dysphagia presentation by muhammad naeem
TRANSCRIPT

Roll no.294 , 261.

Learning outcomeat the end of this discussion studentsshould be able to ;
Learn the history and examination
Differential diagnosis
Investigation
Treatment and management.

Dysphagia means difficulty in swallowing.
Disease of the esophagus causing dysphagia are both structural and functional.
In structural disease,dysphagia is more marked to solids while in functional disease,it is more marked to liquids .
Painful swallowing is called odynophagia.

Painful conditions of oral cavity. Any painful condition of mouth and throat
(stomatitis,tonsillitis) will cause dysphagia.
Lesion is visible on examination of oral cavity.
Reflux esophagitis Abnormal reflux of gastric contents into the lower
esophagus is the most comon cause of esophagitis .
Reflux is most likely to occur in smokers and obese.

Symptoms. Patient gives history of retrosternal burning sensation
and pain(heart burn)which increase on bending forward and on lying flat.
It’s relieved by antacids.
Water brash (excessive salivation due to reflex stimulation of salivary glands as acid enters the esophagus) is common.
Bitter taste in the morning is frequent.
Aspiration of regurgitant material can cause laryngitis (hoarseness of voice) and aspiration pneumonia(nocturnal cough which mimics asthma)
Signs.
Patient may look pale; otherwise there is no physical sign on examination.
Investigation. Barium swallow will demonstrate reflux .esophygeal
ulcers may be seen.
Endoscopy shows hyperemic mucosa with or without ulcers .
pH monitoring is more objective way of documentation and quantification of reflux and establishing its relation with symptoms.

Treatment. 1.proton pump inhibitors.
Omeprazole,esomeprazole,lansoprazole,rabeprazole,pantoprazole_these drugs equal in efficacy.and increase the pH of gastric contents to a level above 4.0.
H2 blockers should be only used if the patient has very mild ,intermittent symptoms.ranitidine,cimetidine.

3.surgery.
<5% will not responds to PPIs and will need to undergo surgery.
Laproscopic Nissen fundoplication.
Placing a circular purse-string suture in the LES to tighten it.
Benign esophageal stricture. There is narrowing of esophagus due to fibrosis.
Reflus esophagitis is the most common cause.
It can also occur after corrosive ingestion.

Symptoms Past history suggestive of reflux esophagitis.
There is slowly progressive dysphagia for solids.
Food sticks in esophagus.
It never leads to complete aphagia
Signs No abnormal physical sign.
Patient may be pale and malnourished.
Investigations On barium swallow, there is narrowing of lower end of
esophagus.
Endoscopy will show narrowing and inflammation
Brush cytology and multiple biopsies required to exclude malignancy.
CA esophagus It occurs in smoking , old age, barrett’s oesophagus
and achalasia.

Symptoms Rapidly progressive dysphagia to solids.
Weight loss is marked.
Patient may develop complete aphagia.
Signs Patient may look pale, malnourished and wasted.

Investigations Barium swallow will show narrowing of esophagus
with irregular margins.
Endoscopy will show stricture/ mass.
Brush cytology and multiple biopsies will confirm diagnosis.
treatment Surgical resection if the disease is sufficiently localized
to esophagus.
5-flourouracil-based chemotherapy is combined with radiation to control locally metastatic disease.

Paralytic dysphagia It is due to weakness of pharyngeal muscles.
Causes.
1.Bulbar/pseudobulbar palsy.
2.myesthenia gravis.
3.polymyositis and dematomyositis.
4.Oculopharyngeal myopathy.
Symptoms and signs Dysphagia is more directed to liquids.
History of nasal regurgitation may be present.
Signs of 10th cranial nerve palsy may be present.(hoarseness of voice with nasal character and soft palate doesn’t move when patient is asked to say “ah”.
Achalasia Lower esophegeal sphincter does not relax in response
to swallowing.
It is a congenital disorder in which ganglion cells in esophagus are less than normal.
Similar situation can also arise in Chagas disease.

Signs and symptoms Long history of dysphagia to solids and liquids.
Vomiting may also be present which is foul smelling and contains food eaten several days ago.
History of recurrent chest infections may be present due to regurgitation.
Clinical examination may be normal.
Investigations Chest X-ray may show widened mediastinum with
dilated esophagus with air fluid level behind cardiac shadow.
Barium swallow shows dilated esophagus with pointed termination (bird’s beak sign).
Endoscopy shows dilated esophagus with smooth mucosa. Endoscopy is necessary to exclude carcinoma.
Manometry shows poor motility of esophagus and lack of lower esophegeal sphincter relaxation

treatment Pneumatic dilation –effective in 80 to 85% patient.
Botulinum toxin injections into LES_ used in those patients whom pneumatic dilation has failed.
If upper both therapies failed than surgical myotomyis performed.

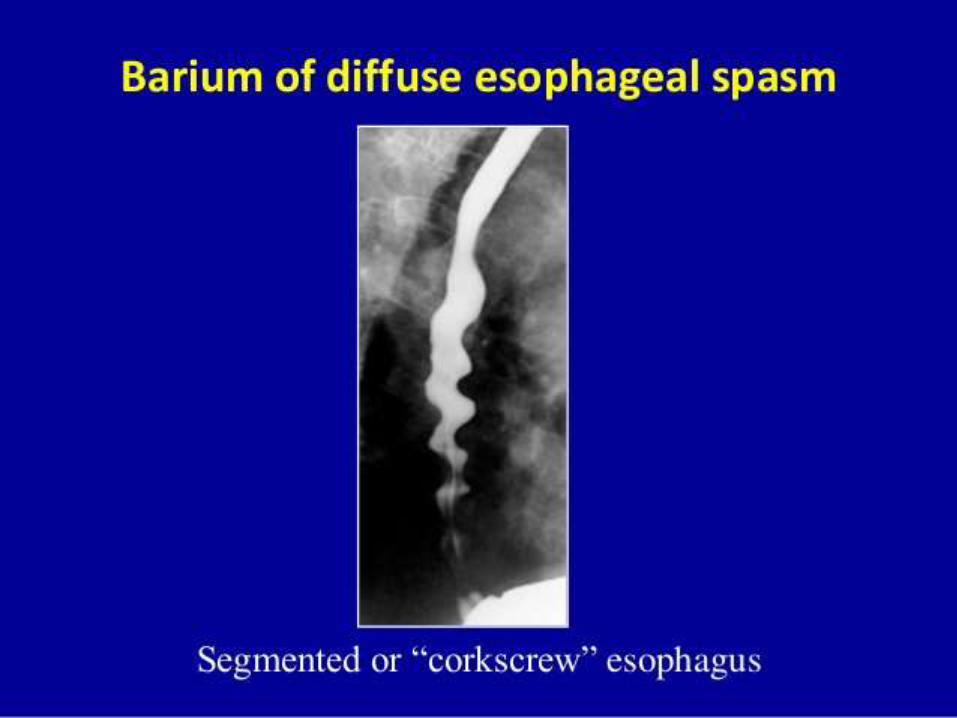
Diffuse esophageal spasm and Nutcracker Esophagus. Esophageal spastic disorders are idiopathic
abnormalities of the neural processses of the esophagus.
Sign and symptoms. Intermittent chest pain and dysphagia.
Pain is not associated with exertion and eating food.
Its precipitated by drinking cold liquids.

investigation Barium studies may show “corckscrew” pattern at the
time of spasm.
The most accurate test is manometric studies.

treatment Calcium channel blockers ,such as nifedipine and
nitrates.

Scleroderma Generalized disorder of connective tissue affecting
skin and many other organs.
Motility of gut is decreased.
Symptoms Reflux esophagitis and dysphagia.
Intermittent abdominal pain, distention, constipation due to hypomotility (pseudo-obstruction)
Fingers swollen , stiff and tips become ulcerated.
Trismus
Raynaud phenomenon.
Polyarthritis
Renal failure (malignant hypertension)
Dyspnea due to pulmonary fibrosis.

Signs Fingers may be swollen. Tips may be ulcerated with or
without calcinosis. Movements are painful.
Skin becomes thick and tight over fingers , face and bony prominences.
Telengiectasis may be present.
Investigations ESR normal.
Anemia due to iron and B12 deficiency ( malabsorption)
Anti Nuclear Antibodies present.
Calcinosis seen on X-ray.
Barium swallow shows dilated esophagus and loss of peristalsis in distal esophagus, patulous LES.
Barium follow through shows delayed emptying in small bowel.
Skin biopsy confirms diagnosis..
treatment Proton pump inhibitors.omeprazole.and
metoclopramide.

Plummer Vinson syndrome; Dysphagia, iron deficiency anemia and glossitis are
features.
Hypopharyngeal web is responsible for dysphagiawhich is demonstrated on barium swallow.
Dysphagia is intermittent and sometimes to liquids as well.
Treat the iron deficiency and dilation procedures for dysphagia.
Compression of esophagus fromoutside Causes are retrosternal thyroid, enlarged mediastinal
lymph nodes( due to lymphomas , leukemias and metastasis) and enlarged left atrium due to mitral stenosis.
Signs and symptoms Dysphagia to solids.
Swelling of face ( if Superior vena cava obstructed)
Symptoms of underlying disease are present.
Thyroid may be enlarged
Pamberton’s sign may be present
Signs of superior vena caval obstruction may be present.
Signs of mitral stenosis may be present.

Investigations Chest X-ray shows wide mediastinum.
Barium swallow shows narrow esophagus.
Endoscopy excludes any esophegeal lesion.
Retrosternal thyroid is picked up on thyroid scan.
CT scan, bronchscopy, Mediastinoscopy and biopsies confirm diagnosis.
Globus Hystericus It is feeling of persistent lump in throat unrelated to
act of swallowing.
No dysphagia.
Responds to psychotherapy and anxiolytics
Clinical scenario A 32 year old man comes to emergency department for
substernal chest pain and burning senation for 2 hours duration.he says that he sometimes gets this pain while lying in bed at night.He is otherwise free of symptoms except for a non productive cough..His physical examination is unremarkable.His ECG is normal.
Clinical scenario. A 62 year old man comes for evaluation of progressive
“difficulty swallowing solids and recently semisolids”.He has noticed a 9-kg weight loss.His past medical history is significant for reflux esophagitis for 15 years and a 40 pack year of smookinghistory.physical examination is unremakable except a lymh node is palpabe in left supraclavicular fossa.
Diagnosis?
Clinical scenario A 32 year old woman comes to your office for the
evaluation of “dificulty swallowing” for solids and liquids foods for one year. She also gives history of vomiting that’s foul smelling and contains food particles.Her symptoms has not worsened all over this time.and weight has been stable.physical examination is unremarkable.
