drowning: submersion emergencies presence regional ems june 2015 ce
TRANSCRIPT
Drowning: Submersion Emergencies
Presence Regional EMSJune 2015 CE
Objectives• Define drowning• Discuss the incidence, risk factors
and prevention of drowning• List the basic rules of providing
water rescue• Outline recovery techniques and
resuscitation efforts required for submersion injuries

Submersion EmergenciesSubmersion Emergencies
Introduction• Drowning emergencies are
emotionally traumatic for relatives and loved ones of the patients and emergency providers.
• Many drownings are preventable tragedies resulting from poor judgement, alcohol consumption and inadequate supervision of children.

Incidence• There are an estimated 4,500
drowning related deaths in the United States every year.
• For every drowning death:– 2 people drown and survive with
no disability.– 2 people drown and survive but
have severe neurological impairment

The Numbers May Not Be Accurate
• Victims of drownings from floods and other natural disasters are not counted in drowning deaths.
• Victims of boating accidents are not counted in drowning deaths.

Who drowns?• Children under the age of 4 years
and adolescents and young adults aged 15 to 24 years make up the majority of drowning victims.
• Water sports and the use of alcohol and/or drugs while swimming increase one’s chance of suffering a submersion related injury.

Submersion Emergencies
• Immersion– An incident in which a patient’s face and/or
airway are covered in water
• Submersion– An incident in which a patient’s entire body
including the face and airway is submerged in water
• Water Rescue– An incident in which a person is alert but
experiences some distress while swimming with minimal or transient symptoms

• Drowning– An event in which a patient has primary
respiratory impairment from immersion or submersion in a liquid. The patient may live or die after this event.
Drowning Death– An event of drowning in which the patient is
pronounced dead within 24 hours of the event. Pronouncement may occur on scene or at the hospital.
• Drowning-related Death– Incident in which a submersion patient dies
more than 24 hours following the event.

The best treatment for drowning is prevention.

Prevention
• Many drowning victims are infants and small children.
• Prevention can be a matter of following some common sense practices.

Prevention of Drowning
• Keep only a few inches of water in the bathtub when bathing young children.
• Never leave young children unsupervised in bathtubs.
• Never leave children alone in or near a pool EVEN FOR A MOMENT regardless of safety precautions such as self locking gate and pool alarms.

• Be sure that adults and adolescents are trained in CPR so that they can rescue a child if necessary.
• Surround pools on all 4 sides with a sturdy five foot fence. The house should not be one of the barriers to the pool if there is a doorway from the home to the pool area.
• Be sure that gates self-close and self-latch at a height that children cannot reach.

• Keep rescue equipment (shepherd’s hook and life preserver) and a portable phone near the pool.
• Avoid inflatable swimming aids such as “floaties”. They are not a substitute for approved life vests and can give children a false sense of security.
• Whenever infants and toddlers are in or around water, an adult should be within arm’s length, providing touch supervision.

Where People Drown
Why Do Drownings Occur?
• Swimming/boating issues:– Exhaustion in the water– Losing control or being swept into deep water– Becoming tangled or entrapped while in the water– Using poor judgment while in or near water– Panicking while in water– Losing a support such as a sinking boat
•
• Precipitating Factors– Using alcohol or drugs in or near the
water– Suffering a seizure, heart attack, or
other debilitating condition while in or near water
– Becoming hypothermic while swimming
– Suffering trauma or a diving accident

Pathophysiology of Drowning
1. Victim’s airway is below the surface of a liquid
2. Victim involuntarily holds breath3. Water swallowing begins into
posterior pharynx and into stomach4. Involuntary laryngospasm (closing
of vocal cords) due to liquids in the oropharynx.


5. Blood oxygen levels drop and carbon
dioxide levels raise.6. Due to worsening low oxygen/high
carbon dioxide and unconsciousness laryngospasm stops and vocal cords open.
7. Gasp reflex – if the victim’s head is out of the liquid may begin coughing and clearing airway

8. If the victim’s head is still under the liquid, liquid enters the lungs.
9. Surfactant “washout” occurs10. Worsening hypoxia11. Cardiac arrest12. DEATH

Drowning Process

Predicting the Outcome of Drowning
• Duration of submersion
• Severity of hypoxia
• Neurologic impairment due to lack of oxygen to the brain

• Drowning victims who have spontaneous respirations and pulses in the field before arrival in the Emergency Department usually recover with good neurological outcomes.

Surviving Drowning/Time
Duration of Submersion Likely to Survive without Neurological Damage
0 to up to 5 minutes 90%
5 up to 10 minutes 44%
10 up to 25 minutes 12%
25 minutes or longer 0%

Surviving Drowning/Clinical Findings
Initial Clinical Findings Likely to SurviveWithout
Neurological Damage
Some coughing, normal breath sounds 100%
Coughing, with wet rales in one lung 99.4%
Coughing, bilateral wet rales or pulmonary edema, good vital signs
95%
Coughing, bilateral wet rales or pulmonary edema, low BP 80%
No spontaneous respirations, pulse is present 56%
Cardio/pulmonary arrest, no spontaneous breathing, no pulse
7%
Drowning Related Death
• People die in the hospital after a drowning incident because of– Brain death from lack of oxygen– Acute respiratory distress syndrome – Multi-organ system failure– Sepsis (system wide infection)

Management of Submersion Emergencies

Management• Rescue• Airway/Ventilation• Hypothermia• Associated Trauma
Rescue• Provider Safety• Don’t Jump in to Help if you Can’t
Swim!!! • Make use of a conveyance device
– Boat– Raft– Floatation device

If you are the only rescuer. . .
• If the victim is not breathing provide 2 minutes of rescue breaths before calling 911.
• If the victim is pulseless
and not breathing provide
5 cycles of CPR (2 minutes)
before calling 911.

Airway/Ventilation• The most dangerous consequence of
submersion emergencies is lack of oxygen.
• Open the victim’s airway as soon as possible and begin assisted ventilations.
• Rescue breathing should begin as soon as a submersion victim is removed from the water.

Let’s practice airway management•Practice opening airway and BVM ventilation•One rescuer and two rescuer
THERE IS NO NEED TO DRAIN WATER FROM THE LUNGS
• Fluids in the airway and lungs of a submersion victim absorb quickly
• Most water will come from the stomach

No Heimlich Maneuver!!
• Routine use of the Heimlich Maneuver or chest compressions to remove water only leads to– Vomiting– Aspiration– Delay in beginning ventilations

Vomiting• 67% of submersion victims who
require ventilation assistance vomit.• 86% of submersion victims who
require ventilation and chest compressions vomit
• If vomiting occurs turn the patient on their side and suction
•

– Body requires core temp of 98.6oF (37oC) for proper function.
– If core temp significantly rises above or falls below 98.6oF (37oC), the cells’ ability to function is impaired, especially those of the brain, heart, and kidneys.
– Can result in permanent disability and/or death of the patient.
Body Temperature: Hypothermia

Submersion and Hypothermia
• Mammalian Diving Reflex– The mammalian diving reflex activates
when a person dives into cold water (<70oF).• Larynx spasms.• Breathing is inhibited.• Heart rate slows.• Blood vessels constrict.• Blood flow to the brain and heart are increased.
• Treat as Hypothermic Cardiac Arrest
How will you manage hypothermia?
• Check for a pulse for at least 10 seconds
• Remove wet clothing• Warm blankets• Turn up heat in unit• Prevent further loss of heat
Associated Trauma• Routine spinal motion restriction in
submersion emergencies is not recommended.
• Applying SMR can delay opening the airway and ventilating the patient.

Spinal Injuries in Submersion Incidents
Suspect spinal injury if:
• Submersion has resulted from a diving mishap or long fall.
• Patient is unconscious.
• Patient complains of weakness, paralysis, or numbness.
• You suspect the possibility of spinal injury.

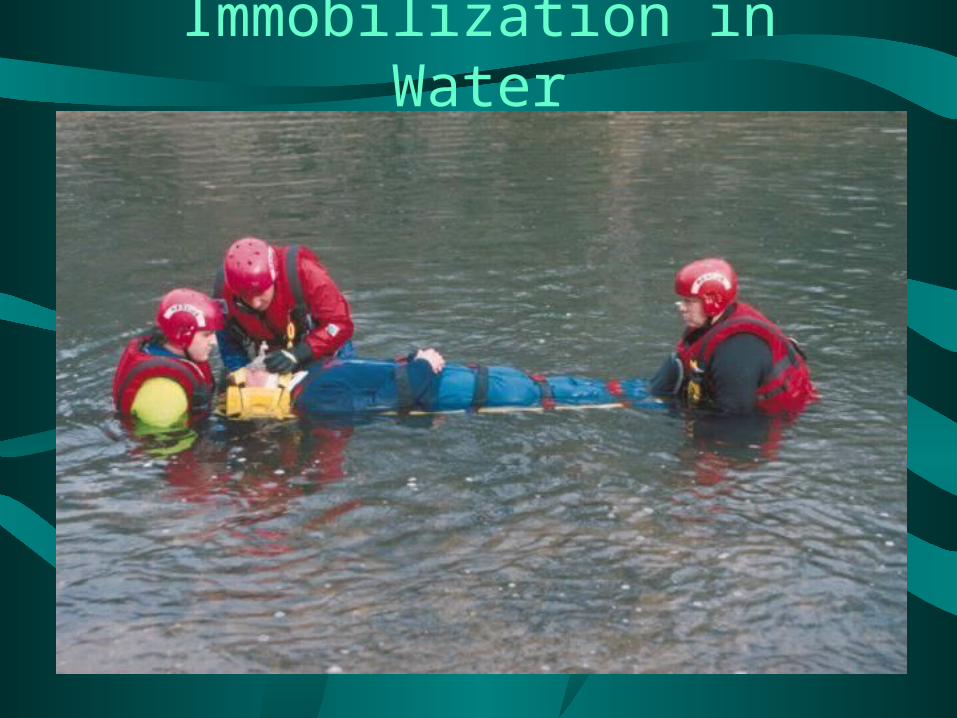
Immobilization in Water
• Turn the patient into the supine position.
• Restore the airway and begin breaths if needed.
• Float a spine board under the patient and secure the patient.
• Remove the patient from the water.
Immobilization in Water

Let’s practice immobilization
•Practice in the water if you can.
Transport• Not all submersion victims suffer cardiac
or respiratory arrest.• Some victims are able to cough and clear
their airway, resuming normal ventilations on their own.
• All victims of drowning who require care by EMS, even if they are alert and demonstrate adequate breathing should be transported to the hospital for evaluation.

Review• Consider the following scenario and
review questions as a group.• If doing this CE individually, please e-
mail your answers to:• [email protected]• Use “June 2015 CE” in subject box.• You will receive an e-mail confirmation.
Print this confirmation for your records, and document the CE in your PREMSS CE record book.

Submersion Emergencies
Review Questions1. All of the following are causes of
submersion emergencies except:
A. ExhaustionB. A full stomachC. Becoming entangledD. Use of alcohol and drugsE. Suffering trauma while in the waterF. Have a medical emergency such as
a heart attack in the water

2. What are the 3 main concerns in submersion emergencies?
A. Rescue, C-spine injury, airway and heat exhaustion
B. Rescuer safety, hyperthermia and fractures
C. Airway, breathing and circulationD. Rescue, airway/ventilation,
hypothermia and associated trauma

3. True or False
Only specially trained rescuers should
attempt to rescue and remove a submersion
victim from deep water.

4. Suspect a C-spine injury in a submersion victim if they are:
A. Awake and talking but confusedB. UnconsciousC. Moving their arms and legs with no
problemD. Complaining of chest pain

5. All but which of these happen to the body when the Mammalian Diving Reflex is activated in cold water?
A. The patient becomes hyper-alertB. Heart rate slowsC. Increased blood flow to the brain
and heartD. Breathing is inhibited

Case Study 1
• You respond with your department to a drowning at a hotel.
• On arrival you find a young adult male lying by the pool with 2 adults performing CPR.
Scene Size Up
• The scene is safe• The hotel pool does not have a life
guard.• Hotel personnel report that bystanders
found the man at the bottom of the pool.
• Hotel personnel say he could not have been there for more than 10 minutes.
• The hotel does not have an AED.

Initial Assessment
• Airway: water is in the airway
• Breathing: the man is not breathing
• Circulation: a faint slow pulse is found at a rate of 30 beats/minute.
• How do you want to proceed?

• Does the patient need an AED at this point?
• If a submersion victim needs an AED what safety precautions must be taken?

SAMPLE History
• No one knows who the man is so no SAMPLE history is available.
• A hotel guest tells you that she thinks this man was diving off the edge of the pool earlier.
• How will this change your management of this patient?

• What else could have caused a submersion emergency in a 20 year-old male?
• Do you need to do any other treatment or can this man be transported?

Case Study 2
• You are called to a family home for an unresponsive toddler.
• On arrival you find a frantic young woman attempting CPR on a small child next to a child’s wading pool.
Scene Size Up
• It is a warm July day• The wading pool has 8 inches of water
in it• The young woman is the mother of the
victim Billy who is 3 years old.• She states “I went to get my cell
phone. I was only gone for a few minutes. He was face down in the pool.
• Do you need to assume spinal motion restriction?

Initial Assessment
• Billy is unresponsive
• There is clear water in the airway
• Billy is not breathing
• Billy has a rapid carotid pulse.
• How do you want to proceed?
• Do you need an AED?

SAMPLE• Allergies: none• Medications: none• Past Medical History: none healthy 3
year-old. Weighs 32 pounds• Last meal: Lunch 2 hours ago• Events: His mother let Billy get in the
pool this afternoon to play. She left him for less than 5 minutes to get her cell phone from the house

• After about 3 minutes of BVM ventilations Billy begins to cough.
• He vomits a large amount of clear water and begins to cry lustily.
• He holds out his arms for his mother.
• Pulse is 120, Respirations are 30 and deep.

Head to Toe• No DCAPP BLS TIC to
– Head– Neck– Chest– Abdomen– Legs, Arms Back

Assessment Cont.• Billy vomited about 500 cc of clear
liquid.• He has some soft rales in the bases
of both lungs.• He is able to be comforted by his
mother.• His lips are pale and he is shivering.

• How is Billy doing?• What additional care does Billy
need?• Does he need to be transported to
the hospital?
Answers• 1. B• 2. D• 3. True• 4. B• 5. A

• Case Study 1– Suction airway– Keep airway open (manual opening, oral
pharyngeal airway) – Ventilate with BVM with 15 liters 02 at
one breath every 6-8 seconds.– Begin chest compressions for slow pulse– Begin passive rewarming (cover with dry
blankets)

• The patient does not need an AED at this point.
• Dry off his chest before attaching the AED pads.

• If the patient was diving into the pool he may have a C-spine injury so Spinal Motion Restriction must be applied.

• The submersion emergency could have been caused by:– Drug overdose– Alcohol intoxication– Seizures– Cardiac episode

• Continue CPR and transport. • If ALS treat Bradycardia PEA and
transport.
• Case Study 2– Spinal motion restriction is not
indicated– Suction Billy’s airway and begin BVM
ventilations on 15 liters O2 at 1 breath every 6-8 seconds.
– No AED is indicated

• Billy is doing better• He needs:
– passive rewarming with blankets– Oxygen by Non-rebreather mask or
blow by– Reassurance
He needs transport to the hospital.
