drug permeation through intestine mario grassi department of chemical engineering (dicamp)...
TRANSCRIPT

DRUG PERMEATION THROUGH INTESTINE
Mario Grassi
Department of Chemical Engineering (DICAMP)UINVERSITY OF TRIESTE

BIODISPONIBILITA’
“Frazione della dose di principio attivo che diviene disponibile al sito (fisiologico) di azione dopo somministrazione”
Farmaco
INTRODUCTIONWHICH IS OUR PROBLEM?
Delivery system

TWO ASPECTS MUST BE CONSIDERED
DRUG RELEASE FROM THE DELIVERY SYSTEM
DRUG ABSORPTION AND
METABOLISM/EXCRETION

SETTING UP OUR PROBLEM
Modern Biopharmaceutics, version 6.03, G. L. Amidon, M. Bermejo, TSRL inc, produced by Judy C. Price.

Modern Biopharmaceutics, version 6.03, G. L. Amidon, M. Bermejo, TSRL inc, produced by Judy C. Price.

DOSAGEFORM
DRUGSOLUTION
SYSTEMIC CIRCULATION
(BLOOD)
GASTROINTESTINALTRACT
CELLULARMEMBRANE
DISSOLUTIONLIMITED
PERMEABILITYLIMITED
0 – CENTRAL POINT: ADME
BLOOD and DEEPER COMPARTMENT
ABSORPTION
DISTRIBUTION
METABOLISM
EXCRETION

Pharmacokinetics is the study of the time
course of drug absorption, distribution,
metabolism and excretion (ADME), and how
these ADME processes are related to the
intensity and time course of the
pharmacological (therapeutic and toxic)
effects of drugs
1 – PHARMACOKINETICS

METABOLISM - EXCRETION
LiverFirst pass metabolism
Delivery System
Pre-systemic metabolsim
Gutmetabolism
Systemic metabolsim
Heart
lung
Kidney
Excretion
Excretion
Modern Biopharmaceutics, version 6.03, G. L. Amidon, M. Bermejo, TSRL inc, produced by Judy C. Price.

F = Fa * Fg * Fh *Fl = BIOAVAILABILITY
SYSTEMIC CIRCULATION

CLEARANCE
“Is the volume of blood that must be cleared of drug per unit time in order to account for drug elimination”
Blood flow
Continuous Drug Supply
Q Drug elimination
Cd

Blood flow
FILTER
Clearing Blood flow
Cd
Q1
Qc
Q
TOTAL DRUG ELIMINATION
NO DRUG ELIMINATION
Qc= CLEARANCE

INTRA VINUS CLEARANCE: Cliv
Cliv= DOSE/AUC
C(mass/volume)
T (time)
AUC

Blood concentration
0
50
100
150
200
250
300
350
0 5 10 15 20 25
t (h)
C(n
g/m
l)
Cls = Dose/ AUC
Cls = 100 / 0.001 = 104 ml/s
ORAL CLEARANCE: Cloral

Cloral = Cliv/ (Fa*Fg*Fh* Fl)
F = bioavailability

DISTRIBUTION VOLUME: V
“Is a measure of the extent of drug distribution and is determined by the drug binding in plasma as well as tissues.”
V = Vb + Vt fb/ft
Vb = blood volume
Vt = issues volume
fb = drug unbound fraction in blood
ft = drug unbound fraction in tissues
ELIMINATION HALF TIME: T1/2
T1/2 = 0.693 V/Cls
Time required to metabolize /excrete half dose

2 – SMALL INTESTINE STRUCTURE
The small intestine is the longest section of the digestive tube and consists of three segments forming a passage from the pylorus to the large intestine
Duodenum:a short section that receives secretions from the pancreas and liver via the pancreatic and common bile ducts
Jejunum:considered to be roughly 40% of the small gut in man, but closer to 90% in animals.
empties into the large intestine; considered to be about 60% of the intestine in man, but veterinary anatomists usually refer to it as being only the short terminal section of the small intestine.
Ileum:

Small intestine is suspended from the body wall by an extension of the peritoneum called the mesentery.
Lymphatic vessels are also present, but are not easy to discern grossly in normal specimens.
blood vessels to and from the intestine lie between the two sheets of the mesentery.

T. Serosa: In most of the digestive tract (stomach and intestines) it consists of a thin layer of loose connective tissue covered by mesothelium (a type of squamous epithelium that lines body cavities)
T. Muscularis: endows the digestive tube with an ability to be motile.

T. Submucosa: immediately beneath the mucosa, is a layer of loose to dense connective tissue containing blood and lymphatic vessels
T. Mucosa: Among the four tunics, the mucosa is most variable in structure and function, endowing the tube with an ability to perform diverse and specialized digestive tasks along its length. Of critical importance are the epithelial cells that cover the mucosa and are thus in direct contact with the lumen.

Substances absorption and much of the enzymatic digestion takes place
on the surface of small intestinal epithelial cells, and to accomodate these
processes, a huge mucosal surface area is required.
Lumenal surface area ≈ 0.5 m2
Real absorptive surface area ≈ 250 m2
Small Intestine macroscopic folding
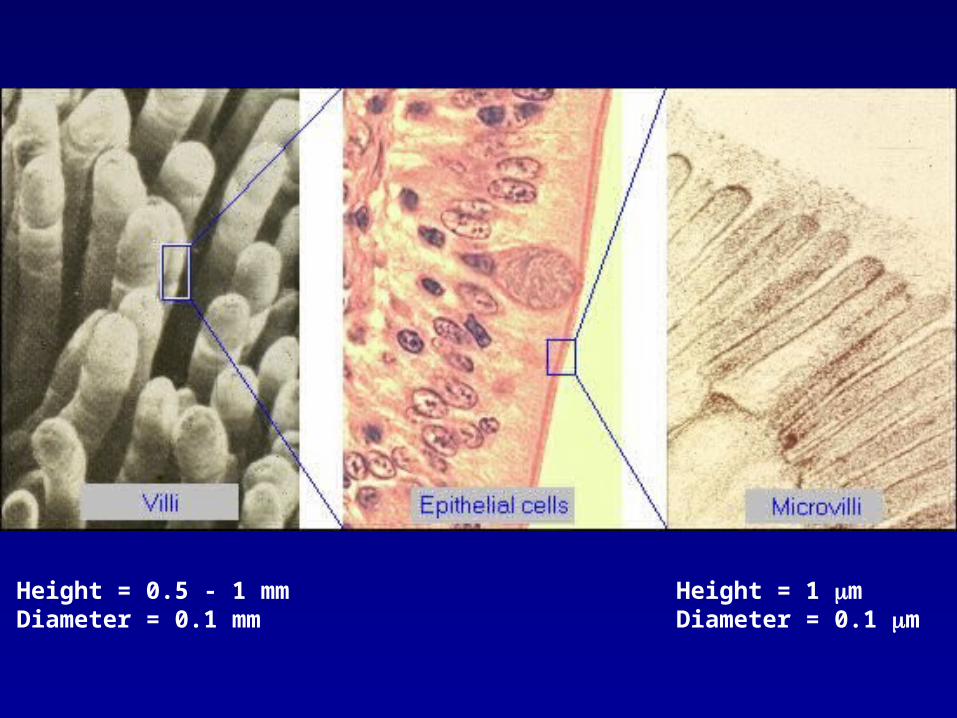
Height = 0.5 - 1 mmDiameter = 0.1 mm
Height = 1 mDiameter = 0.1 m
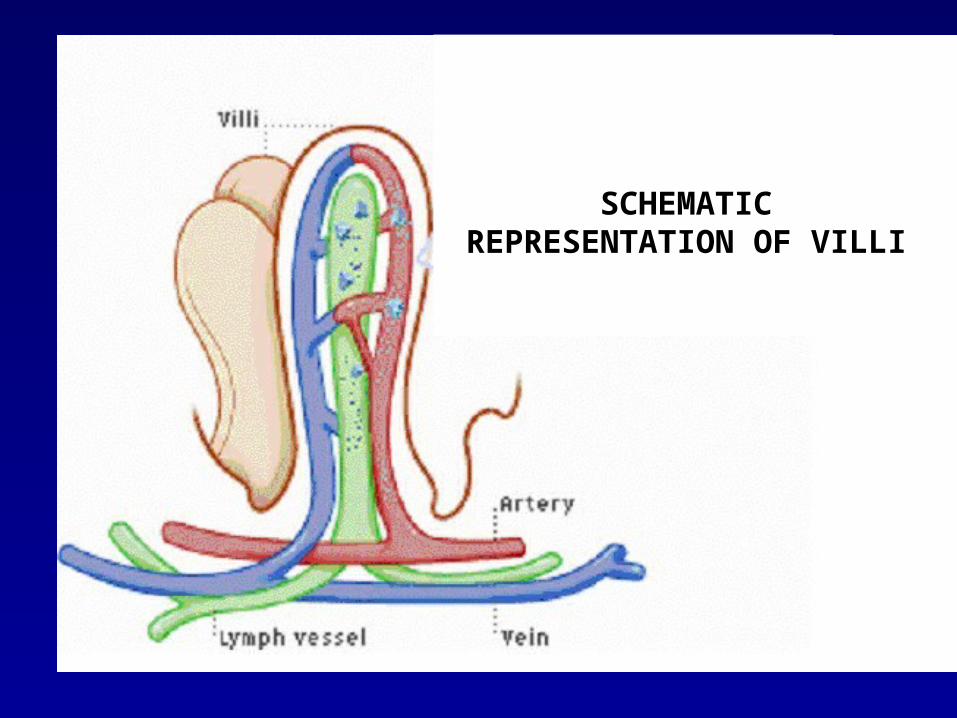
SCHEMATIC REPRESENTATION OF VILLI
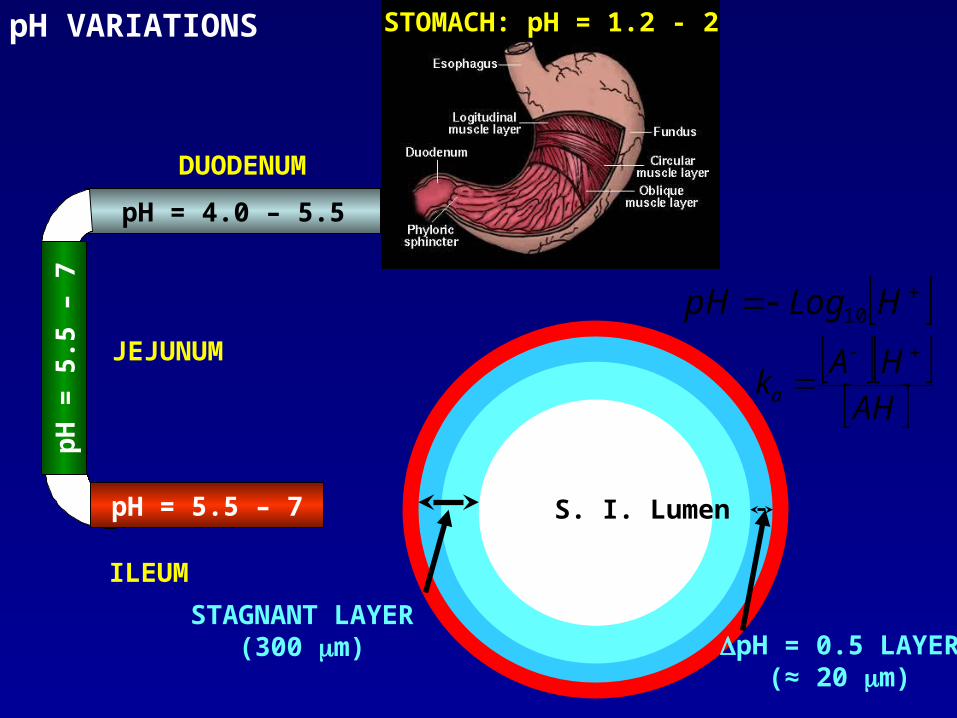
pH = 4.0 – 5.5
DUODENUM
STOMACH: pH = 1.2 - 2
pH
= 5
.5 –
7
JEJUNUM
pH = 5.5 – 7
ILEUM
S. I. Lumen
STAGNANT LAYER(300 m) pH = 0.5 LAYER
(≈ 20 m)
pH VARIATIONS
AH
HAka
HLogpH 10
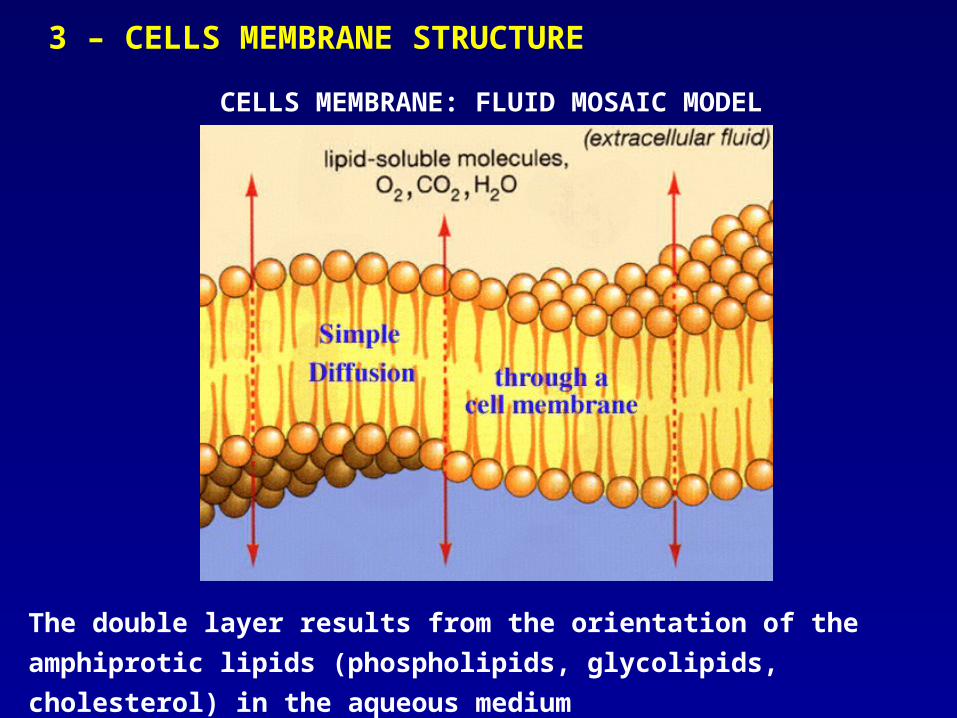
3 – CELLS MEMBRANE STRUCTURE
CELLS MEMBRANE: FLUID MOSAIC MODEL
The double layer results from the orientation of the amphiprotic lipids
(phospholipids, glycolipids, cholesterol) in the aqueous medium

In the membrane, different proteins are embedded performing different functions. Some proteins form selective ion-channels (Na+, K+, Ca++, Cl-).

By the interaction of membrane proteins at the contact surfaces
between single cells so called tight junctions are formed. In most
membranes, these tight junctions contain fenestrae, which can be
regarded as pores filled with water
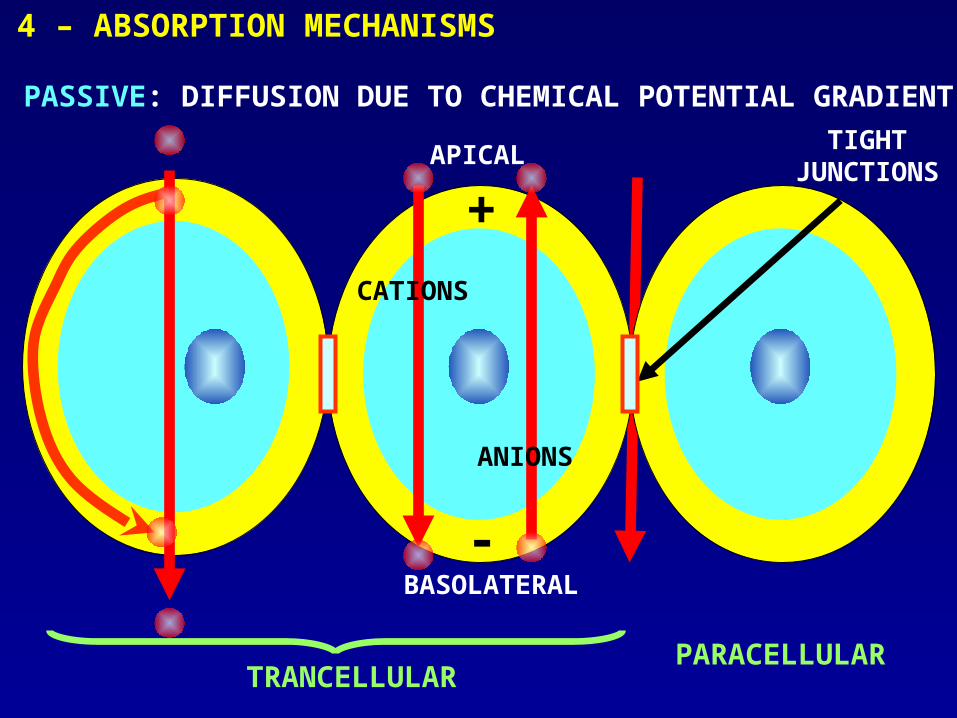
TIGHT JUNCTIONS
PARACELLULAR
4 – ABSORPTION MECHANISMS
PASSIVE: DIFFUSION DUE TO CHEMICAL POTENTIAL GRADIENT
TRANCELLULAR
+
-BASOLATERAL
APICAL
CATIONS
ANIONS

In the small intestine, the surface area presented by paracellular
route constitutes only a small fraction (0.01%) of the total
membrane surface area
DRUG MW < 200
TRANSCELLULARIMPORTANT
PARACELLULAR IMPORTANT
DRUG MW > 200
TRANSCELLULARIMPORTANT
PARACELLULAR NOT IMPORTANT
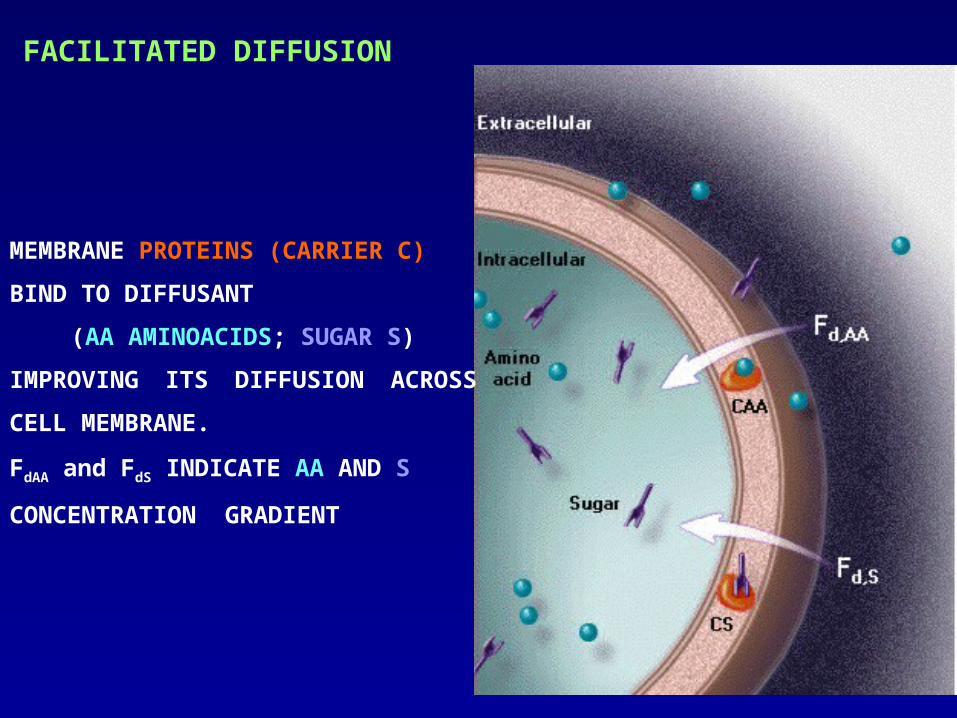
FACILITATED DIFFUSION
MEMBRANE PROTEINS (CARRIER C)
BIND TO DIFFUSANT
(AA AMINOACIDS; SUGAR S)
IMPROVING ITS DIFFUSION ACROSS
CELL MEMBRANE.
FdAA and FdS INDICATE AA AND S
CONCENTRATION GRADIENT

FILTRATION
All passive diffusion processes my be
superimposed by an osmotic water flow,
able to drag along the molecules (=
solvent drug)

ACTIVE: ENERGY IS SUPPLIED TO DIFFUSANT
Endocytosis or Transcytosis:Very large molecules are transported by invagination of the
membrane and subsequent vesiculation and devesiculation
Co-transport:Target molecule associates to another compound that crosses the
cellular membrane due to the existing concentration gradient (this the
case of glucose and aminoacids that associate to Na+ crossing the
cellular membrane according to the concentration gradient).
ATP pump:Energy required for molecules transport is supplied by the hydrolysis
of high energy compounds such as ATP (ATP => ADP + P + energy). A
typical example is represented by the Na+ - K+ pump.

0 6 12 18 24
t(h)
Con
cen
traz
ion
e (
g/m
l)limite di tossicità
limite terapeutico
t(h)
Con
cent
razi
one
(mg/
ml) limite di tossicità
limite terapeutico
sistema tradizionale
sistema a ril. contr.
4 – CONTROLLED RELEASE SYSTEMS

SRCSISTEMA A RILASCIO CONTROLLATO
AUMENTO DELLA PERFORMANCE(EFFICACIA TERAPEUTICA, COSTI)
PROGETTAZIONE
MODELLI MATEMATICI
MODELLI MATEMATICI
MODELLI MATEMATICI
MODELLI MATEMATICI

CRS CATEGORIES
1 PASSIVE PREPROGRAMMED
2 ACTIVE PREPROGRAMMED
2 ACTIVE SELF PREPROGRAMMED

Chamber ISWELLABLE GEL
Chamber IIAQUEOUS SOLUTION
Chamber IIIINSULIN SOLUTION
Glucose permeable membrane(diffusion)
Inward oneway valve(convection)
Outward oneway valve(convection)
Rigid housing
diaphgram
partition
Chamber ISWELLABLE GEL
Chamber IIAQUEOUS SOLUTION
Chamber IIIINSULIN SOLUTION
Glucose permeable membrane(diffusion)
Inward oneway valve(convection)
Outward oneway valve(convection)
Rigid housing
diaphgram
partition

MEMBRANE IMMUNOISOLANTI
RILASCIO DI INSULINA
L. Leoni et al., Advanced Drug Delivery Review, 56 (2004) 211
INSULINMICROFABRICATED
MEMBRANE55
8 m
ENCAPSULATED CELLS
IMMUNOGLOBULINSNa+, K+, Oxygen,
Glucose

S. Z. Razzacki et al., Advanced Drug Delivery Review, 56 (2004) 185