dr. tamer bedair lecturer of medical microbiology and immunology
TRANSCRIPT

Streptococci Dr. Tamer BedairLecturer of Medical
Microbiology and Immunology

Contents :1. Character of Streptococci2. Classification of Streptococci3. Strept. pyogenes a. virulence factors and pathogenesis b.diseases c. lab. Daignosis d. post Streptococcal sequelae or
complication e. treatment and prevention
4. Strept. pneumoniae (pneumococci) 5. Viridans Strept.6. Strept. agalactia5. Strept. faecalis (enterococci)

Causes of tonsilitis or pharyngitis
Group A hemolytic strept. is the most common cause especially in children
Viral causes (most common in adults) as rhinoviruses, influenza virus, parainfluenza, adenovirus, EBV, HSV…
Characters of StreptococciMorphology: Gram positive cocciChains or pairsPathogenis strains usually capsulatedNon motile and Non spore formingCulture character: Fastidious and grow on blood agar except strept
faecalis which is not fastidious and can grow on nutrient agar
All Strept. need 0.03% CO2 except Strept. pneumoniae which need CO2 5—10%
Biocemical reaction: All Streptococci are Catalase negative
(Staphylococci are catalase positive)

Classification Oxygen requirements
Anaerobic (Peptostreptococcus)Aerobic or facultative anaerobic
(Streptococcus)Serology (Lanciefield Classification)
Hemolysis on Blood Agar (BA)

I-Classification of Streptococci Based on Hemolysis on Blood Agar
Hemolysis on BA– -hemolysis
Partial hemolysisGreen discoloration around the coloniese.g. non-groupable streptococci (S. pneumoniae & S. viridans)
– -hemolysisComplete hemolysisClear zone of hemolysis around the coloniese.g. Group A & B (S. pyogenes & S. agalactiae)
– -hemolysisNo lysise.g. Group D (Enterococcus spp)

Hemolysis on Blood agar
-hemolysis
-hemolysis
-hemolysis

II-Serology: Lanciefield Classification
Streptococci classified into many groups from A to U
Classification based on C- carbohydrate antigen of cell wallGroupable streptococci
A, B and D (more frequent) C, G and F (Less frequent)
Non-groupable streptococci S. pneumoniae (pneumonia) viridans streptococci
e.g. S. mutans

Group A streptococci = Strept.pyogenesGroup A streptococcal infections affect all ages but peak incidence at 5-15 years of age
The most common infection caused by Strept. pyoenes is pharyngitis and tonsillitis especially in children
Pathogenesis and Virulence FactorsStructural components
M protein, which interferes with opsonization and phagocytosis
Hyaluronic acid capsule, which interferes with and phagocytosis
EnzymesStreptokinasesDeoxynucleases C5a peptidase
Eythrogenic toxins Produced by lysogenic (temperate) phage and causes rash of scarlet fever & associated with a toxic shock-like syndrome
StreptolysinsStreptolysin O lyse red blood cells, white blood
cells, and plateletsStreptolysin S
facilitate the spread of streptococci through tissues

Diseases caused by Strept. pyogenesA)Supppurative infections
B) Toxogenic diseases
C) Post streptococcal sequelae
Suppurative (pus forming)
Pharyngitis & acute follicular tonsilitis
Otitis media Bronchopneumonia Bacteremia and septicemiaMeningitis Skin infection, Impetigo, Pyoderma, erysipelas and cellulitis

Cellulitis
Impetigo

B) Toxogenic dise1- toxic shock like syndrome - similar in pathogenesis and manifestation to staphylococcal toxic shock syndrome .
2-Scarlet fever (erythrogenic toxin)
Usually affects children ,characterized by fever, skin rash & stomatitis (Strawberry tongue) .
The skin rash is due to direct effect of the erythrogenic toxin on the skin .

Lab. diagnosis1. sample: according to clinical disease - tonsilitis, pharyngitis and scarlet
fever: throat swab - erysipelas, and bacteremia: blood
(blood culture)2. Direct microscopic examination by
Gram stain: G. +ve cocci, capsulated in long chain
3. culture: on BA, at 37 C →β hemolytic colonies
4. Colonies identification: a. film stained by G. stain:
b. biochemical reactions: catalase -ve & bacitracin sensitive


Diagnosis of scarlet fever By throat swab: processed as before ……+
5-Schultz Charlton reaction (rapid diagnosis ):-Toxin anti toxin neutralization test-Injection of antierythrogenic toxin in the
rash → disappearance of the rash within 6-12 hours , due to neutralization of the toxin with specific antitoxin .
6. Dick test : Toxin anti toxin neutralization test Used to assess susceptibility of individual
and detect immunity to scarlet fever

C) Post streptococcal sequelaeNon suppurative complication which follow
strept. pyogenes infection by 1-3 weeksAffect mainly in children between 5 – 15
yearsOccur following pharyngitis or skin infection
(nephrogenic strains)No bacteria present in pharynx at time of
occurance of the complicationsThese complication includes 1. rheumatic pancarditis (rheumatic
fever) with subsequent damage in heart valves
2. glomerulonephritis 3. migratory polyarthritis
C) Post streptococcal sequelaePathogenesis: 1. similarity and cross reactivity
(molecular mimicry): M protein of Strept pyogenes is similar with
heart myosin glycoprtein so antibodies against M protein will cross react with heart myosin glycoprtein (autoimmunity)
2. Immune comples disease (type III hypersensitivity):
Due to prolonged antigenemia in vivo, antigen antibody complexes will be formed into the circulation and precipitate on basement membrane of renal glomeruli ten damage of renal glomeruli occur by type III hypersensitivity

C) Post streptococcal sequelaeDiagnosis: Jones criteria……….Lab. Diagnosis:
a-Non specific tests:
C- reactive protein High ESR
b-Specific tests : by detection of an increase in antibody titer to
at least one of the streptococcal antigens including antistreptolysin O (ASO) which is most widely used ,anti-DNase , antihyaluronidase& antistreptok
ASOaim: to determine the titre of Ab against
Sterptolysin Otype: done in tube or on slide (passive
agglutination)interpretation:
titre = highest dilution of serum with no haemolysis
titre expressed in Todd’s unitsignificant titre = 200 or more Todd’s unit

Treatment and prevention:No vaccine is available to combat S.
pyogens infections.The antibiotic of choice is penicillin
(inhibit cell wall peptidoglycan synthesis) or erythromycin (inhibit 50S of ribosome)
Long acting penicillin can be used to prevent recurrent pharyngitis and its immune-mediated sequelae.

Group B Streptococci (Stretococcus agalactiae)
Flora of vagina Morpholog and culture character : similar
with Strept. pyogenesBiochemical reaction: catalase -ve &
bacitracin resistant& CAMP test +veDiseases: Neonatal septicemia , pneumonia
and meningitis Prevention: IV ampicillin to pregnant
mothers who have Group B in vagina.Diagnosis:……….

Strept. pneumoniaeMorphology: G. +ve cocci, capsulated, in
pairs, non motile and non spore forming.Culture character: grow on blood agar with
CO2 5—10% (capnophilic) →αHBiochemical reactions: catalase –ve, optochain
sensitive, bile soluble, ferment inulineVirulence factors: - main virulence is due to polysaccharide capsule →
antiphagocytic

Strept. pneumoniae- According to polysaccharide capsule → 80
serotypes- Humans infected by pathogenic 23 strains - Quelling reaction: when specific Ab against
capsule bind with capsule → capsular swellingDiseases: 1. lobar pneumonia2. Otitis media 3. Bacteremia and septicemia 4 Septic meningitis

Strept. pneumoniaeLab. Diagnosis:sample: sputum, blood2. Direct microscopic examination by Gram
stain: G. +ve cocci, capsulated in pairs (dipolococci)
3. culture: on BA, at 37 C →α hemolytic colonies 4. Colonies identification: a. film stained by G. stain:
b. biochemical reactions: catalase -ve & optocain sensitive &……….
5. Quelling reaction:………….

Strept. pneumoniaeTreatment: penicillin or β lactam antibiotic
but if resistance suspected vancomycin can be used
Prevention: Polyvalent polysaccharide capsule Ag from
most pathogenic 23 strains which infect human → given to to children & elderly & post-spleenectomy

Viridans Strept.Bacteria flora of oral cavityMorphology, culture characters: similar to
pneumococci but not capsulatedBioch. Reactions: catalase –ve, optochain
resistant, bile insoluble, ferment rafinose Diseases: dental plaques, dental caries and
infective endocarditis (on tooth extraction in patients with heart diseas).
Prevention: any patients with tooth extraction should take prophylactic antibiotics before and after tooth extraction.

Group D StreptococciDivided into
Enterococci (present in the intestine as flora)
Non enterococci not present in the intestine

Enterococcus faecalisFlora of intestine → inducator for faecal pollution of
waterMorphology: G+ve cocci in short chain, non
capsulated, non motile, and non spore forming
Culture character: the only strept. which can grow on nutrient agar & also grow on blood gar (ɣH)
Biochemical reaction: catalase –ve & can grow in 6.5% Na Cl broth
Diseases: UTI & intra abdominal sepsis & wound infections
Diagnosis: ………Resist antibiotics and cause nosocomial
infections
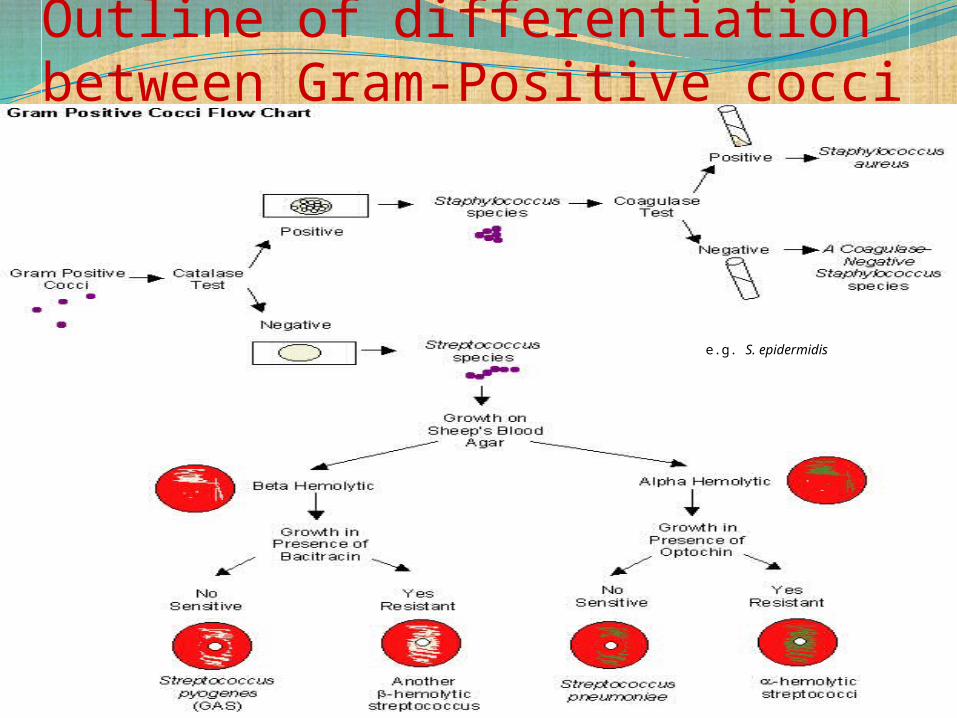
Outline of differentiation between Gram-Positive cocci
e.g. S. epidermidis

Causes of Membrane on the tonsilAcute follicular tonsilitis: Strept.
pyogenes………..Diphtheria: G +ve bacilli, in chinese letter
appearance& cultivated on loffler’s serum or blood agar
Oral thrush: Candida which appear as G +ve yeast & cultivated on Sabouraud’s dextrose agar
Vincent’s angina: B. vencenti (coiled bacteria) & Fusbacterium (anaerobic fusiform G –ve bacilli)
Infectious mononucleosis: EBV which diagnosed by monospot test or Paul Bunnel test

Thanks for your attention