early intervention: an outcomes based evaluation of disparity in access taletha m. derrington, m.a....
Post on 19-Dec-2015
213 views
TRANSCRIPT

Early Intervention: An Outcomes Based Evaluation of Disparity in Access
Taletha M. Derrington, M.A. and Beppie J. Shapiro, Ph.D.
Center on Disability Studies, College of Education, University of Hawai`i
www.seek.hawaii.edu, [email protected], [email protected],

Definitions
Early Intervention – Part C of IDEA, a mandated system of services for babies under age 3 with special needs (EI)
Child find – Efforts to ensure that babies with special needs are identified and referred to early intervention
Context
Required Child Find function
Community programs
No history of evaluation

Context
Infant Toddler Development Programs Delays in 2 domains
Public Health Nursing Sections Medical condition or single delay
Service areas Geographically defined for rural areas Parental choice for urban areas (2/3 state
population)

Why Did We Study Disparity?
National focus on disparities in health care - Minority ethnicity
- Low income- Recent immigrants- Limited English proficiency
– Homelessness– Uninsured

What Demographics Predict Disparity?
Ethnicity vs. SES

Unfortunate Coincidence
Family demographics predict child delays
Same family demographics predict less access to services

Processes Studied for Equity in Access
Public Awareness: Media campaigns, brochures, public education
Identification: Parent or professional notices a child’s need
Referral to an EI program: First EI record created
Intake process at EI program Program contact with parent
Intake record created
Eligibility determination
Enrollment If eligible and parent agrees
Service record created

Demographics Studied for
Equity in Access
EnrollmentReferral
Low-Income Uninsured Immigrant Limited English proficiency Military Homeless

Metric for Equity in Access
Ideally: compare # served with # in population (prevalence)
Problem: prevalence either unknown or based on # served
Assume: prevalence of EI eligible conditions evenly spread across all sub-populations
% referred or enrolled = % in population
How we measured prevalence
Census is best population – wide data But census does not give statistics for
children aged 0 – 3 So we had to estimate statistics for
children 0 – 3 from Census statistics for children aged 0 – 18 or 0-5

Example:
45,412 children aged 0 – 3/ 295,767 aged birth to 18 = .15 or 15%
If census reports 1000 children 0 – 18 are poor, we calculate 1000 X .15 = 150 children 0 – 3 are poor.
Note: new assumption – same % among poor as among total population
Expect 15% of babies referred to EI to be poor.

Data Sources
Intake records at EI programs (1997)– 4 ITDPs– 2 PHNs
Study-specific questions added to intake (1996-97)– 6 ITDPs– 5 PHNs– State information & referral line
Statewide EI management information system (1997)

Process
Sub-Group IntakeStudy-Specific
MIS
Referral
Low-Income161 286 No data
Uninsured161 No data No data
ImmigrantNo data 286 No data
Limited English proficiency
No data 286 No data
MilitaryNo data 286 No data
HomelessNo data No data No data
Sample Sizes - Referral
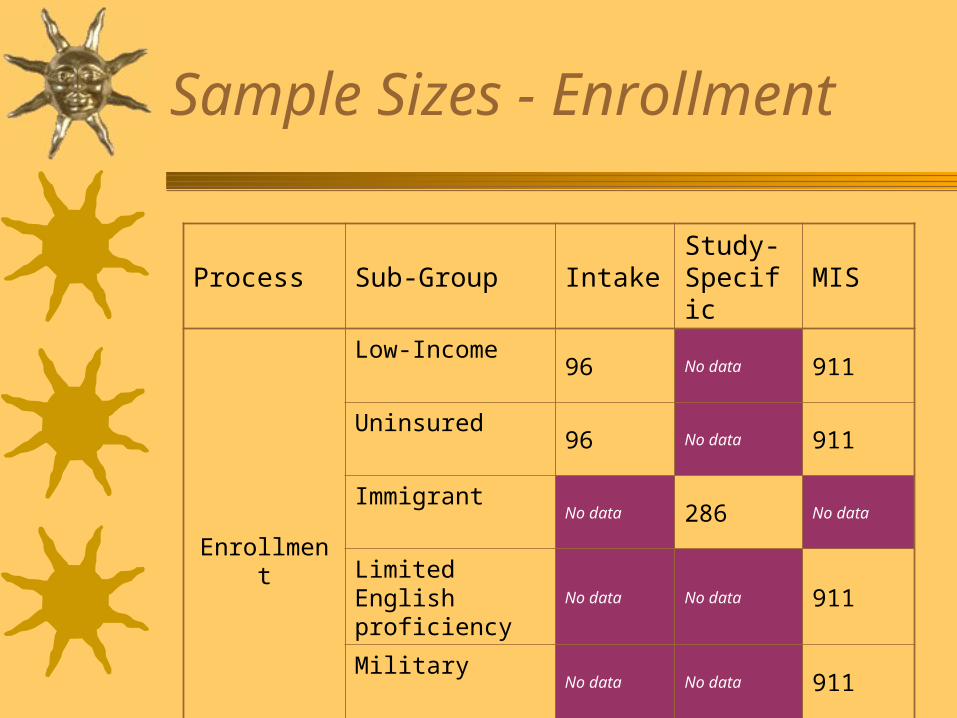
Sample Sizes - Enrollment
Process Sub-Group IntakeStudy-Specific
MIS
Enrollment
Low-Income96 No data 911
Uninsured96 No data 911
ImmigrantNo data 286 No data
Limited English proficiency
No data No data 911
MilitaryNo data No data 911
HomelessNo data No data No data

Data Analysis
Determine if observed and population %’s differ using chi squared
If so, calculate the effect size using “Relative Risk”

And We Found…

Income/Public Insurance
0
10
20
30
40
05
101520253035404550
Referral
Public InsurancePoor
0
10
20
30
40
50
60
70
Expected % Observed %
Public Insurance
Enrollment

Uninsured Children
Referral Enrollment
0
1
2
3
4
5
6
7
Expected %
Observed %
0
1
2
3
4
5
6
7

Immigrants
0
2
4
6
8
10
12
Expected %
Observed %
Referral

Limited English Proficiency
0
1
2
3
4
5
6
7
Not at All Not Well orAt All
Expected %
Observed %
0
1
2
3
4
5
6
Not At All Not Well + At All
Referral Enrollment

Children in Military Families
10
12
14
Expected %Observed %
0
2
4
6
8
10
12
Referral Enrollment

Where Do We Go From Here?
Limitations– 1997 data; same in 2005?– Estimations for population comparison
data

Uninsured Children
56% less likely to be referred66% less likely to be enrolled Disparity may be over-estimatedStill a cause for concern

Limited English Proficiency
Self-report a limitation for both study and population figures
Equity in referralDisparity in enrollment possible for
families who speak only some English– Need for interpreter not recognized by
program staff?– What happens between referral &
enrollment?

Children in Military Families
Equity in referralDisparity in enrollment
– Coordination with military Exceptional Family Member Program
– What happens between referral & enrollment?

Homelessness
How can you study this without turning away needy families due to stigma?
Data Privacy

Further Study
Multiple risk factorsIncreased risk, over-
representation, or over-referral?

Group Discussion
How can we address demographically based access barriers?– Uninsured– Limited English Proficiency– Military dependents
What can we do to address difficult-to-study demographics?
How can or should we use data collected several years before its publication?

February 28, 2005
MAHALO!
Please complete an evaluation for this session

Contact & Reference
Taletha M. Derrington, M.A. and Beppie J. Shapiro, Ph.D.
Center on Disability Studies, College of Education, University of Hawai`i
www.seek.hawaii.edu, [email protected], [email protected],
Shapiro, B. & Derrington, T. (2004). Equity and Disparity in Access to Services: An Outcomes-Based Evaluation of Early Intervention Child Find. Topics in Early Childhood Special Education, 24(4), 199-212.