dr surinder singh. what is the concern? head injury (hi) rarely occurs alone 21% require life...
TRANSCRIPT

ANESTHESIA FOR NON-NEUROSURGICAL SURGERY IN HEAD INJURY
Dr Surinder Singh

What is the concern?
Head Injury (HI) rarely occurs alone 21% require life saving surgery for control of
bleeding laprotomies and thoracotomies Only 2.5% patients undergo craniotomies More severe HI; More Non-NS operations Severe HI patients invariably admitted in ICU Risk of further Neurological deterioration
Literature Resources…
Recent Advances in anesthesia & Analgesia 20 1998 Brain Trauma Foundation Guidelines 3rd Ed 2007 Millers 7th Edition 2010 Traumatic Coma Data Bank TCBD Pub med
Evidence level: Grade-III and very limited Grade II
Implications: The concepts apply to adult patients Advisory and subject to change with time Clinical judgment in each case is MOST important All cases MLC documentation is utmost important
Classification of brain damage
Primary brain damage, which is damage that is complete at the time of impact, may include:
Skull fractures Contusions Hematomas/blood clots Lacerations Diffuse axonal injury: damage to nerve
cells in the brain's connecting nerve fibers
Classification...... Secondary brain damage:
Further neurological deterioration of primary injury
Evolves over time spanning hour to days or weeksCauses include:
Brain swelling (Edema) Raised intracranial pressure (ICP) Epilepsy Intracranial infection

Classification of Head injury
Grade Incidence GCS Severe 10% <8 Moderate 10% 8 – 12 Mild 80% 13 – 15 Mild to moderate injury most recover well Some deteriorate due to ICH/ brain edema Diagnosis may be delayed/ masked

Problems due to Non NS surgery
Interruption of: Resuscitaion Monitoring Clinical care Delay in the diagnosis of worsening of
brain damage Delay in institution of treatment Non NS surgery and anesthesia →
Worsening
What are the issues?
More severe the HI; more nonNS trauma More trauma: more operations (Multispeciality)
What is urgent ? Brain or non NS trauma Life saving surgery for controlling major bleeding
is more important than brain Brain is more important in non-vital trauma
What is the priority of surgery? Life saving vascular, laparotomy, thoracotomy
first Stabilization of the patient next CT scan/ neuroradiological imaging next Orthopedic, facio-maxillary and plastic last

How to manage in between?
The transfer, imaging or waiting for surgery
Resuscitation Monitoring Stabilization Prevention of secondary brain injury
ResuscitationA: Tracheal Intubation: Airway 45%have
obstruction Loss of airway reflexes Significant bleeding into the airway Hypoxia - PaO2 < 98mmHg on oxygen Hypercarbia - PaCO2 > 45mmHg Spont. Hyperventilation PaCO2 < 30mmHg Inadequate/Irregular/Abnormal breathing GCS < 8 Seizures Neurological deterioration
(↓ of ≥ 1 points in M component of GCS Before Inter-facility or Inter-hospital patient transfer Bilateral fractured mandible
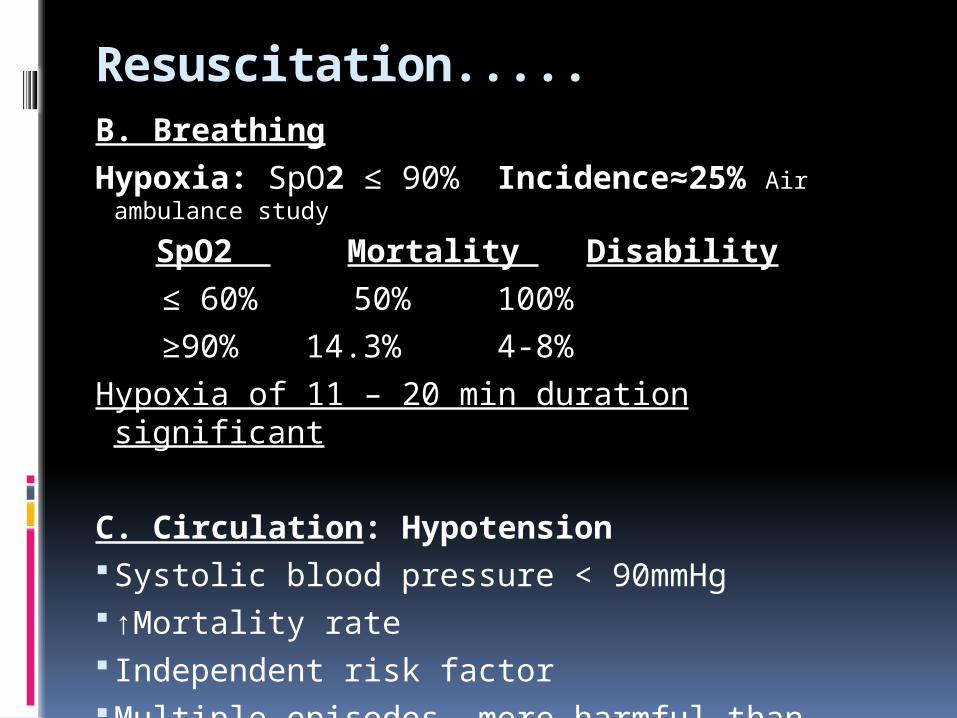
Resuscitation.....B. Breathing
Hypoxia: SpO2 ≤ 90% Incidence≈25% Air ambulance study
SpO2 Mortality Disability
≤ 60% 50% 100%
≥90% 14.3% 4-8%
Hypoxia of 11 – 20 min duration significant
C. Circulation: Hypotension Systolic blood pressure < 90mmHg↑Mortality rate Independent risk factor Multiple episodes more harmful than single Duration ∞ Mortality and disability
Resuscitation.... Hypotension ↓ CPP More damaging in the presence of ↑ICP TCDB: Early hypotension seen in 14% In adults not due to head lacerations BUT Due to abdominal/ thoracic bleeding Late hypotension in 32% (over hours) Due to fractures/ non-visceral trauma
Pediatric patients: Scalp bleeding alone may cause hypotension

Resuscitation..... Impact of Hypotension: The only insult in 24% cases Vegetative
survival or Death
Hypotension Mortality
None 17%
Early 47%
Late 66%
Early and late 77%
Resuscitation.....Comprises of: Prevention of Hypoxemia Prevention of Hypotension Prevention/ control of bleedingAll before CT head/ Neuro-radiological imaging
Diagnosis: Abdominal/ Thoracic CT Scan& USG time consuming Diagnostic limitations& require expertise DPL: Diagnostic peritoneal lavage Quick, reliable, bedside ≥ 10 ml blood or ≥500 WBCs Or ≥1,00,000 RBC/cumm or fecal/ enetric/vegetable material is diagnostic
Anesthetic Management:General anesthesia:Pre operative Management:
Severe HI may already be intubated: Manage oxgenation and ventilation
Investigations: Blood biochem, Gp/ CM and ABG
X-ray chest & Neck should be obtained
Monitoring: ECG, NIBP, SpO2 EtCO2 and Temperature
2 large bore iv lines
In severe HI/ unstable patients
CVP: Antecubital or femoral vein
Arterial pressure

Anesthetic Management...General anesthesia:
Check hemodynamic status
Be prepared for difficult intubation
Assume C Spine Injury – Inline intubation
Fiberoptic intubation
Cricothyroidotmy/ Tracheostomy
RSI is the best:
Anesthetic Agents& Doses: based on hemodynamics
Too much anesthetic – Hypotension and ↓CPP
Too little anesthetic – ↑ICP → ↓CPP
Inappropriate use of ketamine – ↑ICP → ↓CPP
Unconscious patients to require A&A, NM Blockade
Anesthetic Management...General Anesthesia Suxa or Rocuronium no difference if adequate depth Prefer suxa if difficult intubation Control hemodynamic response Safe: lignocaine, esmolol, metoprolol Unsafe: NTG, Sod Nitroprusside ↑ CBF, ↑ICP, ↓MAP →
↓CPP
Cushing’s Triad in raised ICP may mask: (HTN,Brady, irregular breath)
Hypovolaemia& severe dehydration e.g. an patient with apparently normal SBP 120-130, HR 70-80
might collapse with thiopentone or propofol
Check input/ output and the doses of diuretics

Anesthetic Management...
General Anesthesia…. Maintenance: IAA Isoflurane at 1MAC is best N2O ↑ CBF but analgesia ↓sympathetic
response TIVA : EVIDENCE IS LACKING however may be Useful if intra or inter-hospital transfer is planned Generous doses of NMBA Too little relaxation ↑ICP Pancuronium or atracurium may ↑CBF ↑ ICP Vecuronium may be better Avoid and prevent hypotension at all stages

Anesthetic Management...
Positioning for surgery:
Slight head-up table top
with head neutral relative to the body
Do not use very tight tapes for securing tracheal tubes
Ensure un-impeded venous drainage from the brain
Reversal or ICU: Severe head injury → NeuroICU/ ICUMild to moderate HI → Assess and reversePrevent extubation responseMonitor and observe in Recovery/ ICU/HDUPrevent hypoxia, hypoventilation

Anesthetic Management...Ventilation: Normocapnea or PaCO2 of 34 – 38mmHg Brief hyperventilation to control ICP >30 PaCO2 ≤ 26mmHg ) ↓↓ CBF, ↑es No. and Intensity of oligemic
areas ↓es SjVO 2 ≤ 56% usually due to ↓ perfusion due to VC,
Hypotension and Hypoxia Is associated with Poor Outcome
Dsaturation Mortality/ Vegetative state No episode 55%
01 episode 74% Multiple episodes 90%
↑ SjVO2 ≥ 75% also assoc. with Poor Outcome (Hyperperfusion or Infarction)
Arterial to jugular vein O2 difference (ADJO2)or Cerebral Oxygen Extraction and has better co-relation
Anesthetic Management...
Fluid Therapy: Objectives Optimal blood pressure Plasma electrolyte homeostasis Normo glycemia Plasma osmolality Crystalloids: Hypotonic: Avoid RL, D5, N/2 saline, Isolyte P NS recommended Hyperglycemia to be avoided Colloids: Hydroxyehtyl starch Not Used Gelatins& albumin have been found safe

Brain Decongestion Therapy:Hypertonic Fluids Mannitol 20% Saline 3% and 7.5% Evidence strongly favours use of Mannitol Not so convincing for SalineDiuretics: Not really justified in severe HI with polytraumaMonitor volume status& electrolytes with all aboveSteroids: Onset of action in HI 72-96 hrs CRASH trial 1008 patients: 3% ↑in Mortality rate ↓ Immunity, ↑ Risk of GI Bleed Best used in tumor/ infective pathology like TBM
Temperature control Prevent hyperthermia at all costs 34-32oC has shown better results in ICU Interferes with reversal, bleeding and
assessment Not recommended below 32oC Post-op shivering↑oxygen demand, ↑ICP,
↓Oxygen availability
Neurological Monitoring:
During General Anesthesia: Signs of ↑ ICP Hypertension and bradycardia remains intact Pupillary signs: Remain intact Size > 4mm significant Asymmetry >3mm significant Less than 50% have hematoma Less than two thirds only have ipsilateral ICH
Blind Burr holes can’t be justified

Ac deterioration/Herniation
Mannitol 0.25g/kg, hyperventilation To buy time for investigate and intervene
Bilateral fixed pupils: 25% evntually survive with moderate
disability Younger patients Extradural hematoma Evacuation of ICH in < 3hours of dilatation

Extent and Duration of surgery
Absolute minimum Repair major vascular injuries to control
bleeding Orthopedic surgery may not be urgent Non-urgent surgery not allowed with
Thoracotomy/laprotomy Splinting for stabilization of #s to be
permitted

Further management
Monitoring, sedation& ventilation to continue: During
CT Scan for HI and neurosurgical interventions Transfer to Neuro-ICU/ ICU/ HDU. Inter-speciality transfer Inter-hospital transfer
After sustained stabilization decide future course:
Whether ICU care and weaning Or non-neurosurgical interventions
Mild to Moderate Head Injury:
GCS 8- 15Immediate Priority for life saving surgery
laprotomy/ thoracotomy/ Bleeding control surgery:
Orthopedic, faciomaxillary or plastic procedures: Usually to be done in first 72 hours Does surgery and anesthesia impose
additional risk? Do the anesthesia techniques differ in
hazards?
Majority of patients make good recovery

Mild to Moderate Head Injury
Small minority deteriorates to develop ICH, brain edema or both
Risk Factors: A review of 183 deteriorated patients: Altered conscious state Headache Vomiting Focal deficit Skull fracture
Deterioration reported even after 5 weeks post injury

Minor to Moderate HI...
CT Scan 20% have some abnormalities 75% have failed auto-regulation of CBF for >
10 days* Normal CT Scan: Unlikely to deteriorate but
with DUE PRECAUTIONS Prevention of hypo& hypertension Prevention of Hypoxia Prevention of hypo& hypercarbia
Anesthetic likely to be implicated for deterioration
* This study was conducted at 10 days post injury

Anesthesia for mild& moderate HI
General Anesthesia: Same as discussed for Severe Head Injury
Epidural anesthesia: 5 – 10ml of epidural NS ↑ ICP even after 1wk Compression of dural sac is implicated Proved in animal model Extremely slow injection with smallest volume
Regional anesthesia...
Spinal anesthesia: Concern for raised ICP Std teaching risk of tentorial herniation But diagnostic lumbar punctures in
meningitis& SAH Lumbar CSF drainage for ICP control in
pediatrics The patient with normal CT Scan is unlikely to
be at risk Do not presume safe without a CT scan The fine needles and small LA volumes offer
advantage

Regional anesthesia....
IVRA: Period just after the release of tourniquette is
critical Lower limbs have more profound impact Several reports of ICP worsening on deflation Quite often complicated by hypotension Profound bleeding may further worsen
hypotension
Regional anestheisa....
Nerve Blocks: Seemingly safer than ESA Toxic doses of LA worsen neurological status Anxiety, pain and vasoconstrictors ↑BP ↑ICP Advantage of post operative analgesia
Post-operative Analgesia:
NSAIDs: May aggravate bleeding/hematoma
Paracetamol: May be safer option
Systemic opioids:→ Respiratory depression
PCA: → ?? Cognitive state
Nerve blocks: Useful but limited duration, limited sites
Limited thoracic epidural: Upper abdomen, rib fractures
Rib fracutres: Ventilation, epidural, paravertebral, intercostal catheter
Therapeutic Targets: ICU PaO2 > 13kPa (98 – 150mmHg ) PaCO2 of 4.5 – 5.0kPa (34- 38mmHg) A lower PaCO2 (30mmHg) for ↑ ICT) SBP > 90mmHg MAP " 80 mmHg (in the absence of ICP
monitoring) Glucose 4 – 8 mmol/l Temperature < 37°C

Therapeutic Targets: ICU
ICP < 20mmHg (Actionable ICP limits 20 – 25 mmHg)
CPP 50 – 70mmHg SJvO2/ SJO2 55- 75% PBtO2/ PBr O2/PBO2 > 10-15mmhg Microdialysis for BS, Glutamate Full calorie replacement within 7 days
NG tube, Jejunal tub/ jeunostomy Or TPN

. .
. .Thanks for patient listening

ICP and other Concepts
40 – 50 mmHg survived wuth disability
5 had 75mmHg died of herniation
Optimal CPP not defined 45- 60mmHg
73 mmHg was associated with abnormal markers
Lund concept: Normovaemia, Hct, PP,Glucose,po2,pco2
Hyperglycemia>15mmol
Age:
Classification: Class III Study Conclusions: GOS Age 1 0-20 (N=62) 32% 21-40 (N=62) 48 41-60 (N=53) 59 ≥ 60 (N=27) 78