echo potpourri part iv case, cases, and more cases! · 66 year old male bicuspid aortic valve...
TRANSCRIPT
Echo Potpourri Part IV
Case, Cases, and More Cases!

Lorraine Chubet, RDCS
St. Francis Hospital and Medical Center

66 year old male
Bicuspid Aortic Valve replaced with a St. Jude valve in December, 2009.
No significant coronary artery disease
Previous echo done at another hospital prior to valve replacement showed LVH, severe AS, and ejection fraction of 45%.

BP of 150/100 mmHg
Heart rate of 90 bpm
Clear Lungs
Grade 3/6 systolic ejection murmur
Remainder of exam normal






There was mild perivalvular aortic regurgitation
Mild MR, mild TR, no PI.
LVEF estimated 40% to 50%
No intracardiac shunt was detected by contrast study with agitated saline
No LAA thrombus
A Cor-triatriatum was present in the LA
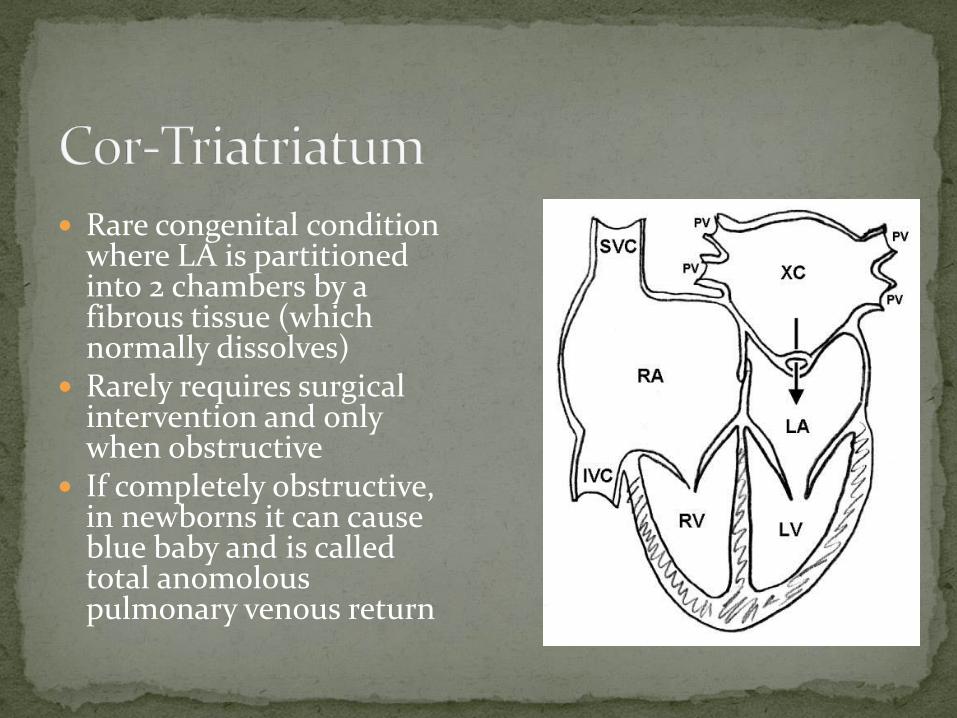
Rare congenital condition where LA is partitioned into 2 chambers by a fibrous tissue (which normally dissolves)
Rarely requires surgical intervention and only when obstructive
If completely obstructive, in newborns it can cause blue baby and is called total anomolous pulmonary venous return

Mollie Boucher BS, RDMS
Student at SFHMC
School of Cardiac Ultrasound
71 year old female arrives at SFH Emergency room
Patient had episode of syncope escalating in patient collapse
BP: 116/73
Temperature 97.4
Sp O2 100%
Pt presents with “LOUD” Murmur

No acute distress
Chest Clear auscultation
No carotid bruits
No Edema

EKG:
Contrast Enhancing Agent


Patient Brought to Cath Lab…
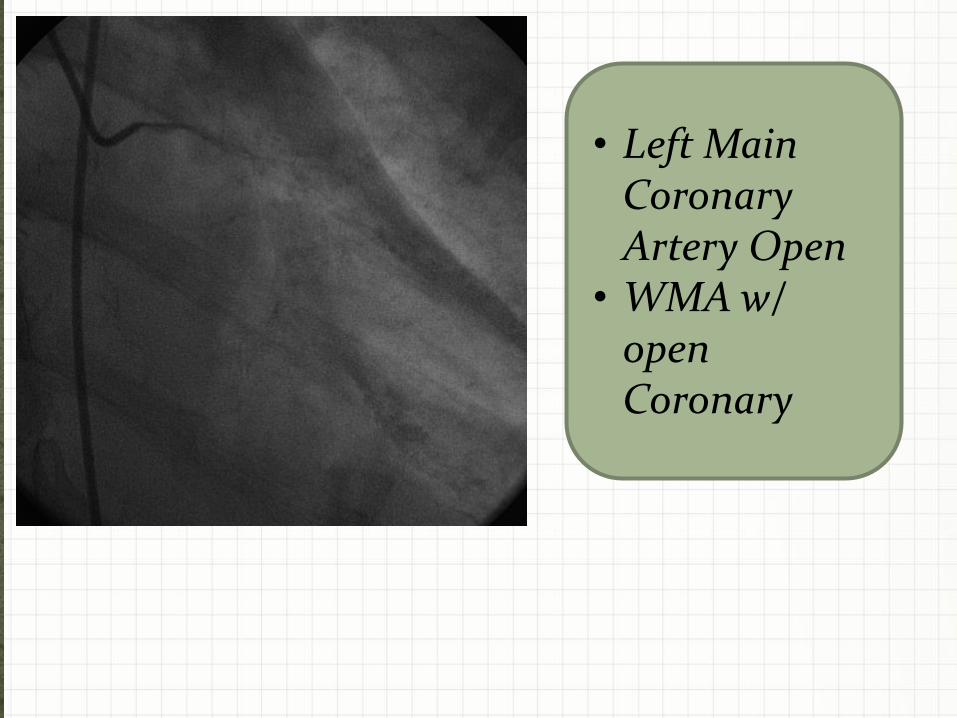
• Left Main Coronary Artery Open
• WMA w/ open Coronary

• Cath Lab
• RCA Open
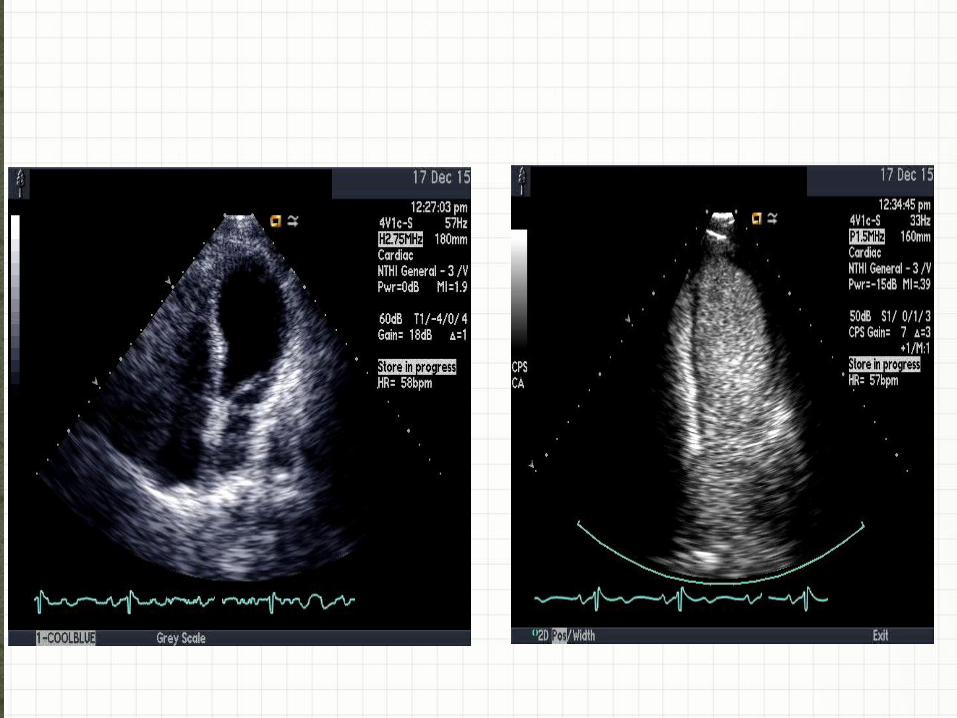
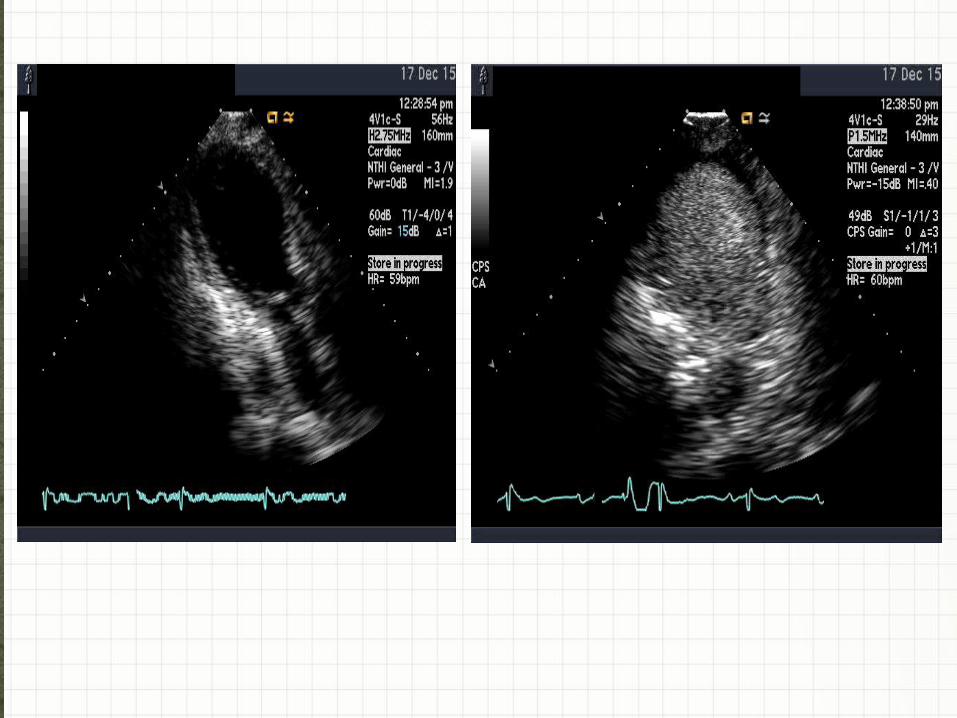
Y • Hyperkinetic Basal Segment
• Hypokinetic Mid Cavity
Y • Normal Motion in Apex
• Coronary Arteries are open
Y • What Do you Think???
Lets Make Diagnosis #1!

• Acute HF precipitated by sudden
intense, emotional or physical stress
• Apical Ballooning- does this patient?
• Reduced Ejection Fraction
• Mid Wall motion abnormalities
• Preserved basal and apical function
• Symptoms mimic acute coronary
syndrome
• Coronary arteries open
• Variations of Takotsubo

Mid- Ventricular Variant of TC
• Open Coronary Arteries
• Hypokinesis of Mid Ventricle
• Hyperkinesis of Apical & Basal segments
• Several different Mechanisms causing this
variant
• Loss of estrogen, catecholamine,
coronary artery spasm, LVOT
obstruction
KEEP THESE IN MIND!


Pulse – Wave Mapping

• LVOT CW quantified
• Dagger
• AS? LVOT?
• Gradient
~40 mm/hg
Almost 4m/s
• Pt performed
valsalva maneuver
and gradient stayed
the same!
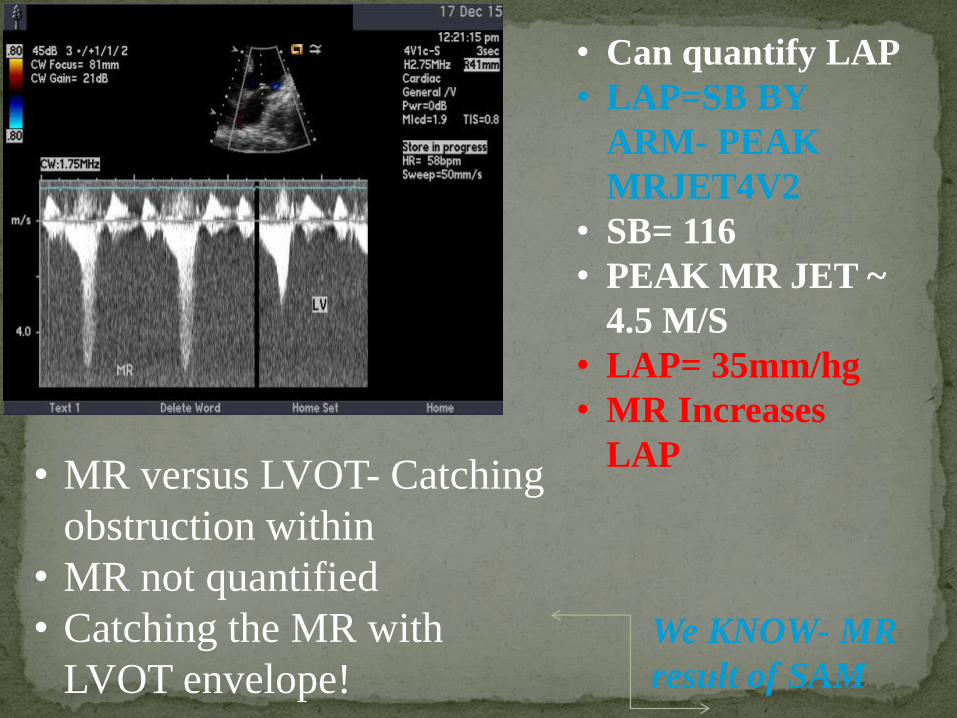
• MR versus LVOT- Catching
obstruction within
• MR not quantified
• Catching the MR with
LVOT envelope!
• Can quantify LAP
• LAP=SB BY
ARM- PEAK
MRJET4V2
• SB= 116
• PEAK MR JET ~
4.5 M/S
• LAP= 35mm/hg
• MR Increases
LAP
We KNOW- MR
result of SAM
ECHO REPORT:
• DECREASED EF 25-35%
• Moderate Mitral Regurgitation
• LA Volume index is normal
• Dynamic subvalvular LVOT
obstruction 40 mm/hg gradient
• With Valsalva 41 mm/hg Gradient
• Normal Right ventricular function
• TR peak Gradient 18.3 mm/hg
Dynamic
outflow
obstruction
40 mm/hg
subaortic
pressure
gradient
PW
doppler
througho
ut LV
Treatment
Hospitalized
until LV
function
restored
Hospitalized until LV function restored
Beta Blockers, ACE inhibitors for heart
muscle recovery
Anti-Anxiety medication- prevent release of stress
hormones

Patient presents with nausea and vomiting for 4 days
Previous chest discomfort 6 days prior
Cardiogenic shock blood pressure 73/52




What is the RVSP?
Wait don’t we already have all the information
Blood Pressure 73/52
TR Jet estimated RVSP was 41 mmHg



Admitted Sunday, January 12, 2014 to St. Francis Hospital ED
Male
61 years old
Flu-like symptoms for the last two weeks, which consisted of fever, cough and nausea
Extremely fatigue for the past two days prior to admission at St. Francis Hospital, along with weakness and dyspnea upon exertion
Inferior wall ST elevation
Decompensated CHF
Holosystolic murmur

Works in construction/home remodeling
Smokes two packs of cigarettes/day for the last 45 years
His father had a MI at 65 years old
The first echo was done on Sunday, January 12, 2014
It was a STAT echo, completed by a fellow

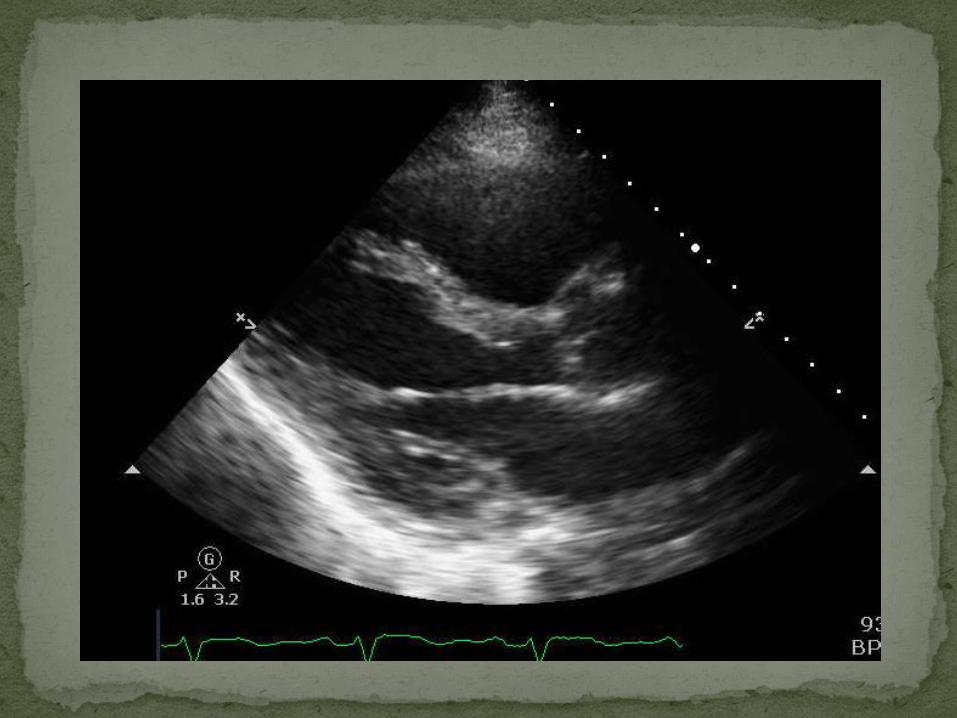
What do you see?
Size and function of chambers?

What do you see?
Regurgitation? If so, where
and how much?
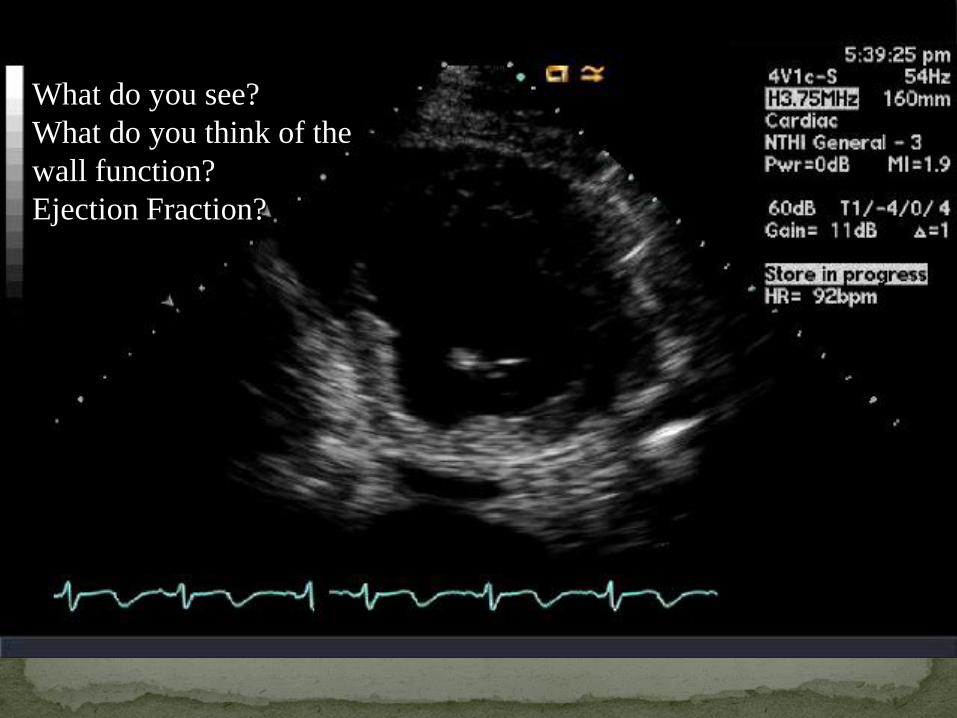
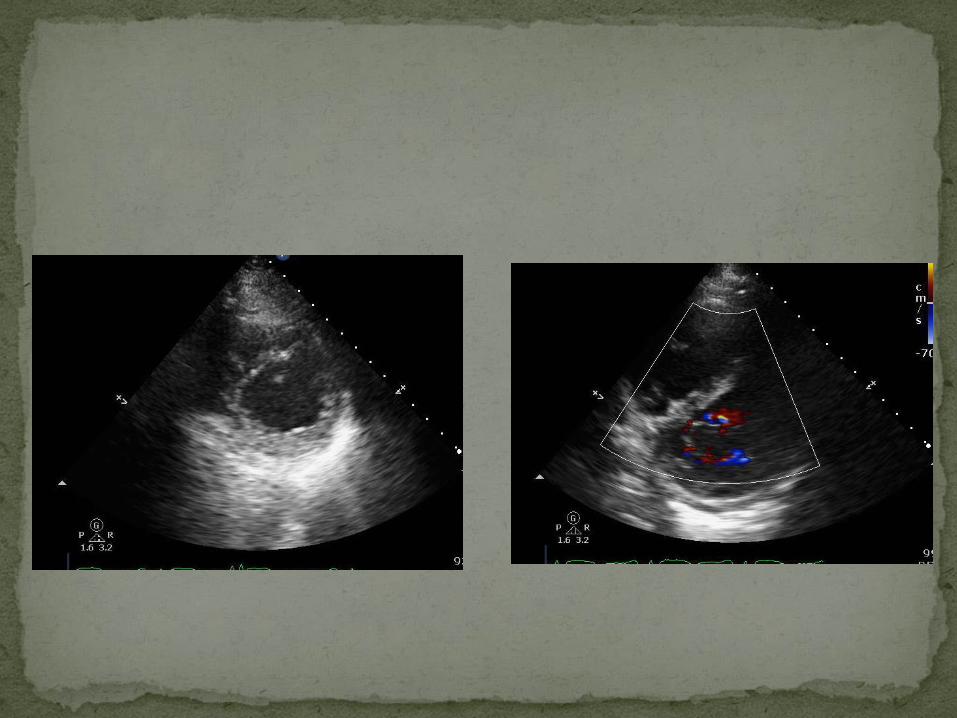
What do you see?
What do you think of the
wall function?
Ejection Fraction?

What do you think about
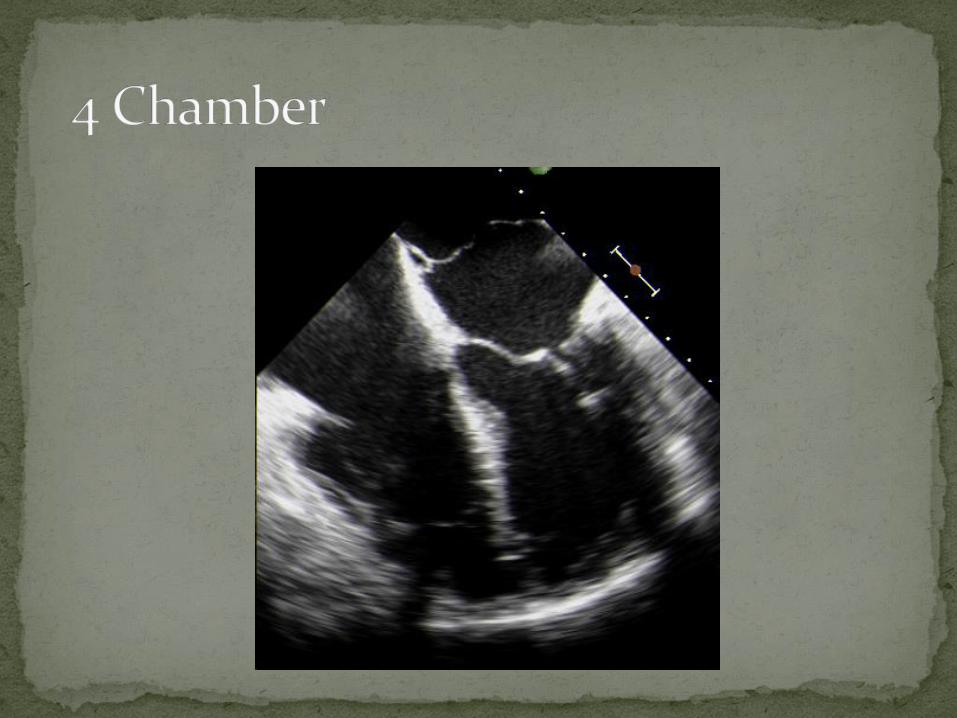
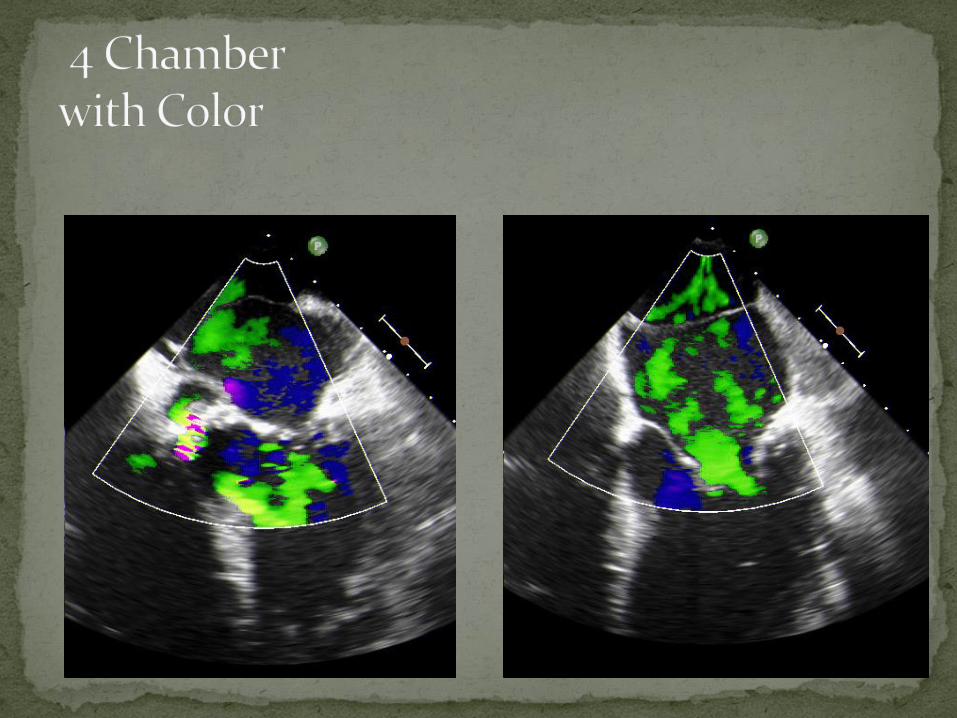
the color flow?
What do you think might
be happening?

What do you see?
Size and function of the
chambers?
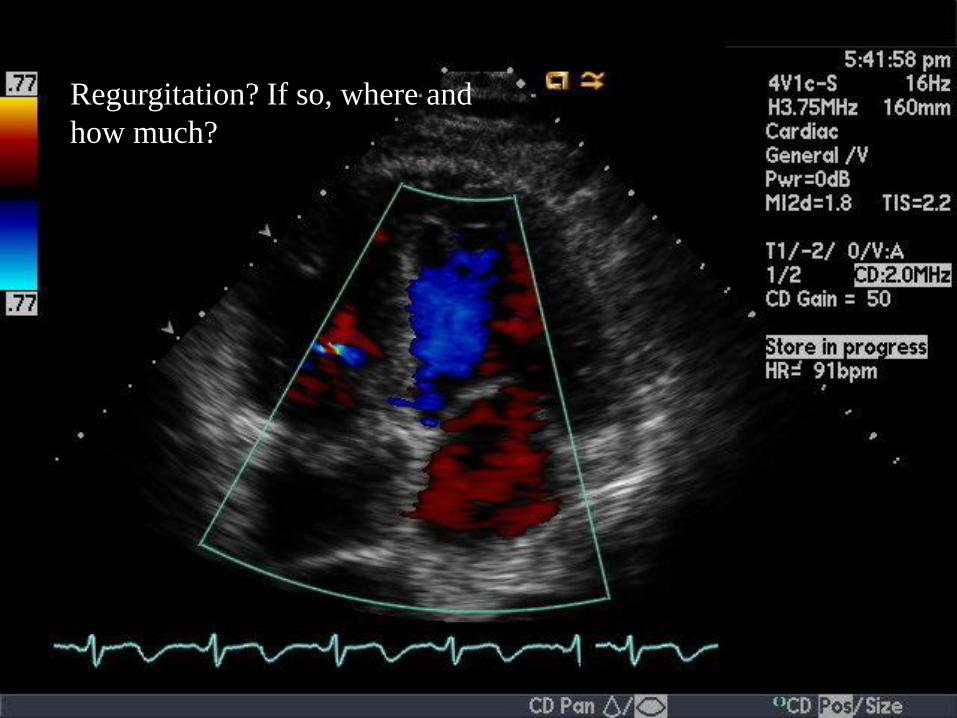
Regurgitation? If so, where and
how much?
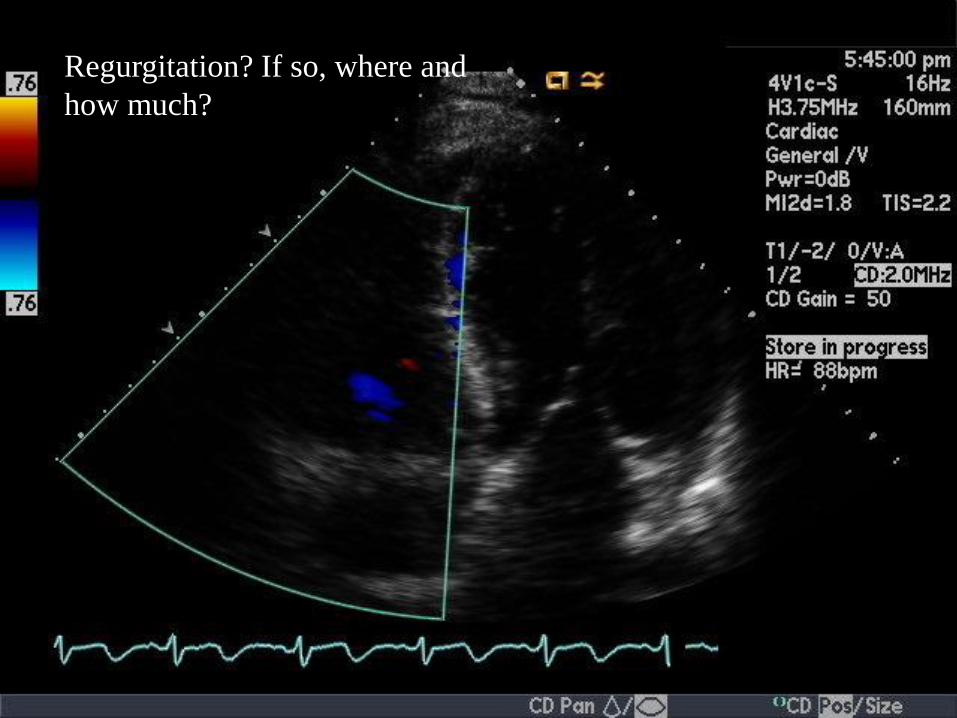
Regurgitation? If so, where and
how much?

Ventricular Septal Defect (VSD) Muscular (Trabecular) – 2nd most common in
adults
Wall Abnormalities (MI occurred) Severe hypokinesis of inferior and infero-septal
walls
Mild LVH and RVH
Dilated RA
Mild MR (+ some MV thickening)
Mild to moderate TR (+ some TV thickening)
Reduced right ventricular global systolic function
40% EF
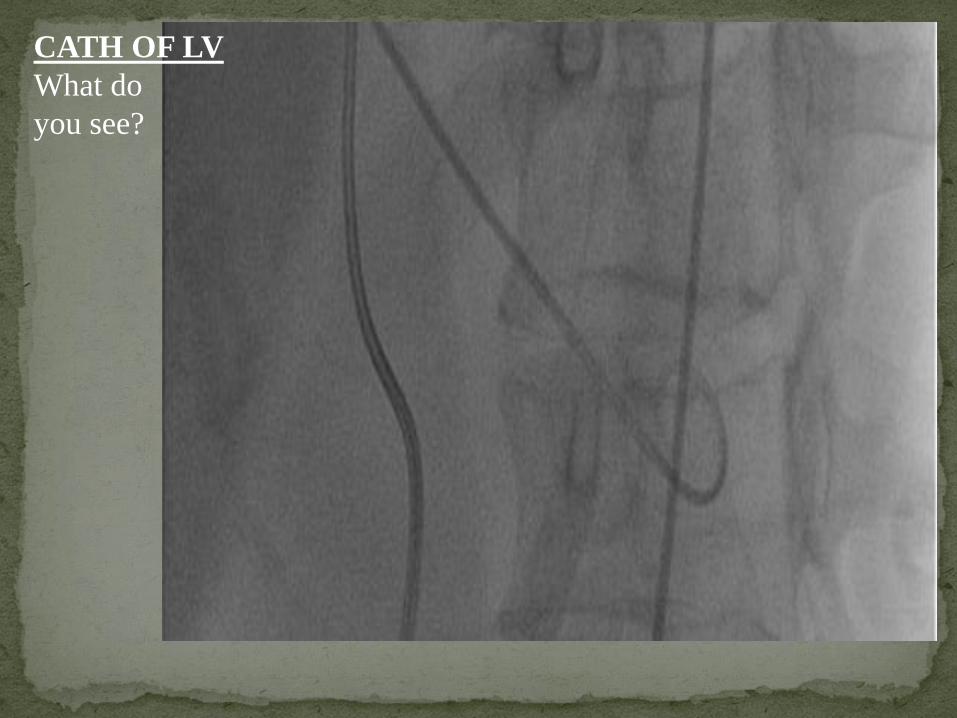
CATH OF LV
What do
you see?

Cath showed occlusion of RCA, You can also see both sides of the heart fill with dye, which confirms that there is a VSD
This makes sense, since the patient experienced a MI and VSD
SIDENOTE: The Cath was actually done FIRST, but for the sake of the presentation

Operation to repair the muscular VSD was done on Monday, January 13, 2014, which was one day after echo findings Hemashield graft was seated and sutured
Pacing wires were placed in the right atrium and right ventricle to help control abnormal heart rhythms like A-Fib and tachycardia
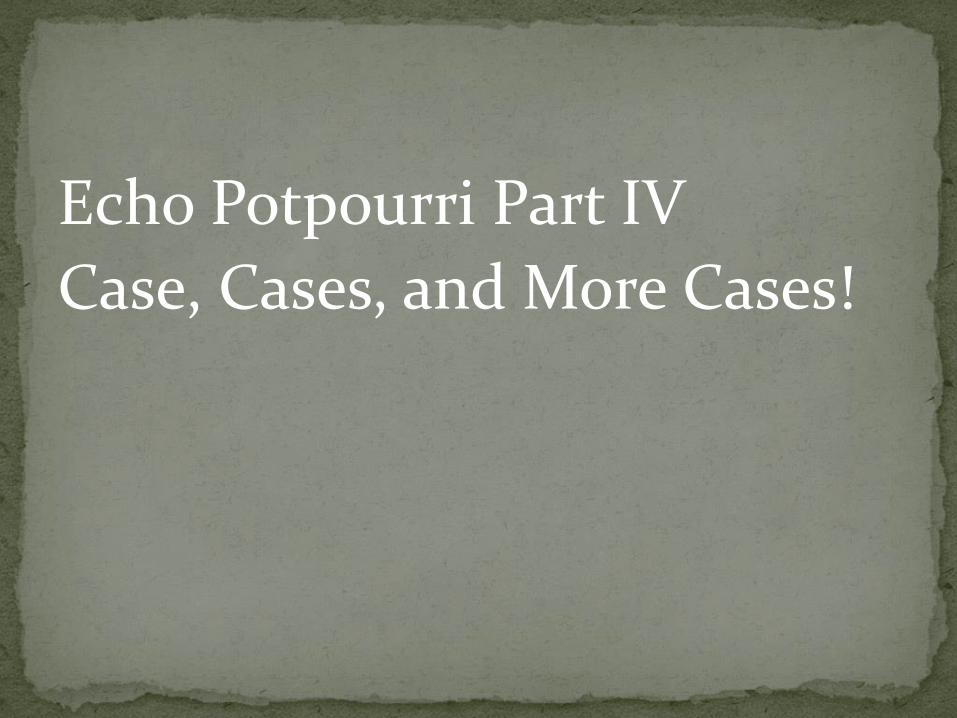
TEE was performed in the OR to check on VSD; it was confirmed that there was no residual VSD
Patient was discharged on Friday, January 17, 2014
Patient was given: Aspirin – Relieves pain and is an anti-inflammatory
Statin – Lowers cholesterol
Beta blockade – Usually given after MI and to prevent another MI from occurring
ACE inhibitor - Treatment of hypertension (elevated blood pressure) and congestive heart failure. Lowers BP
Patient was re-admitted on Sunday, January 19, 2014, just two days after hospital discharge
Now present with:
Acute respiratory failure
Severe pulmonary edema
Cardiogenic shock
Tachycardia

The second echo was done on day of re-admission
It was a STAT echo
By Hadley Santos BS, RCS

What do you
see?
Size and
function of
chambers?

What do you see?
Regurgitation? If so, where and
how much?

What do you see?
What do you think of the
wall function?

What do you see?
Size and function of
chambers?

Size and function of chambers?
Regurgitation? If so, where and
how much?

What do you think of the envelope?
What is the severity?

What do you see?
Size and function of chambers?
Regurgitation? If so, where
and how much?
TR Peak Gradient = 56.8 mmHg
Right Ventricular Systolic Pressure = 66.8 mmHg
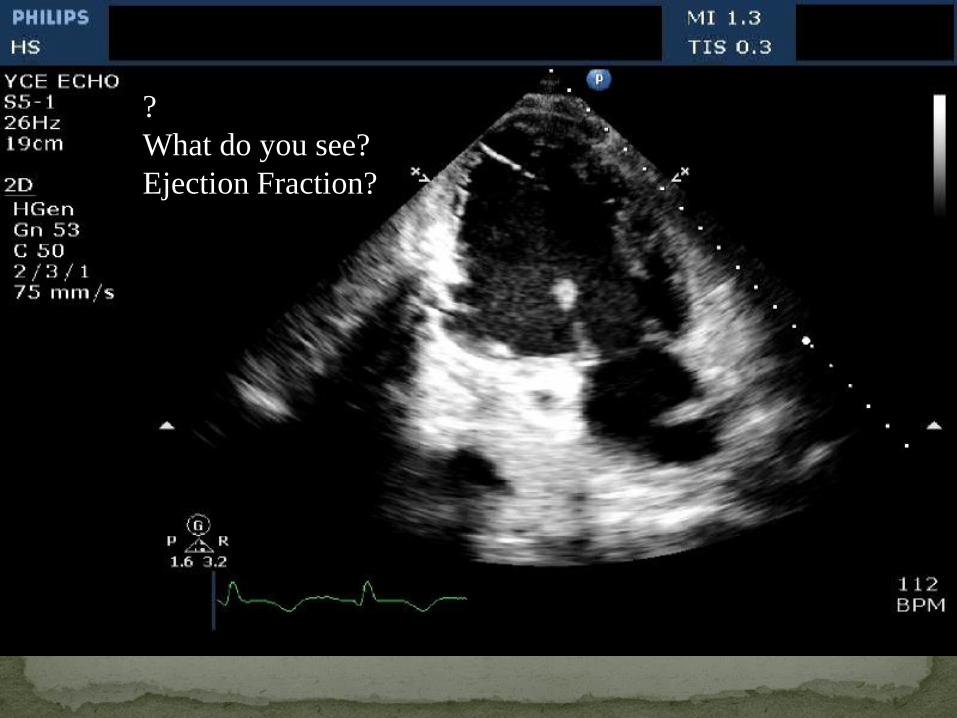
?
What do you see?
Ejection Fraction?

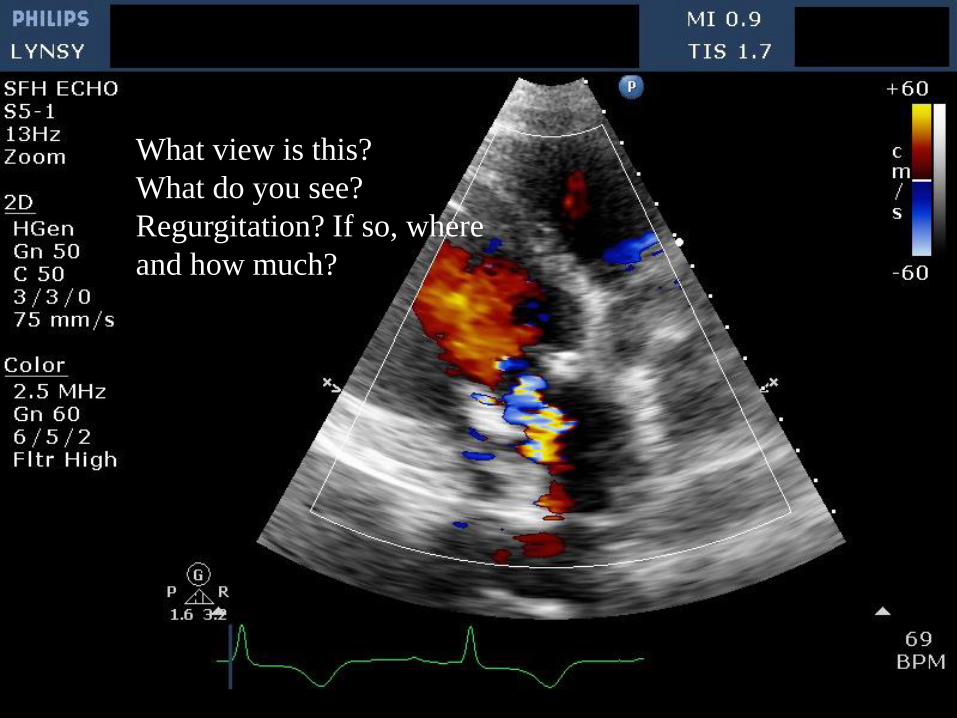
What view is this?
What do you see?
Regurgitation? If so, where
and how much?
Improvements?
Ruptured posterior papillary muscle with flail posterior MV leaflet
Wall Abnormalities (from MI) Inferior hypokinesis
Repaired muscular VSD
Right/left pleural effusion
Severely dilated LA
Mild LVH and RVH
High pulmonary artery pressure of 66.8 mmHg, which is considered “moderate” almost severe *not pictured
Severe MR
Moderate AI and TR
60% EF (increased since Echo #1)
Immediate admission to the operating room
The posterior papillary muscle was removed
The mitral valve was replaced with a bio-prosthetic valve

A follow up echo was done on Thursday, January 23, 2014
Completed by Lynsy Friend BS, RCS, FASE

What do you see?
Size and function of the
chambers?
What view is this?
What do you see?
Regurgitation? If so, where
and how much?

What do you think?
Size and function of
chambers?

What do you see?
Regurgitation? If so,
where and how much?

What do you see?
Size and function?
Ejection fraction?
New bio-prosthetic mitral valve Wall Abnormalities (MI)
Inferior hypokinesis
Minimal anterior pericardial effusion Significant pleural effusion (not visualized in the clips
I provided) Mildly dilated LA Normal RA size Mild LVH Moderate pulmonary artery pressure at 45.3 mmHg
(decreased since Echo #2) *not pictured Some MR (+ some MV thickening) Moderate TR (+ some TV thickening) Mild AI ( + some AV thickening) 20-30% EF (decreased since Echo #3)

29 y/o white female
Fibromyalgia
Vascular necrosis of lower extremities
Chronic pancreatitis
Systemic Lupus Erythematosus
Bilateral total hip replacement
Splenectomy
No tobacco use
No family history of CAD
MDs charted in past hospital visits that pt was a “drug seeker”
Female age 40
Immigrated from El Salvador at age 18
Developed abdominal pain, diarrhea, nausea, vomiting
Unable to walk more >3 steps at a time due to exertional CP and SOB
Labs: Eosinophils 17% (reference range 0-7%)

1+ RV lift and palpable P2
Second heart sound widely split during inspiration with an increased pulmonic component 3+/4+ intensity
Soft 1/6 diastolic decrescendo murmur, high pitched quality, at the left sternal border
JVP not elevated


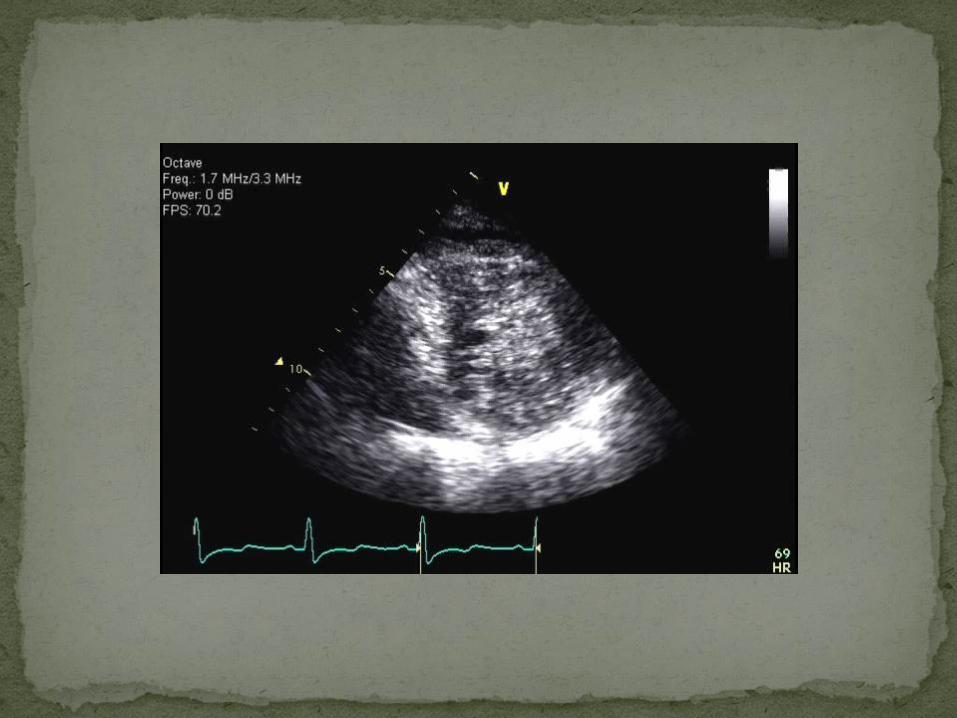

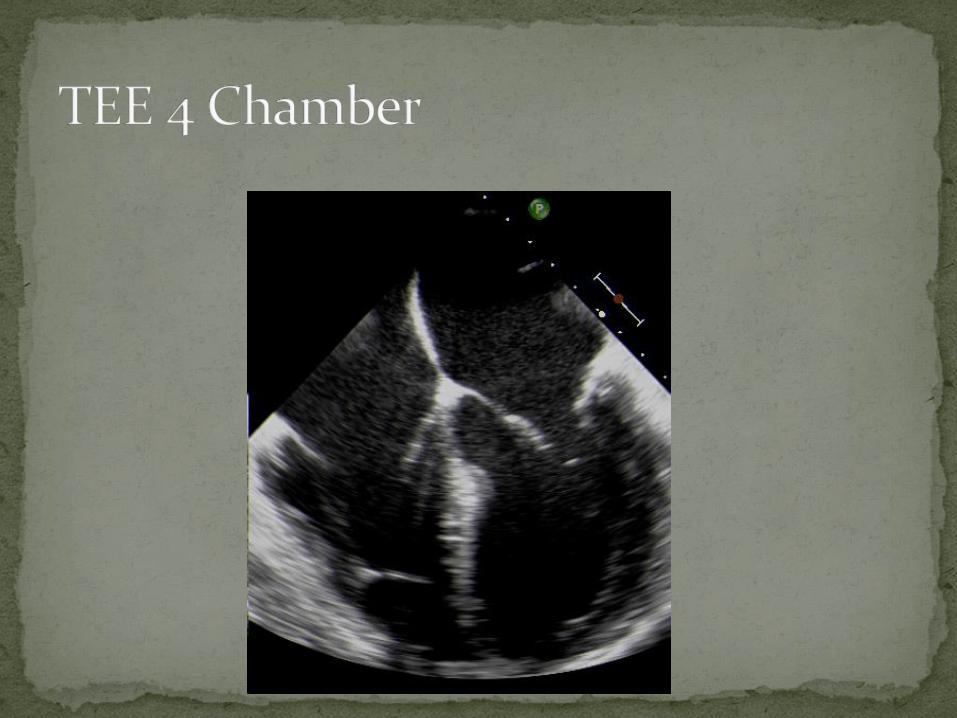
Mayo Clinic Apical 4 Chamber

Mayo Clinic Apical 4 Chamber

Mayo Clinic Apical 4 Chamber
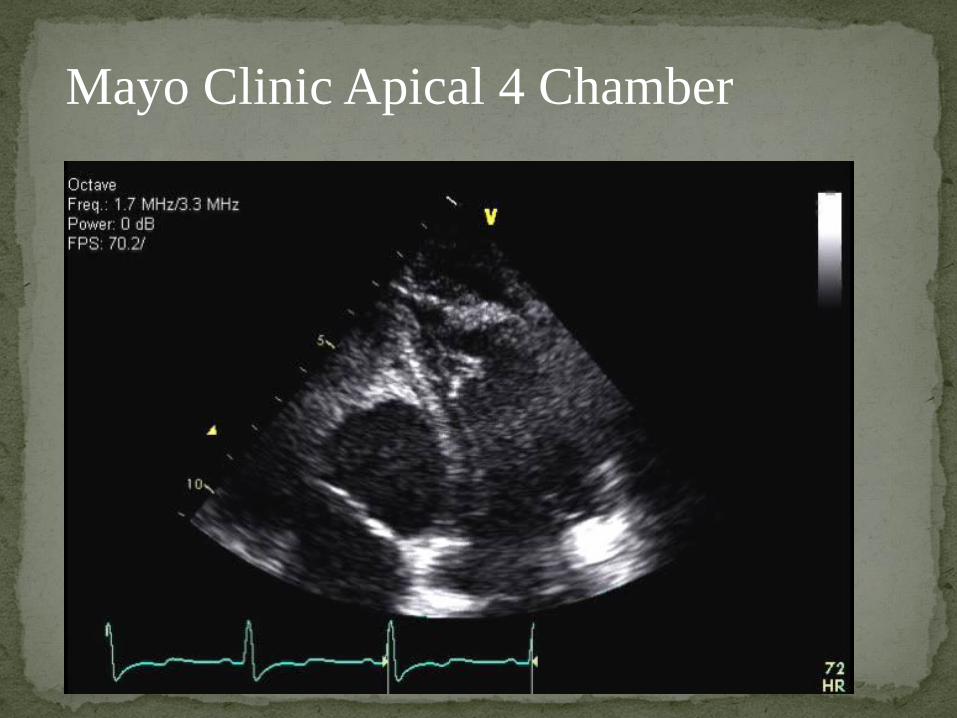
Mayo Clinic Apical 4 Chamber

1. LV non-compaction
2. Apical hypertrophic cardiomyopathy
3. LV and RV thrombus
4. Something else
Findings consistent with hypereosinophilic syndrome
Large laminated thrombus occupies apical 2/3 of LV cavity. Small apical RV thrombus.
Mild LVE, EF 49%, Grade 3/4 diastolic dysfunction
Thickened MV and TV without subvalvular thrombotic involvement or leaflet tethering. Mild MR and TR.

Large LV thrombus
Diffuse subendocardial delayed enhancement of LV and RV
LVEF 48%
Tiny pericardial effusion
Findings suggestive of eosinophilic myocarditis secondary to a parasitic infection

Extensive excision of fibrosis and organized thrombus in LV and RV cavities. Substantially improved both cavity sizes
Posterior mitral valve also appeared involved with moderate regurgitation
S/P 29- mm St. Jude mitral valve replacement, normal prosthetic function
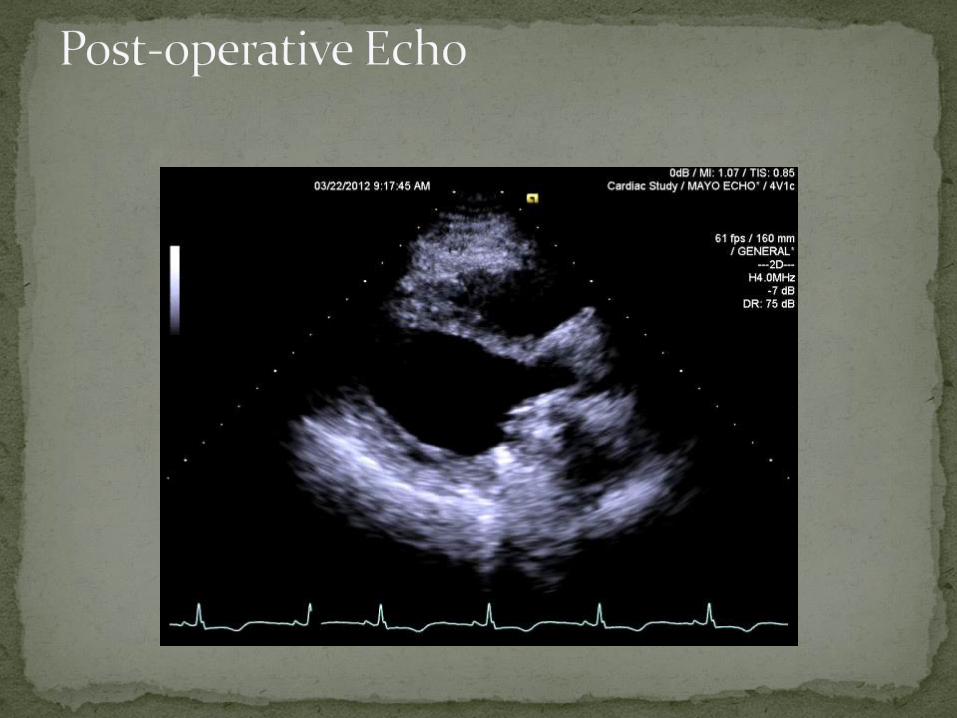



Normal LV size, EF 60%
Small area of endocardial fibrosis at LV and RV apex
No new intracavitary thrombi
RVSP has decreased
Normal MV prosthetic function

Marked endocardial fibrosis with organizing degenerating mural thrombus, encasing tendinous chords and extending to MV and into myocardium

Patient is feeling well other than overall feeling of weakness
No shortness of breath, chest pain or congestive heart failure symptoms
Follow up again in six months
Happy Mother’s Day to all the Mothers.
Safe Travels Home
Hope to see you all next year