were all young mothers so results may not be
generalisable to other age groups there was an age by group interaction but there were no
significant differences between group means at each age problems were encountered with scheduling visits with 20%
requiring rescheduling due to mothers not being at home when home visitor called
funding constraints limited the number of visits to eight compared with 12 to 16 visits in a previous study
Comments
home visits lasted one hour and were carried out by two mature women who had raised their own families and who were knowledgeable about infant development and attachment theory/research
dyads in intervention group received eight home visits between 7 and 12 months; comparison group received one visit at 9 months; SSP was conducted at approximately 12 months
the intervention procedure was designed to promote sensitivity, a behaviour theoretically unrelated to disorganization
the differential effectiveness of the intervention was attributed to the impact of the intervention on the sensitivity of the mothers. The intervention was only effective in promoting a secure mother-infant attachment relationship only when the mother was not classified as unresolved/disoriented on the AAI.
Authors’ conclusions Results showed that interaction-focused intervention in the first year of life can improve the quality of the relationship between adolescent mothers and their infants and that the improvement in interactions persists at least into the second year of the child’s life.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
32
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Murray et al. (2003) UK
Interventions Non-directive counselling Cognitive Behavioural Therapy Psychodynamic Therapy Control Routine primary care
A community sample of 206 women with major depressive disorder was identified. Of these 193 were randomly assigned to one of three intervention groups or routine care. Inclusion criteria
primiparous living within a 15-mile radius
of the maternity hospital women with post-partum
depression (Edinburgh Postnatal Depression Scale)
English as first language Exclusion criteria
women who had delivered prematurely (before 36 weeks gestation)
if their infant had any gross congenital abnormality
if they had not had a singleton birth
if they were intending to move out of the area within the period of the intervention
Baseline differences between intervention and control groups were not found for background demographic factors and negative orientation to motherhood. More women in the control group had experienced high levels of adversity (35%) and fewer women in the psychodynamic therapy group (10%).
Randomised controlled trial.
Experimental groups versus control, pretest/posttest. Data were collected at baseline, immediately after treatment (4.5 months postpartum) and at 18-months and 5-year postpartum.
Therapy was conducted in the women’s own homes on a weekly basis from 8 to 18 weeks post-partum. Mother-infant interaction was videotaped before and after treatment and independently rated.
Attrition Of the eligible participants 83% (n=171) completed therapy. Nineteen dropped out of treatment early or moved away from the study area. Of those successfully assigned 10% did not complete the trial.
Assessment and outcome measures Strange Situation Procedure (SSP) Behavioural Screening Questionnaire Mental Development Index of the Bayley Scales of Infant Development Rutter A2 Scale Preschool Behaviour Checklist
Maternal sensitivity at 2 and 4.5 months postpartum The three treatments were found to be comparable with the control condition after level of maternal sensitivity at 2 months was controlled for. For women with low levels of social adversity those in the control condition had higher levels of sensitivity than women in the CBT or PT groups. No significant difference was found between the control condition and non-directive counselling. For women with high social adversity, women who received non-directive counselling were found to have higher levels of maternal sensitivity than women in the control condition. There were no treatment effects for CBT or PT. Maternal sensitivity at18 months postpartum Compared with the control group, after controlling for social adversity and the significant effect of maternal age, the effect of treatment was significant for non-directive counselling (p=.001), with PT (p=.03) and CBT (p=.06) showing some improvement compared to control. Infant attachment The rates of secure (B) and insecure (A, C and D) attachment were similar for all four groups and no significant differences were found between the treated groups and the control condition.
Limitations the sample was one that was generally low risk, and
comprised of first time mothers so the generalisability to high-risk and multiparous populations is unknown
the sample was underpowered to detect differences between the treatment groups
although the efficacy of the interventions has been demonstrated for some outcomes, effectiveness studies are required to establish whether such benefits would be obtained in routine practice
indications of a positive benefit were limited despite symptomatic improvement underlying maternal
vulnerabilities persisted and to prevent longer-term difficulties in child functioning more prolonged interventions may be required.
Comments
routine care involved normal care provided by the primary health team (GP plus health visitors) with no input from research team
cognitive-behavioural therapy (CBT) with a focus on problems identified by mother in management of her infant
psychodynamic therapy promoting an understanding of the mothers representation of her infant and her relationship with her infant by exploring aspects of the mothers own early attachment history
non-directive counselling where women were given the opportunity to air their feelings about current concerns
Authors’ conclusions Findings indicated that the treatments had no significant impact on security of infant-mother attachment but in mothers who experience social adversity, whose interactions with their infants were particularly poor, non-directive counselling produced a more sensitive pattern of mother-infant interaction.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
33
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Olds et al. (2002) USA
Intervention Nurse home visitation. Paraprofessional home visits. Control.
A total of 1178 consecutive women from 21 antepartum clinics were invited to participate (Denver). Of these, 735 were randomized. Nurse home visits, n= 235 Paraprofessional home visits, n=245 Control, n=255 Nurses (paraprofessionals) home visit average was 6.5 (6.3) during pregnancy/21 (16) visits from birth to 2nd birthday. Ethnicity Caucasian 35-37% Hispanic (Mexican American) 44-46% African American 16-17%. Inclusion criteria
no previous live births qualified for Medicaid or had
no private health insurance enroll any time prior to
delivery informed consent.
Exclusion criteria none stated. The treatment groups were similar at baseline.
Randomised controlled trial. Experimental groups versus control, assessment at baseline with follow-ups at 6, 12, 15, 21 and 24 months. Attrition for interviews 6 mths 17.7% 12 mths 16.7% 15 mths 23.8% 21 mths 12.7% 24 mths 14.3% Rates of attrition were slightly higher for the child assessments. Assessment and outcome measures: Mental Development Inventory, Mother-reported behavior problems Mother-infant interaction (NCAST) Home Observation for Measurement of the Environment (HOME)
Data were modeled statistically using treatments (3 levels), maternal psychological resources (high vs low) and the interaction between these classifications. In addition a number of covariates were included in model. Addition of the covariates did not alter the model greatly. Nurse-visited mother-child pairs interacted with each other more responsively than those in the control group (p=0.05). At 6 months, nurse-visited infants were less likely to exhibit emotional vulnerability to fear stimuli and nurse-visited infants born to women with low psychological resources were less likely to exhibit low emotional vitality in response to joy and anger stimuli. At 21 months nurse-visited children were less likely to exhibit language delays and at 24 months exhibited superior mental development. There were no program effects on women’s use of prenatal services, educational achievement or children’s temperament or behavior problems.
Limitations absence of statistical significance probably due to limited
statistical power to detect small effects higher rates of refusal among women who smoked may limit
generalisability to smokers and probably users of other substances
higher study attrition among the nurse-visited women women visited by nurses and paraprofessionals may have
altered their interview responses and behaviour during the observations to coincide with what they thought was expected of them
given the large number of dependent variables, some findings may be spurious
several of the outcome measures are not independent of one another.
Comments
no specific measures of attachment status were reported mother-infant interaction was videotaped either in the
laboratory or home at all postpartum assessments using 2 validated procedures
infants home environments were rated at 12 and 21 months more of a difference was noted between groups with the
subsample of women classed as having low psychological resources
Authors’ conclusions When trained in a model program of prenatal and infancy home visiting, paraprofessionals produced small effects that rarely achieved statistical or clinical significance. Nurses produced significant effects on a wide range of maternal and child outcomes including more responsive mother-infant than those visited by non-nurses.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
34
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Toth et al. (2006) USA
Interventions Toddler-Parent Psychotherapy (DI) Control groups Depressed mothers (DC) Nondepressed mothers (NC)
A total of 202 mothers with a history of major depression were recruited. Of these 130 were eligible and were randomly assigned to one of two intervention groups. A group of 89 mothers were recruited for the NC, of which 21 were not eligible. DI, n=66 DC, n=64 NC, n=68 Inclusion criteria
mothers with and without a history of major depressive disorder since the child’s birth
child aged approximately 20 months
mother met DSM-III-R criteria for major depression
Exclusion criteria
low socioeconomic status determined by reliance on public assistance
parents without high school education
diagnosis of bipolar disorder other prior or current
psychiatric disorder (for second control group only)
Baseline differences in pre-intervention attachment classification were found between intervention and control groups, based on Strange Situation Procedure (p<0.001).
Randomised controlled trial. Experimental groups versus control, pretest/posttest. Data were collected at baseline (on average child aged 20 months), and at the 16-month (on average child aged 36 months) follow-up. Attrition Of the original sample of 198, DI, n=20 (30%); DC, n=10 (15.6%); and C, n=5 (7%) did not complete the post-intervention assessments. However no significant differences due to completion status were found for baseline maternal scores, demographic characteristics and a range of other variables. Therefore no specific evidence of selection bias in the retained sample was found. Assessment and outcome measures The Diagnostic Interview Schedule (DIS-III-R) Beck Depression Inventory (BDI) Strange Situation Procedure (SSP)
The pattern of secure versus insecure classification at post-intervention shifted in agreement with the predicted effect of the intervention. The overall distributions of post-intervention attachment differed significantly (p<.001). The pattern of the groups had also changed markedly. Maternal depression was found to be related to insecure attachment. Prior to the initiation of the intervention, offspring in the DI and DC groups both had higher rates of attachment in security than the NC group. The same was true of disorganized attachment. Following completion of the TPP intervention, offspring in the DI group showed increased attachment security compared with offspring in both the DC and NC groups. Thus offspring with depressed mothers who had participated in TPP actually had more secure attachment relationships than did offspring of well mothers. In intervention effect size for difference in proportions between DI and DC group was 1.084, indicating a large treatment effect associated with the intervention. Furthermore there was a greater degree of change from insecure to secure attachment in the DI group relative to the DC group with a large effect size of 1.11. For further detail see the original article which lists a variety of comparisons.
Limitations a significant amount of attrition occurred during the study,
though this was a largely self-referred sample and that motivation to participate was not enhanced or encouraged by any external service providers
because only one intervention was provided it is not possible to demonstrate whether the improvement in outcomes was specific to an attachment-theory informed mode of intervention
sample was predominantly low risk (married, well educated, financially comfortable) so results may not be generalisable to high risk populations, therapists could focus on mother-child relationship rather than issues associated with poverty, substance abuse and domestic violence
efficacy trial where co-occurring risk factors were minimized rather than effectiveness (real world) study, possible that participants received a “purer” dose of attachment-focused intervention and this could account for the positive results
Comments
mothers in the DI and DC groups were not restricted from being involved in other mental health treatment during the course of the study and 75% (DI) and 67% (DC) respectively were engage in some form of intervention
although this is a research trial some of the assessment sessions were conducted in the home
all therapists received extensive training and supervision, the intervention was manualized, and the fidelity of the intervention was monitored closely by videotaping and reviewing taped sessions
the efficacy of TPP in modifying disorganized attachment is consistent with findings that suggest treating parental depression is insufficient to improve parenting behaviours
the presence of fewer risk factors enabled therapists to focus on implementation of TPP in the absence of crisis situations that would require departure from the therapeutic protocol
the authors note that where populations have more extreme needs, a more multifaceted and less focused intervention may be necessary
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
35
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Toth et al. (2006) USA Continued
The groups were comparable on a range of demographic characteristics.
Authors’ conclusions Results demonstrated the efficacy of toddler-parent psychotherapy in fostering secure attachment relationships in young children of depressed mothers.
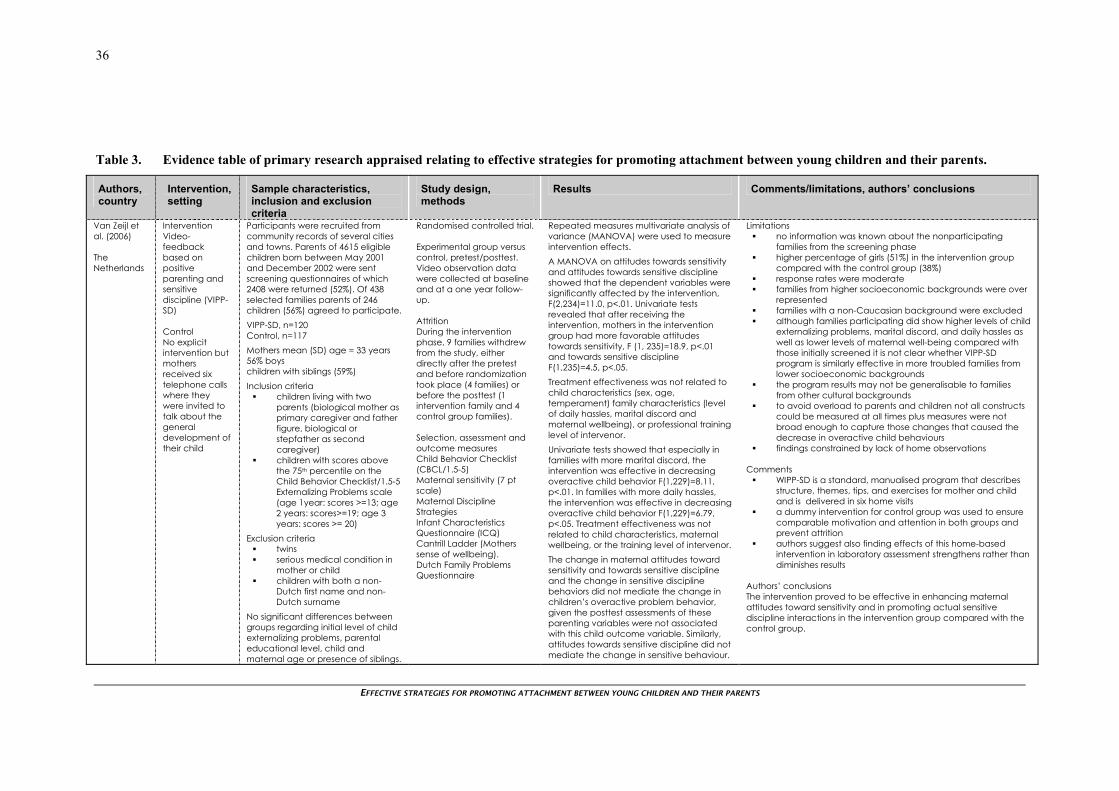
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
36
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Van Zeijl et al. (2006) The Netherlands
Intervention Video-feedback based on positive parenting and sensitive discipline (VIPP-SD) Control No explicit intervention but mothers received six telephone calls where they were invited to talk about the general development of their child
Participants were recruited from community records of several cities and towns. Parents of 4615 eligible children born between May 2001 and December 2002 were sent screening questionnaires of which 2408 were returned (52%). Of 438 selected families parents of 246 children (56%) agreed to participate. VIPP-SD, n=120 Control, n=117 Mothers mean (SD) age = 33 years 56% boys children with siblings (59%) Inclusion criteria
children living with two parents (biological mother as primary caregiver and father figure, biological or stepfather as second caregiver)
children with scores above the 75th percentile on the Child Behavior Checklist/1.5-5 Externalizing Problems scale (age 1year: scores >=13; age 2 years: scores>=19; age 3 years: scores >= 20)
Exclusion criteria twins serious medical condition in
mother or child children with both a non-
Dutch first name and non-Dutch surname
No significant differences between groups regarding initial level of child externalizing problems, parental educational level, child and maternal age or presence of siblings.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Video observation data were collected at baseline and at a one year follow-up. Attrition During the intervention phase, 9 families withdrew from the study, either directly after the pretest and before randomization took place (4 families) or before the posttest (1 intervention family and 4 control group families). Selection, assessment and outcome measures Child Behavior Checklist (CBCL/1.5-5) Maternal sensitivity (7 pt scale) Maternal Discipline Strategies Infant Characteristics Questionnaire (ICQ) Cantrill Ladder (Mothers sense of wellbeing). Dutch Family Problems Questionnaire
Repeated measures multivariate analysis of variance (MANOVA) were used to measure intervention effects. A MANOVA on attitudes towards sensitivity and attitudes towards sensitive discipline showed that the dependent variables were significantly affected by the intervention, F(2,234)=11.0, p<.01. Univariate tests revealed that after receiving the intervention, mothers in the intervention group had more favorable attitudes towards sensitivity, F (1, 235)=18.9, p<.01 and towards sensitive discipline F(1,235)=4.5, p<.05. Treatment effectiveness was not related to child characteristics (sex, age, temperament) family characteristics (level of daily hassles, marital discord and maternal wellbeing), or professional training level of intervenor. Univariate tests showed that especially in families with more marital discord, the intervention was effective in decreasing overactive child behavior F(1,229)=8.11, p<.01. In families with more daily hassles, the intervention was effective in decreasing overactive child behavior F(1,229)=6.79, p<.05. Treatment effectiveness was not related to child characteristics, maternal wellbeing, or the training level of intervenor. The change in maternal attitudes toward sensitivity and towards sensitive discipline and the change in sensitive discipline behaviors did not mediate the change in children’s overactive problem behavior, given the posttest assessments of these parenting variables were not associated with this child outcome variable. Similarly, attitudes towards sensitive discipline did not mediate the change in sensitive behaviour.
Limitations no information was known about the nonparticipating
families from the screening phase higher percentage of girls (51%) in the intervention group
compared with the control group (38%) response rates were moderate families from higher socioeconomic backgrounds were over
represented families with a non-Caucasian background were excluded although families participating did show higher levels of child
externalizing problems, marital discord, and daily hassles as well as lower levels of maternal well-being compared with those initially screened it is not clear whether VIPP-SD program is similarly effective in more troubled families from lower socioeconomic backgrounds
the program results may not be generalisable to families from other cultural backgrounds
to avoid overload to parents and children not all constructs could be measured at all times plus measures were not broad enough to capture those changes that caused the decrease in overactive child behaviours
findings constrained by lack of home observations Comments
WIPP-SD is a standard, manualised program that describes structure, themes, tips, and exercises for mother and child and is delivered in six home visits
a dummy intervention for control group was used to ensure comparable motivation and attention in both groups and prevent attrition
authors suggest also finding effects of this home-based intervention in laboratory assessment strengthens rather than diminishes results
Authors’ conclusions The intervention proved to be effective in enhancing maternal attitudes toward sensitivity and in promoting actual sensitive discipline interactions in the intervention group compared with the control group.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
37
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Velderman et al. (2006a and 2006b) The Netherlands
Intervention Video-feedback and brochures (VIPP) Video-feedback, brochures and discussion (VIPP-R) Control No explicit intervention
Mothers with first-born children were identified by town hall records and child health center records. Selected mothers (n=311) were invited to participate in an interview about their childhood as part of a study on the influence of their own childhood on child development. Of these 262 AAIs were administered (16% attrition). From this 84 mothers tentatively classified as insecure were included in the study. VIPP, n=28 VIPP-R, n=26 Control, n=27 Mothers mean (SD) age = 27.7 (3.6) years Mean educational level 2.51 (0.96) Inclusion criteria
mothers with more than 8 but less than 14 years of formal education
Exclusion criteria None stated. Control groups were on average two years older than intervention mothers (p<.01) but did not differ on educational level or on intelligence. No significant differences in sensitivity between the intervention and control mothers were found at pretest.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Video observation data were collected at baseline and at a 6-month follow-up. Attrition Of 84 mothers, 81 participated in all activities (3.6% attrition). Selection, assessment and outcome measures Adult Attachment Interview (AAI) Strange Situation Procedure (SSP) Infant Behavior Questionnaire (IBQ) The AAI was used as a selection instrument and mothers were selected on the basis of their insecure attachment representation. Home visitors made video observations of mother-infant dyads to assess sensitive responsiveness during free play. A further four home visits were scheduled with a posttest video observation assessment of sensitivity made by research assistant unknown to the mother.
At posttest, intervention mothers were significantly more sensitive than control mothers (p<0.05, d=0.49). Univariate ANOVA with pretest as the covariate showed that sensitivity of intervention mothers increased significantly more than control mothers’ sensitivity (p<0.05, d=0.46). Mothers’ posttest sensitivity in both intervention groups was significantly higher than in the control group (for the VIPP group p<0.05, d=0.46 and for the VIPP-R group p<0.05, d=0.52) and the effectiveness of the two types of interventions did not differ. The intervention was less effective in changing children’s attachment security. Although 67% of the intervention groups developed a secure attachment to their mothers, the same was true of 56% of the infants in our control group (p=0.17, d=0.22). The number of secure infants in both intervention groups was not significantly higher than in the control group. The effectiveness of the two different interventions did not differ. The infants of mothers who showed more increase in sensitivity were more securely attached (using continuous security scores). Mothers of highly reactive infants profited more from the intervention than others. At posttest, sensitivity in the highly reactive intervention group differed significantly from sensitivity in the highly reactive control group (p<0.01, d=2.27). There was no difference between the less reactive groups.
Limitations small sample size may be underpowered even a brief home-based intervention such as this requires
significant resources and effort to implement a larger sample might have resulted in a significant
interaction effect instead of a trend for intervention effects on attachment security for highly versus less reactive infants
the use of the IBQ may be less robust than observational assessment of negative reactivity
there may be a ceiling effect due to the selection of mothers on the basis of the AAI from audiotape as this may not have led to a sample of 100% insecure mothers, in a completely insecure sample the possibility of improvement in maternal sensitivity and infant attachment security would be higher
the approach of assigning classifications to AAI from tape instead of transcript needs to be validated.
Comments
WIPP focused on enhancing mothers’ sensitive responsiveness by providing them with video feedback about their own (in-sensitive) behaviours
VIPP-R aimed to enhance sensitivity and restructure mothers’ attachment representation (representational level)
discussions in VIPP-R were of mothers’ childhood attachment experiences in relation to their current caregiving
educational level scale ranged from 1 to 4, with 1 = primary school or junior secondary vocational education and 4 = senior secondary general education followed by senior secondary vocational education
the authors suggest the findings are important for mental health providers planning and implementing intervention or prevention programs in that is seems promising and possibly cost effective to implement brief interventions with a clear focus that may have an effect.
Authors’ conclusions Post-intervention, both groups of intervention mothers were found to be more sensitive than control mothers. The two interventions were equally effective at enhancing maternal sensitivity but failed to produce a significant effect on infant attachment security.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
38
Table 3. Evidence table of primary research appraised relating to effective strategies for promoting attachment between young children and their parents.
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Velderman et al. (2006a and 2006b) The Netherlands Continued
Finally, mothers were invited to the Child and Family Studies Center to participate in the SSP.
This differential intervention effect cannot be ascribed to differences in pretest sensitivity between mothers of highly reactive infants and mothers of less reactive infants (p=0.99).
The interventions were most effective for highly reactive children and their mothers, providing support for theories suggesting that there may be differential susceptibility to rearing influences.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
39
OVERVIEW
Emotional and behavioural problems in infancy are mostly viewed as relational so there is general agreement that the intervention focus for infants should be on improving the quality of parent-infant relationships. Within this context most studies are guided by the theoretical framework of attachment to delineate goals and components of specific interventions (Cohen et al. 1999). Hence this report summarises the evidence from studies seeking to promote attachment between young children and their parents. For pragmatic reasons (primarily timeframe) this report was limited to studies conducted in the last eight years only.
Overall quality of evidence
Of the 27 eligible articles identified, two systematic reviews were appraised (see Table 2, pages 7-10) and 18 separate primary studies were appraised from a total of 24 articles (see Table 3, pages 11-38). An additional trial focusing on an eligible form of attachment intervention was originally appraised but subsequently excluded due to its focus on adoptive children (see Appendix 3b).
Summary of evidence for the effectiveness of interventions promoting attachment between young children and their parents
Secondary studies
Two secondary studies (see Table 2, pages 7-10) met selection criteria and are summarised below.
Bakermans-Kranenburg et al. (2005) published a systematic review that examined intervention studies designed to prevent disorganised attachment. Ten studies with 15 preventive interventions (n=842) were found that included infant disorganised attachment as an outcome measure. The effectiveness of these interventions ranged from negative to positive, with a non-significant overall effect size (d = 0.05). A meta-analysis showed that disorganised attachment may respond to sensitivity-focused interventions but the authors’ suggest that interventions that specifically focus on the prevention of disorganisation may also be warranted.
An earlier systematic review by the same principal author provides what is the most comprehensive summary of the relevant literature in this field to date. Bakermans-Kranenburg et al. (2003) identified seventy relevant studies including 88 interventions effects on sensitivity (n=7636) and /or attachment (n=1503). Not all of the studies considered used true experimental designs to test intervention effectiveness so to estimate the combined effect size, a smaller group of studies consisting of only the intervention studies with randomised control group design were selected.
A core set of 51 randomised controlled trials was established (6282 mothers with their children) and a meta- analysis of these studies was done. Randomised interventions appeared rather effective in changing insensitive parenting (d=0.33) and infant attachment insecurity (d=0.20). The results suggested that interventions with a clear focus and a modest number of sessions may be preferable. Furthermore interventions with an exclusively behavioural focus on improving maternal sensitivity appear to be the most effective not only in enhancing maternal sensitivity but also in promoting children’s attachment security.
Primary studies
Eighteen independent randomised controlled trials were reported from a total of 24 articles. All of these studies had either a focus on promoting attachment or maternal sensitivity or responsiveness, as either a primary or a secondary outcome and included studies that satisfied pre-determined selection criteria. These studies are summarised briefly on the following pages and further detail is provided in Evidence Tables (see Table 3, pages 11-38) and in an overall summary table (see Table 4, page 41).
In the following sections studies have been grouped either by their risk status or by some other common identifying feature of the population of interest.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
40
Mothers with or at risk of depression
Maternal depression is believed to have an adverse impact on the mother-child attachment relationship but empirical findings are equivocal. A significant but modest association has been confirmed (Martins and Gaffan 2000) especially when depression is severe or protracted. In some studies maternal depression has not been associated with insecure attachment, and in all studies it is clear that a substantial number of mothers with depression are able to provide a sensitive caretaking environment for their children (McMahon et al. 2006). Three intervention studies were found that specifically targeted mothers with or at risk of depression in one of the experimental groups.
A study by Ammaniti (2006) focused on three groups of participants, those at risk of depression (high or low risk) and an additional group of low risk women who had fewer psychosocial risk factors. The comparison group received only scheduled visits for data collection. The intervention group women all participated in a home visiting programme theoretically based on attachment theory that was designed specifically to promote child development, improve parenting practices, and facilitate positive parent-child relationships. The intervention was effective at 6 and 12 months post-intervention, as sensitive maternal behaviours toward their child in the combined group of mothers receiving the intervention increased significantly.
Murray et al. (2003) recruited mothers with post-partum depression into a treatment study that compared the effectiveness of non-directive counselling with cognitive behavioural therapy, psychodynamic therapy and routine primary care. Sensitivity and attachment were both primary outcomes in this study. Findings indicated that the treatments had no significant impact on security of infant-mother attachment but in mothers who experience social adversity, whose interactions with their infants were particularly poor, non-directive counselling produced a more sensitive pattern of mother-infant interaction.
Mothers with and without a history of major depressive disorder since their child’s birth were offered Toddler-Parent Psychotherapy, a manualised intervention based on attachment theory (Toth et al. 2006). Two control groups, one of depressed mothers, the other of non-depressed mothers received usual care. In many regards this was an efficacy trial, in that co-occurring risk factors were deliberately minimised in the sample and the intervention was not delivered in the home. The authors suggest that their results demonstrate the efficacy of toddler-parent psychotherapy in fostering secure attachment relationships in young children of depressed mothers but qualify this by stating that it is yet to be ascertained whether the same magnitude of effect (i.e. large) would be found in more heterogenous samples or where a lesser amount of therapy was received.
Adolescent mothers
Several researchers have targeted adolescent mothers for intervention. This is because children of adolescent mothers are at risk for a variety of developmental difficulties. Jaffee et al. (2001) found compelling evidence that negative outcomes for children of adolescent mothers are associated with both family circumstances (social influence) and maternal characteristics (social selection). They concluded that the personal characteristics of adolescent mothers contribute to adverse outcomes for their children, even when the negative social consequences of early childbirth are taken into account. Furthermore adolescent mothers have been shown to be less responsive to their infants’ signals, to use more intrusive and physical interventions, and to provide less verbal stimulation than adult mothers (Culp et al. 1991).
Three programmes were identified that sought to intervene with adolescent mothers.
The Keys to Caregiving programme was designed to promote high-quality parent-infant interaction through improving parents’ understanding on infant behaviours, cues and needs. Several articles by Letourneau and colleagues (2001a; 2001b) and Letourneau (2001) provide the results from a small pilot study of this intervention. Across multiple sample sizes, observers, data coders, testing sessions, types of analysis, and instruments, significant differences between groups were found. Interpretation of these results is limited by the small size of the sample however this study does provide tentative support for a nursing intervention programme to improve parent-infant interactions. A full trial with an adequate number of participants is required to make stronger conclusions about this particular intervention’s effectiveness.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
41
Table 4. Summary of aim, mode of delivery, settings and theoretical basis of interventions appraised in primary studies
Primary study Country
Aim and mode of service delivery Sample
Theoretical basis
Ammaniti et al. (2006), Italy
Home visiting programme to enhance the quality of mother-infant interaction.
Sample at risk of psychosocial problems or depression.
Intervention based on attachment theory.
Armstrong et al. (2000), Australia
Home visiting programme to enhance quality of maternal-infant attachment and mothers’ relationship with the child.
Multi- risk sample.
Intervention promoting optimal child development.
Caughy et al. (2004), USA
Pediatric office visits plus home visits to enhance sensitive interaction and attachment security.
Low risk sample.
Intervention promoting optimal child development.
Cicchetti et al. (2006), USA
Home and center-based sessions to optimize mother-infant relationship and parenting.
Multi-risk sample.
Based on nurse home visitation model and mothers attachment history.
Cohen et al. (1999), USA
Center-based intervention to improve attachment security and mother-infant interaction.
Heterogeneous sample, self-referrals.
Based on attachment theory.
Constantino et al. (2001), USA
Home visitation to promote infants’ social and emotional development.
Multi- risk sample.
Based on attachment theory.
Fraser et al. (2000), Australia
Home visitation to determine if home visiting improves home environment and parent-child interaction.
Multi-risk sample.
Early intervention model.
Goodson et al. (2000), USA
Home visitation to improve a wide range of developmental outcomes for children.
Multi-risk sample.
Early intervention model.
Heinicke et al. (1999, 2000 and 2001), USA
Home visitation to improve mother-infant interaction and family functioning.
Multi-risk sample.
Based on attachment theory and early intervention model.
Letourneau et al. (2001a and 2001b), USA
Home visitation to promote high-quality parent-infant interaction.
Adolescent mothers.
Based on Barnard’s model which promotes sensitivity to infant cues.
Klein and Rye. (2004), Israel/Ethiopia
Home-based visitation and institution-based to improve quality of adult-child interactions and promote learning.
Specific ethnic population, at risk.
Based on attachment theory and Feuerstein’s theory of mediated learning.
Koniak-Griffin et al. (2003), USA
Home visitation to improve social and emotional competence.
Adolescent mothers.
Based on social-learning theory.
Moran et al. (2005), Canada
Home visitation to increase the probability of a secure infant-mother attachment relationship.
Adolescent mothers.
Based on attachment theory.
Murray et al. (2003) and Cooper et al. (2003), UK
Home visitation.
To improve mother-child relationship and child outcome.
Women with post-partum depression.
Early intervention model.
Olds et al. (2002 and 2004), USA
Home visitation to improve a wide range of developmental outcomes for children, including mother-child responsivity.
Mixed sample (includes multi-risk).
Early intervention model.
Toth et al. (2006), USA
Home- and lab-based to foster improved attachment security.
Women with post-partum depression.
Based on attachment theory.
Van Zeijl et al. (2006), The Netherlands
Home-based visitation to enhance sensitive parenting.
Low-risk sample.
Based on attachment and coercion theory.
Velderman et al. (2006a and 2006b), The Netherlands
Home visits and clinic-based assessment to improve infant attachment security.
Mothers classified with insecure attachment.
Based on attachment theory.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
42
Two further studies were identified that focused primarily on intervening with adolescent mothers. Koniak-Griffin et al. (2003) implemented an early intervention programme that started with preparation for parenting classes pre-birth and incorporated intensive post-birth home visitation from nurses. Mother-child interaction was only a secondary outcome and no improvements were noted specifically for this measure.
A trial by Moran et al. (2005) compared another home visiting programme with a minimal intervention consisting of one home visit only. The latter study had a much stronger focus on attachment and mother-child interaction was a primary outcome measure. Results showed that an interaction-focused intervention in the first year of life can improve the quality of the relationship between adolescent mothers and their infants and that the improvement in interactions persists at least into the second year of the child’s life. The authors also noted that there was a sizeable subgroup (25%) for whom the intervention appeared to be of no benefit.
Mixed or multi-risk populations
Interventions that focus on mixed or multi-risk populations tend to have a broader focus, although this is not always the case. A range of studies were found that looked at either home visiting as an intervention alone or home visiting plus adjunctive education programmes with a relationship focus. Eight groups of studies (some with more than one publication3) were reported in this category.
Armstrong et al. (2000) examined two groups, families who received child health nurse home visits and families who received usual care which may have included accessing their local community child health clinic. Both the quality of maternal-infant attachment and the mothers’ relationship with the child, were significantly enhanced in the experimental group and intervention mothers showed greater emotional responsivity to their infants and more readily accepted their infants’ behaviour.
A recent trial by Cicchetti et al. (2006) compared infant parent psychotherapy (IPP), a psychoeducational parenting intervention (PPI) to a community control group and a second normative comparison group (from non-maltreating families). This study was one of only a few to directly examine the change in attachment pattern from pre intervention to post intervention and to also include a normative comparison group. Post intervention, all mother-child dyads were reassessed using the Strange Situation Procedure and significant differences were found that showed the pattern of differences had changed, indicating substantial intervention effects. The authors suggest that an attachment-theory informed intervention (IPP) and an intervention that focuses on improving parenting skills, increasing maternal knowledge of child development, and enhancing the coping and social support of maltreating mothers (PPI) were both successful in altering the predominantly insecure attachment organisations of infants in maltreating families.
Another study that also looked at mother-infant psychotherapy was conducted by Cohen and colleagues (1999). They compared two interventions, the “watch, wait and wonder programme” and psychodynamic psychotherapy. A mixed sample of mothers both self-referred and referred by health professionals were randomly assigned to receive either intervention. Both attachment security and change in attachment security status were examined along with other measures of mother-child interaction. Overall the “watch, wait and wonder group” showed more organised or secure attachment relationships and a greater improvement in cognitive development and emotional regulation than infants in the comparison group.
Constantino et al. (2001) investigated the effectiveness of an educational programme which had a socioemotional-development focus. The intervention was offered as an adjunct to home visitation to a cohort of families already receiving home visits and to another cohort of families not previously enrolled in home visits. A further group that acted as a control received no educational programme. There was no clear evidence from this study that the group education intervention delivered positively influenced children’s development independent of the increase in participation in home visitation. A trend for improvement in parental ability to interpret infant’s emotional cues was noted. The authors suggest that group meetings designed to promote parents’ practical understanding of children’s earliest
3 Where multiple publications exist, results from more than one article may have been combined in a single Evidence Table or a summary article selected for appraisal. For example, for some studies such as the Nurse Family Partnership programme (Olds and colleagues) only the most relevant publications are listed in the references.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
43
social relationships may however be an effective means of engaging hard-to-reach families in home visitation.
A home visiting programme delivered to at risk women in Australia by Fraser et al. (2000) reported on a number of secondary outcome measures related to attachment. No significant differences were reported between intervention and comparison groups for parental attachment. However maternal-infant interactions were more likely to be positive, with significantly higher (better) scores in aspects of the home environment related to optimal development in children, particularly maternal-infant attachment. Despite some changes that were noted over time in this study, no sustained, overall intervention effect was demonstrated at the 12- or 18-month follow-up.
In a similar but much larger scale, multisite study Goodson et al. (2000) compared families who received services from the Comprehensive Child Development Program (CCDP) against families who received no CCDP services but were able to access other local services. There were no significant differences between the groups on maternal behaviours including sensitivity to cues, response to child distress, fostering of socio-emotional growth, or on total maternal score, nor was there a significant difference in the observed behaviour of the programme and control children. Findings suggest that a combination of case management and parenting education, delivered through home visits, is not an effective means of improving developmental outcomes for low-income children.
A series of articles by Heinicke and colleagues (1999; 2000; 2001) reported on a relationship oriented and home visit-based programme (the UCLA Family Development Project). Children receiving the intervention were more secure and their mothers more responsive to their needs in the first and second year of life relative to a group receiving paediatric follow-up. The authors concluded that the intervention made a significant impact on several socio-emotional mother-infant transactions including parental responsiveness.
Nurse home visitation was compared to paraprofessional home visits by Olds et al. (2002 and 2004). Nurse-visited mother-child pairs interacted with each other more responsively than those in the control group (p=0.05). A very large number of outcomes were studied in this trial. At six months, nurse-visited infants were less likely to exhibit emotional vulnerability to fear stimuli and nurse-visited infants born to women classed as having low psychological resources were less likely to exhibit low emotional vitality in response to joy and anger stimuli. The authors concluded that nurses produced significant effects on a wide range of maternal and child outcomes including more responsive mother-infant interaction compared to those visited by non-nurses.
Low-risk populations
Several studies focused on low risk participants. One of the main reasons for focusing on a sample with a lower level of risk is that it is theoretically easier to deliver a more focused, intensive intervention.
An intervention that combined paediatric office with home visits (Healthy Steps) was compared to usual care by Caughy et al. (2004). Only two of the original fifteen sites (six of which used a randomised design) were examined in this report. Results suggested that mothers participating in Healthy Steps were more likely to interact sensitively and appropriately with their children than mothers in the comparison group by the second assessment point (age 34-37 months) but not at the first assessment point (age 16-18 months). From a developmental perspective this is consistent as it may reflect the fact that programme effects start to emerge and become evident at later time points. Findings indicate that child development services can be offered through paediatric (primary care) practices. What remains unclear from this study is whether the observed effect is due primarily to the home visiting or paediatric visit components of the intervention or whether it is a combined effect.
Van Zeijl et al. (2006) delivered an early intervention programme to low-risk mothers that used video-feedback and was based on a standard manualised programme. The focus of the programme was on improving sensitivity and sensitive discipline. While the control group did not receive any explicit intervention mothers in this group did receive a number of phone calls over the course of the study where they had the opportunity to talk about the general development of their child. The intervention proved to be effective in enhancing maternal attitudes toward sensitivity and sensitive discipline and in promoting sensitive discipline interactions. The change in maternal attitudes toward sensitivity and towards sensitive discipline and the change in sensitive discipline behaviours did not mediate any

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
44
changes in children’s overactive problem behaviour. Similarly, attitudes towards sensitive discipline did not mediate any change in sensitive behaviour.
Other studies
One novel trial reported by Klein and Rye (2004) was conducted in Ethiopia among families in two very poor communities. This intervention focused on improving the quality of parent-child interactions including maternal sensitivity and responsiveness. One year following the intervention, mothers in the intervention group were found to be more sensitive, more responsive, and optimistic about their potential to affect their child’s development than were mothers in the comparison group. Six years later significant changes were still noted in the quality of the adult-child interactions and developmental measures of the children. Further interpretation of the results from this article was limited by the lack of information provided on the statistical analyses4 but this study stood out as being unique in its community development approach.
Finally, an intervention study by Velderman et al. (2006a and 2006b) was aimed at breaking the intergenerational cycle of insecure attachment. Eighty-one first time mothers were randomly assigned to receive video-feedback and brochures to enhance sensitive parenting. The second intervention involved additional discussions of mothers’ childhood attachment experiences in relation to their current caregiving. By the time of the six-month follow-up, intervention mothers were found to be more sensitive than control mothers. Furthermore the interventions were most effective for the highly reactive children and their mothers.
One additional study was appraised (see Appendix 3b) that falls outside of the scope of the current review (due to the population rather than intervention considered). This trial looked at the effectiveness of a “personal book” intervention with and without sessions of home-based video feedback in adopted children (Juffer et al. 2005b). This short-term preventive intervention program lowered the rate of disorganized attachment in this specific population. The effectiveness of this intervention documents the importance of parenting in the development of infant attachment disorganization, particularly in children with a heightened risk of attachment problems. Although the results of this study may not be generalisable to children who are not adopted, the intervention approach itself could have application with non-adopted children and their parents.
Discussion
Thirteen out of the 18 eligible studies (72%) reported a statistically significant improvement on one or more outcomes of interest by the time any follow-up was completed. Of the remaining studies, three reported no effect, one study reported a trend to improvement on the primary outcome measure of interest and one additional study reported a positive effect but did not include data to verify this in the published report (see Table 5, page 45).
Overall, when all the trials are considered disregarding their methodological differences the evidence is relatively consistent, suggesting that interventions based on attachment theory and delivered to different populations, are moderately effective despite the wide range of different intervention approaches and different comparison groups used.
This body of evidence should however not be considered without due consideration to a number of methodological issues and limitations.
Methodological Issues
Attachment security is only one factor in a multi-risk model of developmental psychopathology and only one of a number of variables that contribute to parent-child relationships, it may be that attachment may serve better as an endpoint or marker of improvement over time rather than an immediate outcome (Cohen et al. 1999). Moreover, in general attachment security may also be more difficult to change than maternal insensitivity.
4 Analyses appear to have been done but have been reported elsewhere primarily in an unpublished PhD which was not able to
be retrieved.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
45
Table 5. Summary of direction of observed effect in intervention group by outcome and the statistical significance or size of the effect
Primary Study Improvement shown on outcome measure for intervention group/s†
Significance/Effect Size
Ammaniti et al. (2006)
Sensitive maternal behaviours At 12 months p<.03
Armstrong et al. (2000)
Emotional responsivity At 4 months p<.05
Caughy et al. (2004) Secure attachment Sensitive interaction
At 37 months p<.01/ES 0.23 At 37 months p<.05/ES 0.18
Cicchetti et al. (2006) Secure attachment (for IPP and PPI respectively)
At 26 months p<.001/ES 1.46 and ES 1.51
Cohen et al. (1999)
Secure attachment At approx 30 months p<.03
Constantino et al. (2001)
Interpreting emotional cues Trend only, p=.08
Fraser et al. (2000)
Short-term improvement on maternal-infant interaction
No effect reported.
Goodson et al. (2000)
No improvement No effect reported.
Heinicke et al. (1999, 2000 and 2001)
Secure attachment Responsivity
At 24 months p<.0001/ES 1.31 At 24 months p<.0001/ES 1.63
Letourneau et al. (2001a, 2001b)
Responsiveness For parent subscale p=.036
Klein and Rye. (2004)
Maternal-infant interaction Statistics not reported.
Koniak-Griffin et al. (2003)
No improvement No effect reported.
Moran et al. (2005)
Secure attachment Maternal-infant interaction
At 24 months p<.05/ES 0.25 At 24 months p<.05
Murray et al. (2003)
Sensitivity (for non-directive counselling) At 18 months p=.001
Olds et al. (2002, 2004)
Responsive interaction At 24 months p<.05
Toth et al. (2006)
Secure attachment At 36 months p<.001/ES 1.08
Van Zeijl et al. (2006)
Attitude towards sensitivity At 12 months p<.01
Velderman et al. (2006a and 2006b)
Sensitivity (for VIPP and VIPP-R respectively)
At 6 months p<.05/ES 0.46 and ES 0.52
† where two effect sizes (ES) are noted, more than one intervention was compared with control
Of the primary studies appraised in this review half of them (n=9) included some measure of attachment security, predominantly the Strange Situation Procedure (which is usually conducted in a laboratory playroom). One study used an alternative measure, Caughy et al. (2004) used the Attachment Q-Sort, results from which have been reported to converge with the Strange Situation Procedure (van Ijzendoorn et al. 2004). Of the studies directly considering attachment as an outcome, six studies reported significant change, usually from an insecure or disorganised pattern of attachment to one that was secure (Caughy et al. 2004; Cicchetti et al. 2006; Cohen et al. 1999; Heinicke et al. 1999; Heinicke et al. 2000; Heinicke et al. 2001; Moran et al. 2005; Toth et al. 2006).
However even if infants shift toward a more secure or organised attachment pattern these types of results still need to be viewed with caution. Some of the earlier literature that predates this report involved even younger infants in the birth through pre-attachment stage. It is important to be aware that the effects of interventions will be dependent on the stage of attachment formation. For this reason studies that include outcomes that were measured beyond very early infancy are useful as there may
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
46
well be a time lag between delivery of an intervention and subsequent changes in outcome measures (or other endpoints).
One of the difficulties is in knowing whether any improvements are due specifically to the intervention or whether the improvements might have occurred naturally over time. To some extent the use of studies with an experimental design addresses this but to directly look at this, a normative control is required in addition to their primary comparison group. A few studies did include a normative group for comparison (Cicchetti et al. 2006; Toth et al. 2006). Cohen et al. (1999) points out it is always a possibility that infants with mental health problems may become less symptomatic over time without treatment, as is observed in some studies with older children. It is also possible, that as mothers mature and become more confident in their role, that they might also become more sensitive and responsive in their interactions with their children. Some researchers have suggested that the introduction of an early intervention actually serves to mitigate a reduction in the number and quality of sensitive and responsive interactions that may otherwise naturally occur over time due to the increased behavioural demands of toddlers and other factors such as the arrival of additional children.
Ideally, intervention studies in this field would also include a waiting list or no treatment control group so that infant behaviour and parent perceptions can be more clearly attributed to the effect of treatment. This was not always possible in all of the studies considered either for ethical reasons or because it was impossible to restrict mothers’ access to services available within their community that might constitute an intervention. Notably, several of the studies which report no effect (Fraser et al. 2000; Goodson et al. 2000) were broader studies where comparison mothers received usual care, with no restriction on other programmes and services they might access during the course of the study.
Nearly without exception all of the studies identified used home visiting as the mode of service delivery, however the extent to which home visits were used varied by study. In some studies the home visiting programme constituted the intervention itself, whereas in other studies it was the vehicle for delivering another specified psychosocial intervention.
Only one study by Cohen et al. (1999) appeared to have not used any home-based sessions. The authors alluded to this by suggesting the need to further test their variant of mother-infant psychotherapy in other settings.
Study Limitations
The specific strengths and limitations associated with each study are set out in the limitations and comments section in the evidence tables. Key points are only very briefly discussed here.
The majority of studies were carried out in the United States (56%), with two studies conducted in the Netherlands and Australia respectively (11%). The remaining four reports were from studies based in Canada, Ethiopia, Italy and the United Kingdom.
The studies ranged in size from small pilot trials to large multi-site studies. Studies with smaller sample size may have lacked sufficient power to detect an intervention effect.
The larger studies that used broader approaches although sufficiently powered may have not resulted in significant effects for a number of reasons. Those delivering the intervention may be required first to enable multi-risk families to engage by problem solving and attending to daily hassles before more focused effective interventions targeting sensitivity and representations could be attempted. These types of programmes are also more likely to demonstrate a pattern of small pervasive benefits than large effect sizes for one specific outcome (Fergusson et al. 2005a; Fergusson et al. 2005b; Fergusson et al. 2006).
For studies where difficulties were experienced with recruitment or retention (particularly those with multiple risk factors), samples may not be representative and therefore less generalisable to others. In particular, differential attrition may present an issue for longer term interventions as it may be difficult for control groups to remain motivated to participate in the face of problems but no active support from the programme (Goodson et al. 2000). Samples that have high rates of initial refusal may also be biased as the overall pattern of attachment may be different, with the rate of secure attachment lower and rate of disorganised attachment higher, in refusers compared to mothers who opted to participate in a

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
47
programme. Clearly, for studies in which specific populations were targeted treatment effects found may hold only for that specific group, for example, Klein and Rye (2004).
Few studies addressed how clinicians might identify those mothers for whom the intervention is more likely to be of benefit. In many articles the aim or objective of the intervention was often described but without reference to the specific individual components of the intervention or detail of the process by which intervention goals were achieved. Three groups of investigators specifically referred to their programme as being manualised (Cicchetti et al. 2006; Toth et al. 2006; Van Zeijl et al. 2006) which implies more detailed information on the intervention would be readily available.
Several of the included studies may be nearer to being efficacy than effectiveness trials (for example, “watch, wait and wonder- mother-infant psychotherapy”) and may therefore may not reflect how a therapy might be more flexibly applied in a real world setting as opposed to the clinic setting where few or no collateral therapies were utilised (Cohen et al. 1999; Toth et al. 2006).
Conclusions
The evidence presented in this Technical Brief supports the earlier findings of Bakermans-Kranenburg et al. (2003) who suggested that the most effective interventions do not always use a large number of sessions with families, in fact fewer contacts may be more effective. It also reinforces the idea that behaviourally focused interventions delivered one-to-one with mothers are useful and that these types of interventions are effective regardless of the presence or absence of multiple problems in the family.
Sample characteristics appear to be unrelated to the effectiveness of interventions, though Bakermans-Kranenburg et al. (2003) noted two exceptions to this. Firstly, samples with a higher percentage of insecurity in the control group where interventions may exert a larger effect on infant attachment compared to normative samples and secondly, clinical groups where interventions also appear to have a greater effect on parental sensitivity.
Interventions that were more effective when Bakermans-Kranenburg et al. (2003) restricted their meta-analysis to studies with both random allocation and a control group were also more effective in the subset of clinical and high-risk samples. More general and long-term support of multi-problem families in coping with daily hassles may be needed before more focused interventions can be implemented successfully in this group.
While changes in attachment security reported were generally in a direction consistent with attachment theory, they are modest. Less broad interventions that target sensitive maternal behaviour are among those that are the most successful both at improving insensitive parenting and promoting better infant attachment security. Infant-parent psychotherapy shows some promise while group educational interventions generally do not.
Overall, evidence from primary and secondary research suggests that a variety of types of intervention for enhancing maternal sensitivity and to a lesser extent attachment security are effective, with nearly all of the different approaches involving the use of some form of home visiting to deliver the intervention.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
48
REFERENCES
Ainsworth, M. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psychological study of the strange situation. Hilldale, NJ.: Lawrence Erlbaum. Ammaniti, M., Speranza, A. M., Tambelli, R., Muscetta, S., Lucarelli, L., Vismara, L., et al. (2006). A prevention and promotion intervention program in the field of mother-infant relationship. Infant Mental Health Journal, 27, 70-90. Armstrong, K. L., Fraser, J. A., Dadds, M. R., & Morris, J. (2000). Promoting secure attachment, maternal mood and child health in a vulnerable population: a randomized controlled trial. Journal of Paediatrics & Child Health, 36, 555-562. Bakermans-Kranenburg, M. J., Juffer, F., & van Ijzendoorn, M. H. (1998). Interventions with video feedback and attachment discussions: does type of maternal insecurity make a difference? Infant Mental Health Journal, 19, 202-219. Bakermans-Kranenburg, M. J., Van Ijzendoorn, M. H., & Juffer, F. (2005). Disorganized infant attachment and preventive interventions: a review and meta-analysis. Infant Mental Health Journal, 26, 191-216. Bakermans-Kranenburg, M. J., van, I. M. H., & Juffer, F. (2003). Less is more: meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin, 129, 195-215. Barlow, J., & Parsons, J. (2006). Group-based parent-training programmes for improving emotional and behavioural adjustment in 0-3 year old children. Cochrane Database of Systematic Reviews, Issue 3. Brisch, K. H., Bechinger, D., Betzler, S., & Heinemann, H. (2003). Early preventive attachment-oriented psychotherapeutic intervention program with parents of a very low birthweight premature infant: results of attachment and neurological development. Attachment & Human Development, 5, 120-135. Caughy, M. O., Huang, K. Y., Miller, T., & Genevro, J. L. (2004). The effects of the Healthy Steps for Young Children Program: results from observations of parenting and child development. Early Childhood Research Quarterly, 19, 611-630. Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2006). Fostering secure attachment in infants in maltreating families through preventive interventions. Development and Psychopathology, 18, 623-649. Cohen, N. J., Muir, E., Parker, C. J., Brown, M., Lojkasek, M., Muir, R., et al. (1999). Watch, wait and wonder: testing the effectiveness of a new approach to mother-infant psychotherapy. Infant Mental Health Journal, 20, 429-451. Cole, M., & Cole, S. (1997). The development of children. New York: W. H. Freeman. Constantino, J. N., Hashemi, N., Solis, E., Alon, T., Haley, S., McClure, S., et al. (2001). Supplementation of urban home visitation with a series of group meetings for parents and infants: results of a "real-world" randomized, controlled trial. Child Abuse and Neglect, 25, 1571-1581. Cooper, P. J., & Murray, L. (1997). The impact of psychological treatments of postpartum depression on maternal mood and infant development. In L. Murray & P. J. Cooper (Eds.), Postpartum depression and child development (pp. 201-261). New York: Guilford Press.
Cooper, P. J., Murray, L., Wilson, A., & Romaniuk, H. (2003). Controlled trial of the short- and long-term effect of psychological treatment of post-partum depression. I. Impact on maternal mood. British Journal of Psychiatry, 182, 412-419.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
49
Culp, R. E., Culp, A. M., Osofsky, J. D., & Osofsky, H. D. (1991). Adolescent and older mothers' interaction patterns with their six-month-old infants. Journal of Adolescence, 14, 195-200. Dunst, C. J., & Kassow, D. Z. (2004). Characteristics of interventions promoting parental sensitivity to child behavior. Bridges Practice Based Research Syntheses, 2, 1-17. Egeland, B., & Erickson, M. F. (1993). Attachment theory and findings: implications for prevention and intervention. In S. Kramer & H. Parens (Eds.), Prevention in mental health: now, tomorrow, ever? (pp. 21-50). Northvale, NJ: Jason Aronson. Fergusson, D., Horwood, J., Ridder, E., & Grant, H. (2005a). Early start evaluation report. Christchurch Health and Development Study. Christchurch: Christchurch School of Medicine and Health Sciences. Fergusson, D. M., Grant, H., Horwood, L. J., & Ridder, E. M. (2005b). Randomized trial of the Early Start program of home visitation. Pediatrics, 116, e803-809. Fergusson, D. M., Grant, H., Horwood, L. J., & Ridder, E. M (2006). Randomized trial of the Early Start program of home visitation: parent and family outcomes. Pediatrics, 117, 781-786. Field, T. M., Scafidi, F., Pickens, J., Prodromidis, M., Pelaez-Nogueras, M., Torquati, J., et al. (1998). Polydrug-using adolescent mothers and their infants receiving early intervention. Adolescence, 33, 117-143. Fraser, J. A., Armstrong, K. L., Morris, J. P., & Dadds, M. R. (2000). Home visiting intervention for vulnerable families with newborns: follow-up results of a randomized controlled trial. Child Abuse & Neglect, 24, 1399-1429. Gelfand, D. M., Teti, D. M., Seiner, S. A., & Jameson, P. B. (1996). Helping mothers fight depression: evaluation of a home-based intervention program for depressed mothers and their infants. Journal of Clinical Child Psychology, 25, 406-422. Goodson, B. D., Layzer, J. I., St. Pierre, R. G., Bernstein, L. S., & Lopez, M. (2000). Effectiveness of a comprehensive, five-year family support program for low-income children and their families: findings from the comprehensive child development program. Early Childhood Research Quarterly, 15, 5-39. Gowen, J. W., & Nebrig, J. R. (1997). Innovations in practice. Infant-mother attachment at risk: how early intervention can help. Infants and Young Children 9, 462-478. Hahn, R. A., Mercy, J., Bilukha, O., & Briss, P. (2005). Assessing home visiting programs to prevent child abuse: taking silver and bronze along with gold. Child Abuse & Neglect, 29, 215-218. Heinicke, C. M., Fineman, N. R., Ruth, G., Recchia, S. L., Guthrie, D., & Rodning, C. (1999). Relationship-based intervention with at-risk mothers: outcome in the first year of life. Infant Mental Health Journal Vol, 20, 349-374. Heinicke, C. M., Goorsky, M., Moscov, S., Dudley, K., Gordon, J., Schneider, C., et al. (2000). Relationship-based intervention with at-risk mothers: factors affecting variations in outcome. Infant Mental Health Journal, 21, 133-155. Heinicke, C. M., Rineman, N. R., Ponce, V. A., & Guthrie, D. (2001). Relation-based intervention with at-risk mothers: Outcome in the second year of life. Infant Mental Health Journal, 22, 431-462. Jaffee, S., Caspi, A., Moffitt, T. E., Belsky, J., & Silva, P. (2001). Why are children born to teen mothers at risk for adverse outcomes in young adulthood? Results for a 20-year longitudinal study. Development and Psychopathology, 13, 377-397. Juffer, F., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2005a). Enhancing children's socioemotional development: a review of intervention studies In D. M. Teti (Ed.), Handbook of research methods in developmental science (pp. 214-232). Malden, MA: Blackwell.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
50
Juffer, F., Bakermans-Kranenburg, M. J., & van, I. M. H. (2005b). The importance of parenting in the development of disorganized attachment: evidence from a preventive intervention study in adoptive families. Journal of Child Psychology & Psychiatry & Allied Disciplines, 46, 263-274. Juffer, F., Hoksbergen, R. A., Riksen-Walraven, J. M., & Kohnstamm, G. A. (1997). Early intervention in adoptive families: supporting maternal sensitive responsiveness, infant-mother attachment, and infant competence. Journal of Child Psychology & Psychiatry & Allied Disciplines, 38, 1039-1050. Klein, P. S., & Rye, H. (2004). Interaction-oriented early intervention in Ethiopia: the MISC approach... More Intelligent and Sensitive Children. Infants and Young Children, 17, 340-354. Velderman, M. K, Bakermans-Kranenburg, M. J., Juffer, F., & van Ijzendoorn, M. H. (2006a). Effects of attachment-based interventions on maternal sensitivity and infant attachment: differential susceptibility of highly reactive infants. Journal of Family Psychology, 20, 266-274. Velderman, M. K,, Bakermans-Kranenburg, M. J., Juffer, F., Van Ijzendoorn, M. H., Mangelsdorf, S. C., & Zevalkink, J. (2006b). Preventing preschool externalizing behavior problems through video-feedback intervention in infancy. Infant Mental Health Journal, 27, 466-493. Koniak-Griffin, D., Verzemnieks, I. L., Anderson, N. L., Brecht, M. L., Lesser, J., Kim, S., et al. (2003). Nurse visitation for adolescent mothers: two-year infant health and maternal outcomes. Nursing Research, 52, 127-136. LaFreniere, P. J., & Capuano, F. (1997). Preventive intervention as means of clarifying direction of effects in socialization: anxious-withdrawn preschoolers case. Development & Psychopathology, 9, 551-564. Letourneau, N. (2001a). Attrition among adolescents and infants involved in a parenting intervention. Child: Care, Health and Development 27, 183-186. Letourneau, N. (2001b). Improving adolescent parent-infant interactions: a pilot study. Journal of Pediatric nursing, 16, 53-62. Letourneau, N., Drummond, J., Fleming, D., Kysela, G., McDonald, L., & Stewart, M. (2001). Supporting parents: can intervention improve parent-child relationships? Journal of Family Nursing, 7, 159-187. Lyons-Ruth, K., Connell, D. B., & Grunebaum, H. U. (1990). Infants at social risk: maternal depression and family support services as mediators of infant development and security of attachment. Child Development, 61, 85-98. Martins, C., & Gaffan, E. A. (2000). Effects of early maternal depression on patterns of infant-mother attachment: a meta-analytic investigation. Journal of Child Psychology & Psychiatry & Allied Disciplines, 41, 737-746. McMahon, C. A., Barnett, B., Kowalenko, N. M., & Tennant, C. C. (2006). Maternal attachment state of mind moderates the impact of postnatal depression on infant attachment. Journal of Child Psychology & Psychiatry & Allied Disciplines, 47, 660-669. Moran, G., Pederson, D. R., & Krupka, A. (2005). Maternal unresolved attachment status impedes the effectiveness of interventions with adolescent mothers. Infant Mental Health Journal, 26, 231-249. Murray, L., Cooper, P. J., Wilson, A., & Romaniuk, H. (2003). Controlled trial of the short- and long-term effect of psychological treatment of post-partum depression: 2. Impact on the mother-child relationship and child outcome. British Journal of Psychiatry, 182, 420-427. National Health and Medical Research Council (2005). NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. Pilot program 2005-2007 NHMRC. Available from: http://www.nhmrc.gov.au/publications/_files/levels_grades05.pdf Accessed on 09.03.07

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
51
Olds, D. L., Robinson, J., O'Brien, R., Luckey, D. W., Pettitt, L. M., Henderson, C. R., Jr., et al. (2002). Home visiting by paraprofessionals and by nurses: a randomized, controlled trial. Pediatrics, 110, 486-496.
Olds, D. L., Robinson, J., Pettitt, L., Luckey, D. W., Holmberg, J., Ng, R. K., et al. (2004). Effects of home visits by paraprofessionals and by nurses: age 4 follow-up results of a randomized trial. Pediatrics, 114, 1560-1568.
Sajaniemi, N., Makela, J., Salokorpi, T., von Wendt, L., Hamalainen, T., & Hakamies-Blomqvist, L. (2001). Cognitive performance and attachment patterns at four years of age in extremely low birth weight infants after early intervention. European Child & Adolescent Psychiatry, 10, 122-129. St Pierre, R.G., & Layzer, J.I., (1999). Using home visits for multiple purposes: the Comprehensive Child Development Program. Future of Children, 9, 134-151 Suchman, N., Mayes, L., Conti, J., Slade, A., & Rounsaville, B. (2004). Rethinking parenting interventions for drug-dependent mothers: from behavior management to fostering emotional bonds. Journal of Substance Abuse Treatment, 27, 179-185. Toth, S. L., Rogosch, F. A., Manly, J. T., & Cicchetti, D. (2006). The efficacy of toddler-parent psychotherapy to reorganize attachment in the young offspring of mothers with major depressive disorder: a randomized preventive trial. Journal of Consulting & Clinical Psychology, 74, 1006-1016. van den Boom, D. C. (1994). The influence of temperament and mothering on attachment and exploration: An experimental manipulation of sensitive responsiveness among lower-class mothers with irritable infants. Child Development, 65, 1457-1477. van Ijzendoorn, M. H., Juffer, F., & Duyvesteyn, M. G. C. (1995). Breaking the intergenerational cycle of insecure attachment: a review of the effects of attachment-based interventions on maternal sensitivity and infant security. Journal of Child Psychology and Psychiatry, 36, 225-248. van Ijzendoorn, M. H., Vereijken, C. M. J. L., Bakermans-Kranenburg, M. J., & Riksen-Walraven, J. M. (2004). Assessing attachment security with the attachment Q Sort: meta-analytic evidence for the validity of the observer AQS. Child Development, 75, 1188-1213. Van Zeijl, J., Mesman, J., Van Ijzendoorn, M. H., Bakermans-Kranenburg, M. J., Juffer, F., Stolk, M. N., et al. (2006). Attachment-based intervention for enhancing sensitive discipline in mothers of 1- to 3-year-old children at risk for externalizing behavior problems: a randomized controlled trial. Journal of Consulting & Clinical Psychology, 74, 994-1005. Zahr, L. K. (2000). Home-based intervention after discharge for Latino families of low-birth-weight infants. Infant Mental Health Journal, 21, 448-463.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
52
APPENDIX 1: LEVELS OF EVIDENCE∗
Level I Evidence obtained from a systematic review (or meta-analysis) of relevant randomised controlled trials.
Level II Evidence obtained from at least one randomised controlled trial.
Level III. 1 Evidence obtained from pseudorandomised controlled trials (alternate allocation or some other method).
2 Evidence obtained from comparative studies (including systematic reviews of such studies) with concurrent controls and allocation not randomised, cohort studies, case control studies or interrupted time series with a control group).
3 Evidence obtained from comparative studies with historical control, two or more single-arm studies or interrupted time series without a parallel control group.
Level IV Evidence obtained from case series, either post-test or pretest/post-test.
∗ From NMHRC 2000

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
53

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
54
APPENDIX 2: SEARCH STRATEGY
Medline 1 exp parent-child relations/ (31995) 2 object attachment/ (7085) 3 1 and 2 (2473) 4 attachment.tw. (45934) 5 resilience.mp. (1673) 6 (wellbeing or well being or wellness).mp. (22494) 7 or/3-6 (71358) 8 child, preschool/ or exp infant/ (982779) 9 7 and 8 (4695) 10 "early intervention (education)"/ (670) 11 early intervention.mp. (4831) 12 (parent$ adj3 program$).mp. (1122) 13 (parent$ adj3 (train$ or educat$)).mp. (3313) 14 (home adj2 visit$).mp. (3318) 15 family therapy/ (6150) 16 (family adj2 visit$).mp. (556) 17 multisystemic therapy.mp. (63) 18 or/10-17 (18780) 19 intervention studies/ (3547) 20 pc.fs. (669817) 21 8 and 18 (5485) 22 19 and 20 and 21 (25) 23 (promot$ and (wellbeing or wellness or attachment or well being)).tw. (5374) 24 23 and 8 (225) 25 (healthy steps or healthy start or early start or healthy famil$).tw. (760) 26 9 and 18 (171) 27 22 or 24 or 25 or 26 (1162) 28 limit 27 to english (983) 29 limit 28 to yr=1995-2006 (701) 30 (vaccin$ or immuni$ or breastfeeding or breast feeding).ti. (123620) 31 29 not 30 (687) 32 letter.pt. (581686) 33 31 not 32 (684)
Embase 1 exp child parent relation/ (16863) 2 emotional attachment/ (2235) 3 1 and 2 (770) 4 attachment.tw. (28465) 5 (resilience or wellbeing or well being or wellness).mp. (22842) 6 or/3-5 (51410) 7 Preschool Child/ (65212) 8 Infant/ (128456) 9 7 or 8 (175620) 10 6 and 9 (845) 11 Early Intervention/ (358) 12 (parent$ adj3 program$).tw. (687) 13 (parent$ adj3 (train$ or educat$)).tw. (2690) 14 (home adj2 visit$).tw. (1922) 15 family therapy/ (3427) 16 (family adj2 visit$).tw. (340) 17 multisystemic therap$.tw. (45) 18 or/11-17 (9078) 19 10 and 18 (26)

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
55
20 exp clinical study/ or intervention study/ (2611468) 21 10 and 20 (520) 22 (promot$ and (wellness or wellbeing or well being or attachment)).tw. (3574) 23 (healthy steps or healthy start or early start or healthy famil$).tw. (499) 24 (22 or 23) and 9 (77) 25 19 or 21 or 24 (586) 26 limit 25 to english (548) 27 (vaccin$ or immun$ or breastfeed$ or breast feeding$).tw. (824803) 28 26 not 27 (497) 29 limit 28 to yr=1995-2007 (396) 30 letter.pt. (335288) 31 29 not 30 (396)
Cinahl 1 exp Parent-Child Relations/ (6245) 2 Attachment Behavior/ (663) 3 1 and 2 (265) 4 (infan$ or preschool$ or pre-school$).tw. (21944) 5 3 and 4 (87) 6 limit 3 to (newborn infant <birth to 1 month> or infant <1 to 23 months> or preschool child <2 to 5 years>)
(140) 7 5 or 6 (156) 8 (attachment or resilience or wellbeing or well-being).tw. (9617) 9 4 and 8 (553) 10 limit 8 to (newborn infant <birth to 1 month> or infant <1 to 23 months> or preschool child <2 to 5 years>)
(808) 11 7 or 9 or 10 (1057) 12 early intervention/ or early childhood intervention/ (2283) 13 early intervention.tw. (1638) 14 (parent$ adj3 program$).tw. (574) 15 parenting/ (2420) 16 (parent$ adj3 (training or educat$)).mp. (4437) 17 (home adj2 visit$).tw. (1477) 18 (multi-systemic therapy or multisystemic therapy).mp. (19) 19 intervention$.mp. (61888) 20 Program Evaluation/ (8269) 21 or/12-20 (75019) 22 11 and 21 (327) 23 (healthy steps or healthy start or sure start or healthy famil$).tw. (269) 24 4 and 23 (47) 25 limit 23 to (newborn infant <birth to 1 month> or infant <1 to 23 months> or preschool child <2 to 5 years>)
(100) 26 24 or 25 (114) 27 22 or 26 (438) 28 limit 27 to english (431) 29 limit 28 to yr=1995-2007 (388) 30 (autism or autistic).ti. (1322) 31 (vaccin$ or immuni$ or breastfeed$ or breast feed$).ti. (10772) 32 29 not (30 or 31) (373)
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
56
Psychinfo 1 exp Parent Child Relations/ (39818) 2 attachment behavior/ (8892) 3 1 and 2 (2872) 4 infant$.tw. (38379) 5 preschool child$.mp. (8130) 6 limit 3 to (120 neonatal <birth to age 1 mo> or 140 infancy <age 2 to 23 mo> or 160
preschool age <age 2 to 5 yrs>) (1235) 7 3 and (4 or 5) (1197) 8 6 or 7 (1557) 9 early intervention/ (4948) 10 early intervention.tw. (4552) 11 parent training/ (3968) 12 (parent$ adj3 program$).mp. (3374) 13 (parent$ adj3 (train$ or educat$)).mp. (10798) 14 (home adj2 visit$).mp. (1998) 15 family therapy/ (13913) 16 family intervention/ (662) 17 exp Multimodal Treatment Approach/ (1202) 18 multisystemic therapy.tw. (169) 19 (promot$ and (wellbeing or well being or attachment or wellness)).tw. (2492) 20 or/9-19 (37420) 21 8 and 20 (114) 22 limit 21 to yr=1995-2006 (82) 23 limit 22 to all journals (58) 24 from 23 keep (selected references) 25 (3 and 20) not 21 (85) 26 limit 25 to yr=1995-2006 (68) 27 limit 26 to all journals (34) 28 from 27 keep(selected references) 29 exp program evaluation/ (11461) 30 treatment effectiveness evaluation/ (7886) 31 treatment outcome/ (13233) 32 or/29-31 (31282) 33 (8 and 32) not (22 or 26) (0) 34 attachment.tw. (14942) 35 resilience.tw. (3340) 36 (well being or wellbeing).tw. (21561) 37 or/34-36 (39062) 38 20 and 37 (3284) 39 limit 38 to (120 neonatal <birth to age 1 mo> or 140 infancy <age 2 to 23 mo> or 160 preschool age <age 2 to 5 yrs>) (326) 40 limit 39 to yr=1995-2006 (223) 41 limit 40 to english (211) 42 limit 41 to all journals (132) 43 from 42 keep (selected references) 44 child abuse/ (15427) 45 20 and 44 (939) 46 limit 45 to (120 neonatal <birth to age 1 mo> or 140 infancy <age 2 to 23 mo> or 160 preschool age <age 2 to 5 yrs>) (129) 47 limit 46 to yr=1995-2006 (67) 48 limit 47 to english (60) 49 from 48 keep (selected references) 50 (early start or healthy families or sure start or healthy start or healthy steps).tw. (185) 51 limit 50 to yr=1995-2006 (120) 52 limit 51 to english (114) 53 limit 52 to all journals (86) 54 from 53 keep (selected references)
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
57
Current Contents 1. Attachment 2. Preschool* OR pre-school* 3. Infant OR infants OR infancy 4. #1 AND (#2 OR #3) 5. Parent SAME (train* OR educat* OR program*) 6. #3 AND #5 7. #4 AND #5 8. #6 OR #7 9. #6 AND (trial OR study OR intevention OR program*) 10. #7 OR #9 11. #10 NOT (vaccin* OR immuni* OR breastfeed* OR breast feed*)
Additional cross database search for home visiting – Medline, Embase, Cinahl, PsychInfo 1 home visit$.mp. (7392) 2 domiciliary visit$.mp. (107) 3 1 or 2 (7487) 4 (infant or infants or infancy).mp. (474538) 5 (preschool child$ or young child$).mp. (128133) 6 child$.mp. (1321036) 7 4 or 5 or 6 (1520448) 8 3 and 7 (3403) 9 limit 8 to english (3257) 10 limit 9 to yr=1996-2007 (2579) 11 random$.mp. (661954) 12 10 and 11 (634) 13 remove duplicates from 12 (374) 14 (breastfeed$ or breast feed$).mp. (27148) 15 asthma$.mp. (108630) 16 (vaccin$ or immuni$).mp. (288546) 17 13 not (14 or 15 or 16) (288)
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
58
APPENDIX 3a: EXCLUDED RETRIEVED PAPERS
Anderson, G. C., Moore, E., Hepworth, J., & Bergman, N. (2003). Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database of Systematic Reviews, Issue 3. Systematic review. Intervention outside scope. Bakermans-Kranenburg, M. J., van Ijzendoorn, M. H., & Bradley, R. H. (2005). Those who have, receive: the Matthew effect in early childhood intervention in the home environment. Review of Educational Research, 75, 1-26. Systematic review. General focus on quality of home environment (responsivity measured by the HOMES scale) rather than attachment interventions delivered by home visitors. Barlow, J., Coren, E., & Stewart-Brown, S. S. B. (2006). Parent-training programmes for improving maternal psychosocial health. Cochrane Database of Systematic Reviews, Issue 3. Systematic review. Did not focus on outcomes of interest. Barlow, J., & Parsons, J. (2006). Group-based parent-training programmes for improving emotional and behavioural adjustment in 0-3 year old children. Cochrane Database of Systematic Reviews, Issue 3. Systematic review. Focus on child behavioural adjustment rather than attachment. Outcomes of interest not reported. Barlow, J., Johnston, I., Kendrick, D., Polnay, L., & Stewart-Brown, S. (2006). Individual and group-based parenting programmes for the treatment of physical child abuse and neglect. Cochrane Database of Systematic Reviews, Issue 3. Systematic review. Focus on child abuse and neglect rather than attachment. Outcomes of interest not reported. Barlow, J., Parsons, J., & Stewart-Brown, S. (2005). Preventing emotional and behavioural problems: the effectiveness of parenting programmes with children less than 3 years of age. Child Care Health and Development, 31, 33-42. Systematic review. Focus on emotional and behavioural adjustment outcomes rather than attachment, responsivity and sensitivity. Barlow, J., & Stewart-Brown, S. (2000). Behavior problems and group-based parent education programs. Journal of Developmental & Behavioral Pediatrics, 21, 356-370. Systematic review. Focus on emotional and behavioural adjustment outcomes rather than attachment, responsivity and sensitivity. Barnet, B., Duggan, A. K., Devoe, M., & Burrell, L. (2002). The effect of volunteer home visitation for adolescent mothers on parenting and mental health outcomes - a randomized trial. Archives of Pediatrics & Adolescent Medicine, 156, 1216-1222. Randomised controlled trial. Outcomes of interest not reported.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
59
Belsky, J., Melhuish, E., Barnes, J., Leyland, A. H., & Romanuik, H. (2006). Effects of Sure Start local programmes on children and families: early findings from a quasi-experimental, cross sectional study. BMJ: British Medical Journal, 332. Cross sectional study. Benoit, D., Madigan, S., Lecce, S., Shea, B., & Goldberg, S. (2001). Atypical maternal behavior toward feeding-disordered infants before and after intervention. Infant Mental Health Journal, 22, 611-626. Randomised controlled trial Focus on feeding disordered infants. Bohlin, G., Hagekull, B., & Rydell, A.-M. (2000). Attachment and social functioning: a longitudinal study from infancy to middle childhood. Social Development, 9, 24-39. Cohort study. No intervention delivered. Boris, N. W., Zeanah, C. H., & Work Group on Quality, I. (2005). Practice parameter for the assessment and treatment of children and adolescents with reactive attachment disorder of infancy and early childhood. Journal of the American Academy of Child & Adolescent Psychiatry, 44, 1206-1219. Background. Bosquet, M., & Egeland, B. (2001). Associations among maternal depressive symptomatology, state of mind and parent and child behaviors: implications for attachment-based interventions. Attachment & Human Development, 3, 173-99. Randomised controlled trial. Specific intervention effects of STEEP (Steps Towards Effective Enjoyable Parenting) were not clearly reported in this article. The focus of this paper was on reporting associations between maternal characteristics with regard to attachment status and their relation to maternal and child behaviour. Research focus. Brisch, K. H., Bechinger, D., Betzler, S., & Heinemann, H. (2003). Early preventive attachment-oriented psychotherapeutic intervention program with parents of a very low birthweight premature infant: results of attachment and neurological development. Attachment & Human Development, 5, 120-135. Randomised controlled trial. Relevant attachment-based intervention however focused on a population of interest (preterm infants) that was outside the scope of this report. Brotman, L. M., Dawson-McClure, S., Gouley, K. K., McGuire, K., Burraston, B., & Bank, L. (2005). Older siblings benefit from a family-based preventive intervention for preschoolers at risk for conduct problems. Journal of Family Psychology, 19, 581-591. Randomised controlled trial. Outcomes of interest not reported. Bugental, D. B., Ellerson, P. C., Lin, E. K., Rainey, B., Kokotovic, A., & O'Hara, N. (2002). A cognitive approach to child abuse prevention. Journal of Family Psychology, 16, 243-258. Randomised controlled trial. Outcomes of interest not reported.
EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
60
Carlson, E. A. (1998). A prospective longitudinal study of attachment disorganization/disorientation. Child Development, 69, 1107-1128. Background. Cassidy, J., & Mohr, J. J. (2001). Unsolvable fear, trauma, and psychopathology: theory, research, and clinical considerations related to disorganized attachment across the life span. Clinical Psychology: Science and Practice, 8, 275-298. Background Chambers, H., Amos, J., Allison, S., & Roeger, L. (2006). Parent and child therapy: an attachment-based intervention for children with challenging problems. Australian and New Zealand Journal of Family Therapy, 27, 68-74. Case study. Cicchetti, D., Toth, S. L., & Rogosch, F. A. (1999). The efficacy of toddler-parent psychotherapy to increase attachment security in offspring of depressed mothers. Attachment & Human Development, 1, 34-66. Randomised controlled trial. Outcomes of interest not reported though intervention based on attachment theory. Cooper, P. J., & Murray, L. (1997). The impact of psychological treatments of postpartum depression on maternal mood and infant development. In L. Murray & P. J. Cooper (Eds.), Postpartum depression and child development (pp. 201-261). New York: Guilford Press. Book chapter. Cooper, P. J., Landman, M., Tomlinson, M., Molteno, C., Swartz, L., & Murray, L. (2002). Impact of a mother-infant intervention in an indigent peri-urban South African context: pilot study. British Journal of Psychiatry 180, 76-81. Comparative study. Used Brazelton Neonatal Behavioural Assessment Scale. Coren, E., & Barlow, J. (2006). Individual and group-based parenting programmes for improving psychosocial outcomes for teenage parents and their children. Cochrane Database of Systematic Reviews, Issue 3. Systematic review. Broader focus than attachment and sensitivity. This review did identify several parenting programs (articles published predate the time restriction for this report) that examined parenting programmes delivered on a one-to-one basis in the home. Results using the NCATS measure indicated a large but non-significant effect favouring infants in the intervention group on responsiveness to the parent. No significant difference was apparent for improving the clarity of interpreting infant cues. Coren, E., Barlow, J., & Stewart-Brown, S. (2003). The effectiveness of individual and group-based parenting programmes in improving outcomes for teenage mothers and their children: a systematic review. Journal of Adolescence, 26, 79-103. Systematic review. Broader focus than attachment and sensitivity.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
61
Cornish, A. M., McMahon, C., Ungerer, J. A., Barnett, B., Kowalenko, N., & Tennant, C. (2006). Maternal depression and the experience of parenting in the second postnatal year. Journal of Reproductive & Infant Psychology, 24, 121-132. Descriptive study. Craig, E. A. (2004). Parenting programs for women with mental illness who have young children: a review. Australian and New Zealand Journal of Psychiatry, 38, 923-928. Narrative review. Diener, M. L., Nievar, M. A., & Wright, C. (2003). Attachment security among mothers and their young children living in poverty: Associations with maternal, child, and contextual characteristics. Merrill Palmer Quarterly, 49, 154-182. Controlled trial. Random allocation not reported. No intervention effects reported. Doherty, W. J., Erickson, M. F., & LaRossa, R. (2006). An intervention to increase father involvement and skills with infants during the transition to parenthood. Journal of Family Psychology, 20, 438-447. Randomised controlled trial. Outcomes of interest not reported. Dunst, C. J., & Kassow, D. Z. (2004). Characteristics of interventions promoting parental sensitivity to child behavior. Bridges Practice Based Research Syntheses, 2, 1-17. Meta-analysis. This is a practice-based summary of the systematic review by Bakermans-Kranenburg et al. (2003). El-Kamary, S. S., Higman, S. M., Fuddy, L., McFarlane, E., Sia, C., & Duggan, A. K. (2004). Hawaii's healthy start home visiting program: determinants and impact of rapid repeat birth. Pediatrics, 114, e317-26. Randomised controlled trial. Attachment outcomes not the focus of article. Elkan, R., Kendrick, D., Hewitt, M., Robinson, J. J. A., Tolley, K., Blair, M., et al. (2000). The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature. Health Technology Assessment, 4, 1-361. Systematic Review. Focus on home visiting not attachment intervention. All age focus. Fergusson, D. M., Grant, H., Horwood, L. J., & Ridder, E. M. (2005). Randomized trial of the Early Start program of home visitation. Pediatrics, 116, e803-9. Randomised controlled trial. Attachment outcomes not the focus of article. Field, T. M., Scafidi, F., Pickens, J., Prodromidis, M., Pelaez-Nogueras, M., Torquati, J., Wilcox, H., Malphurs, J., Schanberg, S., & Kuhn, C. (1998). Polydrug-using adolescent mothers and their infants receiving early intervention. Adolescence, 33, 117-43. Controlled trial, method of assignment unclear. Mothers using drugs.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
62
Galano, J., Credle, W., Perry, D., Berg, S. W., Huntington, L., & Stief, E. (2001). Developing and sustaining a successful community prevention initiative: the Hampton Healthy Families Partnership. Journal of Primary Prevention, 21, 495-509. Descriptive study of a programme. Garbers, C., Tunstill, J., Allnock, D., & Akhurst, S. (2006). Facilitating access to services for children and families: lessons from Sure Start Local Programmes. Child & Family Social Work, 11, 287-296. Background. Presents models of three types of parental service use. Guyer, B., Hughart, N., Strobino, D., Jones, A., & Scharfstein, D. (2000). Assessing the impact of pediatric-based development services on infants, families, and clinicians: challenges to evaluating the Health Steps Program. Pediatrics, 105, E33. Randomised controlled trial. Describes evaluation design and study. Herschell, A. D., Calzada, E. J., Eyberg, S. M., & McNeil, C. B. (2002). Parent-child interaction therapy: New directions in research. Cognitive and Behavioral Practice, 9, 9-15. Background to the therapy. Not a study. Hoffman, K. T., Marvin, R. S., Cooper, G., & Powell, B. (2006). Changing toddlers' and preschoolers' attachment classifications: the Circle of Security intervention. Journal of Consulting and Clinical Psychology, 74, 1017-1026. Pre-test/post-test study with no control group. Horowitz, J. A., Bell, M., Trybulski, J., Munro, B. H., Moser, D., Hartz, S. A., et al. (2001). Promoting responsiveness between mothers with depressive symptoms and their infants. Journal of Nursing Scholarship 33, 323-329. Randomised controlled trial. Only one relevant outcome reported. The treatment group did show significantly higher maternal infant responsiveness after an interactive coaching intervention to promote responsiveness (as measured by the Dyadic Mutuality Code). Johnston, B. D., Huebner, C. E., Anderson, M. L., Tyll, L. T., & Thompson, R. S. (2006). Healthy steps in an integrated delivery system: child and parent outcomes at 30 months. Archives of Pediatrics & Adolescent Medicine, 160, 793-800. Randomised controlled trial. Outcomes of interest not reported. Juffer, F., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2005). Enhancing children's socioemotional development: a review of intervention studies In D. M. Teti (Ed.), Handbook of research methods in developmental science (pp. 214-232). Malden, MA: Blackwell. Book chapter.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
63
Juffer, F., Bakermans-Kranenburg, M. J., & van, I. M. H. (2005). The importance of parenting in the development of disorganized attachment: evidence from a preventive intervention study in adoptive families. Journal of Child Psychology & Psychiatry & Allied Disciplines, 46, 263-74. Randomised controlled trial. Sample of adoptive children outside predetermined scope but included as a separate appendix. Kaaresen, P. I., Ronning, J. A., Ulvund, S. E., & Dahl, L. B. (2006). A randomized, controlled trial of the effectiveness of an early-intervention program in reducing parenting stress after preterm birth. Pediatrics, 118, e9-19. Randomised controlled trial. Conference Abstract. Kendrick, D., Elkan, R., Hewitt, M., Dewey, M., Blair, M., Robinson, J., et al. (2000). Does home visiting improve parenting and the quality of the home environment? A systematic review and meta analysis. Archives of Disease in Childhood, 82, 443-451. Systematic review. General focus on home visiting programmes and quality of home environment (measured by the HOMES scale) rather than attachment interventions delivered by home visitors. Klein Velderman, M., Bakermans-Kranenburg, M. J., Juffer, F., & van Ijzendoorn, M. H. (2006). Effects of attachment-based interventions on maternal sensitivity and infant attachment: differential susceptibility of highly reactive infants. Journal of Family Psychology, 20, 266-274. Descriptive study. Kivijärvi, M., Räihä, H., Kaljonen, A., Tamminen, T., & Piha, J. (2005). Infant temperament and maternal sensitivity behavior in the first year of life. Scandinavian Journal of Psychology, 46, 421-428. Cross-sectional study. No control group. Lagerberg, D. (2000). Secondary prevention in child health: effects of psychological intervention, particularly home visitation, on children's development and other outcome variables. Acta Paediatrica Supplement, 89, 43-52. Narrative review. Methods not outlined. Includes sensitivity and attachment interventions. Landry, S. H., Smith, K. E., & Swank, P. R. (2006). Responsive parenting: establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42, 627-642. Randomised controlled trial. Only reported one outcome of interest (responsivity) and did not report any outcome measures for attachment. The study compared term infants with those born at very low birth weight with a developmental comparison group. The target group that received the intervention showed greater increases in responsiveness than the comparison group, with changes in emotionally supportive behaviours strongest for the low birth weight babies and mothers. Leitch, D. B. (1999). Mother-infant interaction: achieving synchrony. Nursing Research 48, 55-58. Quasi-experimental study. Random assignment to intervention group at time of registration. Reports on a brief prenatal intervention but relevant outcomes only measured 24 hours post-birth.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
64
Letourneau, N. (2001). Improving adolescent parent-infant interactions: a pilot study. Journal of Pediatric Nursing, 16, 53-62. Randomised controlled trial (pilot study). Only one outcome of interest reported (NCATS). Love, J. M., Kisker, E. E., Ross, C., Raikes, H., Constantine, J., Boller, K., et al. (2005). The effectiveness of early head start for 3-year-old children and their parents: lessons for policy and programs. Developmental Psychology, 41, 885-901. Randomised controlled trial. This was a high quality trial however this article did not specifically report outcomes of interest (sensitivity, responsiveness, attachment) although child oucome measures did include relevant instruments such as the Child Behavior Checklist (CBCL) and the Home Observation for Measurement of the Environment (HOME). Early Head Start children had lower levels of aggression and rated higher on engagement with their parents compared with children in the control group. Luster, T., Perlstadt, H., McKinney, M., Sims, K., & Juang, L. (1996). The effects of a family support program and other factors on the home environments provided by adolescent mothers. Family Relations: Journal of Applied Family & Child Studies, 45, 255-264. Randomised controlled trial. Attachment outcomes not the focus of article. Lynch, K. B., Geller, S. R., & Schmidt, M. G. (2004). Multi-year Evaluation of the effectiveness of a resilience-based prevention program for young children. Journal of Primary Prevention, 24, 335-353. Narrative review. MacLeod, J., & Nelson, G. (2000). Programs for the promotion of family wellness and the prevention of child maltreatment: a meta-analytic review. Child Abuse & Neglect, 24, 1127-1149. Meta-analysis. Only one outcome measure (HOME) of interest reported and no detail on sensitivity subscales. Martins, C., & Gaffan, E. A. (2000). Effects of early maternal depression on patterns of infant-mother attachment: a meta-analytic investigation. Journal of Child Psychology & Psychiatry & Allied Disciplines, 41, 737-746. Meta analysis but not of intervention studies. Marvin, R., Cooper, G., Hoffman, K., & Powell, B. (2002). The Circle of Security project: attachment-based intervention with caregiver-pre-school child dyads. Attachment & Human Development, 4, 107-124. Case study. McMahon, C. A., Barnett, B., Kowalenko, N. M., & Tennant, C. C. (2006). Maternal attachment state of mind moderates the impact of postnatal depression on infant attachment. Journal of Child Psychology & Psychiatry & Allied Disciplines, 47, 660-669. Longitudinal study. Focus on implications for intervention.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
65
Mercer, R. T., & Walker, L. O. (2006). A review of nursing interventions to foster becoming a mother. JOGNN: Journal of Obstetric, Gynecologic, and Neonatal Nursing, 35, 568-582. Systematic review. Focus on brief postnatal interventions (up to 4 months post-partum). Minkovitz, C. S., Hughart, N., Strobino, D., Scharfstein, D., Grason, H., Hou, W., Miller, T., Bishai, D., Augustyn, M., McLearn, K. T., & Guyer, B. (2003). A practice-based intervention to enhance quality of care in the first 3 years of life: the Healthy Steps for Young Children Program. JAMA, 290, 3081-91. Randomised controlled trial (by site). Attachment outcomes not the focus of article. Nelson, G., Westhues, A., & MacLeod, J. (2003). A meta-analysis of longitudinal research on preschool prevention programs for children. Prevention & Treatment, Vol 6, Article 31. Meta-analysis. Not outcomes of interest. Socioemotional outcomes only reported at a broad level. Norr, K. F., Crittenden, K. S., Lehrer, E. L., Reyes, O., Boyd, C. B., Nacion, K. W., & Watanabe, K. (2003). Maternal and infant outcomes at one year for a nurse-health advocate home visiting program serving African Americans and Mexican Americans. Public Health Nursing, 20, 190-203. Randomised controlled trial. Only one outcome of interest reported (HOMES). Nylen, K. J., Moran, T. E., Franklin, C. L., & O'Hara, M. W. (2006). Maternal depression: a review of relevant treatment approaches for mothers and infants. Infant Mental Health Journal, 27, 327-343. Narrative review. O'Connor, T. G., & Zeanah, C. H. (2003). Attachment disorders: assessment strategies and treatment approaches. Attachment & Human Development Vol, 5, 223-244. Background. Olds, D. L. (2006). The nurse-family partnership: an evidence-based preventive intervention. Infant Mental Health Journal, 27, 5-25. Narrative review. Onozawa, K., Glover, V., Adams, D., Modi, N., & Kumar, R. C. (2001). Infant massage improves mother-infant interaction for mothers with postnatal depression. Journal of Affective Disorders, 63, 201-7. Randomised controlled trial. Not intervention of interest. Palfrey, J. S., Hauser-Cram, P., Bronson, M. B., Warfield, M. E., Sirin, S., & Chan, E. (2005). The Brookline Early Education Project: a 25-year follow-up study of a family-centered early health and development intervention. Pediatrics, 116, 144-152. Comparative study. Outcomes of interest not reported.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
66
Reynolds, A. J., & Ou, S.-R. (2004). Alterable predictors of child well-being in the Chicago longitudinal study. Children and Youth Services Review, 26, 1-14. Descriptive summary of cohort study. Sajaniemi, N., Makela, J., Salokorpi, T., von Wendt, L., Hamalainen, T., & Hakamies-Blomqvist, L. (2001). Cognitive performance and attachment patterns at four years of age in extremely low birth weight infants after early intervention. European Child & Adolescent Psychiatry, 10, 122-9. Pseudorandomised controlled trial. Not population of interest. Schuler, M. E., Nair, P., Black, M. M., & Kettinger, L. (2000). Mother-infant interaction: effects of a home intervention and ongoing maternal drug use. Journal of Clinical Child Psychology, 29, 424-31. Randomised controlled trial. Mothers using drugs Siddiqui, A., & Hagglof, B. (2000). Does maternal prenatal attachment predict postnatal mother-infant interaction? Early Human Development, 59, 13-25. Cross sectional study. Background on maternal responsive behaviour. Stormshak, E. A., Kaminski, R. A., & Goodman, M. R. (2002). Enhancing the parenting skills of Head Start families during the transition to kindergarten. Prevention Science, 3, 223-34. Randomised controlled trial (by site). Attachment outcomes not the focus of article. Suchman, N., Pajulo, M., DeCoste, C., & Mayes, L. (2006). Parenting interventions for drug-dependent mothers and their young children: The case for an attachment-based approach. Family Relations, 55, 211-226. Narrative review. Also describes the development of a pilot randomised controlled trial. Suchman, N., Mayes, L., Conti, J., Slade, A., & Rounsaville, B. (2004). Rethinking parenting interventions for drug-dependent mothers: from behavior management to fostering emotional bonds. Journal of Substance Abuse Treatment, 27, 179-85. Background. Mothers using drugs. Sweet, M. A., & Appelbaum, M. I. (2004). Is home visiting an effective strategy? A meta-analytic review of home visiting programs for families with young children. Child Development, 75, 1435-1456. Meta analysis. General focus on home visiting programmes rather than attachment interventions delivered by home visitors. Suchman, N., Mayes, L., Conti, J., Slade, A., & Rounsaville, B. (2004). Rethinking parenting interventions for drug-dependent mothers: from behavior management to fostering emotional bonds. Journal of Substance Abuse Treatment, 27, 179-185. Comparative study. Population group outside the scope of this report.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
67
Tessier, R., Cristo, M., Velez, S., Giron, M., de Calume, Z. F., Ruiz-Palaez, J. G., et al. (1998). Kangaroo mother care and the bonding hypothesis. Pediatrics, 102, e17. Randomised controlled trial. Intervention outside the scope of this report. Toth, S. L., Maughan, A., Manly, J. T., Spagnola, M., & Cicchetti, D. (2002). The relative efficacy of two interventions in altering maltreated preschool children's representational models: implications for attachment theory. Development & Psychopathology, 14, 877-908. Randomised controlled trial. Outcomes of interest not reported in this article. Wendland-Carro, J., Piccinini, C. A., & Millar, W. S. (1999). The role of an early intervention on enhancing the quality of mother-infant interaction. Child Development, 70, 713-21. Randomised controlled trial. Brief postnatal hospital-based intervention. Wiggins, M., Oakley, A., Roberts, I., Turner, H., Rajan, L., Austerberry, H., et al. (2004). The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas. Health Technology Assessment, 8, 1-139. Randomised controlled trial. Not outcomes of interest. Willinger, U., Diendorfer-Radner, G., Willnauer, R., Jorgl, G., & Hager, V. (2005). Parenting stress and parental bonding. Behavioral Medicine, 31, 63-69. Background. Zahr, L. K. (2000). Home-based intervention after discharge for Latino families of low-birth-weight infants. Infant Mental Health Journal, 21, 448-463. Pseudo-randomised controlled trial. Focus on low-birth-weight infants.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
68
APPENDIX 3b: APPRAISED RETRIEVED PAPERS (EXCLUDED)
Authors, country
Intervention, setting
Sample characteristics, inclusion and exclusion criteria
Study design, methods
Results Comments/limitations, authors’ conclusions
Juffer et al. (2005b) The Netherlands
Intervention Personal book group (PB) Personal book plus three sessions home-based video feedback (VF) Control No intervention
Participants were 90 families with a first adopted child and 40 families with birth children and a first adopted child. All families were randomly recruited through adoption agencies and not selected in future problems. Adopted children were not selected by, nor matched to, the characteristics of their future adoptive parents. n=130 (66 boys, 64 girls) Inclusion criteria
family with first adopted child child came into adoptive care
before 6 months of age Exclusion criteria None specifically stated. Baseline differences between intervention and control groups were not found for family background characteristics, e.g. socioeconomic status or parent’s age, the number of boys or girls, or the adopted child’s health problems on arrival. There were significant differences with respect to the association between country of origin and age on arrival. Post hoc tests indicated that infants in the video-feedback group arrived at an older age than the children in the book-only or control group.
Randomised controlled trial. Experimental group versus control, pretest/posttest. Data was collected and mother-child interactions videotaped in the home at baseline (6 months) and at follow-up (12-months). In addition at 6 and 9 months mother-child interaction was videotaped in all families. In the video-feedback group, videotapes were used in the intervention whereas in the other groups they were not. At 12 and 18-months infant-mother attachment was observed in the laboratory. Attrition There was no attrition between pre- and posttests. Assessment and outcome measures Strange Situation Procedure (SSP) Dutch Temperament Questionnaire
Intervention effects were computed using analysis of covariance (ANCOVA). Sensitive Responsiveness The standardized composite score for sensitive responsiveness at 12 months was conducted with experimental condition (video feedback, book-only and control) as the independent variable and pretest responsiveness (standardized composite score) as the covariate. A significant main effect of the experimental condition was found (p=.01). Two further planned comparisons were examined. The book intervention did not yield a significant effect compared with the control (p=.07). However there was a significant main effect for the video-feedback intervention (p<.01). Post hic analyses confirmed that the effects on sensitiveness responsiveness were in the same direction and of comparable magnitude in families with and without birth children. Disorganized Attachment The intervention with video feedback was effective and lowered the number of disorganized infants as well as the continuous disorganization score. A moderate effect size of d=0.46 for the effect on the disorganized attachment classification, and a medium to strong effect size of d =.62 for the effect on the continuous disorganization ratings. The book-only intervention did not result in a significant decrease of infant disorganization, although infants in this group had lower ratings than in the control group
Limitations sample of adopted children who may be a special case
of attachment insecurity, may limit generalisability the study intervention was not specifically aimed at
changing attachment disorganization but may have affected aspects of parenting that are important for this
Comments
the intervention was primarily aimed at promoting sensitive parenting and secure attachment
the authors note that the discovery of a distinct effect of the video-feedback intervention is important, as a follow-up study has found that infant disorganized attachment in combination with difficult temperament is predictive of less optimal cognitive development and less optimal ego-control in middle childhood
adoptive families were particularly open to intervention and eager to receive support (as noted by the zero attrition rate)
the success of the intervention cannot be explained by post-adoption support as no such service were available at the time of the study
sample consists of parents with genetically unrelated, adopted children who were not selected but placed by chance so results are not confounded by genetically transmitted risks or protective factors for attachment disorganization.
Authors’ conclusions A short-term preventive intervention program with video feedback and a book lowered the rate of disorganized attachment. The effectiveness of the intervention documents the importance of parenting in the development of infant attachment disorganization.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
69

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
70
APPENDIX 4: APPRAISED RETRIEVED PAPERS
Secondary Articles
Bakermans-Kranenburg, M. J., Van Ijzendoorn, M. H., & Juffer, F. (2005). Disorganized infant attachment and preventive interventions: a review and meta-analysis. Infant Mental Health Journal, 26, 191-216.
Bakermans-Kranenburg, M. J., van, I. M. H., & Juffer, F. (2003). Less is more: meta-analyses of sensitivity and attachment interventions in early childhood. Psychological Bulletin, 129, 195-215.
Primary Articles
Ammaniti, M., Speranza, A. M., Tambelli, R., Muscetta, S., Lucarelli, L., Vismara, L., et al. (2006). A prevention and promotion intervention program in the field of mother-infant relationship. Infant Mental Health Journal, 27, 70-90.
Armstrong, K. L., Fraser, J. A., Dadds, M. R., & Morris, J. (2000). Promoting secure attachment, maternal mood and child health in a vulnerable population: a randomized controlled trial. Journal of Paediatrics & Child Health, 36, 555-62.
Caughy, M. O., Huang, K. Y., Miller, T., & Genevro, J. L. (2004). The effects of the Healthy Steps for Young Children Program: results from observations of parenting and child development. Early Childhood Research Quarterly, 19, 611-630.
Cicchetti, D., Rogosch, F. A., & Toth, S. L. (2006). Fostering secure attachment in infants in maltreating families through preventive interventions. Development and Psychopathology, 18, 623-649.
Cohen, N. J., Muir, E., Parker, C. J., Brown, M., Lojkasek, M., Muir, R., & Barwick, M. (1999). Watch, wait and wonder: testing the effectiveness of a new approach to mother-infant psychotherapy. Infant Mental Health Journal, 20, 429-451.
Constantino, J. N., Hashemi, N., Solis, E., Alon, T., Haley, S., McClure, S., Nordlicht, N., et al. (2001). Supplementation of urban home visitation with a series of group meetings for parents and infants: results of a "real-world" randomized, controlled trial. Child Abuse and Neglect, 25, 1571-81.
Cooper, P. J., Murray, L., Wilson, A., & Romaniuk, H. (2003). Controlled trial of the short- and long-term effect of psychological treatment of post-partum depression. I. Impact on maternal mood. British Journal of Psychiatry, 182, 412-419.
Fraser, J. A., Armstrong, K. L., Morris, J. P., & Dadds, M. R. (2000). Home visiting intervention for vulnerable families with newborns: follow-up results of a randomized controlled trial. Child Abuse & Neglect, 24, 1399-429.
Goodson, B. D., Layzer, J. I., St. Pierre, R. G., Bernstein, L. S., & Lopez, M. (2000). Effectiveness of a comprehensive, five-year family support program for low-income children and their families: findings from the comprehensive child development program. Early Childhood Research Quarterly, 15, 5-39.
Heinicke, C. M., Fineman, N. R., Ruth, G., Recchia, S. L., Guthrie, D., & Rodning, C. (1999). Relationship-based intervention with at-risk mothers: outcome in the first year of life. Infant Mental Health Journal. Vol, 20, 349-374.
Heinicke, C. M., Goorsky, M., Moscov, S., Dudley, K., Gordon, J., Schneider, C., & Guthrie, D. (2000). Relationship-based intervention with at-risk mothers: factors affecting variations in outcome. Infant Mental Health Journal, 21, 133-155.

EFFECTIVE STRATEGIES FOR PROMOTING ATTACHMENT BETWEEN YOUNG CHILDREN AND THEIR PARENTS
71
Heinicke, C. M., Rineman, N. R., Ponce, V. A., & Guthrie, D. (2001). Relation-based intervention with at-risk mothers: outcome in the second year of life. Infant Mental Health Journal, 22, 431-462.
Letourneau, N., Drummond, J., Fleming, D., Kysela, G., McDonald, L., & Stewart, M. (2001a). Supporting parents: Can intervention improve parent-child relationships? Journal of Family Nursing, 7, 159-187.
Letourneau, N. (2001b). Improving adolescent parent-infant interactions: a pilot study. Journal of Pediatric Nursing, 16, 53-62.
Klein, P. S., & Rye, H. (2004). Interaction-oriented early intervention in Ethiopia: the MISC approach... More Intelligent and Sensitive Children. Infants and Young Children, 17, 340-354.
Koniak-Griffin, D., Verzemnieks, I. L., Anderson, N. L., Brecht, M. L., Lesser, J., Kim, S., et al. (2003). Nurse visitation for adolescent mothers: two-year infant health and maternal outcomes. Nursing Research, 52, 127-136.
Moran, G., Pederson, D. R., & Krupka, A. (2005). Maternal unresolved attachment status impedes the effectiveness of interventions with adolescent mothers. Infant Mental Health Journal, 26, 231-249.
Murray, L., Cooper, P. J., Wilson, A., & Romaniuk, H. (2003). Controlled trial of the short- and long-term effect of psychological treatment of post-partum depression: 2. Impact on the mother-child relationship and child outcome. British Journal of Psychiatry, 182, 420-7.
Olds, D. L., Robinson, J., O'Brien, R., Luckey, D. W., Pettitt, L. M., Henderson, C. R., Jr., et al. (2002). Home visiting by paraprofessionals and by nurses: a randomized, controlled trial.. Pediatrics, 110, 486-496.
Olds, D. L., Robinson, J., Pettitt, L., Luckey, D. W., Holmberg, J., Ng, R. K., et al. (2004). Effects of home visits by paraprofessionals and by nurses: age 4 follow-up results of a randomized trial. Pediatrics, 114, 1560-1568.
Toth, S. L., Rogosch, F. A., Manly, J. T., & Cicchetti, D. (2006). The efficacy of toddler-parent psychotherapy to reorganize attachment in the young offspring of mothers with major depressive disorder: a randomized preventive trial. Journal of Consulting & Clinical Psychology, 74, 1006-1016.
Van Zeijl, J., Mesman, J., Van Ijzendoorn, M. H., Bakermans-Kranenburg, M. J., Juffer, F., Stolk, M. N., et al. (2006). Attachment-based intervention for enhancing sensitive discipline in mothers of 1- to 3-year-old children at risk for externalizing behavior problems: a randomized controlled trial. Journal of Consulting & Clinical Psychology, 74, 994-1005.
Velderman, M. K., Bakermans-Kranenburg, M. J., Juffer, F., & van, I. M. H. (2006a). Effects of attachment-based interventions on maternal sensitivity and infant attachment: differential susceptibility of highly reactive infants. Journal of Family Psychology, 20, 266-74.
Velderman, M.K, Bakermans-Kranenburg, M. J., Juffer, F., Van Ijzendoorn, M. H., Mangelsdorf, S. C., & Zevalkink, J. (2006b). Preventing preschool externalizing behavior problems through video-feedback intervention in infancy. Infant Mental Health Journal, 27, 466-493.