dr.ganesh kodaikanal-ppt
TRANSCRIPT

IMPLANTS & IMPLANTOLOGY… – FROM EXOTIC TO EVERYDAY
Dr.P.R.GANESH Periodontist & ImplantologistChennai.
Lecture by
This Lecture Covers -
1. What did the profession believe in late 1970's about the then new field of implantology?
2. What do we believe now in 2015 and why?
3. Where do we believe that osseointegration research and the practical applicability of oral implants will go in the next 5–10 years?
W. R. Laney - International Journal of Oral and Maxillofacial Implants (JOMI)
An Implant Is Defined As ….
An Artificial Material Or Tissue That Shows
Biocompatibility Upon Its Surgical Implantation
Ankylotic Anchorage of a CP Titanium Implant
has been accepted as the desirable interface
between bone as a living tissue
and a metal implant.
(Albrektsson et al. 1981; Brånemark et al. 1969/77)
OSSEOINTEGRATION……
Osseo-integration & Dentistry…in The Beginning

From Transplants To Implants….Who on earth was the first to come up with the idea of using an ARTIFICIAL tooth root to replace a missing natural tooth?
•The idea of replacing a missing tooth with someone else's NATURAL tooth goes back to Ancient Egyptian Times.
•But it didn't work very well! In fact, transplanting a tooth from one person to another has never really worked, even nowadays with all the advances in transplant medicine.
So the technology simply moved on from transplants to implants
1st Historic Record of Implant
The first person to publish a description of the technique
of modern dental implants was a French dentist,
MAGGIOLO J IN 1809.
Maggiolo described a method to implant 18-karat gold alloy, with
three branches into the jawbone and to install a porcelain
crown as a superstructure in his book:
“Le Manuel de l’Art du Dentiste” (1809)

1st Historic Record of Implant…
Maggiolos’s Implant Model
In 1850’s …..to 1890’s
• Harris constructed a socket in the jawbone to insert a
column made of PORCELAIN - coated with a rough layer of lead
in order to increase the supporting strength (so ceramic implants are not that
new an idea)
• Berry constructed a root-form porcelain implant that was Lead-free.
• Pajime - Silver implant.
• Bonwil - Gold And Iridium implant.
The 20th century…..• 1905 - Scholl made a root-form, porcelain implant.
• 1937 – Stock used Vitallium, a cobalt-chromium-
molybdenum alloy .
• 1940- Dahl was the first to attempt subperiosteal implant.
And we all know who had the bright idea
for an artificial titanium dental implant in 1969.

RIP …a tribute….

Branemark’s Original research – titanium chambers in rabbit bone- Osseointegrated
• Per-Ingvar Brånemark (May 3, 1929 – December 20, 2014) a Swedish physician, touted as the "FATHER OF MODERN DENTAL
IMPLANTOLOGY".
• In 1982 in Toronto, Brånemark presented work that had begun 15 years earlier in Gothenburg.
• Brånemark's investigations into the phenomenon of OSSEOINTEGRATION or the biological fusion
of bone to a foreign material, in this case TITANIUM, reinvigorated the field of implantology.
• The Toronto conference brought widespread recognition to the Brånemark implant methods and is one of the most significant
scientific breakthroughs in dentistry.

“A vast number of patients are indebted to the Toronto
Osseointegration Conference in Clinical Dentistry in May
1982. This singular initiative rendered the use of implant
interventions for edentulousness available to
the general public much earlier than usual for new
treatment modalities, which often take years to be
implemented.”
Dr,Asbjørn Jokstad
Implantologist
33 Years (1982-2015) since …..
Professor Branemark
introduced Osseo-integration and founded the field of
Implantology...
Why The Excitement About Implant Rehabilitation?
Firstly, in earlier days, old age was associated with almost
INEVITABLE EDENTULISM, with consequences for personality,
nutrition, communication etc. Now even those patients can receive
rehabilitation of oral function, with the same results and prognosis as
for any other patient.
Secondly, through OSSEOPERCEPTION, the dentate mouth
communicates with the brain, improving not only daily function, but
also being an important factor in NEURONAL STIMULATION- another
reason to include the mouth in considerations of overall health

In Branemark’s own words….
• The mouth is a much more important part of the human body than modern medicine recognizes.
The edentulous patient is an amputee, an oral invalid, whom we
should help with rehabilitation.
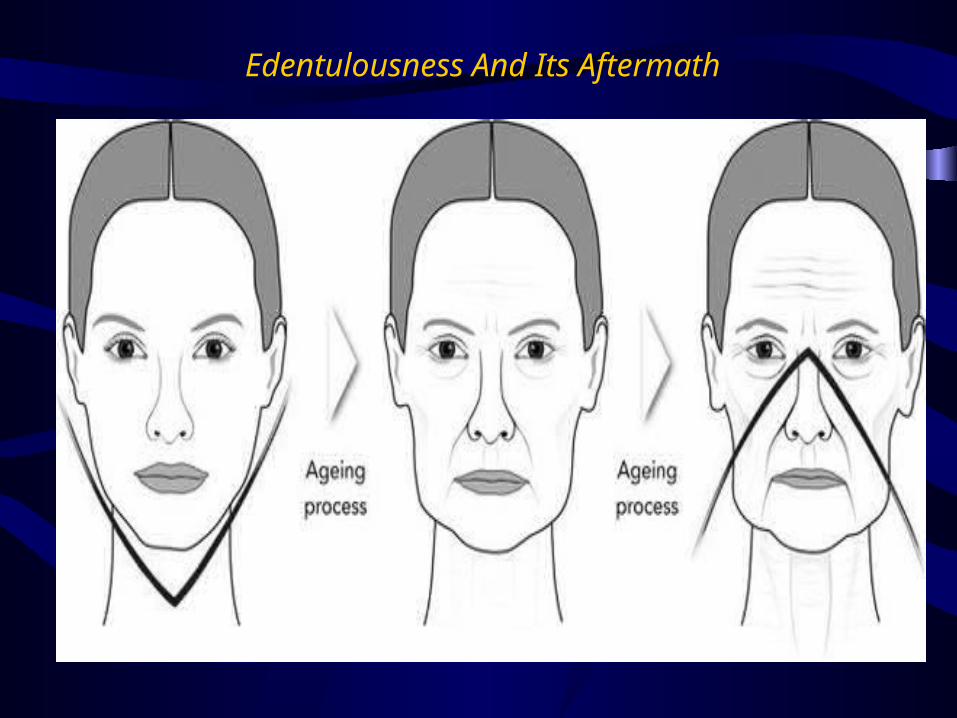
Edentulousness And Its Aftermath
So Rehabilitation – according to Brånemark et al. 1977
should include…
Restoring FORM,
FUNCTION, AND
AESTHETICS has always
been the goal of oral
rehabilitation .
The 33rd anniversary of
Osseointegration (1982-2015) is an
appropriate time to take stock of
what has been achieved and to
focus on what is emerging as new
and innovative developments in the
field of osseointegration.

So What’s New After 30 Years ?
30 years ago we did not have answers to questions such as:
1. Does The Technology Work?- Effectiveness
2. How Does The Technology Work?- Process
3. Does It Matter To Patients? – Salience
4. Will It Do More Good Than Harm? - Safety 5. Is It Worth Paying For The Intervention?- Cost
Effectiveness.
These clinical questions of relevance now have a few answers after 30 years.
So what has changed in 30 years ?
In 1982 the protocol advocated by Dr. P.I.Branemark
A. 1- Implant Design, B. Made From 1- Grade Of Titanium, C. Using 1- Surgical Procedure, D. For 1 Indication i.e. Completely Edentulous Jaws.
Today, we are confronted with a phenomenal diversity of products, materials, techniques and applications of
technologies built on osseointegration.
Original Branemark Protocol -
Changes in Treatment Planning/ Indications
Original Protocol - Fully Edentulous Patients
Modern Protocol - All types of Indications -extraction & immediate implant

Changes in Indications & Criteria
Original Protocol –Strict
Inclusion & Exclusion
Criteria
1. Bone Height of 10mm
2. Bone Width of 7-8mm
Modern Protocol –Rare
Exclusion criteria-
A. Guided Bone
Regeneration
B. Sinus Lift
C. Bone Expansion

No more “Ideal” implant criteria..
Modern Protocol - GBR
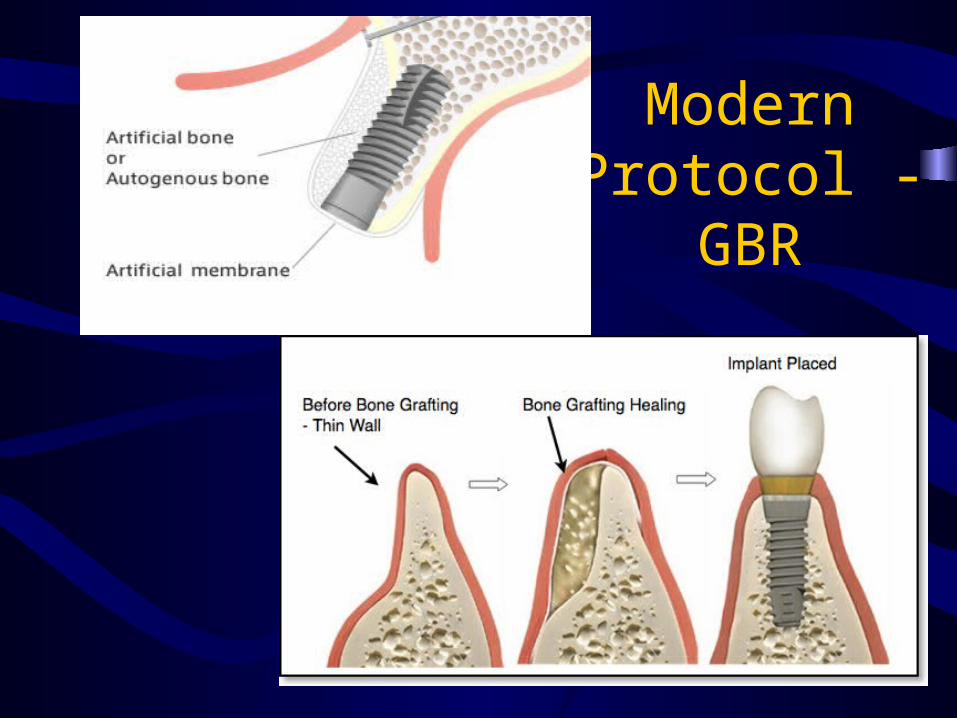
Modern Protocol -
GBR
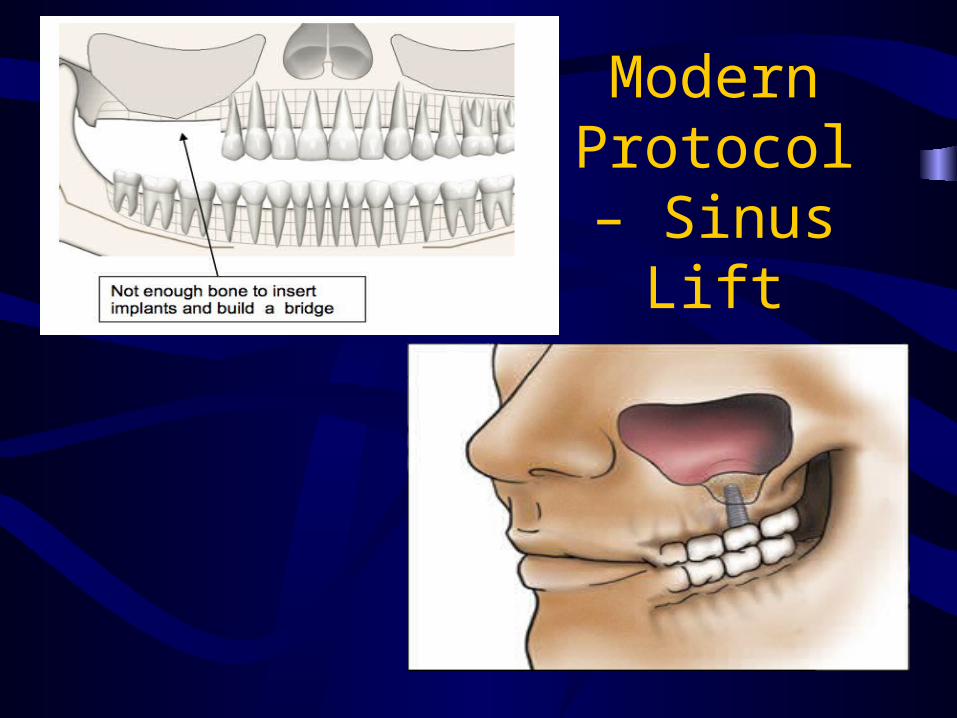
Modern Protocol – Sinus Lift
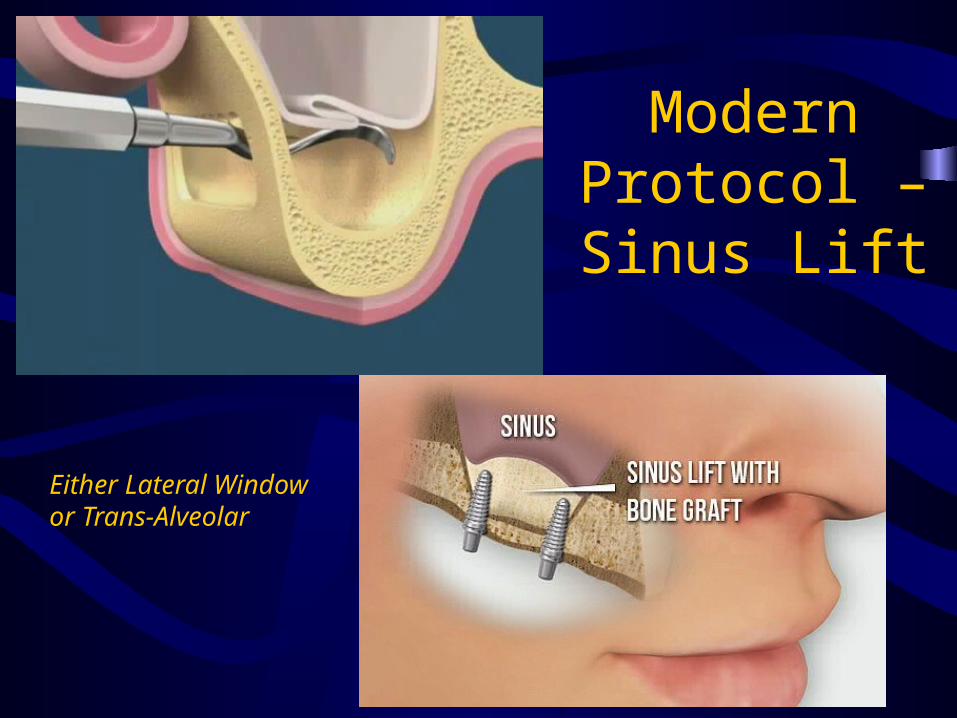
Modern Protocol – Sinus Lift
Either Lateral Window or Trans-Alveolar
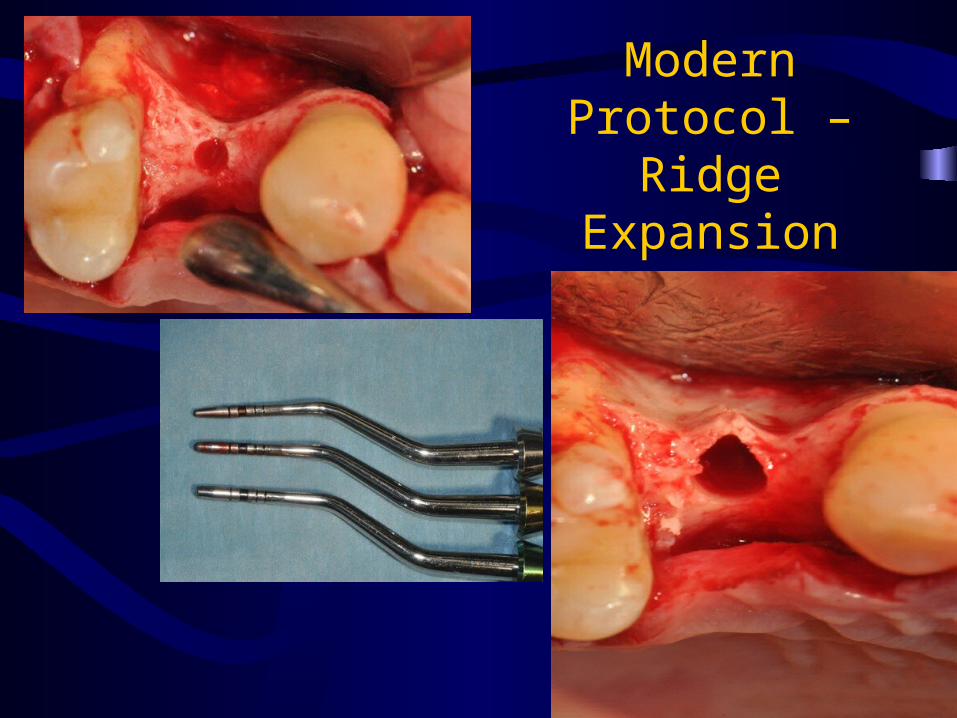
Modern Protocol – Ridge
Expansion
Changes in Treatment Planning
Original Protocol -
1. OPG
2. Lateral Cephalogram
3. Periapicals
Modern Protocol –
1) CT
2) CBCT
3) Guided Implant
Placement
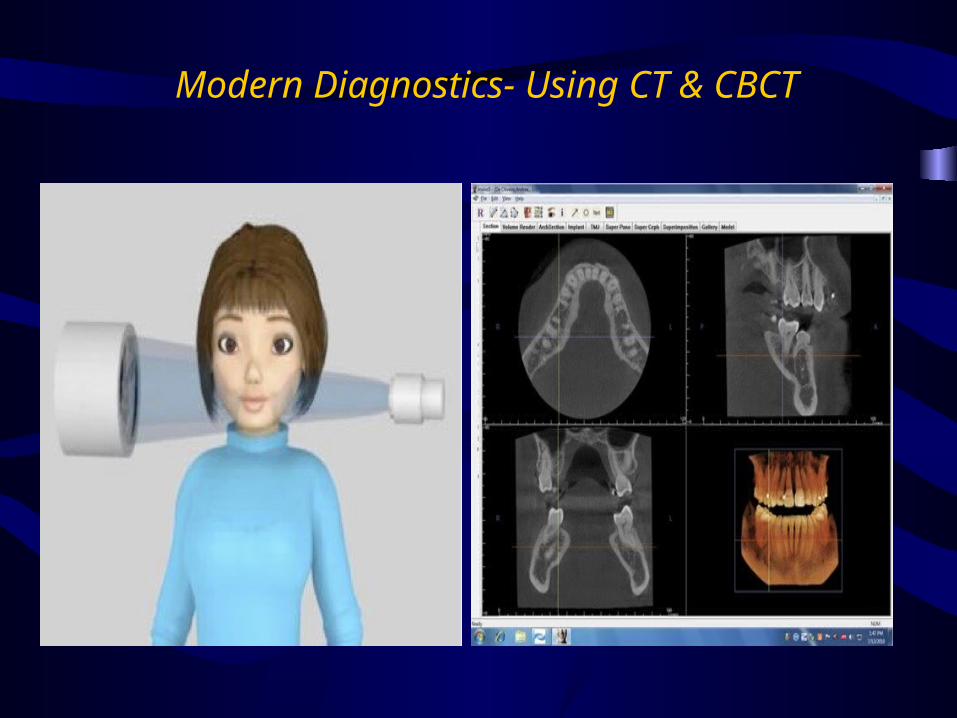
Modern Diagnostics- Using CT & CBCT
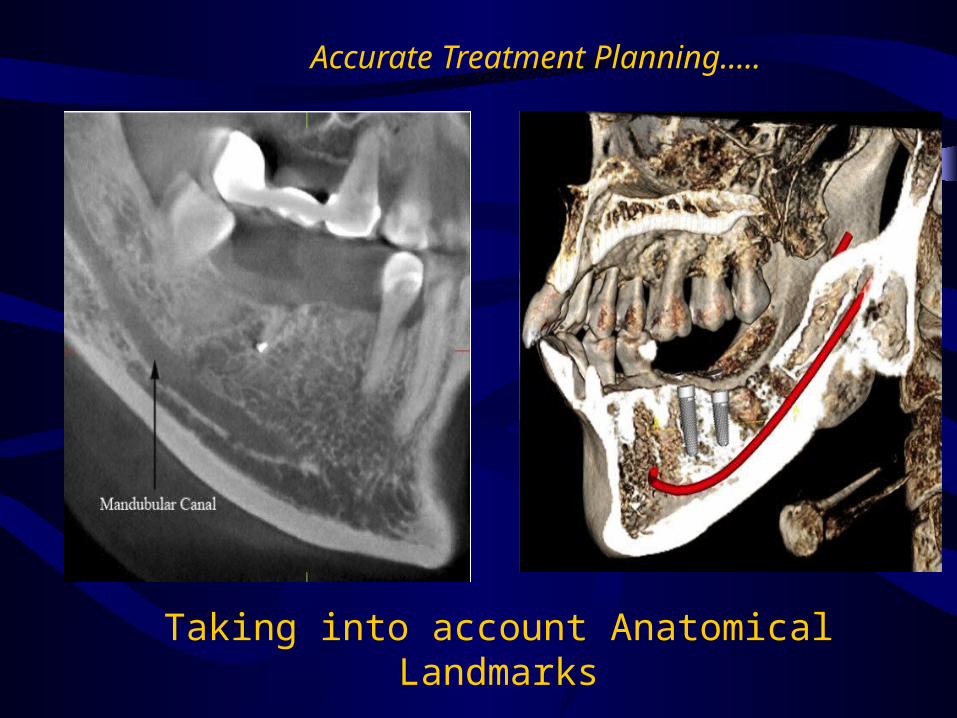
Accurate Treatment Planning…..
Taking into account Anatomical Landmarks
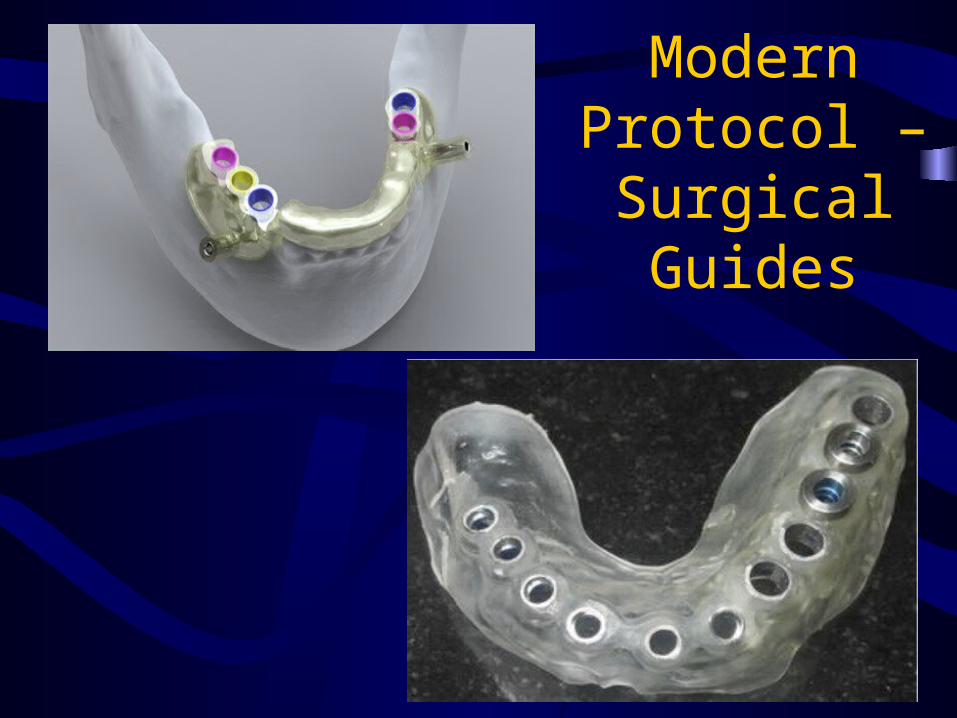
Modern Protocol – Surgical Guides

Modern Protocol- Risky Patients?
• SMOKING may be associated with a greater incidence of
implant failure, but studies have often analyzed data at the
implant rather than the patient level, thereby biasing
conclusions.
• DIABETIC patients may have greater risk of implant failure,
but evidence is not strongly supportive.
• Compelling evidence does not exist to link OSTEOPOROSIS or
use of oral bisphosphonates to implant failure, yet concern does
exist with possible post-surgical side effect of osteonecrosis
with bisphosphonates.

Changes in Surgery – Quirynen etal Perio 2000 Vol.66, 2014
Original Protocol
a) Pre-surgical & Post
Surgical Antibiotics
b) Low speed placement/
excessive cooling
c) Two-Stage Surgery
d) Delayed Loading
e) Screw retained Prosthesis
Modern Protocol
1) Only Pre-surgical
Prophylaxis
2) Higher Speed Placement/
cooling not essential
3) One-Stage Surgery
4) Immediate Loading
5) Cemented Prosthesis

Are prophylactic antibiotics effective in reducing postoperative infections and failures? Esposito et al. 2008.
•A meta-analysis suggested that 2 G Of Amoxicillin given 1
hour pre-operatively significantly reduces early failures of
dental implants.
•Therefore it might be sensible to suggest the routine use
of one dose of prophylactic amoxicillin just before placing
dental implants.
•It remains unclear whether an adjunctive use of post-
operative antibiotics is beneficial.

So Modern Protocol- Pre-op YES and Post-op NO for Antibiotic Prophylaxis.

1-Stage Vs. 2-Stage… ? ? ?
Is A One-Stage Implant Placement Procedure As Effective As A Two-Stage Procedure Submerging The
Implants Under Soft Tissue For Undisturbed Healing? Esposito 2008
NO RELEVANT CLINICAL DIFFERENCES
appear to exist between a One- Or a Two-stage Implant Procedure.
The major clinical implication is that the one-stage approach might be preferable since it has only one
surgical intervention and shortens treatment times.

1-Stage Vs. 2-Stage
However, a two-stage submerged approach is
preferable ….
A. When an implant has not obtained an optimal
primary stability or
B. When barriers are used for guided tissue
regeneration.

Flap Vs. Flapless ? ? ?
Flap Vs. Flapless ? ? ? - Esposito 2008 -Systematic Review
• Evidence suggests that flapless procedures cause less
postoperative pain, edema and consumption of analgesics
than conventional flap elevation.
• Flapless surgery performed by skillful clinicians in
properly selected cases can be as successful and
complication-free as conventional.
• However clinicians should select patients for flapless
implant placement with a great deal of caution in relation
to their own clinical skills and experience

Flapless- is like a banana peel…only with good clinical skills

When Brånemark et al. (1977) introduced the
principles of osseointegration 30 years ago –
a. Primary Stability
b. Lack Of Micromotion
were considered to be the Two Main Factors
necessary for achieving predictable high successes
of 92–98% for Osseointegrated implants after 10
years in the maxilla and mandible, respectively
(Adell et al. 1990)
Loading…Original Protocol

Delayed Vs..…Immediate Loading
Loading……Why Immediate?
Mechanical loading is known
to be a
particularly potent stimulus
for
bone cells if it does
not exceed certain values
(Robling et al. 2006)
Loading……Why Immediate?Controlled implant loading leads to a positive effect
on the initial bone formation.
Gotfredsen et al. 2001- reported that static continuous loads on implants resulted in
Increased Bone Density.
Heitz-Mayfield et al. 2004 - transient functional loads act physiologically as a
Trigger For Bone Remodeling
Modern Protocol- Immediate Loading beats Delayed Loading
Esposito et al - Systematic Review (2009) - came to the following
conclusions:
“It is possible to successfully load dental implants
immediately or early after their placement in selected
patients, though not all clinicians may achieve optimal results
when loading the implant immediately” {CLINICAL SKILLS}
“A high degree of primary implant stability (high value of
insertion torque) seems to be one of the prerequisites for a
successful immediate/early loading procedure.” {PRIMARY
STABILITY}
Loading – Immediate Vs Delayed
Screw Vs Cemented….

In the early era of osseointegration most prostheses were screw-
retained as the long-term predictability of implants, was
questionable.
But once it became evident that implants, once osseointegrated,
maintained stability within bone – it reduced the emphasis on
retrievability of prostheses.
Increase in popularity of cement-retained restorations.
Cement-retained restorations - provide aesthetic
advantages over screw-retained restorations and
fewer mechanical complications.
Screw Vs. Cemented Prosthesis

The Future Of Implantology? ? ?

Next Few Years….
• Short Implants- 8mm & Extra Short Implant of 5mm (Renouard, Nissand etal Clin Oral Implant Res 2006)
• Recombinant Proteins - recombinant Bone Morphogenic Protein 2 (rhBMP-2) and Recombinant Platelet Derived Growth Factor (rhPDGF-BB) that potentiate the ability to manage bone deficiencies
From PRF to Stem Cells…just a step away..
Now we have seen the Positives lets look at some Negatives…
We have today close to 600 different implant systems
produced by at least 146 different manufacturers
located in all corners of the globe.
Every year at least 27 new implant companies surface
in the market.•
So How Many Implant Systems are there after 30 years ? ? ?
FDI Science Committee was asked to investigate the issue and the findings were
rather alarming (Jokstad et al. 2003).
Not only did the quantitative issue cause concern, but also the QUALITATIVE
ASPECTS - many manufacturers did not appear to follow international standards for
manufacturing their products.
How Effective are these Different Implant Systems ? ? ?
Were these new implants clinically documented ? ? ?
• NO, according to Albrektsson and Sennerby (1991);
• NO, according to the American Dental Association (ADA 1996);
• NO, according to Eckert and colleagues (1997);
So who, if anyone has been doing anything about this?
• None- according to the best of my knowledge.
• And I leave it to this esteemed audience to think over it.
• And I urge those who can- to do something about this.

Do think it over….

After this 33 years journey of implantology …we are still to taste the
nectar fully..

Change Is
Mandatory…
Adaptation Is Optional
My Conclusion…..
WHEN IT COMES TO DOING IMPLANTS….
Thank You
For all further doubts, queries and general advice
Mail me- [email protected] - facebook.com/gputtuTwitter - @ganeshputtu Google Plus - +GaneshPuttuCall/Watsapp - +91 8438295269