draft - university of texas system · web viewnote to the evaluators: this project was conducted...
TRANSCRIPT
Overview: Cheryl to help with this 1) where the work was completed: The Ambulatory Treatment Center (outpatient), Surgical and Medical ICUs (inpatient). These were the pilot areas to act as ‘beachhead’ for designing a sustainable Hand Hygiene (HH) program throughout the institution.
2) the reason the change was needed: It is widely accepted that proper Hand Hygiene (HH) is vital for preventing nosocomial infection, yet compliance rates remain low and capturing its data is difficult.
The existing method of monitoring HH was conducted by Infection Control which placed them in a policing mode instead of a reporting mode. Nursing’s perception of their HH compliance didn’t match Infection Control’s data, thus was suspicious of the reported findings.
Data collection time consuming, not consistently representative in terms of time coverage or number of observations.
House wide compliance was unsatisfactory and the risk of patient infection too high.
The aggregate HH compliance percentage took a long time to generate did not lead to targeted reporting for corrective/congratulatory feedback.
A task force was assembled to design a sustainable Hand Hygiene program. The first step was a brainstorming session with 45 attendees, spanning 18 departments. After the event 6 sub-teams were enlisted to take the generated ideas and problems from brainstorming event and convert them into solutions.
3) what faculty/staff/patient groups were involved: The brainstorming session had 45 attendees and spanning 18 departments. After the event 6 subteams were enlisted to take the generated ideas and problems from brainstorming event and convert them into solutions.
PROJECT NAME: Hand Hygiene ProgramInstitution: M.D. Anderson Cancer CenterPrimary Author: Cheryl Perego, MPH, CICSecondary Author: Duke Rohe, BSProject Category: Patient Safety
Choose most appropriate category: 1) Patient Safety, 2) Patient Centered Care, 3) Timeliness, 4) Efficiency, 5) Effectiveness, 6) CS & E Projects Implemented at a New Site, 7) General Quality Improvements or 8)Sustained CS & E Projects

4) The effort aligned to institutional goals on prevention:
Note to the evaluators: This project was conducted using an unconventional design methodology (called a Solution Session) instead of a typical PDSA problem solving path. It won’t align perfectly with the scoring but it will demonstrate great QI results.
Aim Statement (max points 150): Describe the problem that you sought to address. The aim of the project was to increase Hand Hygiene compliance rates on an outpatient unit which already had compliance and two high acuity inpatient units which reported unacceptable rates. Aim Statement was
Increase the HH compliance rate in the o Ambulatory Treatment Center (ATC) from 92% to 95% complianceo MICU and SICU units from 50% and 57% respectively to an 90%
complianceo This was to be accomplished in each unit within three months of their
implementation (February 2011)Remember these pilot units were beachhead experiments to launch sustainable HH program throughout the institution.
Measures of Success: How did you measure the impact of your proposed change? Success measured by the compliance of observed hand washing in accordance to
Infection Control guidelines. Each unit had an evaluation of their processes and

specific operating definitions were set for HH compliance based on the sterile processes.
o Observations: must be conducted by trained unit staff with sufficient backup the number of observations collected per month needs to be sufficient
to draw statistical inference (approximately 100/month) For a 90% HH compliance rate, 100 observations would provide accuracy of plus or minus 5%, at a 95% confidence level.
would capture department and name of individual observed so targeted feedback (corrective or complimentary) can be provided.
o Reporting: weekly observation counts are generated and fedback to the unit to
promote appropriate sample size for monthly reporting monthly HH compliance percentages are sent the pilot unit managers
as well as to leadership of the various professional roles…RN, RT, MD, Midlevel Providers, PharmDs, Lab etc.)
Use of Quality Tools (max points 250): What quality tools did you use to identify and monitor progress and solve the problem? Provide sample QI tools, such as fishbone diagram or process map. Messes, Problems (Causes) and ideas were generated at 4 hour creative problem
solving session. 190 possible causes/ideas were generated and sorted in 18 categories for design work
o Problems and ideas consolidated into focus areas which were assigned to 6 subteams to design interventions: Communication, Education, Resources, Motivation, Empowerment, Accountability
o Sub Teams took these and designed changes that made sense and had a good business case
o The proposals from each of the subteams were ‘wired’ together as a system of changes needed to achieve the compliance rates on the pilot units
Note to the abstract evaluator: Since this project was not conducted in a problem solving PDSA method, it did not use QI Tools. It used a design method which captures all the known problems/causes in an idea generated event, sets up teams to design changes to mitigate the problem then retrofits the system of changes back into the organization and culture.
Interventions (max points 150 includes points for innovation): What was your overall improvement plan? How did you implement the proposed change? Who was involved in implementing the change? How did you communicate the change to all key stakeholders? What was the timeline for the change? Describe any features you feel were especially innovative. An awareness campaign was conducted to convince staff, physicians etc, that things
are changing regarding HH. The goal is exceptional HH compliance or we have failed!

o Introduction of New signage, kickoff meeting, PowerPoint presentation, new observer method were part of the awareness.
An observer tool was web-based tool created for nursing that:o was easy to collect and log HH findings (under a minute)o stealth to the person being observedo quick and accurate capturing the department and name of the observedo could be accessed at a desktop computer or an I-pad
This is the report from the tool team After reviewing available software, smart phone applications on the market,
and the Joint Commission’s Web-Based Tool, the Hand Hygiene project team worked with MD Anderson’s Clinical Operations Informatics staff to develop a custom web-based Hand Hygiene Collection Tool (HHCT). The HHCT was developed with simplicity and ease-of-use in mind and could be accessed from any internet browser within the institution by Blackberry, iPad, or computer. The HHCT data fields were based on MD Anderson’s Hand Hygiene policy and reporting needs of the clinics and institution. On the two pilot units observers were on trained on proper HH requirements and inputting the observations in the MDACC Hand Hygiene Collection Tool. iPads were purchased for observers to use for collection. After the baseline was established, Infection Control educated all pilot staff on appropriate hand hygiene. The collection of “real” data began after training was completed.
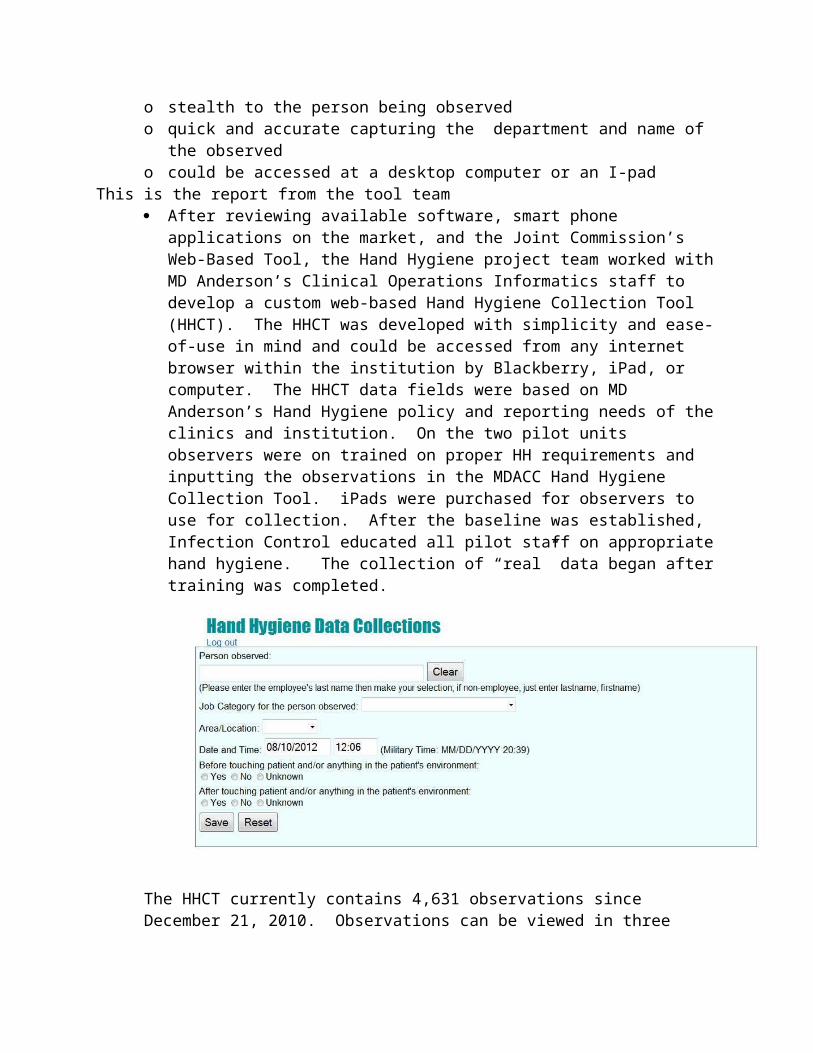
The HHCT currently contains 4,631 observations since December 21, 2010. Observations can be viewed in three different formats including a table format, chart by % compliance, and chart by number of observations.
Custom observer training was essential. Each observer received:o A presentation of the observation process for their unit, an exam of what they
learned and validation of their observations and entryo Training on the use of the web-based collection tool, given instruction on how
to give feedback to caregivers (especially physicians), gently informing them they forgot to wash going in or out of the patient room
Facilities checked gel dispensers volumes were at the beginning of shift and signage on dispensers had Facilities’ extension one them to report if refills were needed
Distribution of a Hand Hygiene Observer newsletter kept the observers aware of their success, and Solution Session team aware of the projects progress
• Physician-to-physician interaction valuable in promoting compliance o Periodic reports compliance by job category Celebrate observers with highest
observation rate
Timeline
Outpatient Pilot – R10 ATC
November 2010
4 iPads purchased for observers to document observations 8 observers trained by Infection Control using PowerPoint presentation Observers shadowed by an ICP to validate observations
December 2010
Baseline compliance data collected R10 ATC staff educated on proper hand hygiene Pilot began – Dec 22, 2010

March 2011
Pilot ended on March 22, 2011
What we learned:
iPads are “triggers” for hand hygiene compliance observers prefer desktop link to institutional database over iPads Limited staff accessibility promotes teamwork and accountability
Inpatient Pilot – ICU
January 2011
8 observers trained by Infection Control using powerpoint presentation Observers shadowed by an ICP to validate observations
February 2011
Baseline compliance data collected All ICU staff educated on proper hand hygiene 3-month pilot began on February 28, 2011 Process Flow Mapping performed by Laura Kaufman
May 2011
3-month pilot ended on May 28, 2011
January 2012
New group of observers trained using The Joint Commission modelo Powerpoint presentationo Written examo Shadowing by an ICP to validate observations
What we learned:
“Open Unit” concept is challenging due to multiple services providing patient care Physician-to-physician interaction valuable in promoting compliance
Results (max points 250): Include all results, using control charts, graphs or tables as appropriate.The HH initiative has been operating with for 15 months with positive results.

Ambulatory Treatment Center increased from a baseline of 92% HH compliance to an average 99% compliance sustained for 15 months. The average monthly number of observations was 106.
MICU increased from a baseline of 54% compliance to 85% compliance (averaged over 15 months). The average monthly number of observations was 60.
SICU increased from a baseline of 50% compliance to 80% compliance (averaged over 15 months) The average monthly number of observations was 24.
Note that the lower ICU rates are rather high for an IC
Compliance by Job Category 2 month Post implementation

Revenue Enhancement /Cost Avoidance / Generalizability (max points 200): What is the revenue enhancement /cost avoidance and/or savings for your project? Did you implement this project in multiple sites after determining that your change was successful? The correlation between hand hygiene compliance and Healthcare associated infections (HAI) has been published in peer-reviewed literature and CDC guidelines. The hand hygiene rates increased from 54% to 85% compliance in MICU and 50% to 80% compliance in SICU.
During the same time period we noted that the rate of overall HAIs in the adult ICUs decreased significantly from 62 HAIs for rate of 7.5 HAI/1000 patient days in FY11(Sep-May) in to 40 HAIs for rate of 5.0/1000 patient days in FY12 (Sept-May) (p-value = 0.035). The attributable cost of overall HAIs per patient has been reported by the CDC with Division of Health Quality Promotion to ranges from $16,300 to $25,900 per HAI in 2007 dollars.
Based on the link between hand hygiene and HAIs, an increase in hand hygiene compliance and decrease in overall ICU HAIs, there is reasonable data to show the avoidance of ~20 HAIs and a cost avoidance of approximately $326,000 during this time period.
Conclusions and Next Steps: Describe your conclusions drawn from this project and any recommendations for future work. How does this project align with organizational goals? Describe, as applicable, how you plan to move ahead with this project. We will expand the training and tool to other units as unit once ‘readiness’
conditions are achieved Focused interview with the observers was collected…approaching physicians about
non compliance is the hardest thing. Initiative expanded to Surgery New group of observers trained using The Joint
Commission model, given exam, validated on observation, preparing for baseline collection.

New units will be added to the program as the ‘readiness conditions’ are in place for successful implementation.