d.rizik, tryton breakfast symposium introduction_the challenge of treating bifurcation lesions
TRANSCRIPT

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
k Tryton Breakfast SymposiumSession Introduction:
The Challenge of Treating Bifurcation Lesions
David G. Rizik, M.D., F.A.C.C., F.S.C.A.I.Chief Scientific Officer
Director of Structural & Coronary InterventionsHonorHealth and the Scottsdale-Lincoln
HealthNetworkHon
orH
ealth
/ Sco
ttsd
ale-
Lin
coln
Hea
lth N
etw
ork

Disclosure Statement of Financial Interest
I, (David G Rizik, MD), DO NOT have a financial interest/arrangement or
affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this
presentation
Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kQ1: Why is stenting the standard for the
treatment of these lesions subsets?
• Discrete• Long Segmental• Calcified• Eccentric • Saphenous Vein Graphs• CTO’s• In-Stent Restenosis• Thrombotic• Type A, B1, B2, C
A1: Stenting provides a wide variety of lesion subsets predictable procedural
success with a durable result.

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kQ2: What is the only major lesion subset which
stenting is not the current Standard?
A2: Bifurcation Lesions: Workhorse stents do not provide the same predictable and durable results as straight lesion
Scot
tsda
le-L
inco
ln H
ealth
Net
wor
k
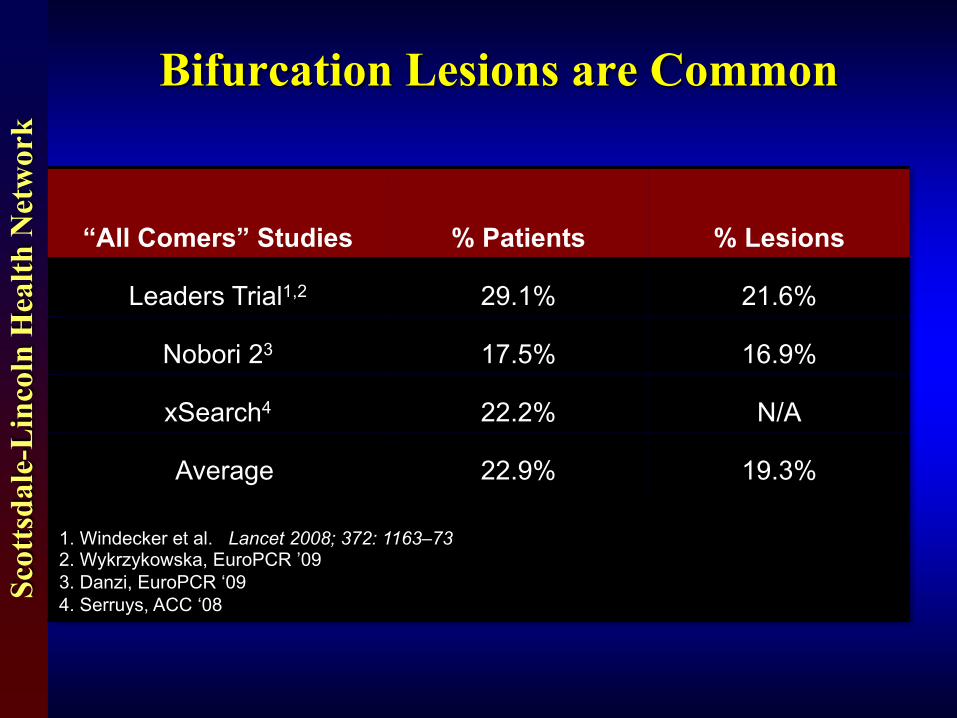
Bifurcation Lesions are Common
“All Comers” Studies % Patients % Lesions
Leaders Trial1,2 29.1% 21.6%
Nobori 23 17.5% 16.9%
xSearch4 22.2% N/A
Average 22.9% 19.3%
1. Windecker et al. Lancet 2008;; 372: 1163–732. Wykrzykowska, EuroPCR ’093. Danzi, EuroPCR ‘094. Serruys, ACC ‘08

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kTreatment of Branching Geometry Lesions Using
Currently Available Technology Yield Complications
• Thrombosis Rate– Incidence: 3.6-3.9%
– Hazard Ratio: 4.6-6.5
• Restenosis Rates– Angiographic 20-40%

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kBifurcation Lesions:
Large Variation: Extent of Disease, Angle & Diameter
Case Courtesy of DrsKutcher & Holland, USA
Courtesy of P Brunel, France
Courtesy of Dr. Dumonteil, France
Courtesy of Prof. R. Kornowski, Israel
Courtesy of Dr. Th. Lefèvre, France
Courtesy of Dr. Schulze, Germany
Courtesy of Dr. M. Lesiak, Poland
Courtesy of Drs. E. Grübe -R. Müller, Germany
Like finger prints: No two bifurcations are alike
Scot
tsda
le-L
inco
ln H
ealth
Net
wor
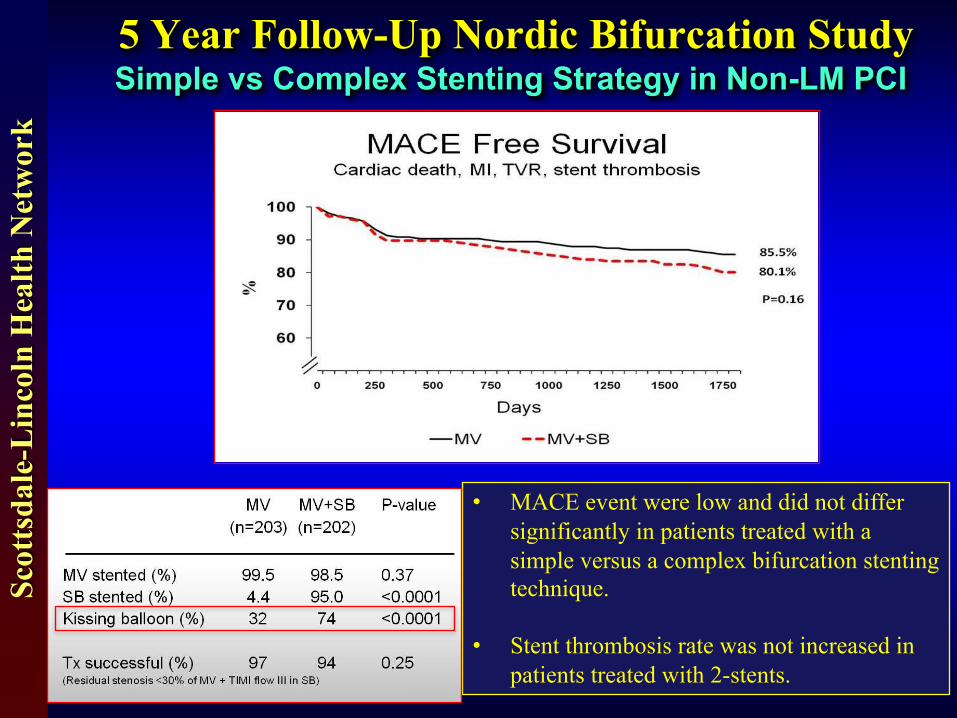
k5 Year Follow-Up Nordic Bifurcation StudySimple vs Complex Stenting Strategy in Non-LM PCI
• MACE event were low and did not differ significantly in patients treated with a simple versus a complex bifurcation stenting technique.
• Stent thrombosis rate was not increased in patients treated with 2-stents.

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kMeta-Analysis: NORDIC I & BBC I (Non LM Bifurcations)
Probability of MACE (Death/MI/TVR)
Difference in MACE favoring a simple strategy
What is the relevance of peri-procedural MI ?
25-50% of patients in randomizedtrials have little or no SB disease.
Most one vs two stent trials have focused on bifurcations with diminutive SB diameters

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kMore Contemporary Trials Involving Large Side
Branches Favor 2- stent Strategy

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
k
Key Points• Bifurcation Lesions: Continues to be problem Only Lesion Subset Not Routinely Stented
• Combined Literature: Supports Provisional over 2 Stent Strategies
• Study Population Primarily Focused on Small SB– BBC 1– Nordic 1
• Studies with Large SB Favors 2 Stent Approach– DK Crush– 2 Stent ‘Simple’ Dedicated Stent
• Tryton is a Dedicated Side Branch Stent: Focused on Providing Straight Forward 2 stent solution

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kTryton Side Branch StentProduct Features
• Cobalt Chromium (CoCr)• Strut thickness: 84µm• Delivery System: Rapid Exchange • Side Branch Diameters: 2.5-3.5 mm
• Guide Size: ≥ 5 Fr (Operator’s Choice)• Guide Wire: 0.014” (Operator’s Choice)
• Main Vessel Stent: Workhorse DES (Operator’s Choice)

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kTryton Side Branch Stent™
Main Branch Zone & wedding band
8mm
*: 5.5mm for Large Vessel diameters**: 18mm for Large Vessel diameters
Total stentlength: 19mm**
Transition Zone
4.5mm
Side Branch Zone
6.5mm*
Necessarily Employs a Save the Side Branch Strategy

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
k
Tryton Deployment Sequence1. Wire both vessels and pre-dilate SB 2. Position Tryton
3. Perform P.O.T. 4. Position DES and remove ‘jailed’ wire
5. Deploy DES and re-wire SB 6. Simultaneous Kissing Balloon

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
kComplex LAD-Diagonal Lesion
A2: Treated Electively via right radial 6 Fr. Sheath with Tryton Side Branch Stent
Case Courtesy of Michael Kutcher, M.D. Wake Forest Baptist Medical Center

Scot
tsda
le-L
inco
ln H
ealth
Net
wor
k
Tryton Breakfast Symposium