edema -what we should know -...
TRANSCRIPT

© 3M 2012 1
Edema:What We Should Know,What Should We Do?What Should We Do?
Terry Treadwell, MD, FACSMedical DirectorInstitute for Advanced Wound CareMontgomery, [email protected]
Massive Edema
Photo used with permission
Edema
• Is the presence of abnormally large amounts of fluid in the intercellular tissue spaces of the body, usually the subcutaneous tissues.
• Can occur in any tissue of the bodyy y
• Fluid contains low levels of protein
• Fluid containing high levels of protein--lymphedema
Dorland’ Illustrated Medical Dictionary, 24th Edition, W.B. Saunders Co., Philadelphia, PA, 1965, p. 467

© 3M 2012 2
Why Worry About Edema?
• Sign of an important systemic condition
• Impairs local cell nutrition
• Is painful
• Gives rise to impaired mobility
• Increases risk of infection (cellulitis)
• Results in blistering of the skin and ulcers
Mortimer PS, Levick JR. Chronic Peripheral Oedema: The Critical Role of the Lymphatic System. Clinical Medicine2004;4(5):448-453
Complications of Edema
Edema With BlistersCellulitis
Why Is Edema Important?
• Can be seen in 1 in 200 people > age 65
• 80% of patients have missed work because of edema
9% h h d l t t t lt f • 9% have changed employment status as a result of edema
Moffatt C, Franks PJ, Doherty DC, Williams AF, et al. Lymphedema: An Underestimated Health Problem. QJM2003;96:731-738
© 3M 2012 3
Etiology of Edema
• The diagnosis of edema is the disease that causes it
• >90% of patients, diagnosis can be determined by history and physical exam
10% f ti t ith d d l b t • 10% of patients with edema need laboratory exam or radiologic studies for diagnosis
Treadwell T, Fowler E, Jensen BB. Management of Edema in Wound Care: A Collaborative Practice Manual for Health Professionals, Fourth Edition. Eds.-Carrie Sussman and Barbara Bates Jensen, Lippincott, Wilkins, and Williams, New York, NY, 2012
Causes of EdemaBilateral1. Cardiac disease2. Renal disease3. Hepatic disease4. GI disease5. Immune disease and allergy
Unilateral1. Venous disease2. Arterial disease usually A-V fistulae3. Lymphatic disease4. Operations5. Trauma5. Immune disease and allergy
6. Nutritional disease7. Endocrine disease8. Pregnancy9. Circulatory problems usually vena
caval obstruction10.Drugs and medications11. Inactivity and dependency of legs
5. Trauma6. Cancer and other tumors
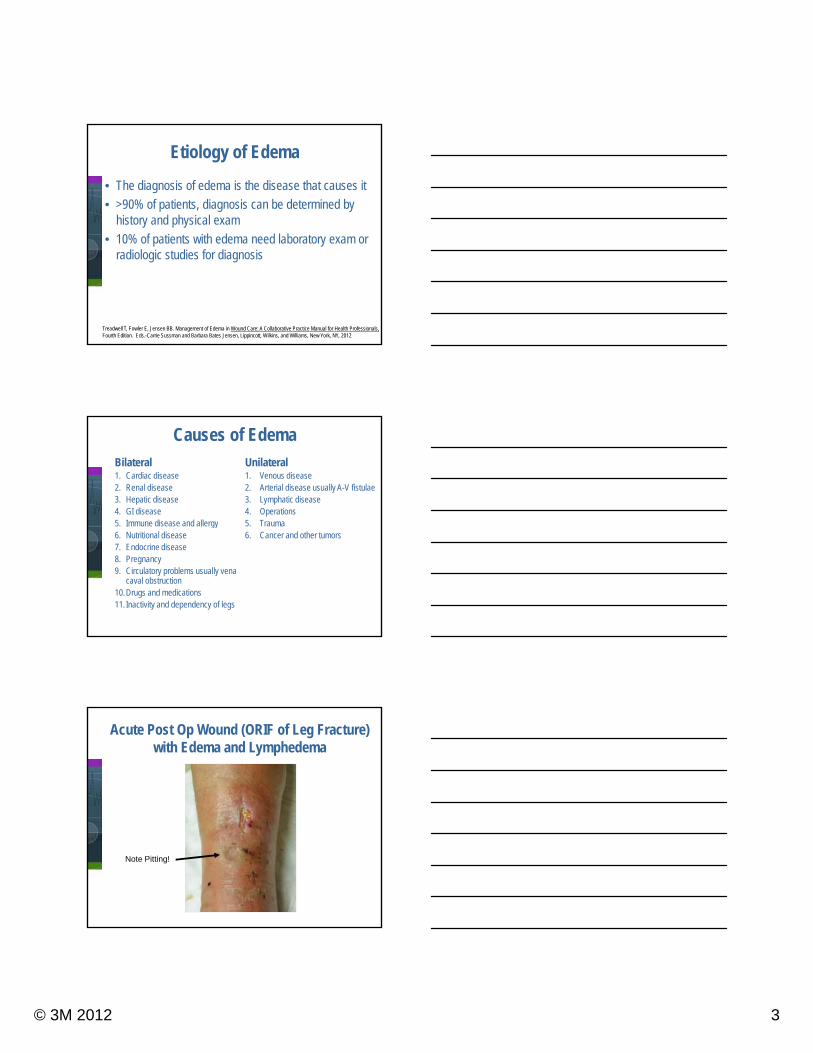
Acute Post Op Wound (ORIF of Leg Fracture) with Edema and Lymphedema
Note Pitting!

© 3M 2012 4
Drugs Causing Edema
• Calcium channel blockers
• Hydralazine
• Clonidine
• Minoxidil
• Reserpine
• Corticosteroids
• Estrogen
• Progesterone
• Tamoxifin
• Testosteronep
• Beta-blockers
• Cilostazol
• Gabapentin
• Pregabalin (Lyrica)
• MAO-inhibitors
• Non-steroidal anti-inflammatory drugs
• Cox-2 inhibitors
Treadwell T, Fowler E, Jensen BB. Management of Edema in Wound Care: A Collaborative Practice Manual for Health Professionals, Fourth Edition. Eds.-Carrie Sussman and Barbara Bates Jensen, Lippincott, Wilkins, and Williams, New York, NY, 2012
Bundens WP. The Chronically Swollen Leg: Finding the Cause: Theory and Practice, in Venous Ulcers, Ed. Bergan JJ and Shortell CK, Elsevier, Boston, MA, 2007, p.73
Venous Insufficiency
• Chronic ambulatory venous hypertension
• Incompetence of valves in veins
–Long-standing saphenous, deep venous, and perforator incompetence
Angle N, et al. Br Med J . 1997;314(7086):1019-1023. Burton CS. Am J Surg. 1994;167(1A):37S-40S.
–Local trauma
–Undetected venous thrombosis
–Operative injury
• Capillary and venular dilatation
• Calf muscle pump failure
Valvular Incompetence
© 3M 2012 5
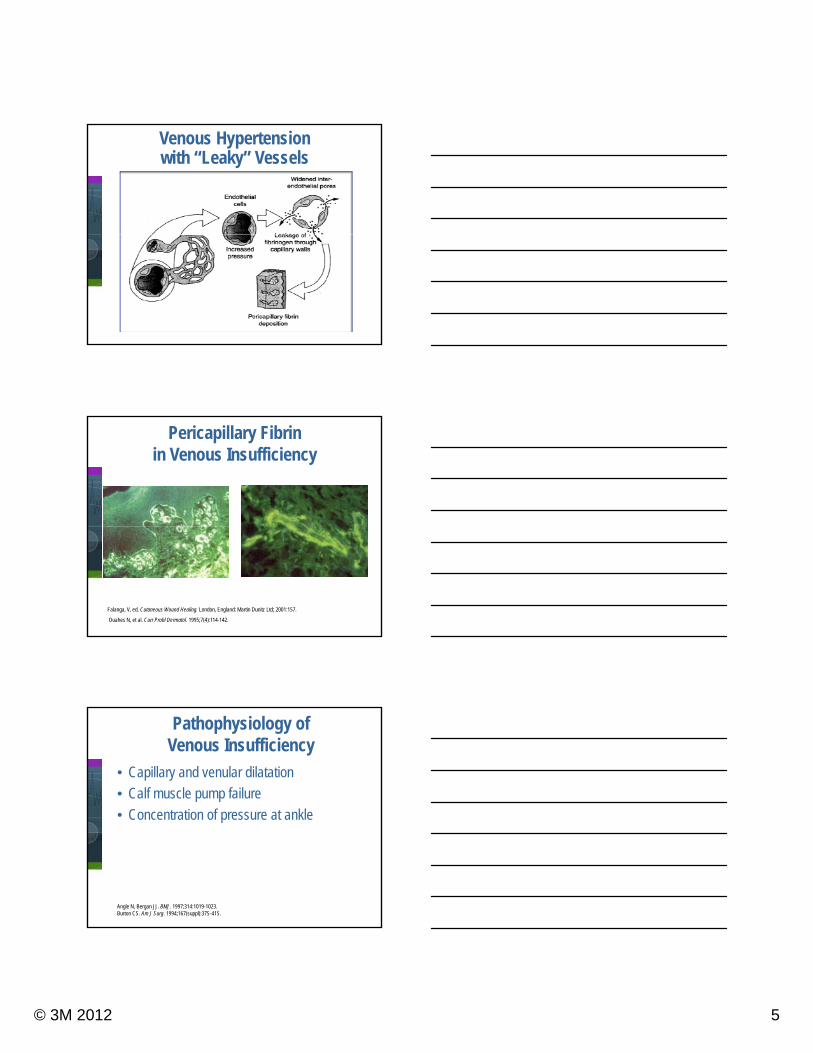
Venous Hypertension with “Leaky” Vessels
Pericapillary Fibrin in Venous Insufficiency
Falanga, V, ed. Cutaneous Wound Healing. London, England: Martin Dunitz Ltd; 2001:157.
Ouahes N, et al. Curr Probl Dermatol. 1995;7(4):114-142.
Pathophysiology of Venous Insufficiency
• Capillary and venular dilatation
• Calf muscle pump failure
• Concentration of pressure at ankle
Angle N, Bergan JJ. BMJ. 1997;314:1019-1023. Burton CS. Am J Surg. 1994;167(suppl):37S-41S.
Concentration of pressure at ankle

© 3M 2012 6
Capillary Pressures at Ankle
• Arterial end ~ 35-100 mm Hg
• Venous end ~ 8-15 mm Hg (1)
• Pressures increase when person pstands—both arterial and venous by average of 100 mm Hg!!! (2)
1) Foldi E, Foldi M. Chronic Venous Insufficiency and Venous-lymphostatic Insufficiency. In: Foldi’s Textbook of Lymphology. 2nd Edition. Munich, Germany: Elsevier; 2006. pp. 434-447
2) Farrow W. Phlebolymphedema—A Common Underdiagnosed and Undertreated Problem in the Wound Care Clinic. Jour Am College of Certified Wound Care Specialists 2010;2:14-23
Development of Edema
Arterial EndVenous End
Normal Circulation
35 mm Hg
8 mm Hg
~30 Liters/day~27 Liters/day
~3 Liters/day
Lymphatics
Development of Edema
Arterial EndVenous End
Increased Arterial Pressure
135 mm Hg
8 mm Hg
>30 Liters/day~27 Liters/day
~3 Liters/day
Lymphatics

© 3M 2012 7
Development of Edema
Arterial EndVenous End
Increased Venous Pressure
35 mm Hg
108 mm Hg
>30 Liters/day<27 Liters/day
~3 Liters/day
Lymphatics
Development of Edema
Arterial EndVenous End
Leaky Capillaries
35 mm Hg
8 mm Hg
>30 Liters/day<27 Liters/day
~3 Liters/day
Lymphatics
Development of Edema
Arterial EndVenous End
Decreased Lymphatic Flow
35 mm Hg
8 mm Hg
~30 Liters/day~27 Liters/day
<3 Liters/day
Lymphatics

© 3M 2012 8
– Macromolecules trap growth factors– Growth factors unavailable to repair or maintain– Leukocytes accumulate and occlude capillaries– Activated leukocytes release toxic metabolites
Complications of Venous Hypertension
y– Free radicals and proteolytic enzymes damage endothelium
Browse NL, et al. Lancet. 1982(8292);2:243-245. Falanga V, et al. Lancet. 1983;341:1006-1008. Coleridge Smith PD, et al. Br Med J (Clin Res Ed). 1988;296(6638):1726-1727.
Capillary Loss with Venous Hypertension
• Prolonged venous hypertension causes damage to and destruction of capillaries in skin 1
• Capillary thrombosis results in decreased number of capillaries in skin and wound bed 1,2,3
1. Junger J, Steins A, Hahn M, Hafner HM. Microcirculatory Dysfunction in Chronic Venous Insufficiency. Microcirculation 2000;7:S3-S12
2.Bollinger A, Jager K, Geser A. Sgier F, Seglias J. Transcapillary and Interstitial Diffusion of Na-Fluorescein in Chronic Venous Insufficiency with White Atrophy. Int J Microcirc Clin Exp 1982;1:5-17
3.Leu AJ, Yanar A, Pfister G, Geiger M, Franzeck UK, Bollinger A. Microangiopathy in Chronic Venous Insufficiency. Dtsch Med Wochenschr 1991;116:447-453
Venous Disease and Ulceration
Edema and Pigmentation Lipodermatosclerosisand Ulceration

© 3M 2012 9
Chronic Venous Disease and Capillary Density
Junger J, Steins A, Hahn M, Hafner HM. Microcirculatory Dysfunction in Chronic Venous Insufficiency. Microcirculation2000;7:S3-S12
Examination of the Swollen Lower Extremity
Medical Conditions
Medicines Venous Disease
Lymphedema
Symptoms Usually none Usually none Heaviness; aching
Heaviness; aching
Bilateral Yes Yes Yes/No Yes/No
Pitting Yes Yes Early-Yes; Late - +/-
No
Skin Changes None None Yes Yes; Can be severe
Location Worse distally Leg; occasionally
foot
Leg; occasionally
foot
Varies but worse distally
Benefit with Elevation
Yes Yes/No Yes Minimal
Adapted from Carson S, Fowler E. Management of Edema. In B Bates-Jensen Ed. Wound Care: A Collaborative Practice
Manual for Health Professionals. 3rd edition. And Bundens WP. The Chronically Swollen Leg: Finding the Cause: Theory and Practice. In Eds JJ Bergan, CK Shortell. Venous Ulcers. Elsevier, Boston, MA. 2007, p. 73
Edema Severity Scale
Depth of Pitting Scale of Pitting
0 to ¼ inch 1+
¼ to ½ inch 2+
½ to 1 inch 3+
> 1 inch 4+
Adapted from Carson S, Fowler E. Management of Edema. In B Bates-Jensen Ed. Wound Care: A Collaborative Practice Manual for Health Professionals. 3rd edition.

© 3M 2012 10
Treatment of Edema
Elevation of Legs? But how high?
http://www.losethebackpain.com/inversion3.html Accessed 8/14/12
Treatment of Edema
Compression!Compression!!
COMPRESSION!!!
Are all compression bandages the same?

© 3M 2012 11
Compression Therapy
• Short stretch or inelastic
• Elastic
1. Single layer
Fletcher A, et al. BMJ. 1997;315(7108):576-580. Cullum N, et al. Cochrane Database Syst Rev. 2000;(3):CD000265. Franks PJ, et al. Wound Repair Regen. 2004;12(2):157-162.
2. Multiple layers
• Higher pressure better than lower pressure
Compression therapy significantly increases healingcompared to no compression
D
Anterior
L
Compartments
Anterior Tibial
Greater Saphenous
Tibia
SuperficialPosterior
DeepPosterior
Lateral
Lesser Saphenous
Dr. HN Mayrovitz
Fibula
Skin
Posterior Tibial
Peroneal
Pressures of Interest
Tibialis m.
Popliteus m
Pe
• Sub-bandage• Surface• Contact
Tibia
Soleus m
Gastroc m.
Popliteus m.Tibialis m.
eroneus
•Tissue•Interstitial
Fibula
• Intramuscular
CompressionBandage or Device
Skin
Dr. HN Mayrovitz

© 3M 2012 12
Resting Pressure
R
Pressure (P) Due to Tension (T) of
Laplace’sLaw
Superficial vessels affected the most
Tension (T) of Bandage and the Radius (R) of the Leg
Dr. HN Mayrovitz
Muscles Contract Bandage
Restricts Muscle
Contraction
Working (Dynamic) Pressure
High Pressure
Develops on Deeper Tissues
Pressure Is From WITHINDr. HN Mayrovitz
Dynamic Pressure Depends on Bandage Material
Form-fitted Steel Pipe
ress
ure
Mayrovitz HN, et al. Clin Physiol. 1997;17(1):105-117.
Bandage “Stretchability”
No External Compression
0
Inelastic(short stretch)
Elastic(long stretch)
Dyn
amic
Pr

© 3M 2012 13
Working vs. Resting PressuresRole of Compression Material
Emptying
ure
(PT)
Emptying
TimeDr. HN Mayrovitz
Tis
sue
Pres
su
TimeDr. HN Mayrovitz Clin Physiol. 1997;17(1):105-117
Control Leg
BeforeBandage
ml/min
Arterial Flow PulsesBelow Knee Blood Flow via Nuclear Magnetic Resonance
Treated Leg
WithBandage
ml/min
Dr. HN Mayrovitz, Univ of Miami
Venous Ulcer99 year old lady with ulcer for 8 months
ABI - 0.45
Informed that BK amputation was the
l thonly therapy
Treated with light compression and bi-layered tissue engineered skin
Wound healed after 47 weeks

© 3M 2012 14
Types of Compression Therapy
Unna’s Boot
The original short stretch compression wrap
2 Layer Compression Bandage
1st Layer Complete CompletedBeginning 2nd Layer

© 3M 2012 15
3 Layer Compression Bandage
4 Layer Compression Bandage
1st Layer 2nd Layery y
3rd Layer 4th Layer Completed
Allergies and Compression Bandages
Allergy to Cotton Wrap Allergy to Elastic Wraps

© 3M 2012 16
Compression Bandage Too Tight Over Bony Prominences
Effective Compression?
• Achieve the appropriate sub-bandage pressure—30-40 mm Hg
• Use the correct techniques
• Use the appropriate materials
Is Effective Compression Therapy Being Used?
• Effective compression therapy—sub-bandage pressure of 30-40 mm Hg.
• Study of compression bandages applied by skilled, experienced wound care nurses p
• 34.9% of compression bandages -- < 20 mm Hg pressure
(56.7% -- applied by nurses with > 10 years experience!)
• 0% of compression bandages -- > 60 mm Hg
Keller A, Muller ML, Calow T, Kern IK, Schumann H. Bandage Pressure Measurement and Training: Simple Interventions to Improve Efficacy in Compression Bandaging. Int Wound J. 2009;6:324-330.

© 3M 2012 17
Sub-bandage Pressure Measurement
Pico Press
Sub-bandage Pressures After Training
• Only 4.8% -- pressures < 20 mm Hg
• 12.7% -- pressures > 60 mm Hg
• 82.5% -- within therapeutic range (30-40 mm Hg)!
Keller A, Muller ML, Calow T, Kern IK, Schumann H. Bandage Pressure Measurement and Training: Simple Interventions to Improve Efficacy in Compression Bandaging. Int Wound J. 2009;6:324-330.
Effective Compression Therapy
PracticePRACTICE
PRACTICE!
With Feedback!!

© 3M 2012 18
Correct Technique
Wrap to the Tibial Tubercle
Always Begin at The Base of the Toes
Not Good!
Oops!
Failure To Wrap All The Way To The The Way To The
Knee

© 3M 2012 19
Failure to Wrap Feet!(Or to the Knees!)
Wrap With Even Pressure
Wrap with Appropriate Materials
1 2 3
Leg Wrapped with Fragments of 3 Bandages!
© 3M 2012 20
Fact: Patients Don’t Like Compression Bandages!
• Only 48.8% of patients wear their compression bandages *
• May be as high as 80% *
• Determinants for NOT wearing compression bandages:g p ga. Age
b. Pain c. Wound sized. Wound depth
* Miller C, Kapp S, Newell N, et al. Predicting Concordance with Multilayer Compression Bandaging. Jour Wound Care 2011;20(3):101-112
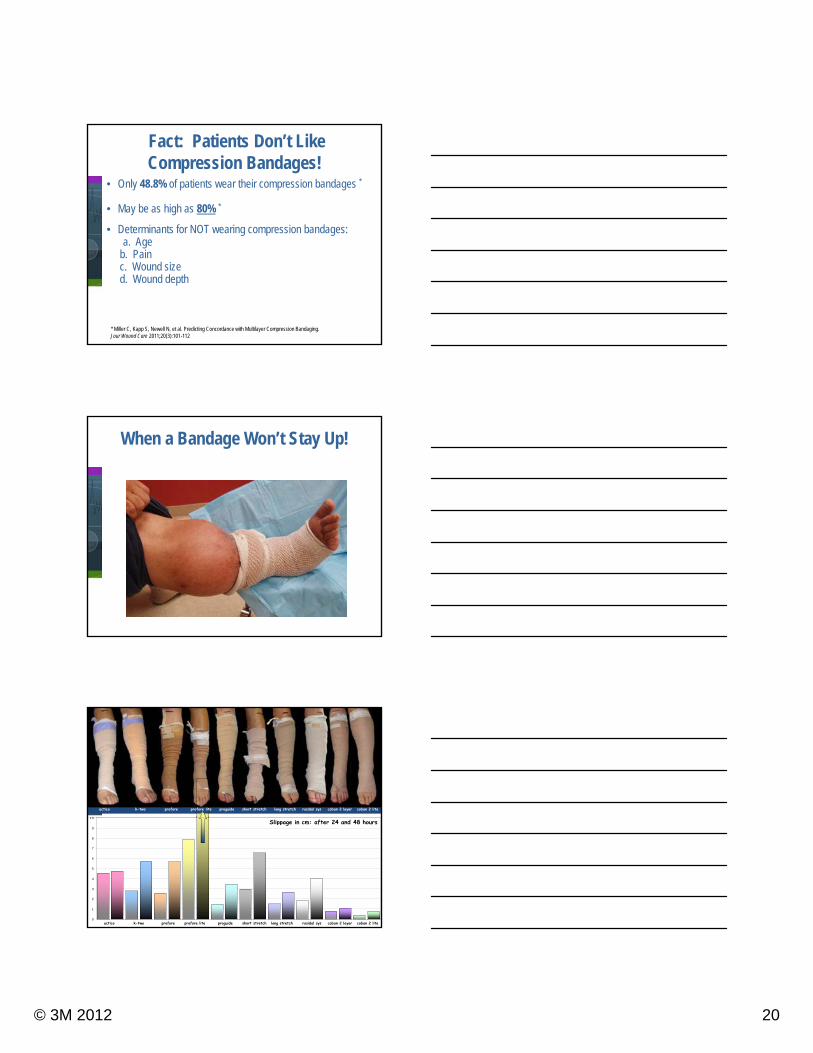
When a Bandage Won’t Stay Up!
10
actico k-two profore profore lite proguide short stretch long stretch rosidal sys coban 2 layer coban 2 lite
0
1
2
3
4
5
6
7
8
9
10Slippage in cm: after 24 and 48 hours
actico k-two profore profore lite proguide short stretch long stretch rosidal sys coban 2 layer coban 2 lite
© 3M 2012 21
Good Therapy?
Sponsored by an educational grant from 3M
For more information on 3M Compression Therapy visit 3M Compression Therapy visit
www.3m.com/coban2layer
3M is a provider approved by the California Board of Registered Nursing, Provider Number CEP 5770. Nurse participants may receive continuing education credit upon completion of education module.