echocardiographic assessment of the right ventricle...
TRANSCRIPT

Echocardiographic assessment of
the right ventricle in paediatric
pulmonary hypertension.
Mark K. Friedberg, MD
No disclosures

Outline
• RV response to increased afterload
• Echo assessment of RV function in PAH – 2-D
– Annular motion: M-mode, TDI
– Myocardial function
– Ventricular-vascular coupling
• Both systole and diastole are important
• Both the RV and LV are important

The RV response to increased afterload determines outcomes
Pulmonary Circulation 2017; 7 361–371
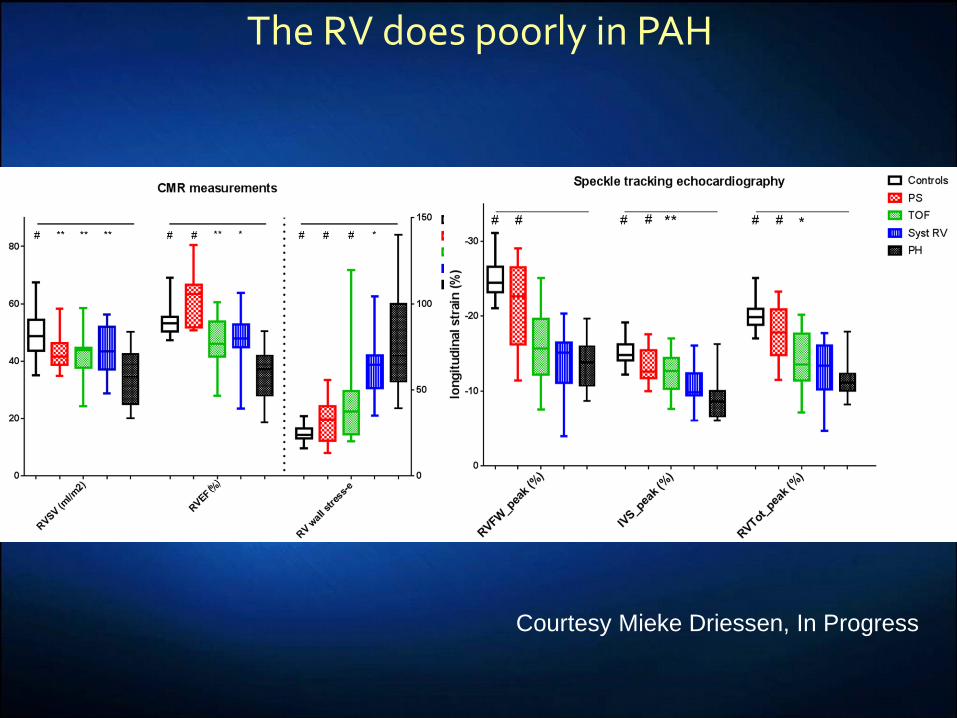
Courtesy Mieke Driessen, In Progress
The RV does poorly in PAH

RV function • 2 layers
– Superficial layer
• Circumferential
– Deep layer:
• longitudinal
• Longitudinal shortening
• Inward (bellows) free wall
motion.
• inlet to outlet propulsion
RV Free
Wall
IVS

Physiology of the hypertensive RV
Chin, Coronary Artery Disease
2005, 16:13–18
Anderson, Semin Thorac Cardiovasc Surg
Pediatr Card Surg Ann 2007 10:76
RV Free
Wall
IVS
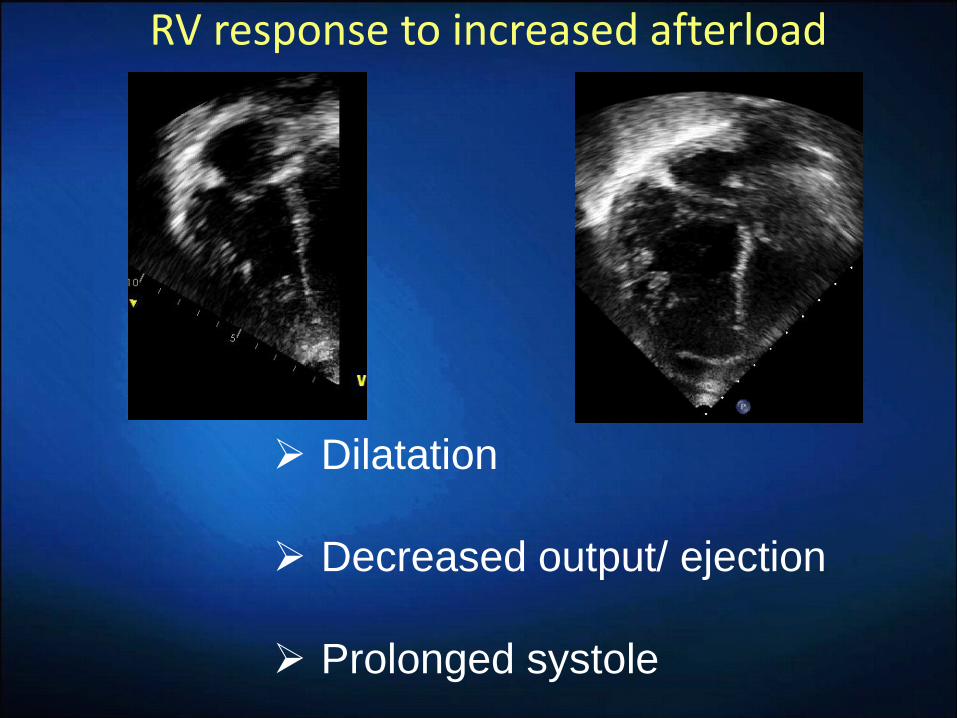
RV response to increased afterload
Dilatation
Decreased output/ ejection
Prolonged systole

RV dimensions
Lopez, J Am Soc Echocardiogr 2010;23:465-95

RV dimensions

RV/LV ratio
Jone PN,. J Am Soc Echocardiogr (2014) 27:172–8.

3-D assessment of RV volumes and EF
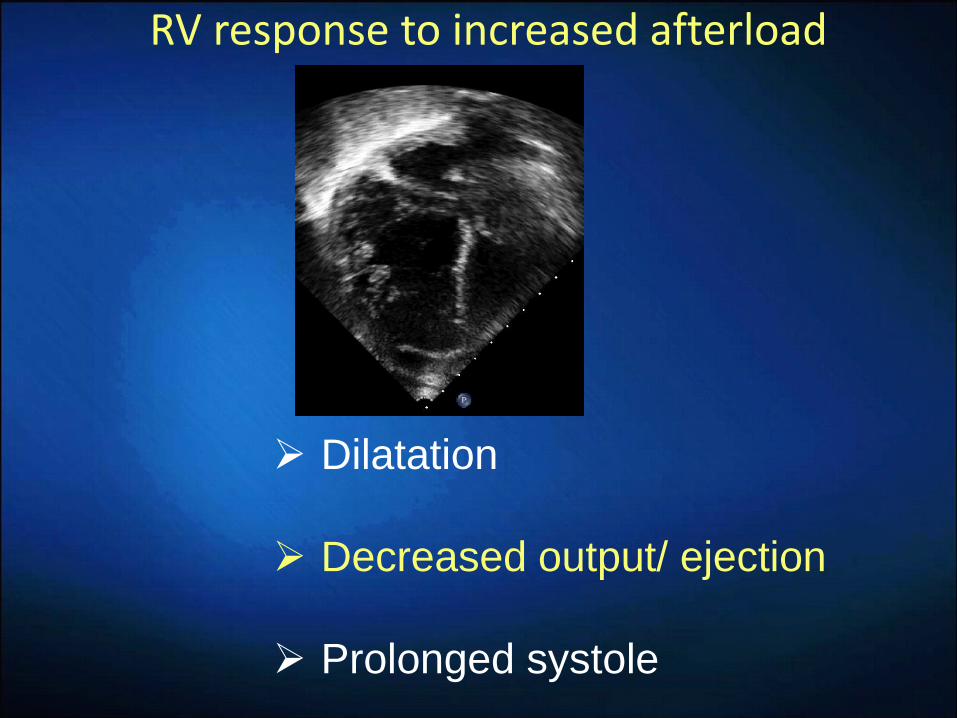
RV response to increased afterload
Dilatation
Decreased output/ ejection
Prolonged systole

Subjective (Eyeball) assessment still most common method
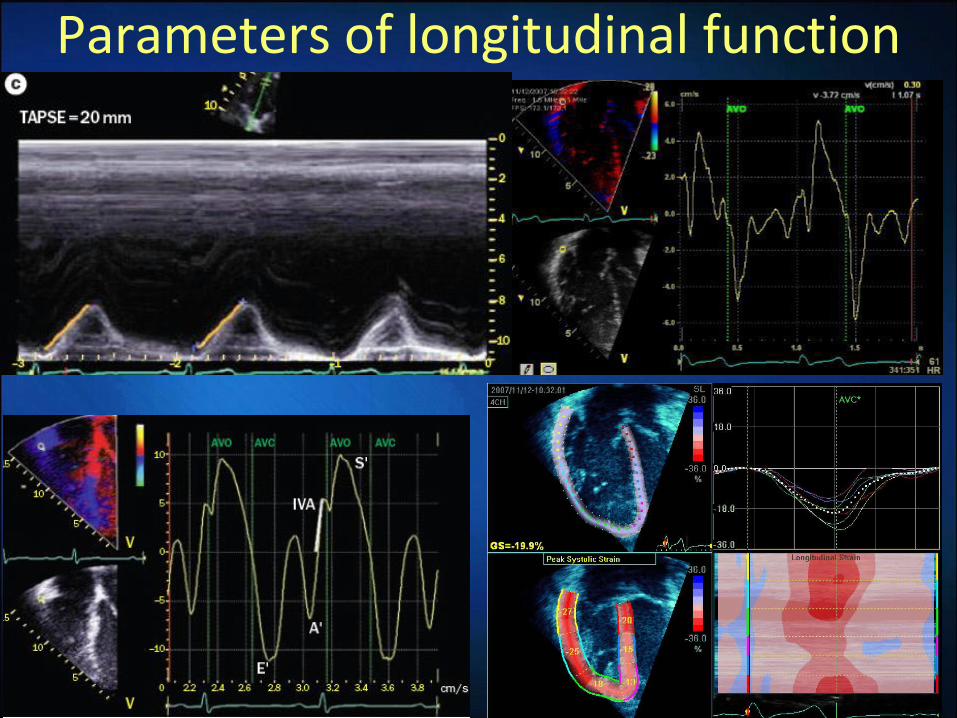
Parameters of longitudinal function

Tricuspid annular plane systolic excursion (TAPSE)
Koestenberger, JASE 2009

Forfia, Am J Respir Crit Care Med, 2006 174:1034
TAPSE correlates with survival

Early Decline in TAPSE Predicts Outcome in Children With Pulmonary Hypertension
0 5 1 0 1 5
0
5 0
1 0 0
S u rv iv a l B y T A P S E a t D ia g n o s is
Y e a rs
Pe
rc
en
t s
urv
iva
l
Z -s c o re > -4
Z -s c o re 4
0 5 1 0 1 5
0
5 0
1 0 0
S u rv iv a l B y T A P S E a t D ia g n o s is
Y e a rs
Pe
rc
en
t s
urv
iva
l
Z -s c o re > -4
Z -s c o re 4
Hauk, Euroecho, 2014
IPAH (18)
PH-CHD (25)
Lung disease (5)

13y, iPAH, PAH worsening, pneumonia

Tricuspid tissue Doppler velocities
Lammers, J Am Soc Echocardiogr 2012;25:504

Tissue Doppler Imaging: Severe PAH

TAPSE pitfalls: Pre-tricuspid Eisenmenger
Normal TAPSE Low FAC% due to apical dysfunction

Fractional area of change
Mertens & Friedberg. Nat. Rev. Cardiol, 2010

RV apical remodeling Control
Pulmonary stenosis
Pulmonary Hypertension
Driessen, Echocardiography 2017

PS patients do better than PAH
• 16 PS pts (10.3±4.7 yrs), 18 iPAH pts (10.8±5.6 yr) and 18 controls (11.2 ± 5.0 yrs).
• RV: LV pressure ratio: 0.71 [0.41-1.57] mmHg in PS and 1.09 [0.46-1.50] in iPAH (p=0.004).
Driessen, Physiological Reports, 2017

RV contraction under stress
Increased circumferential/ radial thickening
ccTGA HLHS PAH
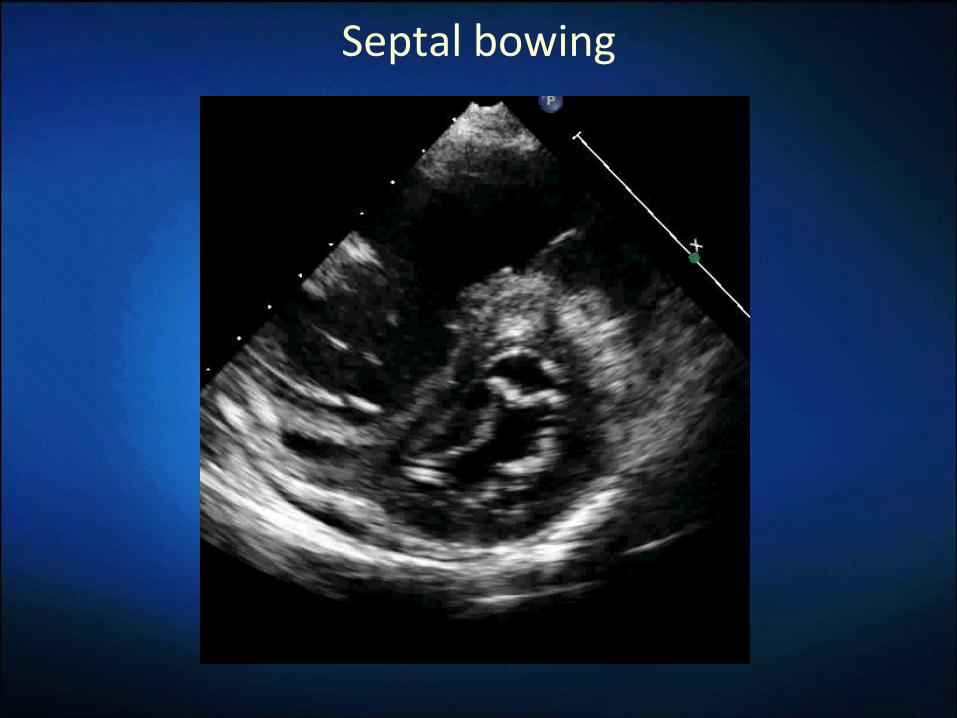
Septal bowing

Inefficient RV transverse motion PS PAH
RV Free
Wall
IVS
Driessen, Physiological Reports, 2017
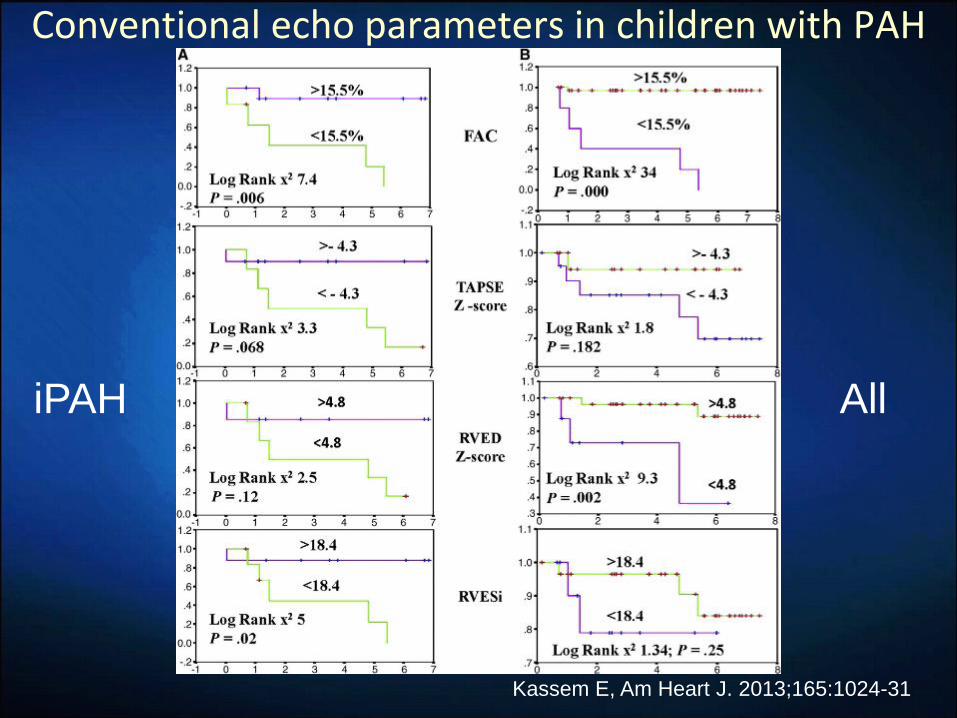
Conventional echo parameters in children with PAH
Kassem E, Am Heart J. 2013;165:1024-31
iPAH All

Strain and strain rate
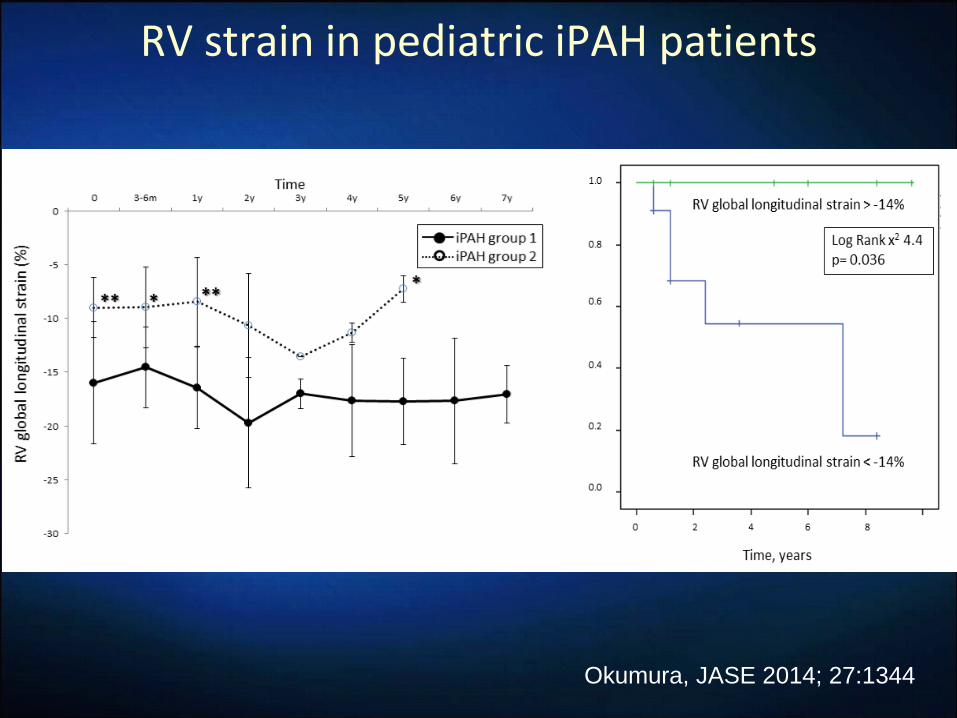
RV strain in pediatric iPAH patients
Okumura, JASE 2014; 27:1344

Tricuspid Pulmonary
Systolic prolongation and MPI

The S:D Duration ratio
Friedberg, JASE, 2006;19:1326

S:D ratio in PAH
Alkon, Am J Cardiol 2010;106:430

13y, iPAH, pneumonia, PAH worsening

Another 13 year old with PAH

Prolonged RV systole=reduced RV and LV filling

Further deterioration

12 year old severe iPAH

Right atrial size
Bustamante-Labarta, JASE 2002;15:1160
Diastolic function
Kassem E, Am Heart J. 2013;165:1024-31
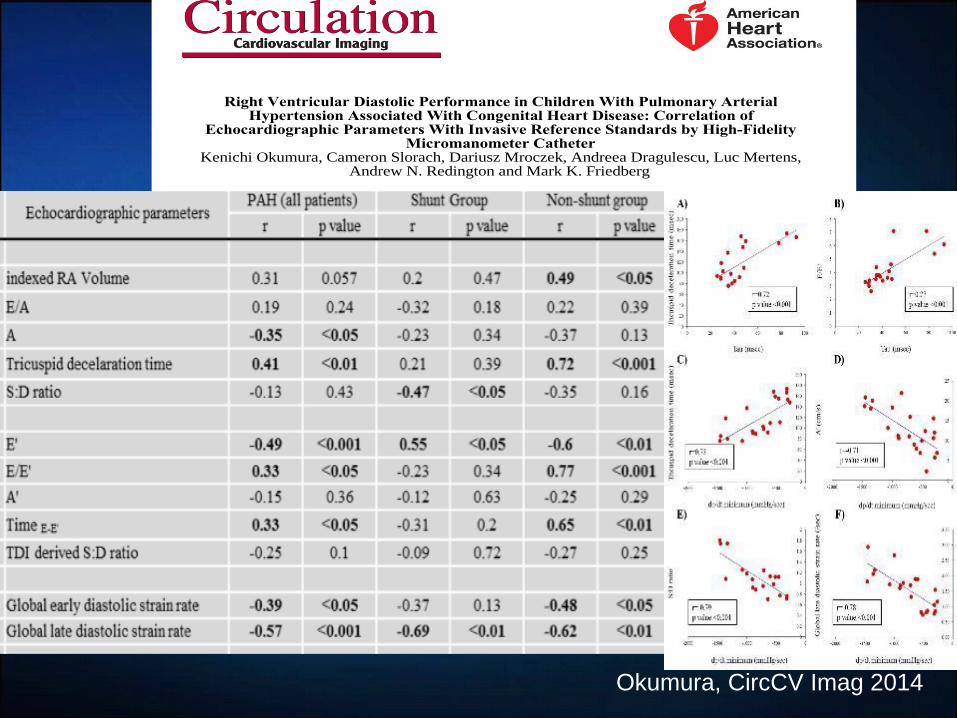
Okumura, CircCV Imag 2014
Andrew N. Redington and Mark K. FriedbergKenichi Okumura, Cameron Slorach, Dariusz Mroczek, Andreea Dragulescu, Luc Mertens,
Micromanometer CatheterEchocardiographic Parameters With Invasive Reference Standards by High-Fidelity
Hypertension Associated With Congenital Heart Disease: Correlation of Right Ventricular Diastolic Performance in Children With Pulmonary Arterial
Print ISSN: 1941-9651. Online ISSN: 1942-0080 Copyright © 2014 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Imaging
doi: 10.1161/CIRCIMAGING.113.0010712014;7:491-501; originally published online February 27, 2014;Circ Cardiovasc Imaging.
http://circimaging.ahajournals.org/content/7/3/491
World Wide Web at: The online version of this article, along with updated information and services, is located on the
http://circimaging.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Imaging Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Imagingin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 20, 2014http://circimaging.ahajournals.org/Downloaded from by guest on May 20, 2014http://circimaging.ahajournals.org/Downloaded from

Future directions
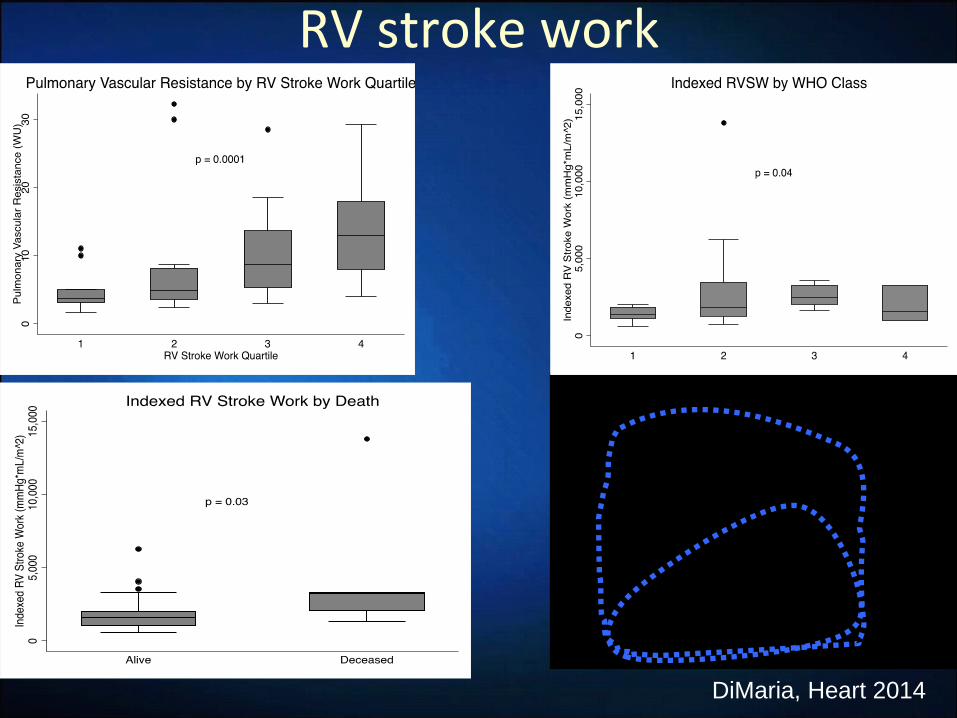
RV stroke work
DiMaria, Heart 2014
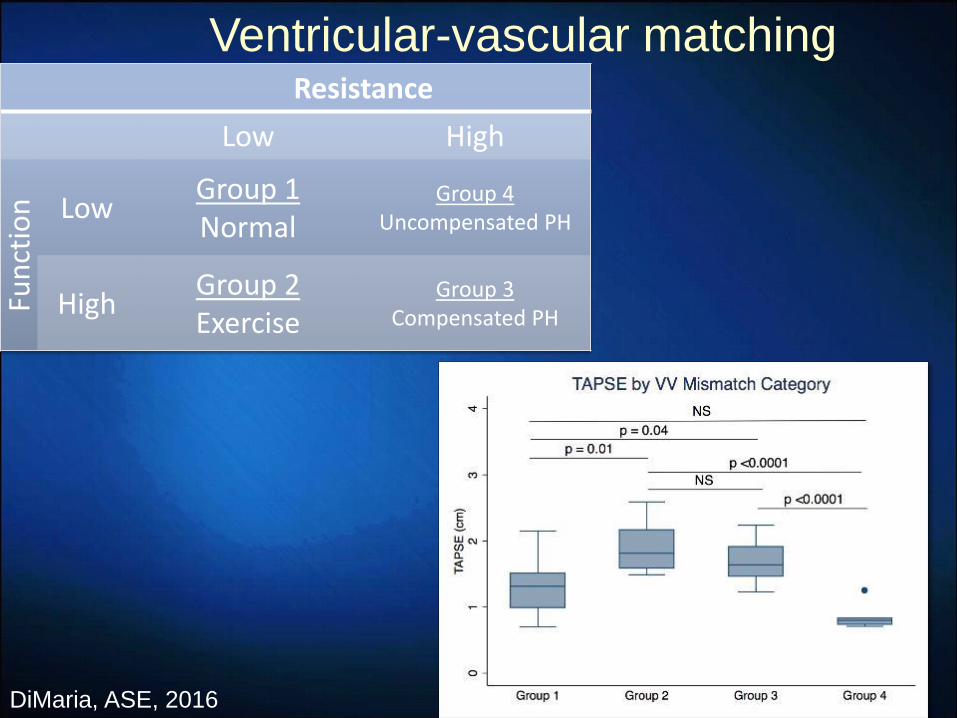
Resistance
Low High
Fun
ctio
n
Low Group 1 Normal
Group 4 Uncompensated PH
High Group 2 Exercise
Group 3 Compensated PH
Ventricular-vascular matching
DiMaria, ASE, 2016

Courtesy Siri-Anne Nayrnes
4-D flow in a PAH patient

RV response to exercise
Baseline 60 watts
Pieles, In Progress

Summary • Assessment of RV function is important to assess for
RV decompensation.
• It is important to qualitatively evaluate RV function as well as use quantitative measures
• Newer methods can be combined with conventional ones for more comprehensive evaluation.
• Further validation of newer methods is needed (especially in terms of increased sensitivity).

Thank you