early cannulation a new model in delivering hemodialysis
TRANSCRIPT

ASVSIstanbul 2013
Early cannulation, a new model in delivering hemodialysis
Jürgen Falkensammer
Department of Vascular and Endovascular Surgery
Wilhelminenspital Wien

Falkensammer ASVS Istanbul 2013
Disclosures
Jürgen Falkensammer, MD
I have the following potential conflicts of interest to report:
Honorarium for the presentation

Epidemiology of RRT
Falkensammer ASVS Istanbul 2013
USRDS 2013

Epidemiology of RRT
Falkensammer ASVS Istanbul 2013
USRDS 2013

Access Types
Falkensammer ASVS Istanbul 2013
incident prevalent
DOPPS, Kidney Int. 2002

HD catheters
Falkensammer ASVS Istanbul 2013
• High morbidity caused by
− Thrombosis
− Infection
K/DOQI 2006

Patient Survival
Falkensammer ASVS Istanbul 2013
Dhingra et al, Kidney Int. 2001
diabetic Non - diabetic
Adjusted for age, race, gender, BMI, history of smoking, PVD, CAD, CHF, neoplasm, ability to ambulate and education level
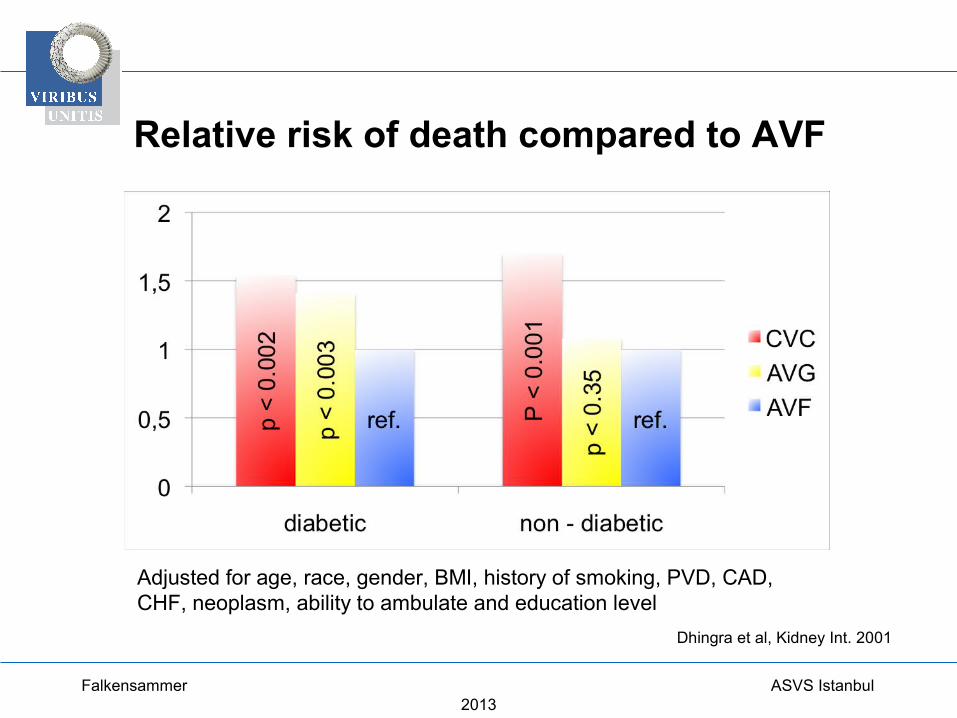
Relative risk of death compared to AVF
Falkensammer ASVS Istanbul 2013
Dhingra et al, Kidney Int. 2001
Adjusted for age, race, gender, BMI, history of smoking, PVD, CAD, CHF, neoplasm, ability to ambulate and education level

HD catheters
Falkensammer ASVS Istanbul 2013
• High morbidity caused by
− Thrombosis
− Infection
• Risk for permanent central venous stenosis or occlusion
• Discomfort and cosmetic disadvantage of an external appliance
• Shorter expected use-life than other access types• Overall lower BFRs, requiring longer dialysis times
K/DOQI 2006

K/DOQI Guidelines
Falkensammer ASVS Istanbul 2013
• Short-term catheters should be used for acute dialysis and for a limited duration in hospitalized patients
Short-term Catheters should not be used in patients with foreseeable chronic HD dependency
K/DOQI 2006

K/DOQI Guidelines
Falkensammer ASVS Istanbul 2013
• Avoid if possible: Long-term catheters
Alternative to long-term catheters?
K/DOQI 2006

K/DOQI Guidelines
Falkensammer ASVS Istanbul 2013
Order of preference for HD access:• radial-cephalic AVF• brachial-cephalic AVF• brachial-basilic transposed AVF +/-• forearm AVG• upper arm AVG• alternative sites

Graft Survival
Falkensammer ASVS Istanbul 2013
DOPPS, Kidney Int. 2002

K/DOQI Guidelines
Falkensammer ASVS Istanbul 2013
Fistula First Strategy
If a primary AVF can not be established, a synthetic AV graft is the next preferred type of vascular access.

Requirements for AV Grafts
Falkensammer ASVS Istanbul 2013
• Easy to implant• Good incorporation• Do not clot• Infection resistant• Easy to cannulate• Does not bleed after cannulation
• Does not form pseudoaneurysms

Requirements for early-cannulation Grafts
Falkensammer ASVS Istanbul 2013
• Does not weep• Is self-sealing• < 24 hours cannulation
Early-access Grafts
Falkensammer ASVS Istanbul 2013
Vectra® Vascular Access Graft
AVflo™ Vascular Access Graft
Gore® Acuseal Vascular Graft
Flixene™ Atrium
Rapidax TM
Polyuretane vs. PTFE

Early-access Grafts
Falkensammer ASVS Istanbul 2013
Multilayered:
Outer layer for tissue integration
Intermediate layer for sealing
Inner layer for blood contact
Special features
Design
Antithrombotic properties
Infection - resistance
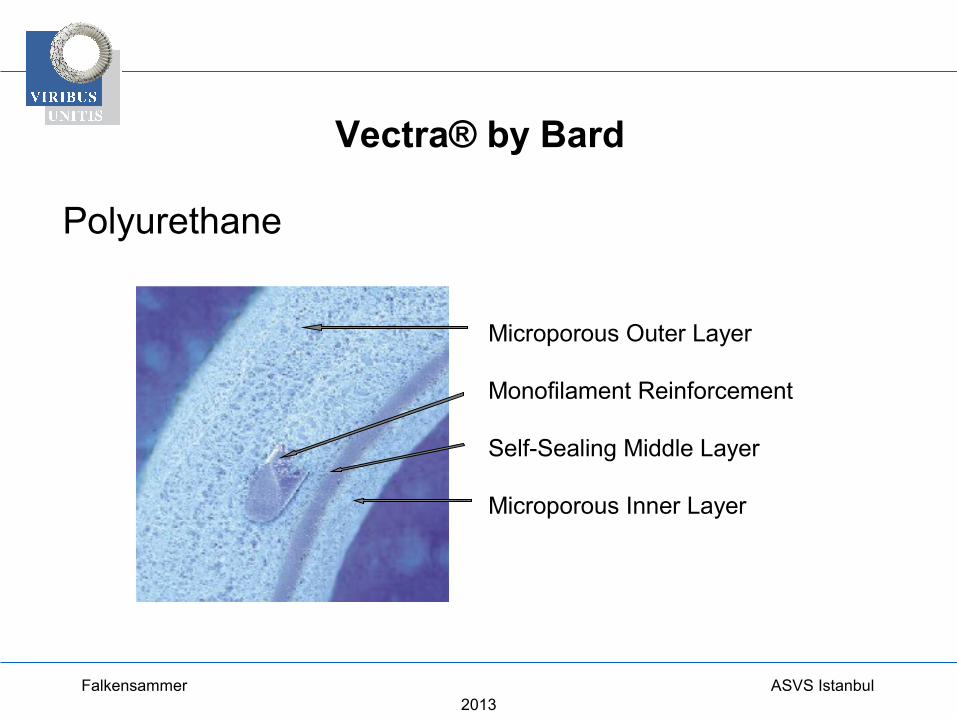
Vectra® by Bard
Falkensammer ASVS Istanbul 2013
Polyurethane
Microporous Outer Layer
Monofilament Reinforcement
Self-Sealing Middle Layer
Microporous Inner Layer
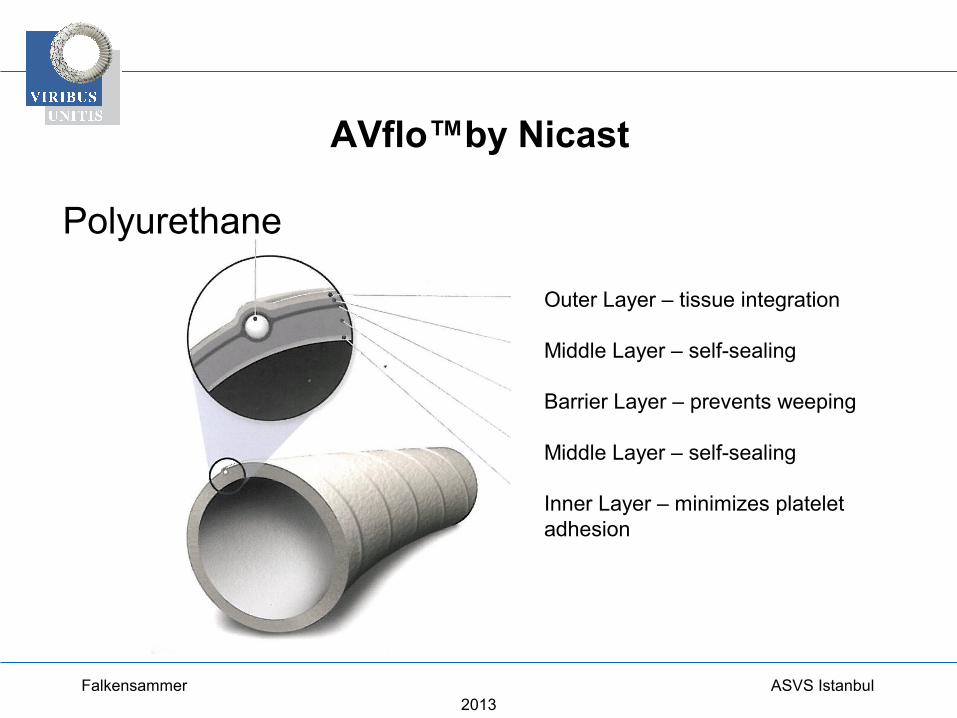
AVflo™by Nicast
Falkensammer ASVS Istanbul 2013
Polyurethane
Outer Layer – tissue integration
Middle Layer – self-sealing
Barrier Layer – prevents weeping
Middle Layer – self-sealing
Inner Layer – minimizes platelet adhesion

Gore® Acuseal
Falkensammer ASVS Istanbul 2013
PTFE
PTFE
Silicone
CARMEDA® BioActive Surface (Heparin)

Flixene™ by Atrium
Falkensammer ASVS Istanbul 2013
PTFE
Tissue Surface
HydrostaticProtectionMembrane
Flow surface

Flixene™ - Special Features
Falkensammer ASVS Istanbul 2013
Resistance
Tapered design
Graduated wall thickness

Flixene™ by Atrium
Falkensammer ASVS Istanbul 2013
Low – profile tunneling system

Flixene™ IFG
Falkensammer ASVS Istanbul 2013

AVF vs. PTFE graft
Falkensammer ASVS Istanbul 2013
Patency of autogenous and PTFE upper extermity AV hemodialysis access: A systematic review(Huber et al, JVS 2003)
• Medline-based systematic literature review and meta-analysis of patency data in life table or KM
• 1966-2001: 211 full text articles identified • 34 studies fulfilled the criteria
Huber et al, JVS 2003

18 – Months Patency Rates
Falkensammer ASVS Istanbul 2013
6 months 18 months
Primary patency
AVF 72% 51%
AVG 58% 33%
Secondary patency
AVF 86% 77%
AVG 76% 55%
Huber et al, JVS 2003

6 – Months Patency Rates
Falkensammer ASVS Istanbul 2013
AVF PTFE Flixene Vectra AVflo
Author Huber et al, JVS 2003 Schild AF et al, J Vasc
Access 2011
Kakkos et al. J Vasc Surg
2008
Wijeyaratne et al, J Vasc Access 2011
N = 1849 1245 33 76 35
Primary patency 72% 58% 49% 75% 73%
Secondary patency 86% 76% 80% 85% 82%
Primary assisted patency!

Indications for early – cannulation AV grafts
Falkensammer ASVS Istanbul 2013
• early access• to avoid a HD catheter• as a revision graft / for interposition: no
‚catheter – bridging‘ needed• possibly whenever no native vessels are
available for fistula creation
>> indication for a ‚conventional‘ access graft?