eccentric compression after sclerotherapy of varicosities
TRANSCRIPT
Eccentric Compression
After Sclerotherapy of Varicosities with
a Self-adhesive, Individually Applied
Silicone Gel Pad
Johann C. Ragg, MD
angioclinic® Vein Centers, Berlin, Germany
Venartis® SGP is property of Venartis® Inc./USA
The method was invented by the presenting author.
The SGP study was funded by Venartis® and
performed by angioclinic® vein centers Europe.
The author is co-owner and consultant of Venartis®.
Conflicts of interest
Background
Compression: applied after vein therapy for a
multitude of purposes
Surgery: prevention of bleeding, swelling,
phlebitis, thrombosis
Method: circular compression
by stockings, bandages

sclerotherapy
Drawbacks: discoloration, induration, inflammation…
sclerotherapy
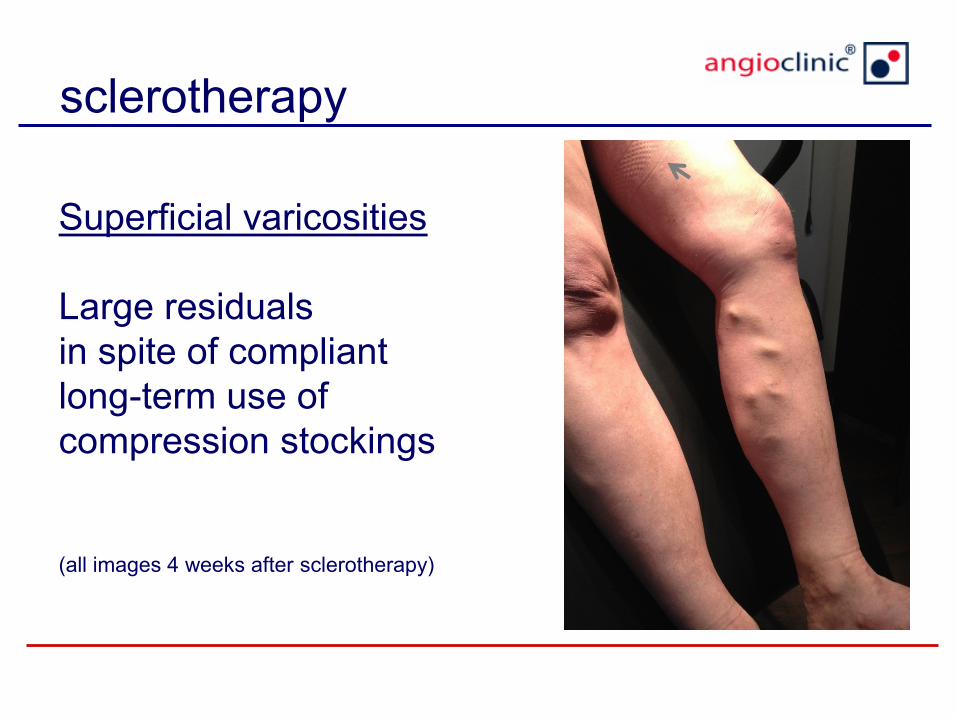
Superficial varicosities
Large residuals
in spite of compliant
long-term use of
compression stockings
(all images 4 weeks after sclerotherapy)

Background
Compression after Sclerotherapy
additional aims:
• prevention of local complaints
(inflammation, induration, discoloration)
• volume decrease of treated veins
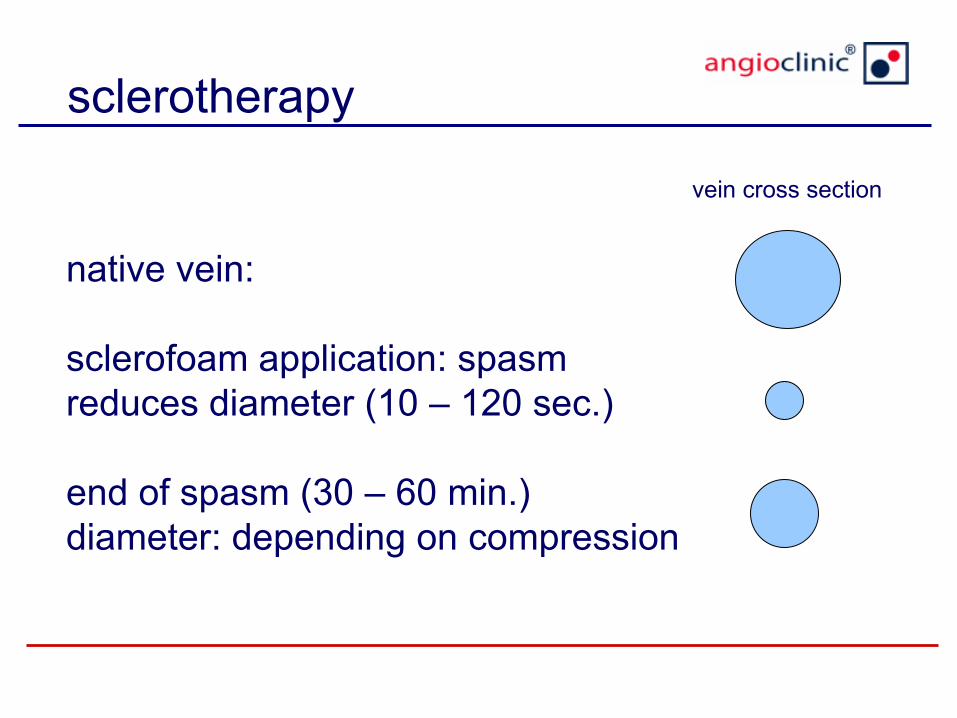
native vein:
sclerofoam application: spasm
reduces diameter (10 – 120 sec.)
end of spasm (30 – 60 min.)
diameter: depending on compression
sclerotherapy
vein cross section

vein closure by thrombi (0.2 – 48 h)
thrombus organization (1 – 42 d)
vein regression (3 -18 mon)
eccentric compression
aim 1: reduction of vein diameter
aim 2: accellerated vein shrinkage
sclerotherapy
vein cross section

Background
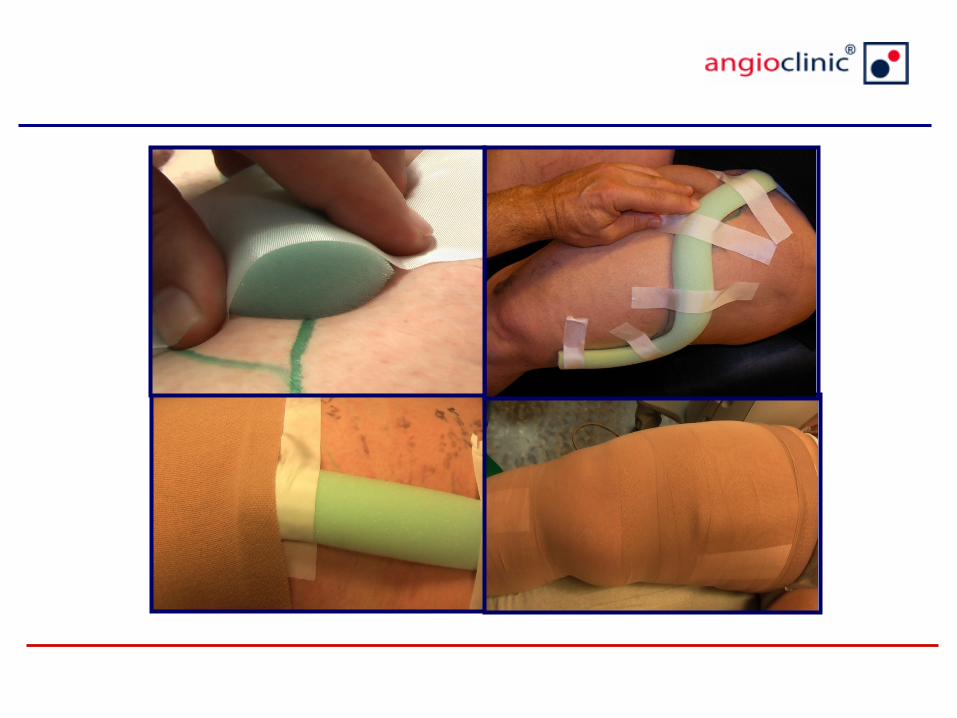
Home made eccentric bandages…
• pressure increased, but not controllable
• difficult to follow curved varicosities
• displacement, wrinkles, friction: skin lesions
hautläsion

History
a b c
a) pressure curve, b) optimized cross-section,
c) plastic foam rod for eccentric compression
12
After sclerotherapy of varicosities, eccentric
compression is meant to apply a focused pressure
directly on the target veins.
We evaluated a new self-adhesive modality called
Venartis® silicone gel pad (SGP).
Background
Venartis® SGP
target vein
skin
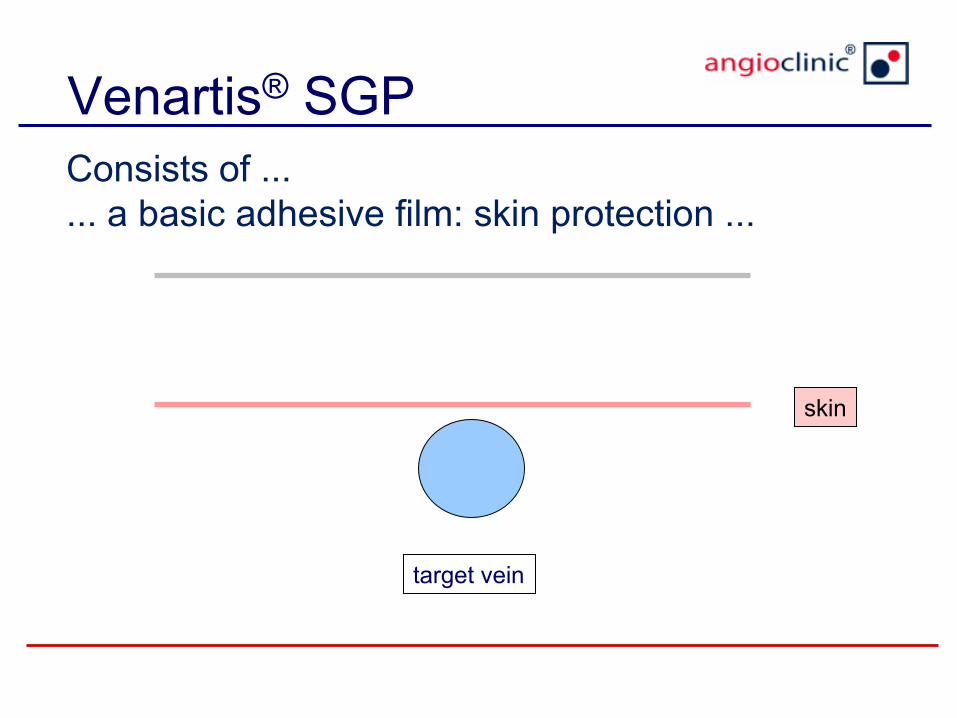
Consists of ...
... a basic adhesive film: skin protection ...

Venartis® SGP
target vein
skin + film
Consists of ...
... a basic adhesive film: skin protection ...

Venartis® SGP
target vein
silicone gel
... a silicone gel deployed from a cartridge ...

Venartis® SGP
target vein
... until R = 2r
silicone gel R
r

Venartis® SGP
target vein
... a second adhesive film to cover the silicone and
to shape the pad ...

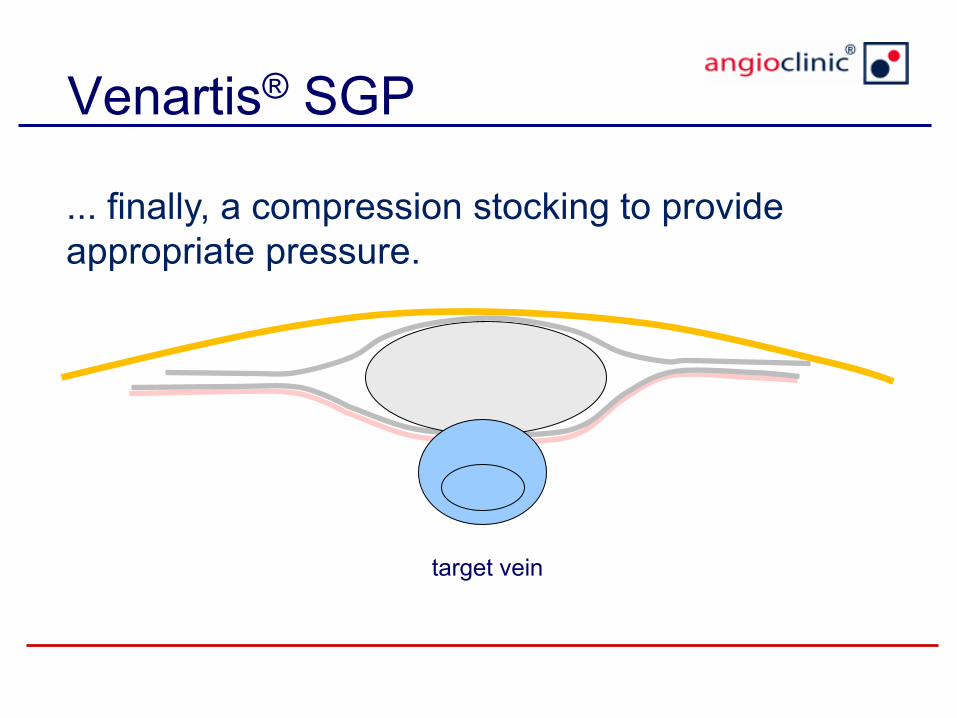
Venartis® SGP
target vein
... finally, a compression stocking to provide
appropriate pressure.
Venartis® SGP
target vein
... finally, a compression stocking to provide
appropriate pressure.

Silicone Gel Pad
• adaptable to size and course of vein
• self-adapting to body surface
• soft and flexible even after silicone hardening
• follows movements without shear stress to skin
• water resistant allowing daily showers
• effect controllable by ultrasound
• easy to remove

Venartis® SGP
varicosity silicone pad week 1 week 4
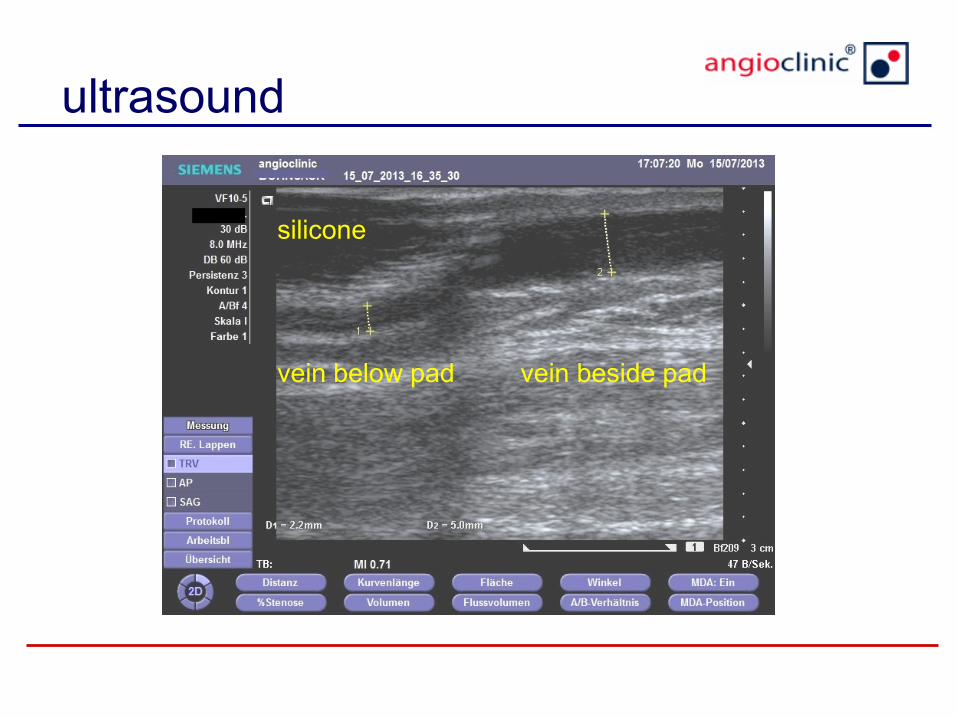
ultrasound
silicone
vein below pad vein beside pad

23
pilot study
Patients
• 68 patients (38 – 74 yr, 46 f, 22 m)
• vein diameter 5.2 – 13.0 mm, mean 7.4
• depth of target vessel: 0 – 15 mm
• polidocanol microfoam treatment
(1-2%, 1+4 with air or O2/CO2, via microcath)

Patients and methods
• at least 20 cm of “symmetric” varicosities of VSAA or saphenous sidebranches
Purpose: to compare comfort of compression media
Patients and methods
Legs randomized for post-treatment compression:
Leg A) SGP + medical compression stocking
Leg B) medical compression stocking only

27
SGP was intended to stay for 2 weeks,
compression stockings for 4 weeks.
Vein diameters were measured by ultrasound (1
sample / 3 cm) after 2, 4 and 8 weeks.
Methods
28
For ethical reasons, patients with symptomatic
phlebitis or indurations underwent thrombectomy,
leading to a bias concerning vein regression.
Segments requiring thrombectomy were excluded
from comparison.
Methods

29
Reduction of vein cross-section after 2 weeks
study group with SGP (A) 51.8% (22.4 – 72.1%),
control group (B) 23.2% ( 8.1 – 36.7%)
Results
30
Reduction of vein cross-section after 4 weeks
study group with SGP (A) 49.8% (35.2 – 64.0%)
control group (B) 26.7% (26.1 – 43.1%)
Difference decreases after SGP removal
Results

31
Reduction of vein cross-section after 8 weeks
study group with SGP (A) 66.8% (32.2 – 82.1%)
control group (B) 41.2% (24.1 – 61.7%)
Results

32
diameter reduction area reduction
native vein 7.4 -
SGP in place 4.0 45.9 % 68.2 %
vein at week 2 4.2 36.5 % 65,2 %
vein at week 4 4.7 39.9 % 56.6 %
vein at week 8 4.2 43.2 % 66.1 %
Sample calculation

33
vein diameter at the edge of SGP
Example
SGP

34
Reduction of vein cross section with SGP in place
study group (A) 72.5% (52.2 – 86.1%)
Results

Results
symptomatic inflammatory reactions
study group with SGP (A) 16.2% (11/68)
control group (B) 33.8% (23/68)

Results
symptomatic indurations
study group with SGP (A) 19.2% (13/68)
control group (B) 45.6% (31/68)

Results
discolorations (week 8)
study group with SGP (A) 11.8% (8/68)
control group (B) 36.8% (25/68)

38
early removal of SGP
due to minor discomfort:
3/68 patients (4.4%)
day 5 – 12
all cases: popliteal fossa
Complications
39
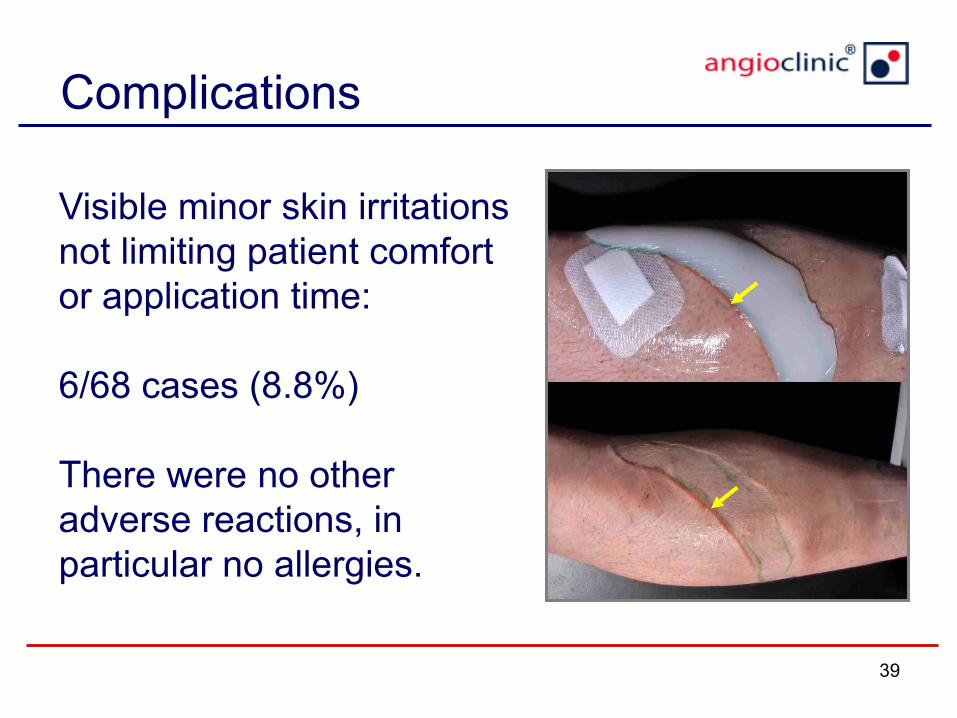
Visible minor skin irritations
not limiting patient comfort
or application time:
6/68 cases (8.8%)
There were no other
adverse reactions, in
particular no allergies.
Complications
40
Effects of SGP
54% faster vein regression
52% less phlebitis
58% less indurations
68% less discoloration
Summary
41
Venartis® SGP is a safe, effective and comfortable
modality to support vein regression of superficial
varicosities after sclerotherapy.
Frequent side effects of sclerotherapy like phlebitis,
induration, discoloration or discomfort can be
significantly reduced.
Conclusions

42
SGP should also be well applicable for superficial
tracts of GSV or LSV, and after treatment with
termo-occlusive modalities.
The effect of SGP, like any external pressure,
decreases with depth. For veins < 15 mm below
skin level other compression modalities should be
preferred (e.g. IntraShape® perivenous modeling).
Conclusions

43
further studies are required to optimize
• pad size
• degree of compression
• formula considering vein size and position
• wearing time
Should other techniques like gluing be included to make superficial sclerotherapy even
more successful?
Conclusions
