ecmo course 4
TRANSCRIPT

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 1/29
Neonatal Physiology
Teka Siebenaler RRT
Cardiopulmonary Services
University of Minnesota Amplat Children!s "ospital
7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 2/29
#etal $ung Stages of
%evelopment• &mbryonic Stage 'rd()th *eek
• Neural Tube closure
• %iaphragm and lung budformation
• +nternal organs in primitiveformation
stomach, liver, pancreas, gallbladder,
bladder and intestinal loop
• -ascular s stems a ears

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 3/29
• Most congenital malformationsoccur during the .th()th *eeks
• Anencephaly/Spina 0i1da• &2tremity deformities
• %iaphragmatic hernia 3)45 on the
left side6

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 4/29
#etal $ung %evelopment
• 7(89 *eeks the formation of thebronchial tree
• 87(:. *eeks primitive gase2change surface forms
• :.(.; *eeks alveolar development
continues• '4 *eeks stable surfactant
production

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 5/29
Postnatal $ung
%evelopment• Ne*born
– Air*ay branching complete
– Alveolar formation is not complete
Age 8(8; years number of alveoli
increase Age 8; to young adult lung gro*s
larger *ith little alveolar gro*th

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 6/29
#un #acts
• Surfactant is produced by alveolarepithelial cells 3type ++6
• Surfactant production increases :*eeks prior to normal birth
• <e are born *ith on 8/9th the
number of alveoli *e *ill need asan adult=
7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 7/29
Surfactant Replacement• Creates a layer bet*een the
alveolar surface and the alveolargas and reduces alveolar collapse
by decreasing surface tension*ithin the alveoli=
• >iven to patients *ith immature
lungs, MAS, R%S, Pulmonary"ypoplasia and C%" – Curosurf vs= +nfasurf vs= Survanta??

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 8/29
Cardiac #ormation
• 0y :: days a endocardial tube has formed• At :) days aortic roots, primitive left atrium,
pericardial cavity, left ventricle have formed
• 0lood begins to shunt from left to right during the
.th
and 4th
*eeks of development• @Abnormalities in heart formation, the most
common form of human birth defects, aict nearly85 of ne*borns, and their freBuency inspontaneously aborted pregnancies is estimated to
be tenfold higher – "oDman, E=+= +ncidence of congenital heart diseaseF ++= Prenatal
incidence= Pediatr. Cardiol. 89, 844(894 38GG46=

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 9/29
#etal Circulation
• #etal Circulation – H2ygenated blood from placenta via
umbilical vein
– 995 shunted past liver by %UCTUS
-&NHSUS to +-C – 4;5 of this blood shunted from right
atrium to left atrium via #HRAM&N H-A$&
– This blood continues to left ventricle,
ascending aorta, and arteries feeding headand right arm

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 10/29
#etal Circulation cont!d
• -enous blood from head 3S-C6 isdirected via right atrium to right
ventricle into the pulmonary artery• G;5 of blood in PA is shunted a*ay
from lungs and into descending aorta via the %UCTUS ART&R+HUS and
returns to the placenta via theumbilical arteries=

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 11/29

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 12/29
Changes in Circulation, Respiration After0irth
•
Pulmonary vascular resistance decreases afterbirth due toF – +ncreased alveolar and arterial o2ygen tensions, *hich
increase nitric oxide
– $ung e2pansion
– %ecrease in PaCH:
– Increase in arterial pH
• Pulmonary artery pressure decreases belo* systemicpressureI pulmonary blood Jo* increases
• $eft and right ventricles pump in series rather thanin parallel as in the fetal circulatory pattern

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 13/29
@Normal Circulation• Closure of Umbilical arteries */in
minutes after birth
• $igation of umbilical vein
3clamped cord6
• Closure of P%A 3minutes to days6
• Closure of #oramen Hvale due toincreased pressure in $eft Atriumand %ecreased pressures in Right
Atrium

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 14/29
3PP"N6
–
Hccurs in : out of every 8,;;; bornlive infants
– Complicates the course of 8;5 ofinfants *ith respiratory distress
– Typically seen in infant!s K'. *eeks – More common in babies that *ere
hypo2ic and acidemic around the
time of birth 3-enous cord Ph L7=:;and 0& ()6
– More prevalent in infants *hosemothers took NSA+%S or SSR+!s
during the 'rd trimester

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 15/29
• @%ue to a patent foramen ovale and
patent ductus arteriosus, *hich arenormally present early in life, elevatedpulmonary vascular resistance in thene*born produces e2trapulmonary
shunting of blood, leading to severeand potentially unresponsivehypo2emia= <ith inadeBuate pulmonaryperfusion, neonates are at risk for
developing refractory hypo2emia,respiratory distress, and acidosis=
» Robin Steinhorn, M%

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 16/29
Cardiac Complications• Persistent
pulmonaryhypertension
• Normal Circulation

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 17/29
PP"N•
' typesF• Result of abnormally constricted
pulmonary vasculature due to lungparenchymal diseases leading tohypo2ia 3mec aspiration,pneumonia, R%S6
• +dopathic 38;(:;5 of all aDectedinfants6
• Pulmonary hypoplasia orstructural defects 3C%", PRHM6

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 18/29
"o* do you kno* it is
PP"N• Cyanosis
• Tachypnea
•
>runting• Pre/post ductal split
• "ypo2ia/hypercapnea/acidosis
•
Response to o2ygen and iNH• Cardiac Ultrasound

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 19/29
Treatment for PP"N• H2ygen therapy
• +nhaled Nitric H2ide
• Normal $ab -alues
• 0lood Pressure support if needed
• Mechanical -entilation
•
&CMH• Time

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 20/29
PP"N and &CMH• Can be -(A or -(- &CMH
• Typically a short run 3'(4 days6
• Survival rates greater than 9)5 ascompared *ith .;5 in infants treated*ith conventional non(&CMH therapy
• Patient needs time for the
pulmonary vasculature to rela2and for the patient!s heart is ableto pump blood to the lungs

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 21/29
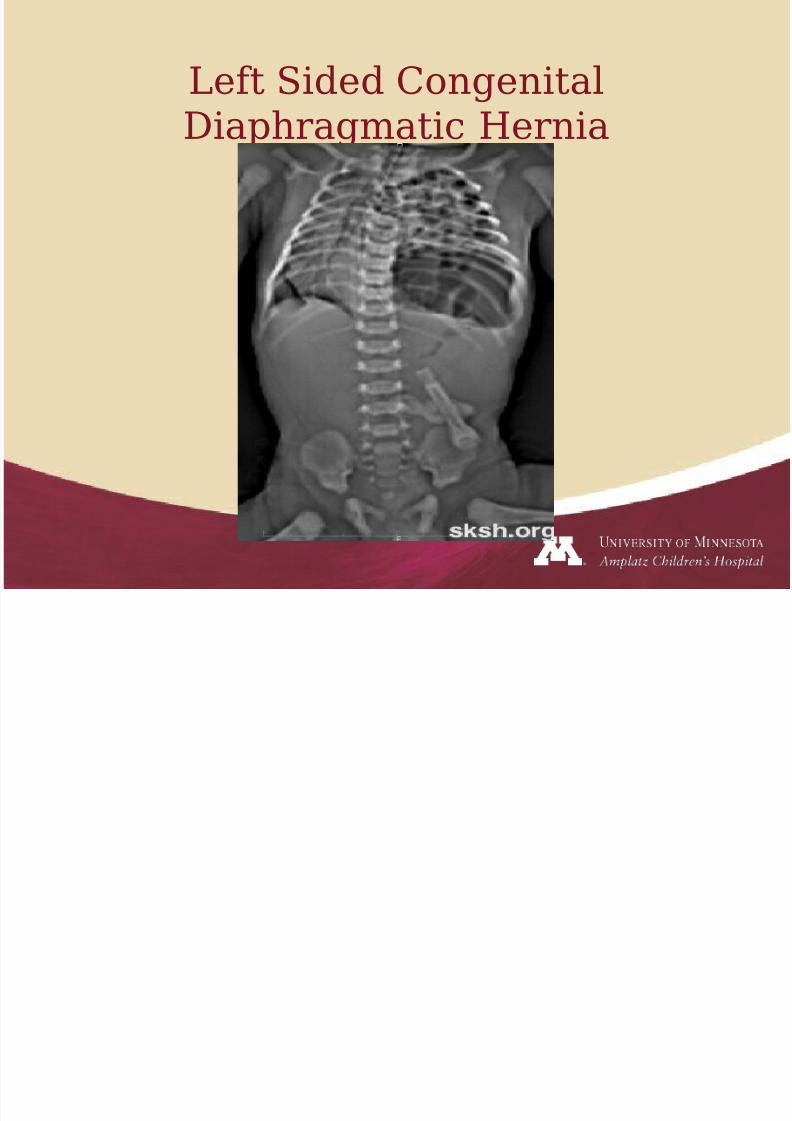
Congenital %iaphragmatic
"ernia• Hccurs in 8 of every :;;;(';;;live births and accounts for )5 ofall maOor congenital anomalies=
Mortality rates are :4(9;5====• The diaphragm initially develops
as a septum bet*een the heart
and liver, progressesposterolaterally, and closes at theleft 0ochdalek foramen at
appro2imately )(8; *eeks

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 22/29
• A severe C%" is believed to occur
during the pseudoglandular stageof lung development= <eeks 7(87and this is *hen pulmonary
circulation develops=• $ung compression results in
pulmonary hypoplasia 3both lungs
may be abnormal6= Pulmonaryhypoplasia is associated *ithfe*er bronchial generations,alveoli, and arterial generations=
7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 23/29
$eft Sided Congenital
%iaphragmatic "ernia

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 24/29
$eft C%"

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 25/29
C%" and &CMH
• Typically -A &CMH• Can be a diDicult cannulation due
to small vessels and cardiac
anatomy• Average run time 8)8(8G7 hours
and 4;5 of patients *ith a C%"
are treated *ith &CMH• Patients are often decannulated
and immediately repaired on the
N+CU

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 26/29
&CMH and Respiratory
#ailure• Meconium Aspiration Syndrome
• Sepsis
• Pneumonia
• Alveolar Capillary %ysplasia
QQQQAll have a component ofPP"NQQQQQQ

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 27/29
Alveolar Capillary
%ysplasia• -ery rare lethal congenital
anomaly
• #ailure of formation of the normalair(blood diDusion barrier in thene*born lung= Alveolar Capillary
%ysplasia is usually associated*ith misalignment of thepulmonary veins=

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 28/29
• Patient *ill not repond tomechanical ventilation, iNH or
&CMH• 745 of these patients *ill have
other organs aDected
• $ongest reported survival is :months post &CMH run

7/23/2019 Ecmo Course 4
http://slidepdf.com/reader/full/ecmo-course-4 29/29
• uestions