e-mental health services in australia 2014: current and future
TRANSCRIPT

e-MENTAL HEALTH SERVICES IN AUSTRALIA 2014: CURRENT AND FUTURE
Helen Christensen & Judy Proudfoot – Black Dog Institute
Alan Woodward – Lifeline
Aram Hosie – ReachOut.com
Britt Klein – Federation University
Christine Morgan – Butterfly Foundation
David Kavanagh – Queensland University of Technology
Gavin Andrews – This Way Up
Georgie Harman – beyondblue
Jane Burns & Michelle Blanchard – Young and Well Cooperative Research Centre
Justin Zachan – mindhealthconnect
Kathy Griffiths – National Institute for Mental Health Research ANU
Katrina Stroud – e-headspace
Maree Teeson & Frances Kay-Lambkin – NHMRC Centre of Research Excellence in Mental Health and Substance use, NDARC
Neil Thomas – Swinburne University
Salote Scharr – Kids Helpline
Sue Spence – Griffith University
Terence Humphreys – Twenty10

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
2

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
3
e-Mental Health Services in Australia 2014: Current and Future
EXECUTIVE SUMMARY This report has been prepared by the e-Mental Health Alliance representing the core group of organisations listed above, who are currently providing highly effective and cost efficient e-Mental Health (eMH) services directly to the Australian population. There is no doubt that technology is changing the way in which healthcare is accessed, received and delivered, and that the role of eMH health will continue to grow. We need to build on the foundations established by government (starting in the Howard years) and industry in this country, to take advantage of rapidly changing technology and patterns of health and social care. The Purpose of the report is to provide the Commonwealth Government and National Mental Health Commission with an up-to-date picture of eMH services in Australia and to propose achievable and scalable solutions to unlock the even greater potential of eMH for the community. The Alliance’s recommendations show how these services can:
be sustainable and continue to assist Australians over the long term;
deliver efficacious, non-stigmatising and immediate support to even more individuals and families;
lower the currently increasing health costs to government;
be funded as a continuing component of the Australian mental health system, rather than as isolated experiments or innovation projects; and
for the first time be linked together as a sector and integrated into a fully functional and more efficient mental health system of stepped care that complements public and private practice.
To achieve this vision, it is recommended that:
1. Australian eMH services are linked together in a “chain or ecosystem of care” with the facility for cross referral where indicated, and they are also linked into the health system at multiple points to enhance referral through several routes:
a) directly from individuals or via community-based organisations (e.g. schools, workplaces)
b) directly from telephone help and crisis lines and online services as referrals of through creating service pathways
c) via primary care (e.g. general practice); and d) via referral by public and private specialist mental health services (e.g. allied
health professionals and NGOs). All eMH services will be linked via an integrated software platform, such as the Synergy Project, which is being used to link youth mental health services. This will facilitate data linkage, referrals and inter-operability across the “chain or ecosystem of care”.

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
4
2. All Commonwealth funded mental health services are required to educate and make the public aware of eMH services as an option available to them using consistent national messages. Together with direct-to-the-public awareness raising initiatives, they will address the limited levels of eMH awareness in the community, particularly in relation to the effectiveness and accessibility of eMH services and empower consumers and families to seek them out or ask for a referral.
3. Training and education programmes for health professionals (such as eMHPrac) are continued in order to:
a) build awareness of existing eMH health programmes and services; b) develop systems that allow for successful incorporation of referral and
follow-up into routine face-to-face practice; and c) coordinate with organisations and professionals in community organisations
(e.g. school counsellors), in a staged approach to expansion.
Training and education programmes for non-health professionals are introduced to build awareness about self-directed eMH programmes and establish systems for client referral to those programmes.
4. A sustainable funding model is established which:
a) includes incentives to General Practitioners (GPs) and eligible allied health professionals (e.g. psychologists) to refer patients to low cost eMH services;
b) identifies and supports areas of unmet need, and funds subsequent innovation, to investigate new models of service delivery;
c) supports the generation and reporting of outcome data, quality control and advice in the form of shared standards, safety protocols and accreditation, while still allowing for the development of new services;
d) incorporates and supports the ongoing nature of programme enhancements and technical upgrades; and
e) takes account of the ethical issues that arise with changes in technology, mental health online delivery, and mental health research.
5. Time-limited governance arrangements are established to facilitate the implementation of Recommendations 1-4, including the re-establishment of the eMental Health Advisory Committee.

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
5
WHAT IS e-MENTAL HEALTH?
e-Mental Health (eMH) is the delivery of services targeting common mental health problems through online and mobile phone interactive websites, apps, sensor-based monitoring devices and computers. The term also extends to telephone crisis lines and online crisis support services. eMH services are delivered in real-time through multiple settings, including the home, the workplace, schools, and through clinicians’ workplaces. Some services offer fully automated self-help programmes, while others involve guidance from clinicians, crisis workers, teachers, administrators or peers. The term e-mental health (eMH) in this paper does not refer to the Government’s work around the Personally Controlled Electronic Health Record. Five types of eMH service or programmes can be distinguished: (see Table 1 for details about individual services/programmes, along with their URLs)
1) Health promotion, wellness promotion and psycho-education Examples of these programmes include BluePages, beyondblue, ReachOut.com, mindhealthconnect, KidsMatter, MindMatters, HeadsUp, Man Therapy and Beacon.
2) Prevention and early intervention Examples of these programmes include BiteBack, Kids Helpline, BraveOnline, Climate Schools, beyondblue’s Support Service, eCouch and MoodGYM.
3) Crisis intervention and suicide prevention Examples of these programmes include Lifeline, Healthy Thinking and ibobbly
4) Treatment Examples of these programmes include myCompass, eCouch, MoodGYM, This Way Up, Mental Health Online, SHADE, eheadspace and others.
5) Recovery and mutual/peer support Examples of these programmes include BlueBoard, an online internet support group for people with depression, or telephone support lines staffed by mental health consumers.
Overall, eMH services in Australia make up an efficient, effective sector, complementary to conventional face-to-face delivery of mental health services. Consumers increasingly are showing their willingness to utilise services delivered through technological means, which supports the importance of linking these services together as a sector and regarding them as components of a fully functional and integrated mental health system.
WHO ARE WE? The e-Mental Health Alliance authored the “e-Mental Health 2020 Vision and Strategy for Australia” in 2009 (1), which outlined the need for efficient eMH service delivery in Australia. This provided the basis for the Government’s “e-Mental Health Strategy for Australia” (2), released in 2012.

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
6
Today, five years on from our initial 2009 “e-Mental Health 2020 Vision and Strategy for Australia”, we review achievements in eMH in Australia, assess the outstanding needs, and propose solutions, in particular the need for a fully integrated and comprehensive eMH care sector that is funded as a continuing component of the Australian mental health system, rather than as isolated experiments or innovation projects. The present document focuses on services currently provided to the community. However, the Alliance aims to include other key players and innovations in the eMH space as new services develop. This includes the broad range of eMH developments currently underway at the Young and Well CRC (e.g. Online Well-Being Centre, Project Synergy, Recharge mobile phone app), beyondblue (e.g. national rollout of redeveloped MindMatters, HeadsUP and New Access) and professional clinic developments at the University of Sydney (e.g. eMH clinical staging) and Orygen Health.
e-MENTAL HEALTH IN AUSTRALIA TODAY
Australia is a world leader in the research, development and delivery of eMH solutions. Table 1 lists eMH promotion, psycho-education, prevention, early intervention, crisis intervention, suicide prevention, treatment, and recovery services provided by Alliance partners. The Department of Health’s Telephone Counselling, Self Help and Web-based Support Programme (Teleweb) supports a number of these services, including the key portal site – mindhealthconnect – which provides links to e-mental health programmes and services, a virtual clinic – MindSpot – and the e-Mental Health in Practice (eMHPrac) training programme which promotes the use of eMH services in primary care settings, plus a range of specific promotional or therapeutic interventions. The Department of Health’s Taking Action to Tackle Suicide (TATS) funding funds a number of other services. Australia’s eMH services are distinguished by the following features:
They are based on “gold standard” evidence.
They lower health costs by limiting the amount of real time involvement of health professionals in the delivery of an ‘episode of care’.
They facilitate help seeking behaviours by people with mental health and suicide issues, and assist those who may not seek traditional health services.
They support the creation of pathways between eMH services and conventional services including primary health care.
They can be easily and cheaply scaled up, and disseminated widely.
STRENGTHS OF THE e-MENTAL HEALTH SECTOR
1. High usage Australian eMH services cater to a range of audiences with different needs and are accessed at high rates, as per Table 1. eMH services are popular, accessible, and acceptable, and appeal to young people, who tend not to access traditional health services (3). Australians report being willing to use eMH services (4, 5) and these services are viewed as acceptable

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
7
as seeing a health professional (6). They are also popular owing to their low or no cost, privacy, anonymity, convenience, and accessibility at any time of day.
eMH services adhere to clinical risk management and security standards. Teleweb-funded services have regular IT security audits and penetration tests which are conducted by independent IT security auditors, sites are hosted by providers with high ISO accreditation, and there is strict adherence to IT governance procedures. With respect to clinical risk, consumers are routinely screened for symptom severity before registration and during programme use, inbuilt alert mechanisms trigger service responses, with users referred or offered face-to-face assistance.
2. Clinical Effectiveness The clinical effectiveness of Australian eMH services is now well-established in all five domains of eMH. A detailed overview of the high levels of clinical effectiveness of Australian eMH services is provided in Table 3. In brief: a) Health promotion, wellness promotion and psycho-education Health promotion and psycho-education programmes (e.g. BluePages) are effective in reducing symptoms (7, 8), while providing consumers with social connections in a safe, non-stigmatising environment. Well implemented programmes providing information and training in community settings such as schools (e.g. KidsMatter) are associated with improvements in academic performance (9), symptoms and behaviours (10) They can also facilitate referral to other services, particularly for hard to reach groups such as men (e.g. Man Therapy) (11) and distressed young people who have not previously accessed health services (e.g. ReachOut.com) (12). b) Prevention and early intervention Contacts with Kids Helpline regarding mental health, emotional wellbeing, suicide, and self-harm have been increasing, with young people reporting that the service provides strategies enabling them to better cope with their concerns (13). beyondblue’s support service which offers brief telephone, email and web chat counselling and referrals have also been found to reduce distress, connect people to treatment and increase motivation to act (14). Positive psychology websites targeting young people (e.g. BiteBack) reduce depression and stress, while improving well-being (15). Internet-based prevention in schools is effective for substance use (e.g. Climate Schools) (16), and depression and anxiety (e.g. MoodGYM) (17), while early intervention with children can reduce anxiety (e.g. BRAVE), with gains persisting for up to 12 months (18). c) Crisis intervention and suicide prevention One third of callers to Lifeline telephone crisis line and almost half of visitors to Lifeline online crisis support chat service report feeling suicidal at the time of contact. Visitors to Lifeline’s online crisis support chat service report decreased distress and sense of aloneness and increased confidence to cope with problems (19). Furthermore, 50% of Lifeline visitors utilised service referrals to access other mental health services including many eMH services. Likewise, there is a measurable reduction in suicidality during a service session for callers to Kids Helpline (20).

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
8
Preliminary data suggest that web-based interventions targeting distress, suicide ideation and impulsivity, such as Black Dog’s Healthy Thinking and ibobbly, can reduce suicidal thinking (21). d) Treatment (e-therapies) Treatment services (e.g. e-couch, myCompass, ThisWayUP) targeting clinical and sub-clinical populations using online cognitive behaviour therapy programmes are effective in reducing symptoms in depressive and anxiety disorders (22-24), with effects comparable to face-to-face treatments (23). The number-needed-to-treat is estimated to be 2.18 (23). The effectiveness of these CBT programmes translates to “real world conditions” (25). They improve work and social functioning (26), they are effective with comorbid alcohol or substance use problems (e.g. SHADE) (27), and integrate with primary care services (28), and psychological treatment services (29). Online interpersonal therapy (IPT) can also reduce symptoms (30). e) Mutual support and recovery services There is evidence that facilitated participation in an online support group (e.g. BlueBoard) (31) can reduce symptoms of depression. Peer support is a promising but under-researched area. Although many of the existing eMH services were developed for people with mild-moderate symptoms, eMH increasingly is being found to be useful for people with more severe symptoms.
3. Cost efficiency International research (including some Australian eMH programmes) shows that delivery of eMH is both cost-effective and cheaper to provide than care as usual (24), particularly for depressive and anxiety disorders. There is significant return on investment from eMH services, which leads to improvements in both cost-benefit ratios and sustainability of care (32). For example, a social return on investment study of Lifeline Online Crisis Support Chat service estimated a return of $8.40 for every $1 dollar invested in this service (19). Figure 1 illustrates a preliminary estimation of costs related to delivering eMH treatments in comparison with the cost of providing other mental health services in Australia. For example, a cost-utility analysis of clinical trial data from the myCompass programme for depression and anxiety shows that the programme can be delivered in a cost-effective manner, with a cost per QALY gain of $3508 (unpublished data). This is approximately one fifth the cost of treatment with antidepressants and a tenth the cost of recommended treatment with a psychologist to achieve the same QALY gain. Recent estimates in Australia have shown that high psychological distress increases employee absenteeism and decreases work productivity up to 20.9%, translating to an annual loss of $5.9 billion (33). Cost-effective treatment services can reduce costs associated with lost productivity (34).

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
9
Figure 1: Stepped care model of eMH service provision and associated costs

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
10
The cost-effectiveness and lower overall expenditures of eMH in relation to other services arise from:
The low marginal costs of providing eMH services to individuals
Volume savings as the number of patients treated increases
Significant clinical improvement despite reduced, minimal or no therapist support, reducing per patient costs while maintaining efficacy (35)
Reduced referrals to secondary mental health services and shortened waiting lists for face-to-face therapy in primary and secondary care (36)
Use of lower cost non-clinical services for information, crisis support and peer support purposes, supplementing the higher cost services as appropriate
Additional benefits arising from immediate and unrestricted access to treatment, easier disclosure of sensitive information, removal of the need to travel to a therapist, and availability of eMH programmes for booster or revision sessions to prevent relapse.
Dissemination of eMH services can also potentially reduce demand on primary and secondary services and lessen medication use and chronicity, leading to further reductions in the individual and societal cost burden. Furthermore, recent overseas research into online preventive interventions reported that they have the potential to be cheaper to implement than some treatment services, even before taking into account lost productivity due to illness (37). Research indicates that the successful prevention of mental illness has the largest impact on labour force participation of any condition (38).
CHALLENGES TO THE e-MENTAL HEALTH SECTOR Although they are acceptable, effective and cost effective, eMH services face challenges. Below we outline three major challenges and their potential solutions. A table showing the challenges and the effects of investment in our strategic response to such challenges is included in the appendix (Table 3).
1. Awareness of eMH services requires attention During a given 12 month period in Australia, 3.2 million people experience a mental disorder such as anxiety, depression, substance abuse (39). However, in 2007, only 34.9% of people with a mental disorder accessed services from a mental health professional (39), with this figure rising to 45% in 2010 through the Better Access Initiative (2). Increasing awareness of eMH services by both the public and health professionals would increase the number of those with a disorder seeking and receiving help, at a significantly reduced cost than increasing traditional face-to-face services. Importantly, the existing high levels of community awareness of national crisis lines and online services, such as Lifeline, could be better harnessed to facilitate the promotion of eMH services.

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
11
Solution: Improve community and professional awareness about the existence and effectiveness of eMH services and programmes and systematically address barriers to use. Establish protocols for referral to eMH services via crisis lines and online services to improve awareness and use of eMH services.
2. eMH services have a place in the health system, but their potential has not been realised and there has been fragmentation in funding and therefore implementation. There is a need to provide access points in multiple (health and non-health) settings, to integrate across providers and with face-to-face health systems, in order to offer tailored responses.
Funding shortages and resource scarcities in the eMH sector have resulted in fragmentation and competition, with consequences for service quality, sustainability and treatment fidelity. The number of services, apps, and websites has produced an increasingly non-integrated system and there are likely to be services with low security and poor adherence to ethical protocols. Solution: The largest gap in mental health service delivery in Australia is for people with mild-moderate mental health disorders (see Table 4). Considering current numbers of people living with mental disorders, based on diagnosis and severity, we estimate that approximately 600 000 people experiencing a mild-to-moderate mental illness are potentially eligible for access to an eMH intervention as a first line of treatment, where interventions are acceptable to the individual. International estimates of future mental health expenditure indicate that the number of cases will increase by 14.2% over the coming 20 year period, service costs will increase by 45% (40), and total cumulative costs associated with mental illness are expected to increase over six-fold (41). While mental disorders make a relatively small contribution to mortality, they are a major disabling condition and will account for 24.2% of all years lost to disease (42).
Table 4: Gaps in mental health treatment access, by symptom severity
Rate of people with a mental disorder accessing treatment (by severity) (43)
Access to treatment as a % of the population living with a mental disorder
N of people living with mental disorders potentially eligible for eMH (44)
Severity Current Target Existing gap
Current Target Existing gap
Anxiety, Affective or Substance use
Mild 25% 50% 25% 2.7% 5.4% 2.7% 444 495
Moderate 59% 80% 21% 2.5% 3.4% 0.9% 172 859
Severe 93% 100% 7% 2.6% 2.8% 0.2%
Total 46% 65% 19% 7.8% 11.6% 3.8% 617 354 NOTE: This table estimates the number of Australian people living with a mental disorder (based on 12 month prevalence data) who would potentially be eligible for eMH services as part of a stepped care intervention. These estimates are derived from epidemiological survey data, combined with administrative data on people receiving mental health care from the Commonwealth
and State and Territories. Targets are based on expert opinion (44).

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
12
Thus, there is substantial economic gain to be made from optimising the prevention and treatment of mental ill health. eMH has the potential to attenuate the impact on resources and costs associated with increased population treatment rates, whilst maintaining effectiveness by leveraging existing technologies. We propose that eMH is integrated within the existing health care system using a stepped care model, with eMH services routinely offered to people with mild-moderate depression and anxiety as a first step (Figure 1), in keeping with the stepped-care framework identified in international guidelines as the method by which treatments for depression should be delivered (45). Access to these services could be direct and through GPs and other face-to-face providers, to ensure that more Australians can be reached, particularly young people in schools and universities (46), those not in contact with health care services (e.g. different cultural groups)(47), those who do not want to access support through traditional mental health services (e.g. men and young people) and people in the workplace. In addition, eMH providers need to be linked in a “chain or ecosystem of care” with governance arrangements that cover referral in and out of each of each other’s services, depending on need and severity (Figure 2). The advantages of offering eMH treatments as a first step in a stepped care model arise because:
Minimal interventions can provide ‘significant health gain’ equivalent to that of traditional psychological therapies, at least for a proportion of patients (equivalence).
Using minimal interventions allows current healthcare resources to be used more efficiently (technical efficiency).
Minimal interventions and the stepped care approach are acceptable to patients and professionals (acceptability).
Figure 1 illustrates how people can either commence a low impact, low cost eMH programme following a referral pathway, or directly engage with an eMH service provider. It also shows how treatment is escalated depending on the response of the individual. The costs of each level of intervention are estimated from our analysis of baseline costs of providing an eMH programme (based on the recent cost effectiveness analysis of myCompass). Costs to the provider for each additional intervention (e.g. GP visit, medication) are based on the current MBS schedule of fees for each professional service, and costs to the patient are based on fee schedules from the Australian Psychological Society. Costs for one course of antidepressant drugs are taken from the Pharmaceutical Benefits Scheme website. Emphasis is on continuity of care, continuity of employment/income, and consequent decreased morbidity for patients.

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
13
3. eMH services need to better incorporate prevention and recovery services, address low adherence and incorporate user input into design. Findings are mixed about the amount and type of support that is optimal to maximise outcomes and there is a need to continually update service platforms to remain compatible with new technologies.
Solution: eMH services will improve via better incorporation of consumer preferences during the design process, identification and removal of barriers to adherence, consistent and ongoing evaluation of newer support models, use of new technologies (e.g. sensor based measures), and customisation for a greater range of cultural groups. Funding to undertake enhancements and extensions of the programmes is an essential component to overcoming these sectoral challenges.
RECOMMENDATIONS
Our vision is for Australia to have a high quality eMH care system, delivering care through a connected eMH ecosystem, which links seamlessly with the broader Australian healthcare system and expanding beyond it. Figure 2 below illustrates this vision by showing interactive referral pathways that encompass multiple points of entry to an integrated model of service delivery. To achieve this vision, it is recommended that:
1. Australian eMH services are linked together in a “chain or ecosystem of care” with the facility for cross referral where indicated, and they are also linked into the health system at multiple points to enhance referral through several routes:
a) directly from individuals or via community-based organisations (e.g. schools, workplaces)
b) directly from telephone help and crisis lines and online services as referrals of through creating service pathways
c) via primary care (e.g. general practice); and d) via referral by public and private specialist mental health services (e.g. allied
health professionals and NGOs). All eMH services will be linked via an integrated software platform, such as the Synergy Project, which is being used to link youth mental health services. This will facilitate data linkage, referrals and inter-operability across the “chain or ecosystem of care”.
2. All Commonwealth funded mental health services are required to educate and make the public aware of eMH services as an option available to them using consistent national messages. Together with direct-to-the-public awareness raising initiatives, they will address the limited levels of eMH awareness in the community, particularly in relation to the effectiveness and accessibility of eMH services and empower consumers and families to seek them out or ask for a referral.
3. Training and education programmes for health professionals (such as eMHPrac) are continued in order to:

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
14
a) build awareness of existing eMH health programmes and services; b) develop systems that allow for successful incorporation of referral and
follow-up into routine face-to-face practice; and c) coordinate with organisations and professionals in community organisations
(e.g. school counsellors), in a staged approach to expansion.
Training and education programmes for non-health professionals are introduced to build awareness about self-directed eMH programmes and establish systems for client referral to those programmes.
4. A sustainable funding model is established which:
a) includes incentives to General Practitioners (GPs) and eligible allied health professionals (e.g. psychologists) to refer patients to low cost eMH services;
b) identifies and supports areas of unmet need, and funds subsequent innovation, to investigate new models of service delivery;
c) supports the generation and reporting of outcome data, quality control and advice in the form of shared standards, safety protocols and accreditation, while still allowing for the development of new services;
d) incorporates and supports the ongoing nature of programme enhancements and technical upgrades; and
e) takes account of the ethical issues that arise with changes in technology, mental health online delivery, and mental health research.
5. Time-limited governance arrangements are established to facilitate the implementation of Recommendations 1-4, including the re-establishment of the eMental Health Advisory Committee.
The benefits to Australian mental health from these recommendations can be seen in Table
3 (Appendix).

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
15
Figure 2: Proposed innovations to eMH service delivery

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
16
APPENDIX
Table 1 – AUSTRALIAN eMH SERVICES and USAGE
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
HEALTH PROMOTION, WELLNESS PROMOTION AND PSYCHO-EDUCATION Beacon
https://beacon.anu.edu.au/
Key audience: consumers and health practitioners
Provides guidance on the content, quality and availability of –ehealth applications including online tools, mobile apps and online support groups
Consumer and researcher ratings are provided
9,810 unique visitors per month, on average.
No registration required.
76,503 pages accessed per month, on average
Beyondblue
http://www.beyondblue.org.au/
Key Audience: all Australians
Communication and education through provision of comprehensive information on depression and anxiety including recognising symptoms
Promotes early action and recovery
208,000 visitors per month, on average
No registrations required
Black Dog Institute
http://www.blackdoginstitute.org.au
Key audience: all Australians
Information, education, psycho-education focused on depression, bipolar disorder and anxiety disorders
Screening tools, referrals to eMH programs and clinicians
Contact point for community education programs
121,332 unique visitors per month, on average
276,115 unique page views per month, on average
No registrations required
1,823,656 annual visitors
BluePages
http://bluepages.anu.edu.au
Key audience: people with depression
Evidence based information about depression
Automated screening tools for depression and anxiety
Information about the experience, symptoms and diagnosis of depression
Information about psychological, medical and alternative/lifestyle treatments for depression
9,701 unique visitors per month, on average
No registrations required
229,638 pages accessed per month, on average
HeadsUp
http://www.headsup.org.au/
Key Audience: workplaces, employer groups and business leaders
Online resource providing information about mental health and the workplace. The website offers simple tools e.g. an action plan for business), practical advice, information and resources to take action
87,000 visits to the website in first six weeks
Since June launch 4,700 businesses and individuals have registered for further information on mentally healthy workplaces

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
17
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
HEALTH PROMOTION, WELLNESS PROMOTION AND PSYCHO-EDUCATION (continued from previous page) KidsMatter
National Primary Schools Mental Health Initiative
www.KidsMatter.edu.au
Key audience: school leadership, teachers and parents
Objective: strengthen capacity of primary school communities to support children’s social and emotional development and to respond effectively to child mental health issues
Provides online resources and training, links to evidenced-based programs and services
2,000+ school communities currently participating
Man Therapy
www.mantherapy.org.au
Key Audience: men - 30-54 years
Practical information for men dealing with stress, anxiety and depression
Online screening tool and links to programs and services
691,302 website visits
152,000 completions of Man Quiz (K10)
Has reached 41% of men aged 30 -54 years (approx 1.5 million)
mindhealthconnect
Healthdirect Australia
www.mindhealthconnect.org.au
Key audience: National e-mental health website for the public and health professionals
Brings together Australia's leading mental health providers in one place
Find relevant mental health and wellbeing information, online programmes, services, tools, news, helplines
Operated by Healthdirect Australia, on behalf of the Australian Federal Government
Data not available at present
MindMatters
National Secondary Schools Mental Health Initiative
Key Audience: school leadership, teachers and parents
Objective: strengthen capacity of secondary school communities to support student resilience and to respond effectively to youth mental health issues
Provides online resources and training, links to evidenced-based programs and services
Online forums
1500 schools to be recruited through to mid-2016
ReachOut.com
www.reachout.com
Key audience: young people aged 14-25
Non-clinical mental health promotion and early intervention service
Information, self-help referral, peer support via online forum
Anonymous, available 24/7, accessible on computers/mobile/tablet
Referral pathways (41% of distressed young visitors to the site said they would be more likely to seek additional help after using R/O)
On average 170,000 unique visitors per month, on average
No registration required
1.7 million annual visits on average

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
18
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
PREVENTION AND EARLY INTERVENTION beyondblue support service
24 hr – 1300 224636
Key audience: people experiencing distress
Telephone (24 hr – 1300 224636), email and web chat counselling with trained mental health professional
Provides brief interventions/support and referral
8,583 contacts per month, on average during the first full year of operation – 2013/14 (telephone, email or web chat)
BiteBack
Black Dog Institute
http://www.biteback.org.au/
Key audience: 12-18 year olds
Prevention
Services: well-being and resilience building
3,400 unique visits per month, on average
75 registrations per month, on average
2,646 registered users since 2011
Brave Online
https://brave4you.psy.uq.edu.au/
Key audience: Children and adolescents with risk factors (e.g. temperament) or early signs of anxiety
Self-help, therapist assisted, or supported by school staff
Full-automated
Current pilot project with 2 schools, available to research populations only
Climate Schools
www.climateschools.com.au
Key audience: secondary school students
Health education courses available via website, with teachers delivering additional activities to reinforce online lessons: alcohol education, alcohol and cannabis use, psychostimulant and cannabis education
313 unique visitors per month, on average
3,716 page views per month, on average
90 schools currently registered and using the programme
e-couch
https://ecouch.anu.edu.au
Key audience: adults aged 20-70years
Information and automated self-help program that includes a literacy component and online tools for prevention and treatment of depression, generalised anxiety disorder and social phobia
Two additional tailored streams for bereavement and loss, and divorce and separation
1,000 community registrations per month, on average
7,256 unique visitors per month, on average
393,038 pages accessed per month, on average
Kids Helpline
1800 55 1800
www.kidshelp.com.au
Key audience: children and young people aged between 5 and 25 years
Kids Helpline Counselling Services – provides free, private and confidential counselling and information/referral for children and young people aged under 26 years across Australia via phone, web and email
www.kidshelp.com.au – provides a range of information and self-help resources for children, young people and adult carers
18,952 counselling contacts per month, on average (15,460 via phone; 1,978 via email; 1,514 via web)
44,531 unique visitors to Kids Helpline website per month, on average
28,105 webpage views of Hot Topics covering information and coping strategies for a variety of problems (14,526 page views of “teens” Hot Topics; 10,666 page views of “grownups” Hot Topics; 2,913 page views of “kids” Hot Topics)
10,337 webpage views of self-submitted stories of young people’s problems and their experiences contacting Kids Helpline
480 connections with Search for a Service function
No registrations required

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
19
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
PREVENTION AND EARLY INTERVENTION (continued from previous page) MoodGYM
http://moodgym.anu.edu.au
Key audience: people at risk of developing a common mental health problem or who are experiencing depression or anxiety symptoms
Automated, self-help CBT for depression with 5 modules and 29 online exercises
9,400 community registrations per month, on average
Over 800,000 registrations
36,834 unique visitors per month, on average
3,154,840 pages accessed per month, on average
New Access
http://www.beyondblue.org.au/resources/health-professionals/newaccess-a-beyondblue-program
Key audience: people with mild-to-moderate depression / anxiety.
Trained coaches provide individually tailored low intensity CBT to clients incorporating e-mental health programs/supports
Currently only available to research participants at three pilot sires located in SA, ACT and NSW
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
CRISIS INTERVENTION AND SUICIDE PREVENTION Lifeline
https://www.lifeline.org.au/
Key audience: Australians experiencing a crisis
Lifeline 13 11 14 – national telephone helpline
Lifeline Online Crisis Support Chat Service – one on one confidential chat service
Lifeline Suicide Hot Spot crisis line – specialist telephone helpline
Lifeline Online ‘Get Help – self-help resources at lifeline.org.au
Lifeline 13 11 14: average 60,000+ calls per month, on average
Online Crisis Support Chat: average 2,500 contacts per month
Suicide Hot Spot Crisis Line: average 1,500 calls per month
No registrations required
lifeline.org.au – on average 58,000+ unique visitors per month
Online ‘Get Help’ resources – 8,000 unique page views per month
Referrals to other services – 2/3 of callers and chat visitors receive referral to other services
iBobbly
Black Dog Institute
Key audience: Aboriginal and Torres Strait Islander peoples aged 16-35 years.
Treatment for suicidal ideation based on acceptance and commitment therapy
Currently undergoing upgrades and improvements
Currently only available to research participants in pilot study in the Kimberley, WA
Public release date TBA

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
20
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
TREATMENT AND E-THERAPY SERVICES BraveOnline
http://www.brave.psy.uq.edu.au/index_brave.html
Key audience: children and adolescents with anxiety disorders
Fully automated online intervention for anxiety in youth, delivered via computer, mobile phone or tablet
Minimal therapist assistance
Cognitive behavioural therapy, problem solving therapy, cognitive challenging, exposure
delivered via 10 interactive modules for young people (plus 2booster sessions)
6 interactive modules for parents (plus booster sessions)
Separate programmes for children vs adolescents
Additional programme with specific sessions for social phobia
To date, the clinician supported version of the programme is only accessible via research group in Australia
Being used with clinically anxious children post the Christchurch earthquake
e-couch
http://ecouch.anu.edu.au
Key audience: adults aged 20-70years
Information and automated self-help program that includes a literacy component and online tools for treatment of depression, generalised anxiety disorder and social phobia
Two additional tailored streams for bereavement and loss, and divorce and separation
1,000 community registrations per month, on average
7,256 unique visitors per month, on average
393,038 pages accessed per month, on average
OnTrack, QUT
www.ontrack.org.au
Key audience: Australians with a health problem
Information services for a range of health conditions
Self-rated quizzes on drinking, mood and relationships with feedback supplied
Interactive online programmes for depression, alcohol & depression, family & friends, psychosis, flood and storm recovery, diabetes
iPhone/iPad apps for meditation
iPad app, Stay Strong, which is used by workers in Indigenous health settings
1,400+ unique visitors per month, on average
No registrations required for screening
916 registrations for web programmes
63,526 page views since 2009
Mental Health Online
https://www.mentalhealthonline.org.au
Key audience: adults aged 18 years or more
Information and self-guided assessment for 21 disorders
Guided and unguided self-help online CBT for generalised anxiety disorder, obsessive compulsive disorder, panic disorder, depression, insomnia, PTSD and social anxiety disorder, as well as a trans-diagnostic programme (depression and anxiety) for same-sex attracted young people
Tailored integrated resources for people with comorbid problems
Availability of therapist support via e-mail, text chat, voice-over internet, video chat and within a VR space
Additional programmes offered through participation in research (e.g. depression, insomnia, compulsive hoarding)
eTherapist Online training and placement opportunities
1,380 unique visitors per month, on average
625 registrations per month, on average
22,098 page views per month, on average

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
21
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
TREATMENT AND E-THERAPY SERVICES (continued from previous page) MoodGYM
http://moodgym.anu.edu.au
Key audience: people with depression or anxiety symptoms. Designed for young people but used by all ages.
Automated, self-help CBT for depression with 5 modules and 29 online exercises
9,400 community registrations per month, on average
Over 800,000 registrations
36,834 unique visitors per month, on average
3,154,840 pages accessed per month, on average
myCompass
Black Dog Institute
www.mycompass.org.au
Key audience: people with mild-mod depression and anxiety
Fully automated online intervention for depression and anxiety, delivered via computer, mobile phone or tablet
Cognitive behavioural therapy, problem solving therapy, positive psychology and interpersonal psychotherapy delivered via 12 interactive self-help modules
Real time tracking/monitoring of symptoms
4,545 unique visits per month, on average (users and general public)
310 registrations per month, on average
24,711 page view per month, on average
15,028 registered users since June 2012
SHADE
National Drug and Alcohol Research Centre, UNSW
www.shadetreatment.com
Key audience: people aged 18 years and over with depression and comorbid substance use problems
Fully automated online intervention incorporating CBT, motivational enhancement training, mindfulness and relapse prevention
Minimal therapist assistance (10-15 minutes per session) via email, telephone or in clinic
Available in 10-session programme (weekly sessions) or a skills module version (1-2 hours each)
Clinician supported version of the programme is only offered via research group in Australia
ThisWayUp
St Vincent’s Hospital
www.thiswayup.org.au
Key audience: people with common mental health problems
Online clinic for registered health providers and their patients
CBT for major depressive disorder, generalized anxiety disorder, panic disorder, social phobia, obsessive compulsive disorder, and co-morbid anxiety and depression
Self-help web intervention for mixed anxiety and depression, crisis management, social phobia
Online courses for schools to teach students how to manage depression and anxiety, alcohol and drugs
1,000 unique visitors per month, on average
Clinic site: 80 patient and 40 clinician registrations per month on average
275 self-help site registrations per month, on average
6,000 registrations to self-help courses since
500 primary and high schools registered to use the courses as part of their lessons
SERVICE ORGANISATION KEY AUDIENCE AND SERVICES PROVIDED USAGE
RECOVERY AND MUTUAL SUPPORT SERVICES BlueBoard
http://blueboard.anu.edu.au
Key audience: people with common mental health problems
Moderated internet support group
Available 24/7; moderated 7am-10pm
Separate bulletin board forums for depression, bipolar, anxiety, social anxiety, panic disorder and borderline personality disorder
110 new member registrations per month
6,073 posts per month, on average
5,408 unique visitors per month, on average
210,671 pages accessed per month, on average

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
22
Table 2 – CLINICAL EFFECTIVENESS and COST EFFICIENCY of AUSTRALIAN eMH SERVICES
Name of programme Number of research trials
Effect sizes Cost data Setting Target and Reference
HEALTH PROMOTION, WELLNESS PROMOTION AND PSYCHO-EDUCATION SERVICES BluePages http://bluepages.anu.edu.au
1 x RCT (quasi indicated prevention)
Within group effect size: d=0.4 (depression symptoms) and d=0.5 for completers Between group effect size d=0.29 (depression symptoms) and d=0.35 for completers (12m follow up)
Community Depression symptoms, depression literacy; reductions in stigma (7, 8)
PREVENTION, EARLY INTERVENTION AND SUICIDE PREVENTION BiteBack http://www.biteback.org.au/
1 x RCT Between group effect sizes: overall d=0.22 (depression symptoms) d=0.34 (high adherence users)
Open access, Australia-wide, community-based trial
Well-being, resilience, depression and anxiety symptoms (15)
Climate schools www.climateschools.com.au
3 x RCTs Within group effect sizes at post: d=0.23 (average alcohol consumption), d=0.2 (binge drinking). AT 6 month follow up: d=0.18 (average alcohol consumption); d=0.19 (cannabis use) At 12 month follow-up: d= 0.38 (average alcohol consumption), d=0.17 (binge drinking); d=0.31 (cannabis use)
Australian secondary school students
Alcohol and drug use, alcohol and drug knowledge, alcohol and drug-related harms, overall wellbeing. (16)
eCouch http://ecouch.anu.edu.au (see also: treatment data)
4 x RCT quasi-indicated prevention trials + 1 x equivalence trial
University/staff users social anxiety stream e-couch; Between group pre-post difference: d=0.71 – 0.93 (for social anxiety). Spontaneous users; e-couch depression IPT and CBT streams: Within group d= 0.80 (ITT) and d=1.44 for completers (depression, CBT); d= 0.67 (ITT) and d=1.02 (completers) (depression, IPT) Cardiovascular disease; d=0.18 (depression) and d=0.16 (anxiety)
Community/young people in the community People with cardio vascular disease
Depression and anxiety (30, 48, 49)
MoodGYM https://moodgym.anu.edu.au
8 quasi indicated prevention; 1 x universal prevention
Within group effect sizes: d=0.4 (depression) and d=0.6 for completers Between group: g=1.19 (depression) and g=0.23 (alcohol misuse)(6 months) Between group:g=0.57 (depression), g=0.74 completers and g=0.82 compliers
Cost effective to translate into another language: 16 QALYS gained per 1,000 treated persons; CER=3,432
Community, schools, universities, lifeline, workplace, NHS choices, Brain Injury
(17, 46, 50)

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
23
Name of programme Number of
research trials Effect sizes Cost data Setting Target and Reference
CRISIS INTERVENTION AND SUICIDE PREVENTION Lifeline 13 11 14 https://www.lifeline.org.au/
N/A N/A
Social Return on Investment study of Lifeline Online Crisis Support Chat service in 2013 calculated a return of $8.40 for this service.
Community based adults
Crisis intervention with suicidal Australians (19)
TREATMENT AND E-THERAPY SERVICES BraveOnline
http://www.brave.psy.uq.edu.au/index_brave.html
3 x RCTs Within group effect sizes at 12 month follow up d=1.85 (child self-reported anxiety); d=2.58 (Clinician Severity Rating)
Adolescents with anxiety
Anxiety symptoms (18, 51)
e-couch https://ecouch.anu.edu.au
3 X RCTs + 1 equivalence trial
e-couch community users: Between group effect size d=2.43 ( generalised anxiety) University/staff social anxiety stream: Between effect (social anxiety ‘cases’) OR=1.7 (social anxiety) Community users e-couch: Between effect (depression ‘cases’): OR= 5.3 (depression) Spontaneous users e-couch CBT: within group effect sizes (depression ‘cases’) d= 0.65 (ITT, 6 mths; (depressive symptoms).
Community (Metro/ regional/rural) University
(30, 31, 48)
Mental Health Online https://www.mentalhealthonline.org.au
Uncontrolled ongoing ‘real world’ open access service results
Within group effect sizes: Social anxiety automated: d=0.84; Post traumatic stress disorder automated : d=0.72; Obsessive compulsive disorder automated: d=0.83; Panic automated: d=1.12; Generalised anxiety disorder automated : d=1.22; In press data re: effect on depression: Panic automated: d=.30; Post-traumatic stress disorder automated: d=.36; Obsessive compulsive disorder automated: d=.33; Generalised anxiety disorder automated: d=.42; Social anxiety disorder automated: d=.07
GAD Online: Therapist-assisted vs face-to-face 59% cost saving; Self-help vs face-to-face 61% cost saving Panic Online iCBT $350 vs. telephone CBT $378 vs. psycho-education only $55 PTSD Online (V1) PTSD ONLINE found to be 3.7 times less expensive than the current cost for psychological therapist time in the traditional face-to-face modality. Anxiety Online (whole service) Estimated labour time cost saving resulting from the Anxiety Online service in the first 18 months of operation is therefore estimated at AU $6.7 million.
Open access real world
Primary and secondary mental health symptoms, number of disorders, confidence in managing mental health and psychological distress (52-54)

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
24
Name of programme Number of
research trials Effect sizes Cost data Setting Target and Reference
TREATMENT AND E-THERAPY SERVICES MoodGYM http://moodgym.anu.edu.au
8 x RCT+2CTs + 1 equivalence trial +1 uncontrolled trial (one TBI)
Within group effect sizes: d=0.9 (depression caseness) completers Callers Lifeline; Between group effect 6 mths (depression ‘cases’): 1.2 (ITT) and 1.4 completers Spontaneous users: Within group effect (depression ‘cases’): =0.61 and 1.36 for completers (at 6 mths). University students between group: g=0.68-0.86 (mild to severe depression ‘cases’) completers and g=0.40-0.90 compliers, Guided primary care between group effect size at post: d=0.65 & d=1.1
Spontaneous users; schools; universities; primary care (GP supported); psychologists; Lifeline; NHS Choices online health portal; public mental health services; brain injury
(30, 55, 56)
myCompass www.mycompass.org.au
1 x RCT 1 x uncontrolled trial (diabetes related distress)
Between group effect sizes at post: myCompass vs attention control - d=0.36 (depression); d=0.4 (anxiety); d=0.22 (stress); d= 0.22 (work and social adjustment) myCompass vs waitlist d=0.46 (depression); d=0.47 (anxiety); d=0.35 (stress); d=0.29 (work and social adjustment) Within group effect sizes myCompass d=0.24 (anxiety)-0.49(depression, work and social adjustment) Diabetes trial within group effect sizes at post (unpublished): d=1.05 (depression); d=0.68 (anxiety); d=04 (work and social); d=1.15 (diabetes distress) Diabetes within group effect sizes at 3 month follow up: d=0.74 (depression); d=0.48 (anxiety); d=0.57 (work and social); d=1.04 (diabetes distress)
Net Monetary Benefits for MyCompass are $12187 for 12 months vs $9245 for face-to-face CBT and $9206 for TAU. [unpublished]
Adults with mild-moderate depression, stress and anxiety Adults with diabetes related distress and mild-mod stress, depression and anxiety
Anxiety, depression & work and social adjustment (26, 57)
OnTrack www.ontrack.org.au
1 x RCT 1 x pilot
Between group effect sizes at 3 month follow up: Unguided brief vs full intervention: d=0.55 (depression); d=0.42 (psychological quality of life)
Adults with depression and alcohol misuse
Depression and alcohol use Depression and psychological quality of life QOL
SHADE www.shadetreatment.com
2 x RCTs 3 x pilots
At 12-month follow-up: DEPRSSION: Clinician-assisted SHADE (d=0.97) vs. therapist-delivered CBT (d=1.16), vs. 1-session (d=0.71), vs. supportive counselling (d=1.03); ALCOHOL: Clinician-assisted SHADE (d=0.87) vs. therapist-delivered CBT (d=1.05), vs. 1-session (d=0.85), vs. supportive counselling (d=0.75) CANNABIS: Clinician-assisted SHADE (d=0.75) vs. therapist-delivered CBT (d=0.53), vs. 1-session (d=0.07), vs. supportive counselling (d=0.17).
SHADE used a minimum of 50% less clinician time than the specialist therapist-delivered CBT to produce equivalent outcomes through to 3-years post-treatment
Adults with depression and alcohol or cannabis or amphetamine use in the community
Depressive symptoms Alcohol use Cannabis use Amphetamine (27, 58) use
e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
25
Name of programme Number of
research trials Effect sizes Cost data Setting Target and Reference
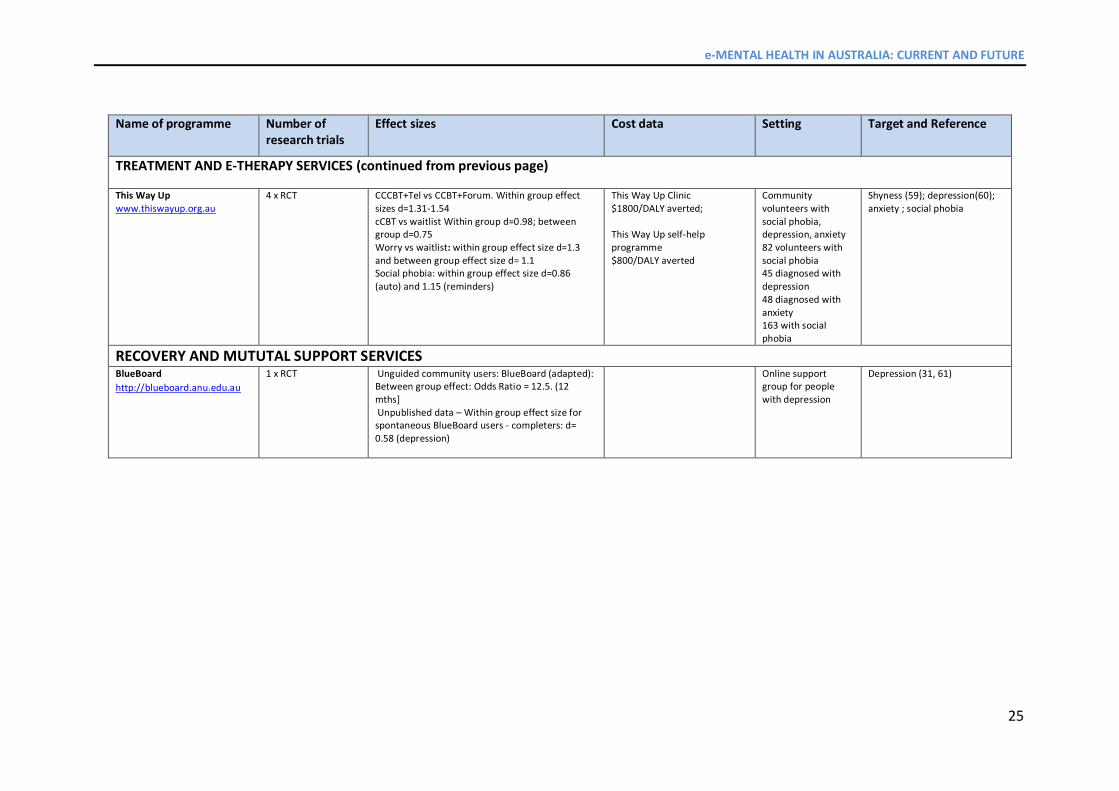
TREATMENT AND E-THERAPY SERVICES (continued from previous page)
This Way Up www.thiswayup.org.au
4 x RCT CCCBT+Tel vs CCBT+Forum. Within group effect sizes d=1.31-1.54 cCBT vs waitlist Within group d=0.98; between group d=0.75 Worry vs waitlist: within group effect size d=1.3 and between group effect size d= 1.1 Social phobia: within group effect size d=0.86 (auto) and 1.15 (reminders)
This Way Up Clinic $1800/DALY averted; This Way Up self-help programme $800/DALY averted
Community volunteers with social phobia, depression, anxiety 82 volunteers with social phobia 45 diagnosed with depression 48 diagnosed with anxiety 163 with social phobia
Shyness (59); depression(60); anxiety ; social phobia
RECOVERY AND MUTUTAL SUPPORT SERVICES BlueBoard
http://blueboard.anu.edu.au
1 x RCT Unguided community users: BlueBoard (adapted): Between group effect: Odds Ratio = 12.5. (12 mths] Unpublished data – Within group effect size for spontaneous BlueBoard users - completers: d= 0.58 (depression)
Online support group for people with depression
Depression (31, 61)

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
26
Table 3 – STRATEGIC INVESTMENT SUMMARY Challenge Benefits Strategic
Response Solution Assets
Changes
Many people with a mental health problem do not get treated in the community
KP1 More Australians will know about mental health services available through the internet KP2 More Australians will seek these services
eMH Alliance Plan is adopted
Awareness campaigns to raise understanding of the availability, safety and efficacy of eMH services
Leverage existing relationships and Funding through Teleweb and other measures
The current GP and mental health services systems are overloaded with consumers who may benefit from eMH health resources.
KP1 More Australians will receive evidence based psychotherapy through a stepped care approach KP2 More Australians are referred to appropriately tailored services, as well as being referred in and out of eMH services KP3 More GPs, psychologists, allied health professionals and NGOs will be trained and feel confident to use eMH tools
eMH services offered through a ‘chain or ecosystem of care’ which takes account of severity and time need Integration of face-to-face and eMH services to reflect need Education programmes for health professionals and GPs New items/measures for accreditation of effective services, products and devices
The costs of GP systems are mounting
KP1 Costs per person will decline as 30% are expected to respond to automated/less costly care/ with majority in mild-to-moderate.
eMH will be offered as a preferred first step treatment in primary care
Common mental health problems are treated too late, and the window for prevention is missed
KP1 New cases are identified and treated by eMH programmes in schools, universities and workplaces. Prevalence drops by 22% through prevention programmes.
Prevention programmes in schools, universities and workplaces use evidence-based eMH
Consumers feel they are not supported in their recovery and demand better services
KP1 More Australians will communicate through online recovery boards and where appropriate be referred to other services KP2 Consumers will be supported through peer-to-peer support mechanisms.
More managed eMH recovery services with potential for linkage to face-to-face services

e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
27
REFERENCES 1. Christensen H, Proudfoot J, Andrews G, Klein B, Kavanagh D, O'Neil D, et al. E-Mental Health: A 2020 Vision and Strategy for Australia. 2009. 2. Australian Government Department of Health. E-mental health strategy for Australia 2012 [27 Aug 2014]. Available from: http://www.health.gov.au/internet/publications/publishing.nsf/Content/mental-pubs-e-emstrat-toc. 3. Australian Bureau of Statistics. 4326.0 - National Survey of Mental Health and Wellbeing 2007 2008 [19 Aug 2014]. Available from: http://www.abs.gov.au/ausstats/[email protected]/Latestproducts/4326.0Main%20Features12007?opendocument&tabname=Summary&prodno=4326.0&issue=2007&num=&view=. 4. Klein B, Cook S. Preferences for e-mental health services amongst an online Australian Sample. e-Journal of Applied Psychology. 2010;6:19-27-39. 5. Proudfoot J, Parker G, Hadzi Pavlovic D, Manicavasagar V, Adler E, Whitton A. Community attitudes to the appropriation of mobile phones for monitoring and managing depression, anxiety, and stress. J Med Internet Res. 2010;12:e64. 6. Schneider J, Sarrami Foroushani P, Grime P, Thornicroft G. Acceptability of online self-help to people with depression: Users’ views of MoodGYM versus informational websites. J Med Internet Res. 2014;16:e90. 7. Griffiths KM, Christensen H, Jorm AF, Evans K, Groves C. Effect of web-based depression literacy and cognitive-behavioural therapy interventions on stigmatising attitudes to depression: randomised controlled trial. Br J Psychiatry. 2004;185:342-9. 8. Mackinnon A, Griffiths KM, Christensen H. Comparative randomised trial of online cognitive-behavioural therapy and an information website for depression: 12-month outcomes. Br J Psychiatry. 2008;192:130-4. 9. Dix KL, Slee PT, Lawson MJ, Keeves JP. Implementation quality of whole-school mental health promotion and students’ academic performance. Child and Adolescent Mental Health. 2012;17:45-51. 10. Slee P, Lawson M, Russell A, Askell-Williams H, Dix K, Owens L, et al. KidsMatter Primary Evaluation Final Report. Centre for Analysis of Educational Futures: Flinders University of Australia, 2009. 11. Ipsos SRI. Beyondbarriers Strategy Evaluation Report. Project 12-087906-01 2014 [24 Sep 2014]. Available from: http://www.beyondblue.org.au/docs/default-source/research-project-files/bw0240_ipsos-sri_beyond-barriers-evaluation-final-report_final_200514.pdf?sfvrsn=0. 12. ReachOut, Inspire Foundation. 2013 ReachOut.com Annual User Survey Results: Who uses ReachOut.com and how it helps them 2013 [28 Aug 2014]. Available from: http://inspire.org.au/wp-content/uploads/2014/07/2013-ReachOut.com-Annual-User-Survey.pdf. 13. Kids Helpline. Kids Helpline Overview: the key issues affecting kids and young people in Australia in 2013: BoysTown; 2013 [11 Sep 2014]. Available from: http://www.kidshelp.com.au/upload/22957.pdf. 14. nous group. Independent evaluation of beyondblue 2014 [24 Sep 2014]. Available from: http://www.beyondblue.org.au/docs/default-source/research-project-files/bw0265.pdf?sfvrsn=0. 15. Manicavasagar V, Horswood D, Burckhardt R, Lum A, Hadzi-Pavlovic D, Parker G. Feasibility and effectiveness of a web-based positive psychology program for youth mental health: Randomized controlled trial. J Med Internet Res. 2014;16:e140 10.2196/jmir.3176. 16. Newton NC, Teesson M, Vogl LE, Andrews G. Internet-based prevention for alcohol and cannabis use: final results of the Climate Schools course. Addiction. 2010;105:749-59. 17. Calear AL, Christensen H, Mackinnon A, Griffiths KM. Adherence to the MoodGYM program: Outcomes and predictors for an adolescent school-based population. J Affect Disorders. 2013;147:338-44. 18. Spence SH, Donovan CL, March S, Gamble A, Anderson RE, Prosser S, et al. A randomized controlled trial of online versus clinic-based CBT for adolescent anxiety. Journal of consulting and clinical psychology. 2011;79:629-42. 19. netbalance. Social Return on Investment Forecast of the Lifeline Online Crisis Support Chat Service 2014 [11 Sep 2014]. Available from: https://www.lifeline.org.au/.../Lifeline_Online_Crisis_Support_Chat_SROI_report_final.pdf. 20. King R, Nurcombe B, Bickman L, Hides L, Reid W. Telephone counselling for adolescent suicide prevention: changes in suicidali ty and mental state from beginning to end of a counselling session. Suicide Life Threat Behav. 2003;33:400-11. 21. van Spijker BA, Majo MC, Smit F, van Straten A, Kerkhof AJ. Reducing suicidal ideation: cost-effectiveness analysis of a randomized controlled trial of unguided web-based self-help. J Med Internet Res. 2012;14:e141. 22. Andersson G, Cuijpers P. Internet-based and other computerized psychological ytreatments for adult depression: a meta-analysis. Cognitive Behaviour Therapy. 2009;38:196-205. 23. Andrews G, Cuijpers P, Craske MG, McEvoy P, Titov N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: a meta-analysis. PloS one. 2010;5:e13196. 24. Hedman E, Ljotsson B, Lindefors N. Cognitive behavior therapy via the Internet: a systematic review of applications, clinical efficacy and cost-effectiveness. Expert Rev Pharmacoecon Outcomes Res. 2012;12:745-64. 25. Christensen H, Griffiths MK, Korten EA, Brittliffe K, Groves C. A comparison of changes in anxiety and depression symptoms of spontaneous users and trial participants of a cognitive behavior therapy website. J Med Internet Res. 2004;6:e46. 26. Proudfoot J, Clarke J, Birch MR, Whitton AE, Parker G, Manicavasagar V, et al. Impact of a mobile phone and web program on symptom and functional outcomes for people with mild-to-moderate depression, anxiety and stress: a randomised controlled trial. BMC Psychiatry. 2013;13:312. 27. Kay-Lambkin FJ, Baker AL, Lewin TJ, Carr VJ. Computer-based psychological treatment for comorbid depression and problematic alcohol and/or cannabis use: a randomized controlled trial of clinical efficacy. Addiction. 2009;104:378-88. 28. Hickie IB, Davenport TA, Luscombe GM, Moore M, Griffiths KM, Christensen H. Practitioner-supported delivery of internet-based cognitive behaviour therapy: evaluation of the feasibility of conducting a cluster randomised trial. Med J Aust. 2010;192:S31-5. 29. Twomey C, O'Reilly G, Byrne M, Bury M, White A, Kissane S, et al. A randomized controlled trial of the computerized CBT programme, MoodGYM, for public mental health service users waiting for interventions. Br J Clin Psychol. 2014. 30. Donker T, Bennett K, Bennett A, Mackinnon A, van Straten A, Cuijpers P, et al. Internet-delivered interpersonal psychotherapy versus internet-delivered cognitive behavioral therapy for adults with depressive symptoms: randomized controlled noninferiority trial. J Med Internet Res. 2013;15:e82. 31. Griffiths KM, Mackinnon AJ, Crisp DA, Christensen H, Bennett K, Farrer L. The effectiveness of an online support group for members of the community with depression: a randomised controlled trial. PloS one. 2012;7:e53244.
e-MENTAL HEALTH IN AUSTRALIA: CURRENT AND FUTURE
28
32. Lokkerbol J, Adema D, Cuijpers P, Reynolds C, Schulz R, Weehuizen R, et al. Improving the cost-effectiveness of a healthcare system for depressive disorders by implementing telemedicine: a health economic modeling study. Am J Geriatr Psychiatry. 2014;22:253-62. 33. Hilton M, Scuffham P, Vecchio N, Whiteford H. Using the interaction of mental health symptoms and treatment status to estimate lost employee productivity. Aust N Z J Psychiatry. 2010;44:151-61. 34. Lim D, Sanderson K, Andrews A. Lost productivity among full-time workers with mental disorders. J Ment Health Policy Econ. 2000;3:139-46. 35. Hedman E, Ljotsson B, Ruck C, Bergstrom J, Andersson G, Kaldo V, et al. Effectiveness of internet-based cognitive behaviour therapy for panic disorder in routine psychiatric care. Acta Psychiatr Scand. 2013;128:457-67. 36. Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J. A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety. Health Technol Assess. 2002;6:1-89. 37. Ruby A, Marko-Holguin M, Fogel J, Van Voorhees BW. Economic analysis of an internet-based depression prevention intervention. J Ment Health Policy Econ. 2013;16:121-30. 38. Laplagne P, Glover M, Shomos A. Effects of health and education on labour force participation. . Melbourne: Productivity Commission, 2007. 39. Slade T JA, Teesson M, Whiteford H, Burges P, Pirkis J, et al. The Mental Health of Australians 2: Report on the 2007 National Survey of Mental Health and Wellbeing. Canberra: Department of Health and Ageing, 2009. 40. McCrone P, Dhanasiri S, Patel A. Paying the price: the cost of mental health care in England to 2026. . London: King's Fund, 2008. 41. Smetanin P, Stiff D, Briante C. The life and economic impact of major mental illnesses in Canada: 2011 to 2041. . Mental Health Commission of Canada, 2011. 42. Begg S, Vos T, Barker B. The burden of disease and injury in Australia 2003. PHE 82. Canberra: AIHW, 2007. 43. Whiteford H, Buckingham W, Harris M. Estimating treatment rates for mental disorders in Australia. Aust Health Rev. 2014;38:80-5. 44. Andrews G. Tolkien II Team. Tolkien II: A Needs-based, Costed Stepped-care Model for Mental Health Services. World Health Organization Collaborating Centre for Classification of Mental Health, 2007. 45. National Collaborating Centre for Mental Health. Depression: The NICE Guideline on the Treatment and Management of Depression in Adults, updated edition. London: British Psychological Society and Royal College of Psychiatrists, 2010. 46. Calear AL, Christensen H, Mackinnon A, Griffiths KM, O’Kearney R. The YouthMood Project: A cluster randomized controlled trial of an online cognitive behavioral program with adolescents. J Consult Clin Psych. 2009;77:1021-32. 47. ReachOut. "Whenever I need it" : Special report on the help provided to LGBTQI young people who access ReachOut.com 2014 [28 Aug 2014]. Available from: http://inspire.org.au/wp-content/uploads/2014/02/ReachOut.com_Report-Special-Report-on-LGBTQI-service-users-Feb2014.pdf. 48. Bowler JO, Mackintosh B, Dunn BD, Mathews A, Dalgleish T, Hoppitt L. A comparison of cognitive bias modification for interpretation and computerized cognitive behavior therapy: effects on anxiety, depression, attentional control, and interpretive bias. Journal of consulting and clinical psychology. 2012;80:1021-33. 49. Glozier N, Christensen H, Naismith S, Cockayne N, Donkin L, Neal B, et al. Internet-delivered cognitive behavioural therapy for adults with mild to moderate depression and high cardiovascular disease risks: a randomised attention-controlled trial. PloS one. 2013;8:e59139. 50. Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the internet: randomised controlled tr ial. BMJ. 2004;328:265. 51. Spence SH, Holmes JM, March S, Lipp OV. The feasibility and outcome of clinic plus internet delivery of cognitive-behavior therapy for childhood anxiety. Journal of consulting and clinical psychology. 2006;74:614-21. 52. Klein B, Meyer D, Austin DW, Kyrios M. Anxiety online: a virtual clinic: preliminary outcomes following completion of five fully automated treatment programs for anxiety disorders and symptoms. J Med Internet Res. 2011;13:e89. 53. Klein B, Mitchell J, Abbott J, Shandley K, Austin D, Gilson K, et al. A therapist-assisted cognitive behavior therapy internet intervention for posttraumatic stress disorder: pre-, post- and 3-month follow-up results from an open trial. Journal of anxiety disorders. 2010;24:635-44. 54. Klein B, Richards JC, Austin DW. Efficacy of internet therapy for panic disorder. Journal of behavior therapy and experimental psychiatry. 2006;37:213-38. 55. Farrer L, Christensen H, Griffiths KM, Mackinnon A. Internet-based CBT for depression with and without telephone tracking in a national helpline: randomised controlled trial. PloS one. 2011;6:e28099. 56. Høifødt SR, Lillevoll RK, Griffiths MK, Wilsgaard T, Eisemann M, Waterloo K, et al. The clinical effectiveness of web-based cognitive behavioral therapy with face-to-face therapist support for depressed primary care patients: randomized controlled trial. J Med Internet Res. 2013;15:e153. 57. Harrison V, Proudfoot J, Wee PP, Parker G, Pavlovic DH, Manicavasagar V. Mobile mental health: Review of the emerging field and proof of concept study. J Ment Health. 2011;20:509-24. 58. Kay-Lambkin FJ, Baker AL, Kelly B, Lewin TJ. Clinician-assisted computerised versus therapist-delivered treatment for depressive and addictive disorders: results of a randomised controlled trial. . Med J Aust. 2011;195:S44-S50. 59. Titov N, Andrews G, Schwencke G, Solley K, Johnston L, Robinson E. An RCT comparing effect of two types of support on severity of symptoms for people completing internet-based cognitive behaviour therapy for social phobia. Aust NZ J Psychiat. 2009;43:920-6. 60. Perini S, Andrews G, Titov N. Clinician-assisted Internet-based treatment is effective for depression: Randomized controlled trial. Aust NZ J Psychiat. 2009;43:571-8. 61. Griffiths K, Crisp D, Christensen H, Mackinnon A, Bennett K. The ANU WellBeing study: a protocol for a quasi-factorial randomised controlled trial of the effectiveness of an Internet support group and an automated Internet intervention for depression. BMC Psychiatry. 2010;10:20.