duke masters of minimally invasive thoracic surgery orlando…€¦ · · 2017-09-19duke masters...
TRANSCRIPT

Duke Masters of Minimally Invasive Thoracic Surgery
Orlando, FL
September 17, 2016
Session V: Minimally Invasive Esophageal Surgery
Giant Paraesophageal Hernia
James D. Luketich MD, FACS
Henry T. Bahnson Professor and Chairman,
Department of Cardiothoracic Surgery
University of Pittsburgh Medical Center
Overview
• Hiatal Hernia Overview and Clinical Presentation
• Review important principles learned from the
open surgical repair of giant paraesophageal hiatal
hernias
• Discuss results of open surgical series of GPEH
• UPMC Results of laparoscopic series of GPEH

Background: Giant
Paraesophageal Hiatal Hernia
• GERD is frequently associated with a simple Type I hiatus
hernia, surgical approach is generally laparoscopic
• Giant Paraesophageal Hernias are less common and
probably represent a progression of Type I hernia to a
Type III
• Most type IIIs are symptomatic and a small percent lethal
• These giant hiatal hernias are more complex to repair, lead
to more recurrences and have been traditionally managed
by open surgery

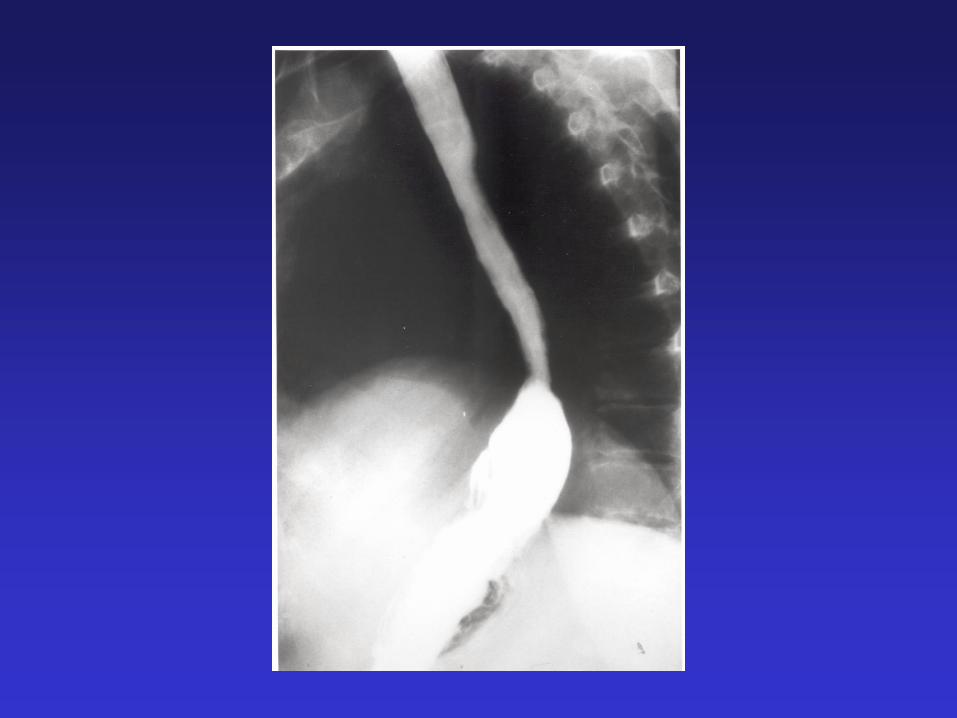
Typical Esophagram of Giant
PEH Intra-thoracic
Stomach

The Essential Steps to Successful Repair of
Giant Paraesophageal Hiatal Hernia-1
• Open surgical results of GPEH are good in the hands of experienced esophageal surgeons
• Results depend upon important operative steps:
– Identification of the plane between the hiatal hernia sac and mediastinal pleura and meticulous dissection of the hernia sac
– Mobilization of the crura, maintaining the peritoneal lining and the integrity of the crural muscle
– Tension-free approximation of intact crura, if either of these conditions cannot be met, consider mesh cruroplasty

• Mobilization of the esophagus, maintianing vagal nerve viabiity to deliver a tension free, 2-3 cm segment of intra-abbdominal esophagus
• If this cannot be achieved, continue mediastinal mobilization, if this still cannot be achieved, consider an esophageal lengthening procedure or an aggressive pexy following as much mobilization as possible
• Perform an anti-reflux procedure, preferably a floppy, 2 stitch Nissen
• If these principles are followed meticulously using an open or laparoscopic approach, good long-term outcomes can be achieved
The Essential Steps to Successful Repair of
Giant Paraesophageal Hiatal Hernia-2

Controversies
• Open vs. minimally invasive
• Primary crural repair vs. buttressed with
mesh
• Short esophagus: ? Incidence, what to do if
present?
• Learning curve series vs extensive
longitudinal experience
• Elective Vs. Emergent
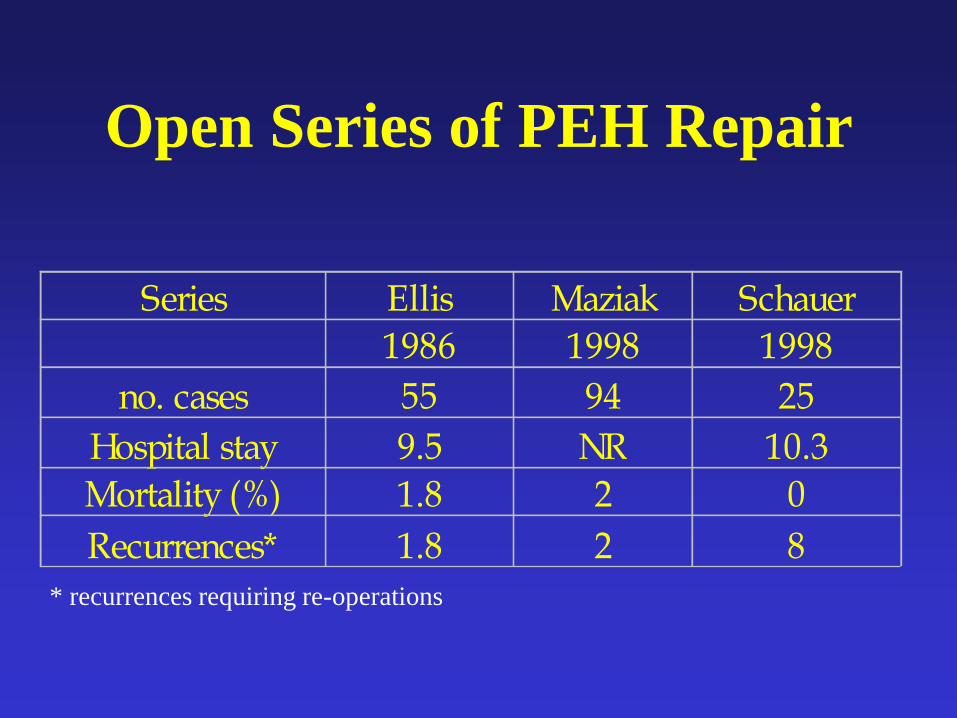
Open Series of PEH Repair
Series Ellis Maziak Schauer
1986 1998 1998
no. cases 55 94 25
Hospital stay 9.5 NR 10.3
Mortality (%) 1.8 2 0
Recurrences* 1.8 2 8
* recurrences requiring re-operations
Open Repair of Giant PEH with
Collis Gastroplasty and Belsey:
Maziak and Pearson • 94 patients with intra-thoracic stomach (type III) operated
upon over a 20 year period
• Operative approach
– Left thoracotomy
– sac excision
– Collis lengthening procedure for shortened esophagus
– no deaths, 1% leak rate
• 91% with good results, 9% with fair results
• At a mean follow-up of 10 years only 2 re-operations required
• JTCVS 1998

Surgical Outcomes: Concerns Over
Increased Morbidity and Recurrences
Associated with Laparoscopic Repair of
Giant Hiatal Hernias
• Laparoscopic report from the Mayo Clinic: 30-day
mortality 5.4%
– Recurrence rate in short-term follow-up: 13%
– First 37 cases
• Similar experience elsewhere in first 50 cases
Deschamps, et al. Ann Thorac Surg. October 2001.

Recurrence Rate of Following
Laparoscopic Repair of Giant Hiatal
Hernia (USC Initial experience)
42
15
0
5
10
15
20
25
30
35
40
45
%
Recurrence
Laparoscopic
Open
• Hashemi et al USC
J Am Coll Surg 2000

Prevalence of a recurrent hernia in the 41
patients (21 open and 20 laparoscopic) that had annual
videoesophagrams
for a minimum of 3 years.
DeMeester et al ; American College of Surgeons 2010, JACS 2011

Role of Mesh in GPEH:
Randomized Trial
• Randomized trial of Surgisis mesh for repair of GPEH
• Median follow-up 6 months interim results closed the trial
– Mesh are 9% recurrence
– Non-mesh arm 16% recurrence
• Their conclusion: Mesh must be used
• Other Conclusions:
– Recurrence rate concerning in either arm, surgical experience not stated to enroll patients
– Results DO NOT depend on a single variable!
Oelschlager et al. American Surgical Association 2006, Ann Surg 2006

Role of Mesh in GPEH
Randomized Trial: Long term Follow-up
• Randomized trial of Surgisis mesh for repair of GPEH
• Median follow-up of 58 months (range 42 to 78 mo)
• 72 completed clinical follow-up and60 repeated a UGI (Primary repair n= 34; Mesh n=26).
• There were 20 patients (59%) with recurrent HH in the Primary repair group – 20 (59%) with recurrent hernia vs. 14 patients (54%) with recurrent HH in the mesh group (p0.7).
• There was no statistically significant difference in relevant symptoms or QOL between patients
Oelschlager et al. J Am Coll Surg 2011

GPEH: Principles of Repair
• Hernia reduction
• Sac resection
• Crural repair
• Fundoplication
• Tension free intra-abdominal repair
• Liberal use of esophageal lengthening

GPEH: Principles of Repair
• Sac dissection (removal from the mediastinum, not necessarily
removal from the body)
• Hernia reduction (occurs by itself if you do the above step
completely)
• Crural repair (primary repair is possible with careful crural
preservation)
• Strive to achieve a tension-free segment of intra-abdominal
esophagus
• If not present, go back to mediastinum and keep working on
mobilization
• If still not present, go back to mediastinum and keep working on
mobilization
• If still not present, consider esophageal lengthening procedure
• Floppy, Nissen fundoplication

• 94 patients ; Massive incarcerated hiatal
hernia
• Transthoracic Repair with Belsey
Fundoplication
• Collis Gastroplasty in 80% of patients
Giant Paraesophageal Hernia:
Open Repair
Maziak, Todd, Pearson JTCVS 1998

What is the incidence of short
esophagus?
Series Year Incidence (%) N
Legacy 1996 14 238
USC 1999 15.6 236
Pittsburgh 2000 27 100
(PEH)
Emory 2001 2.9 1000
Toronto 1998 80 94
Pittsburgh 2002 56 200
(PEH)
Hill Career 0 Career
Emory 2003 4.3 1579

Conditions Associated With
Higher Incidence of Short
Esophagus
•Long standing, severe disease
•Re-do cases
•Stricture
•Non-reducible large hiatal hernia
(>5cm)
•Barrett’s esophagus
•Paraesophageal hernia (type III)

Factors Contributing to Laparoscopic
Failure to Recognize Short Esophagus
• Failure to dissect fat pad and identify esophago-cardia junction
• Failure to recognize a relatively tubularized gastric cardia
• Caudal tension on penrose drain
• Caudal migration with rigid Bougie
• Cephalad migration of diaphragm with pneumoperitoneum pressure
• Failure to have a plan if you do encounter it: “If all you have is a hammer, everything looks like a nail!”

• 94 patients ; Massive incarcerated hiatal
hernia
• Transthoracic Repair with Belsey
Fundoplication
• Collis Gastroplasty in 80% of patients
Giant Paraesophageal Hernia:
Open Repair
Maziak, Todd, Pearson JTCVS 1998
• Follow up : Mean 94 months
• 24 patients followed more than 10 years
• Standard Questionnaire : Every year for 5
years, then 2 year intervals
• Routine Ba Swallow: 1, 5, 10 years
• Follow-up Manometry, pH testing done
selectively
Results : Open GPEH Repair

• Excellent to good results in 94% of patients
• Recurrence in 2 patients (both symptomatic)
• Reoperations in 2 patients (both had Collis
Gastroplasty done during the reoperation)
Results: Open GPEH Repair

Key Elements: Sac Dissection

Key Elements: Sac Dissection
Video
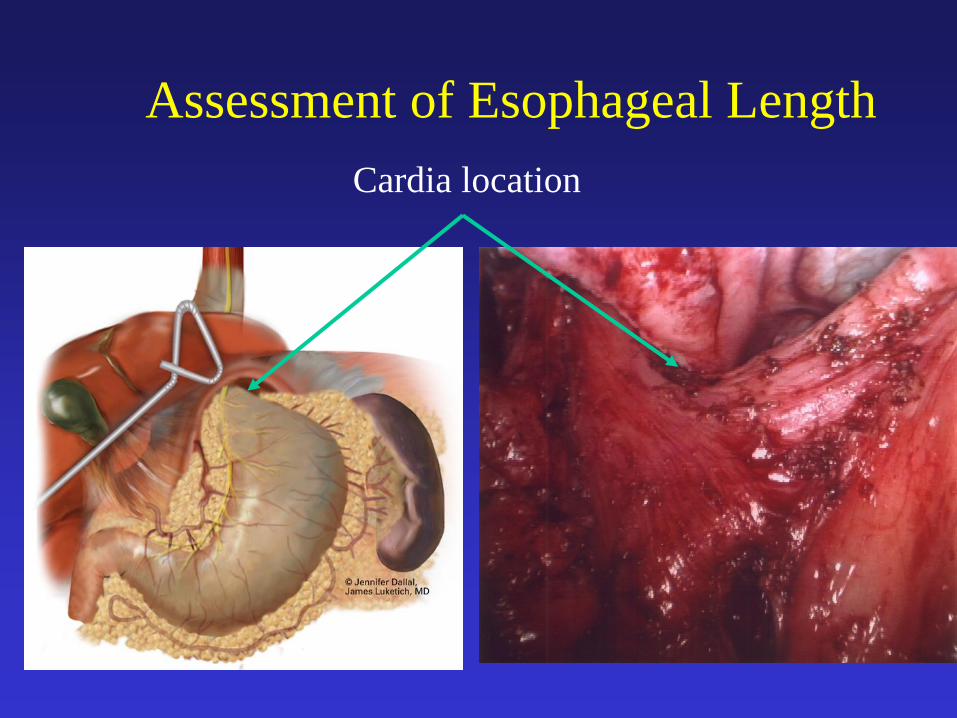
Assessment of Esophageal Length
Cardia location

Key Elements: Maintaining the
Crural Integrity (Video)
What to do if you encounter a
short esophagus?
• Look for it!
• Keep working to gain length !
• Have a plan!
• Open if necessary!
• Laparoscopic Collis in selected cases


Endo-GIA Application to Create Collis Segment

Collis Segment Created with EEA and Endo-GIA
Neo-esophagus

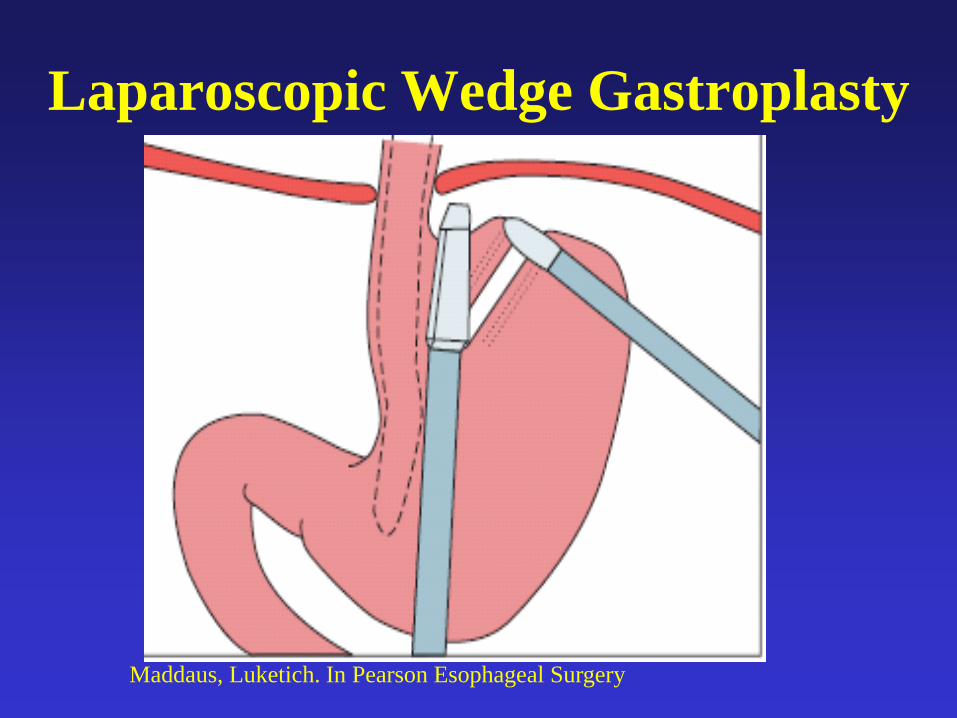
Laparoscopic Wedge Gastroplasty
Maddaus, Luketich. In Pearson Esophageal Surgery

Laparoscopic Wedge Gastroplasty
Maddaus, Luketich. In Pearson Esophageal Surgery
Laparoscopic Wedge Gastroplasty
Maddaus, Luketich. In Pearson Esophageal Surgery

Laparoscopic Wedge
Gastroplasty (Video)

Overview of Completed gastroplasty
Maddaus, Luketich. In Pearson Esophageal Surgery

Factors Contributing to Laparoscopic
Failure to Recognize Short Esophagus
• Failure to dissect fat pad and identify esophago-cardia junction
• Failure to recognize a relatively tubularized gastric cardia
• Caudal tension on penrose drain
• Caudal migration with rigid Bougie
• Cephalad migration of diaphragm with pneumoperitoneum pressure
• Failure of surgeon to have experience with a laparoscopic method of lengthening

Collis Gastroplasty and Reinforced
Crural Repair (Maddaus Series)
• University of Minnesota Series:
• 61 patients underwent Giant Para esophageal Hernia Repair with Collis Gastroplasty, complete fat pad dissection, hernia sac excision with reinforced crural repair, NO Mesh
• Complications: Esophageal leak 1, Pneumonia 1, Death 1
• Mean GERD QOL Score was 1.15 (0=asymptomatic; 45= severe symptoms)
• Ba Esophagram obtained at median of 323 days (4-1080 days)
• Ba Swallow Data available in 54 ( 89%) of patients.
• No short term recurrence; 1 (1. 9%) small asymptomatic recurrence Whitson et al. Presented at the AATS 2006, JTCVS

“Shoe Shine” of Wrap


Laparoscopic Repair of Diaphragm

• 662 patients had attempted non-emergent
laparoscopic repair
• 75% female
• Median age 70 years (IQR 19-92)
• 15% had a BMI ≥35
• 49% had an age-adjusted Charlson
Comorbidity Index score ≥ 3
UPMC Series:
Laparoscopic Repair GPEH
UPMC Series:
Laparoscopic Repair GPEH • 662 patients had attempted non-emergent
laparoscopic repair; 652 (98.5%) completed
laparoscopically
• 63% required Collis gastroplasty
• 13% mesh cruroplasty
• 98% fundoplication (647/662)
– Floppy Nissen 79% (512/647)
– Partial fundoplication 21% (135/647)
• LOS median 3 days
Luketich et al, AATS, JTCVS 2010

Results – Perioperative Outcomes
• Overall rates of major morbidity and
mortality low
– Mortality 1.7% (11/662)
– Pneumonia 4% (29/653)
– Post-operative leak 2.5% (16/653)

Summary of Findings
• Symptomatic improvement is excellent
– 89% of patients express satisfaction with surgery
– 90% report good to excellent GERD-related
quality of life
• Median follow-up: 25 months
• 3.2% of patients underwent reoperation in
subsequent follow-up

UPMC Experience : Long Term Results
• 1997 – 2003 -187 patients with laparoscopic
approach
• Fundoplication in 183/187 (98%), Collis
Gastroplasty in 160/187 (86%) of patients
• Mesh Cruroplasty in 30/187 (16%)
• Median clinical follow up - 77 months
• QOL questionnaire (GERD – HRQOL ; SF
-36)
• Follow up Ba Swallow
Nason K, Luketich et al. Presented at DDW 2008, J Gastr Intest Surg

Long Term Results
• Reoperations in 7 patients (4.4%)
• Ba Swallow – 154 patients
• Median time to Ba swallow: 50 months
• Radiographic Recurrence in 23 patients
(15%)
– 7 (4.4%) chose reoperation
– 16 on medical treatment with variable success
– Crural Mesh reinforcement was not associated
with a reduced risk of radiographic recurrence

UPMC Experience : Long Term
Results
Quality of Life (Obtained at median of 77
months after repair):
GERD HRQOL (0-45) (Fair to excellent in 90%)
• Excellent : 78%
• Good : 8%
• Fair : 4%
• Poor : 9%
SF – 36 (Preserved)
• Physical component score : 52
• Mental component score : 53

Successful Repair of Giant Paraesophageal
Hiatal Hernia?
• No single step is “The Key Step”, Several Important Steps
• Identification of the plane between the hiatal hernia sac and mediastinal pleura and meticulous dissection of the hernia sac
• Mobilization of the crura, maintaining the peritoneal lining and the integrity of the crural muscle
• Tension-free approximation of intact crura, if either of these conditions cannot be met, consider mesh cruroplasty (needed infrequently in our experience)

• Mobilization of the esophagus, maintaining vagal nerve viability to deliver a tension free, 2-3 cm segment of intra-abdominal esophagus
• If this cannot be achieved, continue mediastinal mobilization, if this still cannot be achieved, consider an esophageal lengthening procedure or an aggressive pexy following as much mobilization as possible
• Perform an anti-reflux procedure, preferably a floppy, 2 stitch Nissen
• If these principles are followed meticulously using an open or laparoscopic approach, good long-term outcomes can be achieved
The Essential Steps to Successful Repair of
Giant Paraesophageal Hiatal Hernia-2
Conclusions • Complex giant hiatal hernias can be managed successfully
by the laparoscopic approach in selected, experienced centers – Our long term data 4% operative recurrence rate (6 years plus)
– 12-14% radiographic recurrence rate, some asymptomatic, most small and not at risk of torsion
• Higher recurrence rates reported from less experienced centers
• Failure to recognize and treat a short esophagus contributes to recurrences, mesh in some cases
• Failure to accomplish complete mediastinal sac dissection and maintain crural integrity
• Other factors involved, including the size of the hiatal defect and open and/or laparoscopic operative experience

Thank You