early interventions for families - wien.gv.at · early interventions for families at risk with ......
TRANSCRIPT

Dr. Andreas Eickhorst Institut für Psychosomatische Kooperationsforschung und Familientherapie
Early interventions for families at risk with
„Nobody falls through the net“ („Keiner fällt durchs Netz“)

Current Situation in Germany
• Severe cases of child neglect and abuse, especially with respect to very small children and infants
• Increasing uncertainity of parents • Focus on families with less access to education • Insufficient integration of children with migrational
background • Possibilties for direct interventions only in severe cases
of child mistreatment


Cumulative Effects of Risk (Sameroff et al. 1987)

Parental strains: • Early founding of a family • Birth as hard and traumatic experience • Postpartal depression of the mother • Chronic excessive demand of the mother
(the parents) • Dysfunctional relation • Severe / chronical physical illness of one
parent • Dissociability
Child‘s strains • Prenatal stress • Low weight at birth • Prenatal drug exposure • Increased sustencibility to illnesses • Disabilities • Preterm birth
Familial strains • Lack of familial support • One-parent family • Age difference between children < 18
months • Chronic illness or disability of sibling Social strains • Lack of social support • Dissocial environment Material strains • poverty • Small appartments
Risk-Screening based on multiple Factors (HBS – Heidelberger Belastungs Skala)

Parental strains: • Early founding of a family • Birth as hard and traumatic experience • Postpartal depression of the mother • Chronic excessive demand of the mother
(the parents) • Dysfunctional relation • Severe / chronical physical illness of one
parent • Dissociability
Child‘s strains • Prenatal stress • Low weight at birth • Prenatal drug exposure • Increased sustencibility to illnesses • Disabilities • Preterm birth
Familial strains • Lack of familial support • One-parent family • Age difference between children < 18
months • Chronic illness or disability of sibling Social strains • Lack of social support • Dissocial environment Material strains • poverty • Small appartments
Risk-Screening based on multiple Factors (HBS – Heidelberger Belastungs Skala)

Parental strains: • Early founding of a family • Birth as hard and traumatic experience • Postpartal depression of the mother • Chronic excessive demand of the mother
(the parents) • Dysfunctional relation • Severe / chronical physical illness of one
parent • Dissociability
Child‘s strains • Prenatal stress • Low weight at birth • Prenatal drug exposure • Increased sustencibility to illnesses • Disabilities • Preterm birth
Familial strains • Lack of familial support • One-parent family • Age difference between children < 18
months • Chronic illness or disability of sibling Social strains • Lack of social support • Dissocial environment Material strains • poverty • Small appartments
Risk-Screening based on multiple Factors (HBS – Heidelberger Belastungs Skala)

Parental strains: • Early founding of a family • Birth as hard and traumatic experience • Postpartal depression of the mother • Chronic excessive demand of the mother
(the parents) • Dysfunctional relation • Severe / chronical physical illness of one
parent • Dissociability
Child‘s strains • Prenatal stress • Low weight at birth • Prenatal drug exposure • Increased sustencibility to illnesses • Disabilities • Preterm birth
Familial strains • Lack of familial support • One-parent family • Age difference between children < 18
months • Chronic illness or disability of sibling Social strains • Lack of social support • Dissocial environment Material strains • poverty • Small appartments
Risk-Screening based on multiple Factors (HBS – Heidelberger Belastungs Skala)

Parental strains: • Early founding of a family • Birth as hard and traumatic experience • Postpartal depression of the mother • Chronic excessive demand of the mother
(the parents) • Dysfunctional relation • Severe / chronical physical illness of one
parent • Dissociability
Child‘s strains • Prenatal stress • Low weight at birth • Prenatal drug exposure • Increased sustencibility to illnesses • Disabilities • Preterm birth
Familial strains • Lack of familial support • One-parent family • Age difference between children < 18
months • Chronic illness or disability of sibling Social strains • Lack of social support • Dissocial environment Material strains • poverty • Small appartments
Risk-Screening based on multiple Factors (HBS – Heidelberger Belastungs Skala)
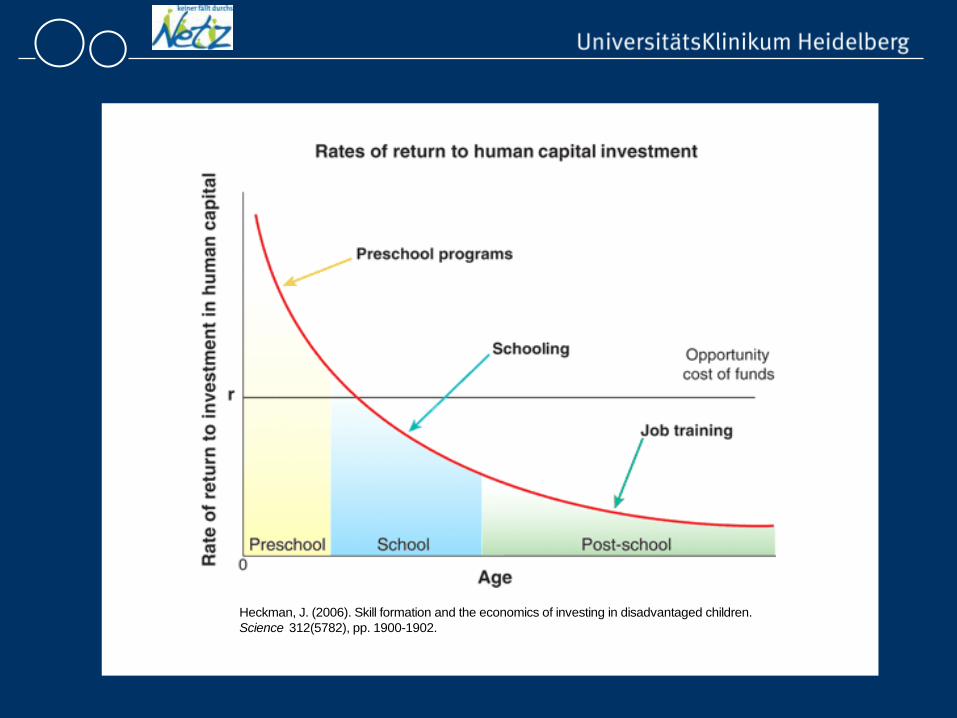
Heckman, J. (2006). Skill formation and the economics of investing in disadvantaged children.Science 312(5782), pp. 1900-1902.

Investment Return Cost effective to intervene earlier
Less use of community resources Health/mental health Social service School Legal system
Large pay off for services for each dollar spent

National Centre on Early Prevention (NZFH) Germany
National Centre on Early Prevention Knowledge platform
Research and monitoring of the development of practices in early prevention Development of criteria for systematisation and assessment of the practice Processing of research findings regarding early prevention Consolidation of knowledge regarding the ten pilot projects

Background of „Nobody falls through the net“
Implementation of research results (psychosocial medicine, developmental psychology and family research) into praxis
Implementation of local projects for a broader public
Reaction to current societal challenges (in this case: providing early interventions for young families)
Evaluation and research to ensure the applicability and adequacy of our project

support all families during the period of getting parents
reach those families that are highly burdened and at high risk
and that mostly don‘t participate in parenting courses or groups.
Aims of „Nobody falls through the net“

In order to detect and assist a family that is at high risk as early as possible, three necessary steps have to be made:
1. Establish an access to the family at risk
2. Identify a risk-constellation
3. Mediate to an appropriate intervention
Three-steps

Reach-Strategy for Early Interventions
• Reaching young families during mother‘s pregnancy and the birth of the child • Having access to nearly all new parents via the health
care system (e.g. gynecologists, midwifes, hospitals)
• Having a screening for risks for parents and baby
In this transition period this is not seen as discriminating
• At the time of birth young families are more open for advices and consultations

Regularly home-visits of midwifes
3. S
tep:
M
ediate
to
an
inte
rven
tion
tha
t mee
ts t
he
requ
irem
ents
of
the
family
2. S
tep:
Pr
omot
e ba
sic
compe
tenc
ies
and
iden
tify
a r
isk-
cons
tella
tion
1. S
tep:
Es
tablish
an a
cces
to
the
fam
ily a
nd
conn
ect
the
family
to
a f
amily
midwi
fe
Screening and if required mediation to an appropriate intervention service
Delivery-Station
Early Intervention For the time being no necessity to intervene
„coming“-structure
„going“-structure
Parenting course:
„Understanding the Baby“
+
or
Home-visiting model: „Understanding the Baby“
Medical Prevention
Psychosocial Prevention

Hessen
County Bergstraße County Offenbach County Werra Meissner
Saarland
All six counties
Baden-Württemberg
City of Heidelberg
County Neckar-Odenwald
2011: Eleven Locations of „Nobody falls through the Net“

Three Main Components
Coordination:
Network for Parents
Coming-Structure: Parenting courses
“Understanding the Baby“
Going-Structure: Home-visiting by family midwifes

Prepares parents for interacting with their infant (signals, needs and demands)
Videotaped parent-infant-interactions as main part
Each project-location will be featured with 15 to 30 course instructors (midwifes, pediatrics,…)
Parenting courses are for all interested parents across the entire state, not specifically for those at risk
I. Parenting Course „Understanding the Baby“

Properties
www.focus-familie.de

Session contents
• 1. Session: I am also taking care of myself. • 2. Session: Relationship challenges • 3. Session: Babies are sending signals • 4. Session: What precedes the crying? • 5. Session: Trust in one‘s own competences

1. Session: “I am also taking care of myself”
• Parental feelings concerning their interactions with their children
• Perception of one‘s own needs, especially recognizing one‘s limits
• strategies for self-care

2. Session: “Relationship challenges”
• Transition from couple to parenthood: a normative crisis
• examination of this life phase and active search for resources
3. Session: “Babies are sending signals”
• Introduction of the concept „parental sensitivity“, recognizing and interpreting infant‘s nonverbal signals as a pretext for adequate and prompt parental reactions
• Getting to know children's signals for readiness to
interact

4. Session: “What precedes the crying?”
• Perception and interpretation of infants‘ stress signals • Crying as a form of child communication • Gaining awareness for body language signs often
preceding crying • Effects of crying • Dealing with strong affective reactions to crying (issue of
baby shaking) • Children's attempts at self-soothing • Soothing strategies

5. Session: “Trust in one‘s own competences”
• Confidence in one‘s own spontaneous parental
reactions • Intuitive parental behavior • Possible limitations of intuitive parental behavior
1. What do you think this baby is feeling? (It is feeling well) Repetition oft he sequence
2. On which details you can recognize it? – Further details? (......) We can see that the baby is feeling well. He keeps face to face contact to his mother. He lays all his attention on her. He looks at her and keeps contact with the eyes.
3. What does the baby communicate on this way? How can we understand him? (...........) The baby shows his mother with this behavior, that in this moment nothing is as fascinating for him as her face. He expresses interest and pleasure. This is the main message: Let’s flirt together, hold the gaze and communicate with me.
„Understanding your Baby“
Example - Analyses of video clips

How do babies communicate?
Eye glance behavior Facial expression Body posture, movements, tension Motor activity Breathing behavior Voice: sounds, crying Mimic behavior
...

What do babies and toddlers tell us?
They show signs of • Hunger,pain,…
...readiness to interact, curiosity, happiess,
...tiredness, sensory overload...

What and how do babies communicate I
• Readiness for social interaction • „I want to interact with you!“
Catching someone‘s eye smiling Moving towards a person Smooth, calm movements of extremities Relaxed sounds Reaching out with their arms …

What and how do babies communicateII
• avoidance • „That‘s too much for me right now!“
Turning away from or pushing away from person Superextension Weepy face Transitive flail Head shaking Spitting up Empty gaze …

Evaluation of the parenting course
• Over proportionally high number of participants with high levels of education, high income, etc.
• Very positive evaluation by participants • More than 90% would recommend the course to others • Same evaluation of „novelty of contents“ across all
social backgrounds • Greater gain in knowledge in parents with lower levels
of education – But no correlation between level of education and evaluation

• Advanced training for family midwifes (model Hessen): 168 hours in 5 x 4 days and 3 days of supervision
• 3-10 family midwifes per project location
• Attendance throughout the infant‘s first year of life
• Families are provided with developmental-psychological and psychosocial care as well as with support concerning primary care
• Continuous project meetings and supervision of the family midwifes
II. Family Midwifes

Why midwifes?
The German health care system already provides costless homevisitations of midwifes during the first 8 weeks of the infant
So homevisits of midwifes are not stigmatized, they are seen as normal routine
Midwifes are positively connotated significant others for the mother
Usually a midwife can become a „family member“ very easily, she is the person a young couple can lean on.

• Parenting course „Das Baby verstehen“: taking care of oneself, transition from couple to parents, baby‘s signals, screaming, intuitive parental capacities
• Basics of family psychology and family therapy
• Communication, work with families
• Parental mental health problems, social crisis situation
• Social legislation/ socialpolitical sanctions
• Public Health and community work, interdisciplinary teams
Curriculum for the advanced training of family midwifes

• Each county sets up a „Network for Parents“
• Members of all professionals in the field of prevention and intervention in early childhood
• Generation of cooperative-structures in order to adequately mediate intervention
• One mediating contact person in the sense of a central coordination (local coordinator)
III. „Network for Parents“

Coordinators
• Each county has its own local coordinator • Administration and coordination of the „Network for
Parents“ • In charge of connecting families at risk with the family
midwifes and mediating further interventions • Working at interfaces:
– University hospital and family midwifes – Families and institutions – University hospital and counties

Coordinator
Local Health Authority
Youth Welfare Office
Community Service
Social Welfare Office
Counselling services
Birth-Delivery-Stations
Pediatrics Gynegologists
Midwifes
Family midwifes
University Hospital
HD

Project experiences I Referral process: • Unexpected high number of families already received support from counseling or child services before: • In part very high risk families (important clientele, but beyond prevention) • How can we improve our access to so far unsupported families? The cooperation between different professions is often associated with various apprehensions, e.g. • Unjustified data collection/ disclosure • Project midwives „taking away“ other midwives‘ work • Project midwives working in typical fields of child protective services or causing them additional work

Project experiences II
It has to be dealt with different, already existing fields of conflict:
• Rivalry between institutions • Reservations between different professions e.g. physicians, social workers vs. midwives • Somatic vs. psychosocial diagnostics background • Professional discretion (§203) vs. child well-being (§ 8a SGBVIII) • Different perception of families: support vs. control

Some evaluation data

Number of cases in the county Offenbach
2007 2008 2009 2010 2007 - 2010
Cases 9 38 30 27 104

Number of home visitations in the county Offenbach
2008 2009 2010 2008 - 2010
Home visitations 619 643 928 2190

0
5
10
15
20
25
30
35
ASD Klinik Hebamme Beratung Ärzte Andere
Number of requests in 2010
Requests
Youth welfare system 31 (21%)
Birth hospitals 13 (9%)
Regularly midwifes 32 (22%)
Counseling centers 15 (10%)
Medics 9 (6%)
Other 33 (23%)
Families themselves 14 (10%)
Total
147 (100%)
All data collected in the project county Offenbach

Medical Care 25,0%
Caring for oneself 30,0%
Singals of the Baby 21,0%
Stress signals of the Baby 5,0%
Strenghtening the parental competence
11,0%
Partnership 8,0%
Data of 3.353 Home visits (2007 – 2010) All data collected in the project area Hessen
Topics in the home visits of the Family Midwifes

T1 4-6 weeks after birth
T2 6 months
T3 1 year
T4 2 years
Control group (150 families at risk)
Intervention group (150 families at risk)
Homevisitations of the family midwives
„PFIFF“: Effects of KfdN Model project of the „National Centre on Early Prevention“
Sample at T1 • N = 302 mother-child-dyads
• Age of the mother: 26,47 (SD = 6,82); 12,3% < 18 years
• Education: 17,2% no graduation; 40,3% Hauptschule (9 years of
schooling; 27,5% Realschule (10 years of schooling)
• 24,9% single mothers; 32,2% married
• Income per household: 52% < 1000€
• Nationality: 80,8% German; 5,4% Turkish
• Children: 52% male, 15% premature birth
Instruments Children Ages & Stages Questionnaire (ASQ, Squires, Potter & Bricker, 1999) Mother-child-interaction CARE-Index (Crittenden, 2004) Mothers EPDS (Cox, Holden & Sagovsky, 1987) Parenting Stress Index (PSI, short version, Abidin, 1995)

Maternal Sensitivity (general; CARE-Index)
Time: p = 0,034 ; Group x Time: not significant (N = 244)

Maternal sensitivity (cognitive aspects; CARE-Index)
Time: p = 0,008 ; Group x Time: not significant (N = 244)

Social development of the children (ASQ) „If you reach out your hand and ask for your baby‘s toy,
does your baby give it to you?“
Time: n.s. ; Group x Time: p = 0,001 (N = 251) Communikation: n.s.
d = .34 d = .34

„Dysfunctional Interaction“ (PSI) „Sometimes it seems to me, that my child doesn‘t like me and
doesn‘t like to be near me“
Time: n.s. ; Group x Time: p = 0,022 (N = 197)
d = .27

„Difficult Child“ (PSI) „My child has heavy mood swings and is rapidly excitable“
Time: p = 0,000 ; Group x Time: p = 0,01 (N = 188)
d = .24

Maternal postpartum depressiveness (EPDS)
„I have been so unhappy, that I could not sleep“
Time: n.s. ; Group x Time: n.s. (N = 191)
d = .23

Conclusion 1: Effectiveness in children’s outcomes
The intervention project showed A direct positive influence on the child: a) social development (ASQ) And as well an indirect positive influence via the perceptions or
attitudes of the mothers towards their children‘s behaviour (PSI).
• There have been no effects concerning the development of language.

Conclusion 2: Effectiveness in the mother-child-interaction
• Dysfunctionality of the mother-child-interaction was alleviated (PSI: self assessment)
• But no intervention effects on the maternal sensitivity (CARE-Index: expert assessment).

Conclusion 3: Effectiveness in the mothers’ outcomes
• The improvement of the maternal depressive symptomatology was meaningful in a clinical sense, but failed significance.
• No influence of the intervention on the maternal stress could be detected.

Thank you for your attention!
Dr. Andreas Eickhorst Institut für Psychosomatische Kooperationsforschung und Familientherapie Universitätsklinikum Heidelberg Bergheimer Str. 54 69115 Heidelberg Mail: [email protected] www.keinerfaelltdurchsnetz.de