draft geriatric practice change agent meeting judith s. black md, mha medical director, highmark...
TRANSCRIPT
DRAFT
Transitions of CareTransitions of CareA Medicare Advantage A Medicare Advantage QualityBLUE QualityBLUE Pay for Performance ModelPay for Performance Model
Geriatric Practice Change Agent MeetingGeriatric Practice Change Agent Meeting
Judith S. Black MD, MHAJudith S. Black MD, MHA
Medical Director, Highmark Senior ProductsMedical Director, Highmark Senior Products
September 27, 2007September 27, 2007

2
AgendaAgenda
•Rationale for the ProgramRationale for the Program
•Overview of the ProgramOverview of the Program
•Program Outcomes to DateProgram Outcomes to Date
• Lessons LearnedLessons Learned
3
Transitions of Care - Definition and RationaleTransitions of Care - Definition and Rationale
• Closely managing patient movement from one level of care to Closely managing patient movement from one level of care to another accomplishes the following:another accomplishes the following:
• Reduces fragmentationReduces fragmentation
• Improves patient satisfactionImproves patient satisfaction
• Results in a reduction in readmissionsResults in a reduction in readmissions
• Ultimately impacts care costsUltimately impacts care costs
• Information related to advance care planning more Information related to advance care planning more consistently communicated to receiving facilityconsistently communicated to receiving facility
• Health plan moved from Per Diem to CaseHealth plan moved from Per Diem to Case Rate in 2005.Rate in 2005.
A set of actions designed to ensure the coordination of care as patients transfer between settings. Transitional care encompasses both the sending and the receiving aspects of the transfer and includes preparation of the patient and family, transfer of information, coordination among practitioners.

4
Variation in Care - Hospital Readmit Variation in Care - Hospital Readmit AnalysisAnalysis
Discharge DRG Weight
Total Readmission Rate
Hospital A 1.16 13.55%
Hospital B 1.23 13.84%
All Acute Hospitals 1.36 14.23%
The above 25 acute care facilities account for 85% of hospital admissions
Readmission Rates for the Top 25 Facilit ies by Acute Admissions
0%
5%
10%
15%
20%
5
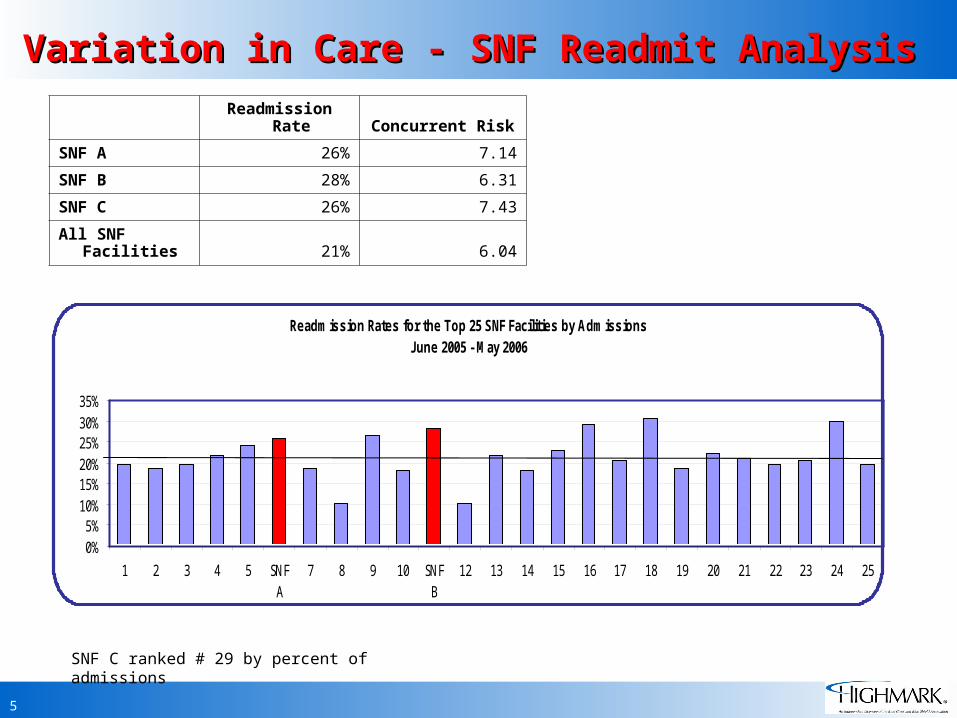
Variation in Care - SNF Readmit AnalysisVariation in Care - SNF Readmit Analysis
Readmission Rate Concurrent Risk
SNF A 26% 7.14
SNF B 28% 6.31
SNF C 26% 7.43
All SNF Facilities 21% 6.04
SNF C ranked # 29 by percent of admissions
Readmission Rates for the Top 25 SNF Facilities by AdmissionsJune 2005 - May 2006
0%5%
10%15%20%25%30%35%
1 2 3 4 5 SNFA
7 8 9 10 SNFB
12 13 14 15 16 17 18 19 20 21 22 23 24 25
6
Highmark Initiative: Highmark Initiative: QualityBLUE Transitions of Care Program QualityBLUE Transitions of Care Program
• Focused Initiative: Three-year SecurityBlue Medicare Focused Initiative: Three-year SecurityBlue Medicare Advantage (MA) Pilot StudyAdvantage (MA) Pilot Study
• Quality Indicator: Transitions of CareQuality Indicator: Transitions of Care
– Involve hospitals in year one. Focus on developing “best Involve hospitals in year one. Focus on developing “best practices” standard for coordination of discharge, i.e., practices” standard for coordination of discharge, i.e., levels of transitions.levels of transitions.
– In year two of the program select skilled nursing facilities In year two of the program select skilled nursing facilities will be asked to participate. Focus on care coordination will be asked to participate. Focus on care coordination between the SNF and the hospital or alternate sites.between the SNF and the hospital or alternate sites.
7
Facility Selection and IncentiveFacility Selection and Incentive
• Volume - top readmit Volume - top readmit rates rates
• Hospital/SNF Hospital/SNF relationshipsrelationships
• Geographic locationGeographic location
• Willingness to work Willingness to work with health plan.with health plan.
• 3 to 5% of SNF payment3 to 5% of SNF payment
• 2.4% of hospital 2.4% of hospital paymentpayment
• Amount payout equal Amount payout equal projected cost savings. projected cost savings.

8
Payment Methodology
Five Parameters
Program AdministrationProgram Administration 5% 5%Planning Planning 35%35%Action Action 40%40%Measurement Measurement
10%10%Results Results 10%10%
90-100% Maximum Level
80-89% Threshold Level
70-79% Minimum Level
< 70% No Pay-for-Performance Payment
9
1st Q04
2ndQ04
3rdQ04
4thQ04
1stQ05
2ndQ05
3rdQ05
4thQ05
1stQ 06
2ndQ06
3rdQ06
4thQ06
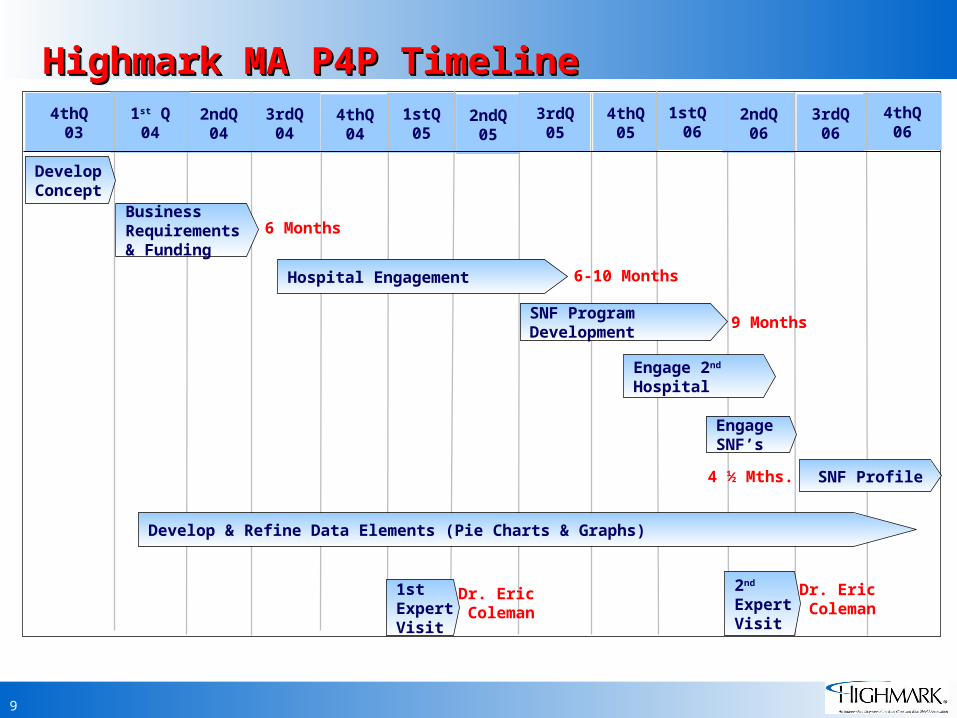
BusinessRequirements& Funding
SNF Profile
4thQ 03
4 ½ Mths.
1stExpertVisit
6-10 Months
EngageSNF’s
Hospital Engagement
2nd
Expert Visit
Highmark MA P4P TimelineHighmark MA P4P TimelineHighmark MA P4P TimelineHighmark MA P4P Timeline
Develop & Refine Data Elements (Pie Charts & Graphs)
SNF ProgramDevelopment
Engage 2nd Hospital
DevelopConcept
Dr. Eric Coleman
Dr. Eric Coleman
9 Months
6 Months

10
Initiative Goals:Initiative Goals:
• To improve the quality of care for the geriatric To improve the quality of care for the geriatric patientpatient
• To develop appropriate reimbursement To develop appropriate reimbursement methodology to align reimbursement between methodology to align reimbursement between health plans and institutionshealth plans and institutions
• To identify indicators and measurement To identify indicators and measurement techniques that focus on “transitions of care” techniques that focus on “transitions of care” issues for the hospitals in year oneissues for the hospitals in year one
• To develop methods for ongoing monitoring of To develop methods for ongoing monitoring of quality indicators. quality indicators.
11
Hospital/SNF Performance Strategies:Hospital/SNF Performance Strategies:
• Reduce readmissions from skilled nursing facilitiesReduce readmissions from skilled nursing facilities
• Reduce admissions for patients transitioned home Reduce admissions for patients transitioned home with diagnoses of heart failure, COPD, or with diagnoses of heart failure, COPD, or pneumoniapneumonia
• Prevent or reduce medication errorsPrevent or reduce medication errors
• Facilitate effective communication sharing Facilitate effective communication sharing between facilities and enhance accountability of between facilities and enhance accountability of patient transferspatient transfers
• Improve patient satisfaction by ensuring their Improve patient satisfaction by ensuring their preferences be passed from one setting to the preferences be passed from one setting to the nextnext
• Ensure patient’s ability to manage their health Ensure patient’s ability to manage their health care condition.care condition.
12
Hospital/SNF Performance Strategies:Hospital/SNF Performance Strategies:
• The Care Transitions Measure ToolThe Care Transitions Measure Tool – To assess caregiver perception (satisfaction) of the To assess caregiver perception (satisfaction) of the
transition process and to assess overall quality of transition process and to assess overall quality of care transitions.care transitions.
• The UCHSC Care Transition MeasureThe UCHSC Care Transition Measure– The hospital staff took my preferences into account in The hospital staff took my preferences into account in
deciding what my health care needs would be after deciding what my health care needs would be after dischargedischarge
– Before I left the hospital, the people that were going Before I left the hospital, the people that were going to help me when I got home clearly understood what to help me when I got home clearly understood what my health care needs weremy health care needs were
– Before I left the hospital, I had a phone number I Before I left the hospital, I had a phone number I could call to get answers to my questions.could call to get answers to my questions.

13
Hospitals Outcomes to DateHospitals Outcomes to Date
• A work group was established to implement this A work group was established to implement this quality initiative and;quality initiative and;
– Evaluated the current transfer/discharge processEvaluated the current transfer/discharge process
– Developed a written model for the Care Developed a written model for the Care Transitions ProgramTransitions Program
– Standardized the transfer process to skilled Standardized the transfer process to skilled nursing facilitiesnursing facilities
– Developed essential data elements to be Developed essential data elements to be conveyed to the receiving practitionerconveyed to the receiving practitioner
– Enhanced discharge instructions for patients Enhanced discharge instructions for patients returning home including a system to establish returning home including a system to establish follow up contact.follow up contact.
14
Hospitals Outcomes to DateHospitals Outcomes to Date
– Developed a medication reconciliation toolDeveloped a medication reconciliation tool
– Developed an advance care planning process Developed an advance care planning process & implemented the POLST& implemented the POLST
– Designed educational programs to inform Designed educational programs to inform staff members of treatment/procedural staff members of treatment/procedural changeschanges
– Established electronic connectivityEstablished electronic connectivity
– Rapid Response Team for 600 bed SNFRapid Response Team for 600 bed SNF
– Established Subcommittee with ED and SNFEstablished Subcommittee with ED and SNF
– Developed tools, audits, and surveys to Developed tools, audits, and surveys to determine the impact of the program.determine the impact of the program.

15
SNF Outcomes to DateSNF Outcomes to Date
The Skilled Nursing Facilities developed a The Skilled Nursing Facilities developed a workgroup and accomplished the following:workgroup and accomplished the following:
• Implemented a Performance Improvement PlanImplemented a Performance Improvement Plan
• Senior Leadership committed to continuity of Senior Leadership committed to continuity of projectproject
• Upon admission to the Skilled Nursing Facility, Upon admission to the Skilled Nursing Facility, project the resident’s length of stay, establish project the resident’s length of stay, establish needs and goals of the resident and regularly needs and goals of the resident and regularly communicate the resident’s progress toward the communicate the resident’s progress toward the goals with the family or responsible partygoals with the family or responsible party
• Developed plans and begun using CTM and Developed plans and begun using CTM and transfer impact survey.transfer impact survey.
• Established a performance improvement plan and Established a performance improvement plan and timeline for incorporating the POLST.timeline for incorporating the POLST.

16
2007 Program Administration
Reimburse-Ment
Determined
ProgramManual & Ongoing
Mtgs.
Mid-YearReview
Year-EndReview
Scoring
ResultsDistributed
17
Program Year 2007-2008
• Hospitals will continue transition of care initiatives with goal to decrease readmissions
• Continue to refine the SNF measures. Less emphasis on Planning & Action & greater focus on Measurement & Results
• Heritage Valley Skilled Nursing Facilities to begin program (The Villa, Friendship Ridge, Beaver
Elder Care).

18
SNF Outcomes to DateSNF Outcomes to Date
• Implemented a mutually agreed upon format for Implemented a mutually agreed upon format for transfer informationtransfer information
• Worked collaboratively with the hospital to utilize Worked collaboratively with the hospital to utilize computer connectivity to enhance transfer computer connectivity to enhance transfer communication.communication.
• Working in a Collaborative on Medication Working in a Collaborative on Medication Reconciliation.Reconciliation.
• Participated in regular conference calls and Participated in regular conference calls and meetings with hospital and health plan.meetings with hospital and health plan.

19
What Were the Challenges?What Were the Challenges?
• Selling the concept to Senior ManagementSelling the concept to Senior Management
• Establishing an effective internal Highmark team Establishing an effective internal Highmark team with commitment to new programwith commitment to new program
• Ongoing funding with a lag in financial dataOngoing funding with a lag in financial data
• Resources with the expansion of the Hospital Resources with the expansion of the Hospital QualityBLUE Program. QualityBLUE Program.
20
What Worked Well?What Worked Well?
• EngagementEngagement
– Bringing in outside expert to help sell the Bringing in outside expert to help sell the programprogram
– Providing comparison data and toolsProviding comparison data and tools
– Sharing experiencesSharing experiences
• ImplementationImplementation
– Team experience with a commercial hospital Team experience with a commercial hospital QualityBLUE programQualityBLUE program
– Detailed scoring gridDetailed scoring grid
– Team work with frequent contact.Team work with frequent contact.
• Relationship buildingRelationship building
– Hospital/SNF working together.Hospital/SNF working together.
21
Lessons Lessons LearnedLearned
• Develop a detailed three year project timelineDevelop a detailed three year project timeline
• Don’t underestimate the engagement timeDon’t underestimate the engagement time
• Collect data in auditable format.Collect data in auditable format.
22
Key Success FactorsKey Success Factors
• Facility ChampionFacility Champion
• Effective TeamEffective Team
• Willingness to share toolsWillingness to share tools
• Leveraging off of other programsLeveraging off of other programs
• Striving for a win/win programStriving for a win/win program
– Rewarding for process measures not just Rewarding for process measures not just bottom line.bottom line.
23
Sustaining the Program

24
Tools/ReferencesTools/References
• www.caretransition.org
• www.polst.org
• “One Patient, Many Places: Managing Health Care Transitions,” a report from the HMO Workgroup on Care Management.
• Coleman, Eric A. et. al. “The Care Transitions Intervention – Results of a Randomized Controlled Trial.” Arch Intern Med. 2006; 166: 1822-1828.
• Davis, M. Neila, et al. “Improving Transition and Communication Between Acute Care and Long-Term Care: A System for Better Continuity of Care.” Annals of Long-Term Care. May 2005; Vol. 13 No. 5: 25-32.
• Coleman, Eric A., et al. “Preparing Patients and Caregivers to Participate in Care Delivered Across Settings: The Care Transitions Intervention.” JAGS 52: 1817-1825, 2004.
• Coleman, Eric A., Berenson, Robert A. “Lost in Transition: Challenges and Opportunities for Improving the Quality of Transitional Care.” Ann Intern Med. 2004; 140: 533-536.