dssri news education support advocacy … december 2010.pdf · prescott h. peirce, co., inc. ......
TRANSCRIPT
DSSRI NEWSDecember, 2010
SUPPORT•
EDUCATION•
ADVOCACY•
PUBLIC AWARENESS
Holiday Party, 2010

2
General Contact and Membership Information
Down Syndrome Societyof Rhode Island, Inc.99 Bald Hill RoadCranston, RI 02920
PHONE: 401-463-5751FAX: 401-463-5337
EMAIL: [email protected]: www.dssri.org
Board of Directors
Steve MuldoonPresident
Adam MooreVice President
Joanne BurgerSecretary
Marilyn BlancheTreasurer
Claudia M. LoweCoordinatorStephanie CerepSaadia CiceroneMatthew CohnJill GauthierStephanie KaczmarzykKatherine LoweSherri Marcantonio-HornBob MacauxRobin StrangKim TevesChristopher Waldeck
Policy DisclaimerThe Down Syndrome Society of Rhode Island, Inc. (DSSRI) was formed by people with a common interest – improving the lives of people with Down syndrome and their families. It is for this reason that we welcome input from various parents and professionals.
We do not, however, as an organiza-tion, support or endorse any particu-lar treatment or therapy. The purpose of this newsletter is to provide a forum for an exchange of ideas.
Please submit information or articles to: DSSRI 99 Bald Hill Road Cranston, RI 02920
DSSRI reserves the right to edit any submissions for appropriate and “person-fi rst” language.
In AppreciationDSSRI NEWS
Kim Teves, REMAX Patriot Properties
Superior Bakery
Shamrock Financial Corp.
Reliable Pest Control
STD MED, Inc.
Pontarelli Funeral Home
Daughters of Isabella
Brian Studley
Cranston Country Club
Santa and Mrs. Claus
IBEW Local #99
Family and Friends of the late Fannie Boober
Citizens Charitable Foundation
Christine Morelli
Fidelity Charitable Gift Fund
Joe Henderson
Patricia Peacock
Peggy Szlosek
Tracey and Phil Rizzuto
“Miss Alice”
Uncle Tony’s Pizza, Cranston, RI
Gayle and Tom Tarzwell
Dr. Sig Pueschel
Gerard Guillemette
Jeffrey DiMillio
Prescott H. Peirce, Co., Inc.
Family Institute of New England, LLC
Crystal Stamping
Warwick Oil Valley Fuel Inc.
Burbank Properties
Pepsi Bottling Company
Stop and Shop, North Kingstown, RI
Starbucks, Garden City
John Johnsen, Sodexho Health Care Services
Taylor Rental, Warwick, RI
Whole Foods, North Main Street, Providence, RI
East Greenwich Fire Department
Shaw’s Admiral Street, North Providence, RI
Seabra, Mendon Road, Cumberland, RI
Frito Lay, Cranston, RI
URI Volunteers
Mackenzie Birrell
Bank of America Matching Gifts
Give with Liberty
Bob and Diane Durgan
East Bay CDC
Jennifer Pesare
Kelly Ducharme
Thomas, Patricia and Maryellen Goodwin
Sheila Connelly
Maureen Larocque
Natalie Melo
Peter and Raquel David
Eduardo and Margaret Melo
The Garofalo’s
Parag & Swati Shah
Kathleen McDonough
Michelle Silva
Donald and Nancy Kinnally
Denise and Anthony Rainha
Carol King
Elizabeth and Robert Iglesias
Paul and Sheila Connelly
Bruce and Cynthia Jacobson
Lynn Domenici
Jacqueline and Phillip Loscoe
Daniel and Margaret Hurley
Regina Dellaposta
Jessica and John Donnelly
David and Cheryl Langevin
David and Karen Stenhouse
Eric and Deanna Fallon
William Kostka
Kourtney Wunschel
Jim and Jacki Marano
Anthony Carnevale Elementary School
Mark and Wendy Miller
Chrissie DeMoranville
John and Dana Mackin
Theresa and Roger Joyal
Maria Upegui
John and Colleen McCarthy
Don and Nancy Rowell
Tracy Madsen
Adam Moore
William and Marie Therese Shaughnessy
Joe Furtado
A special, “Thank-you” to all our members and friends who help us with the day-to-day operation of DSSRI. Have a wonderful Holiday Season!
General Membership Meeting ..................................................March/April, 2011
New Family Gathering .........................................................................Spring, 2011
Fundraiser Breakfast; Dave’s Bar and Grill ................................... May/June, 2011
Buddy Walk® ................................................................................ October 2, 2011
New Parent Gathering .............................................................................. Fall, 2011
Holiday Party ............................................................................ November 27, 2011
Calendar of Events

Landing Firmly on Two FeetBy Kelle Hampton, Naples, FL
CH
ILDR
EN
On my 21st birthday, I opted out of the gift my dad traditionally gave me. It was not clothes I wanted that year. In fact,
it wasn’t even something you could touch. I wanted an experience — I wanted to sky-dive. Yes, I was terrified; but, at the same time exhilarated at the thought of what 60 seconds of breathtaking free-fall would feel like. And so, after silently gliding over Lake Okeechobee, I landed victoriously on two feet, able to say I had done it.
It is 10 years later. I am 31, no longer single and seeking thrills, but fulfi lling my desire for adventure and inspiring explorations in different plains — through motherhood, family and the proverbial dream of a home with a white picket fence.
This year, my world was rocked and that white picket fence crumbled — or so I thought. On January 22, we welcomed our second little girl and discovered she came with something extra. It was crippling in the beginning, like starting from scratch after watching the home you had built and secured with years of memories be ripped apart by tornado winds.
But, slowly, you rebuild. And you rebuild something better — more beautiful than before. When you raise the crumbled picket fence and let it stand again, you realize it may no longer be white like the other fences. The different color makes it vibrant, full of life and wonder and things you never knew.
I am new to this world of colorful fences. I am still learning and at times I’m a bit afraid. But I am smitten with love for my child and for the things she is teaching me. I am excited for the family we are becoming. In six months I have felt my soul take new shape, and I am beginning to see the world differently — in a uniquely beautiful way.
When my Nella was just four months old, I realized the National Down Syndrome Congress Convention would be here in my home state of Florida, just a few hours away. I didn’t know if I was ready.
Acceptance is a journey. I felt I had landed in such a place of peace and love that I was truly beginning to accept our new world; but, I was nervous about this next step. As I contemplated taking it, I began feeling the same emotional stirrings I felt 10 years ago just before I boarded a small plane that soared into the clouds. Then, when the door opened and I braced myself in its frame, I jumped and felt my heart catch in my throat as I stretched out my arms to feel the fall, the thrill, and the freedom.
So, I knew I needed to go. I began an inner dialogue of “Brace Yourself; Push Yourself; Brace Yourself; Push Yourself” and prepared for whatever the universe had in store for the upcoming Orlando weekend. I braced myself for sadness — for a second wave of accepting new things I might witness, for new understanding that would come from more education and exposure to experiences we will encounter on this journey. Instead, I was met with a fl ood of emotions I hadn’t expected...love, peace, gratitude.
It felt warm and inviting to walk into the Coronado Springs Resort. As I held little Nella in the crook of my arm, I witnessed other families on this journey with me. I felt a bit like I was gliding again — parachute launched, free-fall completed, and left with nothing more than the job of enjoying the ride.
From up high, you see things you have never noticed before. You gain a new perspective.
3
I couldn’t help but smile as I met other children like Nella and felt my
growing excitement for who she will become.
— (continued next page)

CH
ILD
REN
4
Landing Firmly on Two Feet— (continued)
And that s exactly what my journey to the NDSC Convention did for me. My fears melted, and in their place was gratitude to be part of a new world of incredible people who are teaching me that life is rich and beautiful and that there are so many ways to enjoy it.
We are more alike than different, and at the core of every one of us exists a passion for sucking the marrow out of life and loving each other. I couldn’t help but smile as I met other children like Nella and felt my growing excitement for who she will become. I was amazed at the trail others are blazing for my girl and am grateful to all who make a difference
in the lives of the beautiful individuals with a little something extra.
At the end of the weekend, I fi rmly landed on two feet, victorious. Ten years ago, my parachute had barely defl ated and my feet had been on solid ground but for a few seconds when I smiled and declared, “I want to do it again.” Today, after the amazing experience I had at the NDSC Convention, I can say — “I can’t wait to do it again.”
Being a grandparent of a child with Down syndrome can be a great joy. You have the opportunity to see your own child become
a nurturing parent and feel a swell of pride as they experience parenthood for themselves.
You have years of parenting knowledge to draw upon if you are needed (that phone call asking if you think the baby is ready to start solid food or should he stay on formula, etc). And then, the most important part, the beautiful child! Whether they are fussy or funny (and let’s face it they are all at one time or another) they bring joy to your life. You can bring them the loving relationship they need to thrive.
The US Census Bureau estimates that at least 3 million children are left in the care of their grandparents at some point each week. For the parents and grandparents of a child with Down syndrome, this relationship can be especially important. You can provide both emotional and practical support for parents as well as providing your grandchildren with an increased range of close relationships.
Having grandparents on hand to share in the care of children is usually a great help to families. Some children with Down syndrome
have special health concerns and can’t be cared for by just any babysitter.
They may require a particular healthcare routine and also need someone who knows them well, someone who can tell when “something just isn’t right” so that a doctor’s care may be sought.
Grandparents can fi ll this role so well and give welcome respite to the parents of a child with special needs. Even when the extended family members are not geographically close, they can be an important source of emotional support.
All children (and their parents) need good role models. This is another area where grandparents can excel, offering a guide for how to manage in the world, how to handle emotions in a healthy way, how to fi ght for what is right and how to remain positive. You’ve been through it all and made it this far. This is the strength and the wisdom of a grandparent.
Reprinted from the Central California Down Syndrome Association Newsletter
The Special Role of a GrandparentBy Kelle Hampton, Naples, FL
Reprinted from Down Syndrome News, the newsletter of the National Down Syndrome Congress, 2010 Convention Issue

Food Rewards: Help or Hindrance?C
HILD
REN
I overheard Melissa talking to a friend the other day. She was explaining her day. “In social skills group, I get a tiny bag of skittles
like the ones you get on Halloween. Mrs. R gives us a chocolate kiss after music. Miss Sally gives me jelly bellies after I do my writing exercises. In Mr. White’s class I have a chart for when I listen carefully. When I get 10 stickers, I get to pick a piece of candy from the jar.”
Use of food as a reward system in schools is not new. It is an easy and universally understood token for students of all ages and abilities. It’s common for a class of students to work toward a pizza party or other food-related event.
However, for students with Down syndrome and related disabilities, the use of food rewards can become so prevalent in teaching methodology it gets in the way of lunch! For Melissa, the candy appears to be the most exciting part of the day.
When working in isolation, these rewards seem harmless. However, the totality of the candy offered throughout the day is a very real problem. Not only do they provide too may empty calories in a day, but the process, the habit, of earning food can wreak havoc later in life.
Think about the behavioral lesson. What is this student learning? She is learning that if she complies with the rules, she gets candy. She is learning that food is an expected part of a good day at work. For some students, this becomes a well established groove into adulthood that is diffi cult to break. For others, good work triggers the desire to eat. It’s diffi cult to fi nd a good reason to continue to offer food as any sort of regular reward.
What to do?
First, use the accommodations and modifi cations section of your child or student’s IEP. An appropriate accommodation for this student is “No food rewards.” This will serve as a reminder to all team members. However, whenever a technique is taken away, it must have an equally effective one. This is where the team work comes in to play. I encourage parents and teachers to create a list of the things that motivate each student.
For many, the best reward is a social connection: a high fi ve, a statement of praise, time with friends doing an infrequent, favored activity, and so on. A visual tool for this would be a reward chart with stickers, building up to special time with friends.
One young lady I worked with was more excited about earning clips and bows for her hair than anything else. We all knew when it was an especially good day when you could barely see her hair for the clips and bows.
When working with middle school and high school students, sit down with them to create the reward list. Ask them what it is they would like to do. Involving students in classroom contracts makes them more meaningful.
Of course there are times when a classroom party is the most appropriate activity for students! Focus the party on activities and what they did to earn the party more than the pizza or ice cream. Regardless, food is an integral part of life. Our job, as parents and educators, is to use it wisely.
Written by: Joan Medlen M. Ed, RD 2010 ©Phronesis Publishing, LLC
Reprinted from Connections, the newsletter of Down Syndrome Guild of Greater Kansas City, Volume 17 Issue 5 September/October 2010.
5
Check out Golf World Charities Issue, Nov. 1, 2010.Our friend, Nathan, is featured on the cover with
Brad and Dory Faxon. Great photo Nathan!

CH
ILD
REN
6
Tongue Protrusion in Individuals with Down Syndrome
Question: My child has problems keeping her mouth closed. Her tongue protrudes out when she tries to swallow and drink from a cup. What can I do to help her?
Answer: Most children typically produce many front sounds early in development. For instance, the lips are needed to produce the /m, n, p, b/ sounds. The lips and teeth work together to pro duce the /f, v/ sounds, and the tongue tip is used to produce the /t, d, I, n, s, z, th/ sounds.
It is important for speech development that early treatment be implemented to help the child keep the tongue back, for using the tongue to scrape and touch various areas of the oral cavity, and to maintain good lip closure. However, before treatment is attempted, the fi rst thing is to consider the oral structure.
The physical structure of the oral cavity may in part be affecting the protruding tone and open mouth postures. That is, it is known that large tonsils and adenoids can cause a child to carry an open mouth posture in order for the child to obtain enough air during breathing. Furthermore, it is also known that the tongue size among most children with Down syndrome is too large for their oral cavity and, therefore, they protrude the tongue again in order to breathe. Another side effect of the tongue protruding is drooling. Unfortunately, both the tongue resting against the lower lip and the drooling has the effect of desensitizing the lip which, in turn, affects lip movement. Most children with Down syndrome have low muscle tone (i.e., hypotonicity) and show weakness in the lip muscles. Please check with your child’s pediatrician regarding these concerns.
All of these oral-motor problems can have a detrimental effect on the lip and tongue tip sounds development. We
encourage early oral motor and speech stimulation activities to assist in the production of sounds. Here are some of the techniques that you can try at home:
• Blowing through whistles- This helps in lip rounding and practice in release of air for sounds like the /h/ and the /wh/.
• Licking lollipops- place the lollipop in front of the mouth and have the child lick the lollipop by moving the tongue tip up and down across the lollipop. Also, after the lollipop is wet, you can move it across the upper and lower lips so the child can scrape along with her tongue.
• Touching under the chin, gently push-ing up, and reminding the child to close her mouth- This may be an activity that the parents, teachers, grandparents, therapists will all need to follow in order to help remind the child to close her mouth.
• Closing the lips around a spoon full of food- Instead of scraping the spoon across the teeth, the parent should have the child close her lips around the spoon and clean the food off with her lips.
• Scraping Lip Balm- Use different flavored lip balm sticks and rub them across the upper and lower lips so she can scrape along with her tongue.
• Strengthen the lips- Place your thumb inside the upper lip and your pointing finger outside the lip, then roll the thumb to open and close the upper lip; or close together the same two fingers under the nose and slide them down across the middle of the upper lip, pressing slightly down, and then open your fingers as so to spread the upper lip apart. These movements are to assist in strengthening the muscle tone.
• Blowing Bubbles- Practice blowing bubbles, this aids in lip rounding and air control.
• Sucking and blowing through straws- Again this helps in the lip rounding and air control.
— (continued next page)
Tongue Protrusion in Individuals with Down Syndrome— (continued)
CH
ILDR
EN
• Using sports bands on the wrists- This allows the child to wipe the drool from their mouth and helps to keep the lips dry.
• Practice chewing with the Baby Safe Feeder- This product is available in infant stores. A mesh bag lets children practice their chewing skills without the risk of choking. All you do is drop a mesh bag into a retainer ring, place food in the bag and screw it tight. The child can then practice chewing.
• Viewing lip and tongue exercise in a mirror- Sit next to your child directly in front of a mirror, produce lip and tongue movements with the appropriate sounds so your child can see and hear the production, encourage your child to imitate and make similar sounds.
7
Hypothyroidism is when the thyroid gland is underactive. The thyroid gland is found in the neck and secretes thyroid hormone.
Once secreted from the thyroid gland, thyroid hormone gets into the blood and spreads to your entire body.
Thyroid hormone regulates the body’s metabolism. In hypothyroidism, normal body processes will slow down, including growth and brain devel-opment (in newborns and infants). Some common signs and symptoms of hypothyroidism in newborns and infants include:
• enlarged tongue
• hoarse cry
• cold extremities with mottled skin
• enlarged “soft spot” on head
• poor feeding
• low muscle tone (floppy)
• prolonged jaundice (yellowing of the skin)
• belly button hernia
• constipation
• low body temperature
• Goiter
It is important to point out that most newborn babies with a underactive thyroid will not have any of the above fi ndings. Older children and teens may also experience:
• poor growth
• weight gain
• decreased energy, increased sleep
• mental retardation if untreated
• thinning or brittle hair
• menstrual problems
As you may have noticed, Down syndrome and hypothyroidism have many symptoms in common. This can make it hard for the physician to determine whether the child’s symptoms are due to Down syndrome or hypothyroidism.
Hypothyroidism is present in about 10% of children with Down syndrome. Children with Down syndrome can have either congenital or acquired hypothyroidism. In congenital hypothyroidism, the child is born without full function of the thyroid gland, most commonly because the thyroid gland did not form correctly.
Hypothyroidism and Down Syndrome
Article Written By: Thomas L. Layton, Ph.D.President/Owner, Talk and Total Communication Board Member, Triangle Down Syndrome Network
Dr. Layton has more than 35 years of expertise in speech pathology, and has done extensive work with individuals with Down syndrome.
Reprinted from Connections, the newsletter of Down Syndrome Guild of Greater Kansas City, Volume 17 Issue 5 September/October 2010.
— (continued next page)
CH
ILD
REN
8
Hypothyroidism and Down Syndrome— (continued)
Almost all infants with congenital hypothyroidism are detected by newborn screening. Thyroid hormone is very important for brain development in first 2-3 years of life and congenitalhypothyroidism should be treated as soon as it is diagnosed. Untreated congenital hypothyroidism can result in mental retardation. In fact, hypothy-roidism is the most common cause of preventable mental retardation worldwide.
In acquired hypothyroidism, the child loses full function of his/her thyroid over time. The acquired form of hypothyroidism is usually the result of an attack on the thyroid gland by the body’s immune system, which is referred to as autoimmune thyroiditis or Hashimoto thyroiditis. This immune attack can destroy or decrease the function of the cells in the thyroid gland that make thyroid hormone. Occasionally this can result in enlargement of the thyroid gland which is also called a goiter.
Because hypothyroidism is easily treated and can improve certain defi ciencies in children with Down syndrome, it is important for children with Down syndrome to be screened for hypothyroidism on a regular basis. Screening for hypothyroidism is done with a simple blood test. Current guidelines, recommend that kids with
Down syndrome be tested for hypothyroidism at birth, 6 months, 1 year, and every year after for the rest of their lives.
If a child is diagnosed with hypothyroidism, they are simply given a pill form of thyroid hormone (often goes by the name of levothyroxine or Synthroid). This medication is given once per day and the pill may be crushed and mixed with liquid or food for infants and toddlers. This medication alleviates the symptoms of hypothyroidism in Down syndrome but may not entirely correct all of the symptoms because of the overlap between the symptoms of Down syndrome and hypothyroidism. Treating a child with Down syndrome without proven hypothyroidism has not shown any benefi t.
Blood tests need to be repeated periodically to determine the correct dose of the thyroid medication. Infants and toddlers may need the blood tests every 2-3 months, whereas older children may have it checked every 6 months. Many of the children with Down syndrome and hypothyroidism are followed by a pediatric endocrinologist (hormone specialist).
It is important to be aware that hypothyroidism can occur in children with Down syndrome. The simple treatment can help increase growth, improve development, increase muscle tone, and overall improve the lives of the children that have been diagnosed with both Down syndrome and hypothyroidism. So if you have a child or know of a child with Down syndrome, please remember to make sure they are getting screened for hypothyroidism because it could greatly improve their quality of life.
Article written by: Joseph Cernich, MD Children’s Mercy Endocrinologist
Reprinted from Connections, the newsletter of Down Syndrome Guild of Greater Kansas City, Volume 17 Issue 5 September/October 2010.
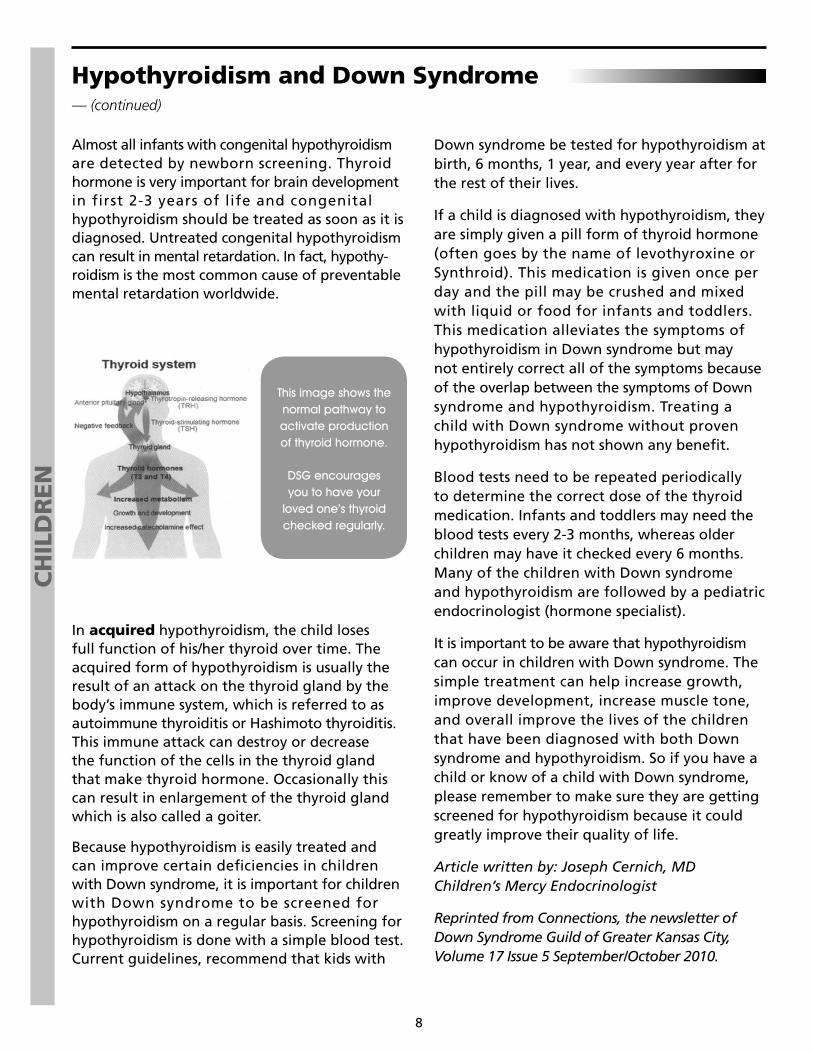
This image shows the normal pathway to activate production of thyroid hormone.
DSG encourages you to have your
loved one’s thyroid checked regularly.
SC
HO
OL A
GE
The phone rings. It’s 3 p. m. and school is calling. Andrew had a bad day again. On the bus line, he cut in front of Mitchell and pushed him. It’s not the fi rst time and the teacher is considering whether a Functional Behavior Analysis (FBA) is needed.
Talk about social skills can mean many things. Diffi culty with social skills is often labeled a behavior problem. This article
focuses on social communication skills, i.e. language in daily use and social interactions, also known as pragmatics. You know that Andrew has been eager to sit near Mitchell on the bus ever since Mitchell brought a toy train to school. Andrew loves trains. How can you handle this when Andrew gets home? Maybe you can talk about lining up or about how he loves trains. Consider modeling and role playing how to ask whether you can sit next to someone on the bus.
Research on pragmatics in typically developing children has been plentiful, but very few studies examine pragmatics in children with Down syndrome (DS). Existing studies generally compare children with DS to children with autism or Fragile X syndrome, and conclude that children with DS score higher in social interactional language than children with autism or Fragile X. As a result, social skills are often seen as a strength for children with DS and therefore are not addressed in therapy. The research confuses sociability with social skills. Children with DS want to interact and communicate with others; they are sociable. But, they often need help learning how to use language in certain social situations. Children with sensory processing diffi culties who don’t like to touch or be touched, or have diffi culty with loud noises and large groups, may not appear sociable. Many children with DS have difficulty initiating, and aren’t sure how to appropriately approach another child.
Social communication such as greetings and nonverbal communication (smiling, pointing) are usually the easiest pragmatics skills for children with DS. The most difficult are advanced conversational skills, such as staying on topic, handling communication breakdowns
and repairs, making requests to other children, saying the “right” thing, and telling someone what happened. This article focuses on the hierarchy of social language skills, and how families can help develop these skills at home and in the community.
The long-term goal for all children with DS is to use appropriate social interactive communication skills. These skills will be developed and practiced in school, at home, in community activities, in recreational activities, in friendships and relationships, and in job settings. A lot of practice is necessary and social interactive communication skills continue developing throughout life.
Social language skills include nonverbal commu-nication, language skills and some speech skills.
NONVERBAL COMMUNICATION SKILLS:
• Kinesics: the use of gestures;
• Proxemics: use of appropriate distance and space when interacting with others;
• Intent: the goal of the communication;
• Eye contact: looking directly at the com-munication partner (also known as reciprocal gaze);
• Facial expression: the emotional meaning of facial movements, such as smiling or frowning;
LANGUAGE SKILLS:
• Requests: asking for something through the communication;
• Conversational skills;• Conversational manners: turn taking and
interrupting;
• Active listening: listening and reacting;
• Stylistic variation: ability to adapt speech and language to different conversational partners and audiences, e.g. formal or casual;
• Diplomacy and appropriate comments;• Presuppositions: assumptions a person
makes that may influence a conversation;
9
Social Communications SkillsBy Libby Kumin, Ph.D., CCC-SLP, Loyola University Maryland
— (continued next page)

Social Communications Skills— (continued)
SC
HO
OL
AG
E
• Topicalization: this includes introducing, staying on, shifting and ending topics;
• Clarification and repairs: asking your conversation partner for information that you don’t understand, and providing information that the listener needs.
SPEECH SKILLS:
• Using vocal volume appropriate to the situation
• Using an appropriate tone of voice
Typically developing children learn to use language socially by observing adults and older children, practice and trial and error. Children with DS also learn skills through observation, but they often need to be made aware of the skills and practice learning to use them.
Inclusion in school and in family and community activities promotes social skill development.
HELPING CHILDREN LEARN SOCIAL SKILLS
• Observe your child and identify the skill that is difficult for him or consult with the speech language pathologist (SLP) and ask for help identifying skills;
• Bring the skill into your child’s awareness;
• Model the appropriate skills;
• Role play using the skills;
• Practice using skills in real situations; and,
• Reinforce use of the skills.
Here is an example:
Identify: Phillip has diffi culty staying on topic. One minute he talks about a report he needs to do about insects and the next he talks about Disney World, Animal Kingdom and his favorite ride.
Awareness: Mom says. “Phillip, tell me about your report. We’re not talking about Disney World right now”
Model: Use visual aids to discuss what’s on topic and what is not. Make two columns — one for information about insects and the other listing what must be included in the report.
Role play: In this case, we role play conversa-tional skills. Make a list of on-topic questions for Phillip to ask. Begin talking about the report topic (insects), and Phillip asks questions. Then, reverse roles; he tells you about the report and you ask questions.
Practice: When grandpa comes over, ask Phillip to tell him about the insect report.
Reinforce: Both you and grandpa can praise Phillip by telling him what a good job he did explaining the report. Let him know that you want to hear about the next report he needs to do for school, and that you want to see the report on insects when he has fi nished it.
SOME ACTIVITIES TO USE
• Use games on conversational manners or on-topic/off-topic. You can purchase social skills games, or create game boards using manila folders and small plastic figures or coins for markers.
• Play an imitation game like Simon Says but use questions or social comments.
• Watch live or videotaped models of a successful social situation. Watching videos and TV shows can form the basis for discussions about social situations that involve communi-cation and how to handle them.
• Use books or personalized stories to set the scenario for real-life situations that can be analyzed and practiced in therapy.
PRACTICE, PRACTICE AND MORE PRACTICE!
Practice can be skill based — that is, focused on learning to use specifi c social skills such as appropriate greetings or conversational skills. Children might also observe their family or watch videos of themselves or others successfully interacting with others to learn the right way to act.
10
Social Communications Skills— (continued)
SC
HO
OL A
GE
Here are some examples:
Sam doesn’t usually greet people in school. The SLP has worked with Sam to teach him to say “hi.” Once he has practiced, they spend an entire speech session walking the halls of the school and saying hi to everyone they meet, including the principal and offi ce staff, the school nurse, cafeteria personnel and other children. The SLP sends a quick email home to Sam’s parents. When Sam arrives home, his mom has lined up all of his beanie babies and stuffed animals. Sam says “hi” to each one. Sam says “hi” to his sister when she comes home from school, he says “hi” and she responds “hi” with a high fi ve. Sam keeps practicing. Soon, it feels natural to say “hi”.
In preschool, Maren and her classmates practice shaking hands. This is very challenging for tactile-defensive Maren. One Sunday, at church, Maren decides to shake hands...with all of the people who passed by the pew where she was standing on their way to communion. That solidifi ed the skill acquisition — lots of practice in a community setting.
Elizabeth knows and understands a lot of language. However, she often does not know what to say in a specifi c situation, freezes up and doesn’t say anything because she is concerned that she will say the wrong thing. When her family sees Elizabeth freeze up, they have begun to spoon feed her language so that she knows exactly what to say and doesn’t need to worry about whether or not it is the correct thing (she trusts her family members not to tell her the wrong thing to say!). Elizabeth relaxes and has begun to start to carry on herself for a few turns after getting over the initial hurdle.
One of the ways Stephanie learns best is by observation. When she began to use the phone, it was clear that she had been paying attention to how her mom and younger sister talk on the phone. Stephanie answers and ends phone calls in the same way, and uses the same words, tone and infl ection. Telephone conversations lend themselves to role playing practice, and learning scripts help children and adolescents feel more comfortable.
Practice may also be strategy based. Using this approach, children are taught to fi rst identify different social situations, then discuss several
different solutions and the consequences of each choice, and finally to select the best solution for the situation. Social StoriesTM are an example of strategy based practice. This approach is better for older children and adolescents since it requires more language and the ability to analyze situations. Carol Gray fi rst created Social StoriesTM as a tool for teaching social skills to children with autism. However, they can be helpful for any child who has trouble understanding social cues, knowing how to act in a given situation, or seeing other people’s reactions and perspectives. After the discussion phase, use role play to practice the skills. Specifi c planned events such as family get togethers, school dances, class oral reports, and preparing for interviews lend themselves well to role playing practice.
You can use Social StoriesTM written specifi cally for a particular child, or prepackaged versions that address common issues such as waiting, taking turns, or entering a conversation. Use Social StoriesTM proactively (before a child has problems in a situation) or reactively (to help him deal with a known problematic situation). Typically, Social StoriesTM are written on paper, with or without illustrations, but there are also videotaped versions of Social StoriesTM, including Carol Gray’s own StorymoviesTM (See online resources at ndsccenterorg).
Reading or watching Social StoriesTM with a child can lead to discussions about:
• Typical situations the child will encounter;
• What the important social cues are;
• How you can tell what other people are thinking or feeling;
• The sequence of events that might occur;
• Appropriate actions to take;
• Appropriate reactions to other people.
The goal of a Social StoryTM is to examine a specifi c situation that a child has (or might have) diffi culty with. For example, Chris may hit other children when he wants a turn on the swings. A Social StoryTM for Chris might go like this:
11— (continued next page)
Social Communications Skills— (continued)
I can do many things with my hands. I can wave, give a high-fi ve, and throw a ball. But I should not use my hands for hitting. When I am on the playground, I am excited and I want to go on the swings and the slide. But if someone is already on the equipment, I have to wait. I can say, “Till me when you fi nish” or “My turn next.” Then I need to wait. Soon, it will be my turn to swing.
Sandbox Learning has a program called Success Stories in which stories and illustrations can be customized for a specifi c child(www.sandbox-learning.com).
Video modeling is another strategy most often used with children on the autism spectrum, but can also benefi t other children who are visual learners, including many children with DS.
Video modeling involves making a video/DVD (or purchasing a commercially available video/DVD) showing appropriate behavior and then having the child watch the video. Video self-monitoring can also be used with older children. The child herself is fi lmed performing the skill or behavior, and then the video is edited so that it only shows the child doing the skill correctly.
Why is video modeling more effective than live modeling or role playing? Videos enable the child to focus on what is essential for him to learn. By zooming in on certain activities, video cuts down on irrelevant environmental features, such as noise and moving people. In the natural
environment, these factors often distract a child. Recent research has shown that video modeling can result in improved social communication skills and behavior. The key is to choose a skill for the child to learn that is not too far above his current abilities. If your child can ask for help in one situation, but not all the time, you might fi lm him asking for help in a new situation. Then allow the child to watch the video/DVD whenever he wants, without lecturing him that this is what he should be doing.
We use social communication skills every day. Knowing how to use social communication skills appropriately increases quality of life for children and adults with DS, with improved success in developing relationships, fi nding and keeping employment and reducing isolation. Opportunities arise every day to teach these important skills both at home and other settings, such as school. By observing what skills are being used successfully and what skills need to be developed, you can help your child learn to socially navigate her world.
Editor’s note: A list of resources for social communication is available online at ndsccenter.org under the Speech and Language Informational Resources tab.
Reprinted from Down Syndrome News, the newsletter of the National Down Syndrome Congress, Vol. 33 2010 #6
12
SC
HO
OL
AG
E
Children with DS want to interact and communicate with others; they are sociable.
But, they often need help learning how to use language in certain social situations.
“We all have ability.The difference is how we use it.”
Stevie Wonder

SC
HO
OL A
GE
13
CREATING HIGH INTEREST READING MATERIAL: The Boy and His DogBy Jennifer Ancelin, M.Ed., Jacksonville, FL
The Boy and His Dog is the result of a delightful collaboration between me and my son, Arik, a fi rst grade student in a general education
“inclusion” class. As a student in a master’s program in Education, I learned that using high interest reading material increases student motivation to read by addressing three key factors: personal interests, book characteristics and choice. As Arik’s mom, I got to see that theory in action as we spent time together creating his personal publication.
Creating high interest reading material is an activity that students of all ages can enjoy because, by its nature, the subject matter is easily adapted in age appropriate and highly personal ways. Arik and I began by talking about subjects, events and activities he fi nds appealing and engaging. I continue to be amazed at what surprising and brilliant ideas that all children —including Arik— come up with when I’m open to their suggestions.
We carefully considered each idea to fi nd one that we could capture in photographs that would support the written story. Arik suggested several topics, including planting tomatoes, skateboarding, pizza and his dog, Agnes Marie.
Arik’s fi rst choice was skateboarding. At the moment, though, Arik needs considerable physical assistance to enjoy skateboarding and perform his favorite tricks. We decided that subject did not lend itself to pictures that would clearly feature Arik as the star of his own adventure. However, Arik and Agnes Marie do numerous fun things together they have invented on their own that would make for entertaining pictures of the exciting plot. That seemed like the best choice and we began using a story board (see Figure 1) to begin conceptually and visually laying out the book. We chose to take some preliminary photos during this stage of the process, but hand drawn pictures or clip art would have worked well, too.
After planning what the pictures would look like, it was time to fi gure out what the text would say. Arik, like many students with DS, fi nds handwriting is a challenging task. So, to keep the process lively, fun and focused on creation, Arik wrote some
of the words and acted out other ideas, which I verbalized to his satisfaction. Arik told me some of his exciting plot lines, which I then wrote down. I fi lled in missing text, soliciting his approval all the while. These techniques also can be used with students who have not yet begun to write. Depending on your student’s age and reading level, the text could include anything from one word to several paragraphs for each picture.
In her book, Teaching Math to People with Down Syndrome and Other Hands On Learners (Woodbine House, 2008), Dr. Deanna Horstmeierrecommends using a “success step” when teaching a student with DS a major new concept. So, the initial pages of The Boy and His Dog were to include mostly words that Arik already knew or were concrete and associated with something of high interest to keep him motivated as he worked to read the whole book. This creates a “can-do” attitude that supports the student through the entire process.
After we were done writing the story, it was time to shoot the photographs we’d planned on the storyboard. It was fun for the whole family, because Arik’s father and sisters joined in this part of the process. We fi rst discussed the intended meaning of the picture and rehearsed the poses necessary to get the shot. Arik loves acting, so we kept this very light and framed it as a grand performance where the “audience” enthusiastically responded every time we completed a frame.
Because we wanted to get just the right photos, we took our time and used a digital camera to shoot many, many takes of each shot. It actually took us four separate sessions to complete all the necessary photos and we quickly learned how to use dog treats to help Agnes Marie enthusiastically perform on cue.
With the text and photos complete, we began compiling the book. Because we have Mac-based technology in our home, it worked well for us to use Apple’s iPhoto software. It provides a variety of easy-to-use templates that gave excellent visuals from which Arik could choose and have a

The Boy and His Dog— (continued)
SC
HO
OL
AG
E
good idea of what his fi nished book would look like. (Several companies provide tools for making photo-books, including Shutterfl y, Kodak, and Winkfl ash, to name a few)
After sending it off to be published, we waited several weeks for our book to be delivered. In the meantime, we created fl ashcards of the more abstract and challenging words from The Boy and His Dog to practice and learn. Some of these words were “neighbor,” “healthy,” and “music.” When the book arrived, a well-prepared Arik was confi dent and eager. The moment the book arrived, he ripped open the package, plopped down in the foyer and began to read it!
Arik initially enjoyed The Boy and His Dog without any requests from the family that he speak about it or read aloud. Independently, Arik read silently and aloud, regarding some pages at great length and fl ipping quickly through others. He made spirited spontaneous comments about the book’s plot and characters. If asked, Arik was glad to point to words on a page and point to specifi c
parts of a photo as related to a comprehension question. After two days, he was clearly comfortable and enjoying his book. I asked Arik if he would like to read it to me. He said “Yep,” sat on my lap, placed his pointer fi nger on the fi rst word of the fi rst page and read, “This is the boy. His name is Arik.”
It took Arik about three days to be able to read The Boy and His Dog in its entirety without assistance. He remained motivated, determined and interested and his reward was an invitation to read his book to his entire fi rst grade class at school during story time. This event was hugely satisfying, resulting in momentary “rock-star” status amongst his peers — which he recounts happily every time he picks up and reads the book.
Editor’s note: Ancelin is an education specialist at The Down Syndrome Center, Hope Haven Children’s Clinic in Jacksonville, FL. Contact her at [email protected]
14
Shot 1: Shot 2: Shot 3:Caption: Caption: Caption:
Shot 4: Shot 5: Shot 6:Caption: Caption: Caption:
Storyboard ArikClient Title
Spot Job #
“The Boy and His Dog”
— (continued next page)
The Impact of Health Care Reform for Individuals with DisabilitiesBy Susan Goodman, Esq., NDSC Governmental Affairs Director A
LL AG
ES
Editor’s note: The room was packed at Good-man’s workshop at the NDSC convention in Orlando with people asking questions about how the recently passed federal health care legislation will affect them. This information is provided for Down Syndrome News readers who may have similar questions.
The Patient Protection and Affordable Care Act (H.R. 3590, Public Law 111-148) was signed into law on March 23, 2010. Imple-
mentation of this law will be a lengthy pro-cess. Some provisions are effective immediately while others do not take effect until 2014.
Two important provisions of the insurance market reforms go into effect immediately. Children with pre-existing conditions (such as Down syndrome), cannot be denied coverage due to the presence of preexisting conditions. Lifetime caps, which limit coverage to fall under a certain dollar amount and may not provide adequate coverage for people with complex medical needs, are also prohibited.
In 2014, when many permanent provisions go into effect, states must have health insurance exchanges (or alternatives) through which individuals and some employers may purchase health insurance. In addition, most people will be required to have health insurance unless
they are eligible for health care through government programs such as Medicare, Medicaid, the Department of Veterans Affairs or military service. There will be refundable tax credits for some people based on income and some small businesses that provide health insurance to their employees will receive tax credits.
Below is a summary of some of the provisions that have an impact on individuals with disabilities and when they take effect.
INSURANCE MARKET REFORMS
• No Discrimination Based on Pre-Existing Conditions
As of 2014, the law prohibits insurance companies from refusing to insure an individual because of a pre-existing condition. Therefore, an individual could not be refused because of a developmental disability or any condition associated with it, such as a heart defect.
Insurers also will no longer be allowed to charge higher premiums based on a disabling condition, withdraw coverage after someone is injured or acquires a new condition, or impose annual caps on benefi ts. Most of these provisions took effect for children on September 23, 2010.
15
• Use a single font sized at least 36 points min-imum. (Doman & Doman, How to Teach Your Baby to Read: The Gentle Revolution)
• Place the words on one page and just one related picture on the other. If transfer-ring hand written text to computer gener-ated text challenges your student’s com-prehension, use a font such as Chalkboard, which keeps letter shape and the letters a, g and q more consistent with hand writing.
• If words are on the left page, keep them on the left page throughout the book. This helps your student learn that the words relate to or describe the picture, ultimately leading to developing an effective word decoding strategy. (Sanacore, 2010, Connecting Rimes to Meaningful Contexts).
Reprinted from Down Syndrome News, the newsletter of the National Down Syndrome Congress, Vol. 33 2010 #6
Literacy Tips
— (continued next page)
The Boy and His Dog
Dear Affi liates-
The Centers for Disease Control and Prevention (CDC) and the National Birth Defects Prevention Network have published a study that updates national statistics regarding the prevalence of Down syndrome in the U.S.
The study indicates that there are about 6,000 diagnoses of Down syndrome each year in the United States. One in every 691 babies is born with Down syndrome. This is an increase from the previously reported statistic of 1 in every 733.
Based on the new study, the National Down Syndrome Society (NDSS) will cite the new prevalence estimates on its website and other materials.
Please feel free to share this information with your members in any way you see fi t.
Best, NDSS
The Impact of Health Care Reform for Individuals with Disabilities— (continued)
ALL
AG
ES
• Lifetime and Annual Benefits Caps
Lifetime caps on benefi ts are prohibitedimmediately. As of 2014, both lifetime and annual caps on benefi ts will be prohibited.
• Temporary High-Risk Pools
Between now and 2014, many people with pre-existing conditions are eligible to purchase coverage through high risk pools.
HOME & COMMUNITY-BASEDSERVICES• Community Living Assistance
Services and Supports — CLASS
In 2011, the CLASS provisions, which establish a national, voluntary insurance program, will take effect. In this program, people with functional limitations can receive benefi ts of (not less than $50 average per day) to pay for services and supports they choose to help them with activities of daily living. To qualify, people will have had to pay premiums, by means of a voluntary payroll deduction plan, for at least fi ve years. Additionally, they need to have worked for at least three years and earned at least one quarter of credit towards Social Security.
• Community First Choice Option
This option allows states to require provision of home and community-based services and supports for individuals with disabilities with incomes up to 150 percent of the Federal Poverty Level. States will receive an additional six percent in the federal government’s share of Medicaid costs to encourage choosing this option.
16
• Essential Benefits
For some health insurance plans —including those of-fered in the exchanges — individual and small group plans, the law mandates coverage of at least the fol-lowing essential benefi ts: ambulatory patient services, emergency services, hospitalization, maternity and new-born care, mental health and substance use disorder services (including behavioral health treatment), prescription drugs, rehabilitative and habilitative services and devices, laboratory services, prevention and wellness services and chronic disease management, and pediatric services including oral and vision care.
The Department of Health and Human Services (HHS) has the authority to further defi ne essential benefi ts consistent with these required elements. HHS is expect-ed to do so.
SUBSTANTIAL EXPANSION OF PEOPLE ELIGIBLE FOR MEDICAIDAs of 2014, health care reform expands Medicaid to cover non-elderly, childless adults for the fi rst time and adults with incomes up to 133 percent of the Fed-eral Poverty Level. It also expands Medicaid to cover children in families with incomes up to 133 percent of the Federal Poverty level, and it extends Early, Pe-riodic, Screening, Diagnosis and Treatment (EPSDT) mandates to all children on Medicaid including those in managed care. EPSDT services address developmen-tal disabilities and delays.
If you have questions or comments, please email me at [email protected].
Reprinted from Down Syndrome News, the newsletter of the National Down Syndrome Congress, Vol. 33 2010 #6
ALL A
GES
17
Our Family’s Journey with Celiac DiseaseAnne Reinertson
Celiac Disease is an inherited autoimmune disease that affects the digestive process of the small intestine, which is connected
to the stomach. When a person who has Celiac Disease consumes gluten—a protein found in wheat, rye and barely—the individual’s immune system responds by attacking the small intestine, therefore inhibiting the absorption of nutrients by the body. 97% of people with Celiac Disease have not been diagnosed.
I fi rst learned about Celiac Disease from an article I read in NADS News. Our daughter was 2 at the time, and she had not gained a pound or had much growth in height in almost a year. I knew something wasn’t right. I discussed Celiac with her pediatrician, then with her endocrinologist. We did a blood test, and sure enough, her levels were off the charts! We then did a biopsy of her small intestine, and there was signifi cant damage. Regan was malnourished due to her little body not being able to absorb the nutrients from the food she was eating. I was relieved to fi nd out that she indeed had Celiac so she could begin to heal and grow . . . but was terrifi ed of the thought that my daughter could NEVER eat another goldfi sh cracker! Looking back, those fears are long gone. There are so many DELICIOUS products on the market today that you can find at your local stores. We even go to our local Home Run Inn and bring them a gluten free pizza crust for our pizza! Our entire family eats gluten free. Our
youngest daughter, Lauren, even likes the gluten free cookies best!
Although Celiac is higher in the Down syndrome community, it is still an inherited disease. My husband and I were tested, and sure enough, my husband had Celiac just like Regan. He never had any symptoms (silent Celiac), but his body was becoming damaged just the same. If left untreated, Celiac can lead to other serious illnesses, including cancer. It is also important that our daughter Lauren gets regular screenings throughout her life to insure that she is still clear of the disease.
When I talk to people about Celiac, they get really nervous about changing their diet. The Gluten Free Grocery in Westchester is a great resource for information, and they have LOTS of great gluten free brands. That is one of the fi rst places we started. The owner has Celiac, so she is very familiar with the products. Having Celiac Disease in my family is now just a way of life. It isn’t as hard as you would think. You just need to know and use your resources to become familiar with the great products that are out there. There are also many restaurants that cater to the gluten free commu-nity. McDonald’s French fries are even gluten free. Eating gluten free is not as bad as you may think! There is LIFE after Celiac disease.
Reprinted from NADS News, the newsletter of the National Association for Down Syndrome, September, 2010
Celiac Disease ResourcesComing Soon: Gluten-Free KidsBy Danna Korn Woodbine House, 2010; $21.95
This updated and revised version of Danna Korn’s earlier book, Kids with Celiac Disease, will be released by Woodbine House in November. Other resources can also be found on the author’s website: http://www.celiac.com/ categories/Celiac-Disease-%26amp%3B-Kids-by-Danna-Korn.
Dr. Sindor Desai, the mother of self-advocate and accomplished musician Sujeet Desai, has founded an online support group for
Asian parents who have a child with Down
syndrome. The support group can be accessed by going to http://health.groups.yahoo.com/group/asianparentsgroup. Her son’s story can be found on his website: www.sujeet.com.
Global Connection Support Group for Asian Parents
18
Holiday Party, 2010

19
Holiday Party, 2010
Down Syndrome Society of Rhode Island
❑ Individual/Family Membership . . . . . . . . . . . . . . . . . .$25+❑ Professional . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .$30+❑ Contributor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .$50+❑ Sponsor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .$100+❑ Sustainer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .$250+❑ Benefactor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .$500+❑ President’s Club . . . . . . . . . . . . . . . . . . . . . . . . . . . .$1000+
MEMBERSHIPLEVEL
To promoting the rights, dignity and potential of all individuals with Downsyndrome through advocacy, education, public awareness and support.DEDICATED
NAME__________________________________________________________
ADDRESS_______________________________________________________
CITY______________________________STATE__________ZIP___________
PHONE ( )____________________________________
Please circle one or more of the following
Parent Family Member Educator Professional Other
MEMBERINFORMATION
Supports the publication of DSSRI NEWSEnables families and professionals to access the most up todate resources available.
YOURMEMBERSHIP
Please make check payable to the Down Syndrome Society of Rhode Island❑ I’d like to help out as a volunteer. Please call me.
NAME__________________________________________________________
ADDRESS_______________________________________________________
CITY______________________________STATE__________ZIP___________
PHONE ( )________________EMAIL____________________________
Are you receiving important updates from DSSRI? If not, please send an email to: [email protected]; in the subject line please write, “Add to email list”