dr. sharma 2
TRANSCRIPT

Niraj Sharma, MD

ATRIAL FIBRILLATIONRATE/AAD/ABLATIONNiraj Sharma MD
4rd Atrial Fibrillation Summit
May 30, 2015
48 year old with symptomatic pAF, occurring 2-3 times a month. Average duration 3 hours. No other medical problems. To maintain normal rhythm, you would now:
1. Refer to Cardiology2. If you are Cardiology refer to EP3. Start Flecanide4. Start Flecanide & Metoprolol5. Recommend ablation6. Evaluate clinically as well as by
EKG/Echo ± TTM for structural heart disease prior to initiation of AAD
7. Start amiodarone

Priorities in the Management of A FIBThe Patient Care Pathway
Rhythm Control
Prevention of Thromboembolism
Rate Control

Pillars of AF management
Rate control:AVN blockersAVN ablation & Pacing
Anti-coagulation:0ASA, ASA+ClopidogrelWarfarinNew agents
Rhythm Maintenance: AADAblation

Rate control
Why?
What rate?
Bipolar afib (tachy-brady)

Rate control
Unchecked HR (≥120bpm) leads to TCMP Poor exercise tolerence Affirm adequate control was defined as an average heart rate of up
to 80
bpm at rest and either an average rate of up to 100 bpm over at least 18 hours of
ambulatory Holter monitoring with no rate greater than 100% of the maximum age
adjusted predicted exercise heart rate or a maximum heart rate of 110 bpm during
a 6-minute walk test
Race II The potential benefits of strict (resting heart rate 80 bpm,
heart rate 110 bpm during moderate exercise) versus lenient (resting heart rate
110 bpm) rate control

RACE II(Rate Control Efficacy in Permanent AtrialFibrillation)
614 patients with permanent AF treated with a variety of atrioventricular (AV) nodal blocking
agents to control heart rate. Primary endpoints were death from cardiovascular causes,
hospitalization for heart failure, stroke, systemic embolism, bleeding, and life-threatening arrhythmias.
The 3-year estimated cumulative incidence of the primary outcome was 12.9% in the lenient-control group and 14.9% in the strict-control group, with an absolute difference between lenient control and strict control of 2.0 percentage points, HR of 0.84 (90% CI, 0.58 to 1.21; P0.001.
Symptoms were also similar in both groups. All patients included in the study were ambulatory and relatively
young (mean age, 68 years), predominantly male, and may have been healthier and less symptomatic than many patients encountered in clinical practice
The RACE II study shows that lenient-rate control 110 bpm is not inferior to strict-rate control 80 bpm

RACE II TRIAL: LENIENT RATE CONTROL IS NOT INFERIOR TO STRICT RATE CONTROL

Rate control: Rate
2011ACC/AHA/HRS Focused Update Recommendation:
Class III–No Benefit Treatment to achieve strict rate control of heart
rate (80 bpm at rest or 110 bpm during a 6-minute walk) is not beneficial
compared to achieving a resting heart rate 110 bpm in patients with persistent AF who have stable ventricular function (left ventricular ejection fraction 0.40) and no or acceptable symptoms related to the arrhythmia, though uncontrolled tachycardia may over time be associated with a reversible decline in ventricular performance.

Heart Rate ControlWhat’s new?

Rate control: AVN blockersWhich ones?
Beta-blockers-which one CCB-when/which one Digoxin ?Amiodarone

Mechanism of Action: β-blockers
Gs Protein
cAMP
β1Stimulation
(Cardiac Sarcolemma)
ProteinKinase A
SR release of CaPhosphorylates Trop IIncrease If in SN/AVN

Beta-Blocker Generations

Differences in BB properties

Beta-blockers


CCB better for Rate control than BBThe RATAF trial (in Select Populations)

Summary Rate control Acute Rate Control
In the acute setting in the absence of pre-excitation, intravenous administration of beta blockers or non-dihydropyridine calcium channel antagonists is recommended to slow the ventricular response to AF, exercising caution in patients with hypotension or heart failure.
In the acute setting, intravenous administration of digoxin or amiodarone is recommended to control the heart rate in patients with AF and concomitant heart failure, or in the setting of hypotension.
In pre-excitation, preferred drugs are class I antiarrhythmic drugs or amiodarone. When pre-excited AF is present, beta blockers, non-dihydropyridine calcium channel antagonists, digoxin, and adenosine are
contraindicated. Use Amiodarone or Procainamide.
Long-term Rate Control
Rate control using pharmacological agents (β-blockers, nondihydropyridine. Calcium channel antagonists, digitalis, or a combination thereof) is recommended in patients with paroxysmal, persistent, or permanent AF.
The choice of medication should be individualized and the dose modulated to avoid bradycardia. In patients who experience symptoms related to AF during activity, the adequacy of rate control should be assessed during exercise,
and therapy should be adjusted to achieve a physiological chronotropic response and to avoid bradycardia. It is reasonable to initiate treatment with a lenient rate control protocol aimed at a resting heart rate <110 bpm. It is reasonable to adopt a stricter rate control strategy when symptoms persist or tachycardiomyopathy occurs, despite lenient rate
control: resting heart rate <80 bpm and heart rate during moderate exercise <110 bpm. After achieving the strict heart rate target, a 24 h Holter monitor is recommended to assess safety. Digoxin is indicated in patients with heart failure and LV dysfunction, and in sedentary (inactive) patients. It is not effective for rate
control during exercise. Rate control may be achieved by administration of oral amiodarone when other measures are unsuccessful or contraindicated. Note
can convert to SR….MUST be adequately ACed Digoxin should not be used as the sole agent to control the rate of ventricular response in patients with AF.

Rate control: Ablate (AVN) & Pace Symptomatic (SOB, DOE, Palpitation,
dizzy..)
Permanent AF or persistent failed AAD/AB
Hypotensive with poor rate control

Rhythm Maintenance
The AFFIRM, RACE, and AF-CHF trials have shown no mortality benefit to a rhythm control strategy compared to a rate control strategy. Therefore, a rate control strategy, without attempts at restoration or maintenance of sinus rhythm (SR), is reasonable in some patients with AF, especially those who are elderly and asymptomatic.
If rate control offers inadequate symptomatic relief, restoration of sinus rhythm becomes a clear long-term goal. Restoration and maintenance of sinus rhythm continues to be a reasonable treatment approach in many patients with AF
Keep in mind rhythm maintenance may not be chronic. Can be used “as needed” for infrequent episodes (once a year) as “pill in pocket”

Affirm
Total Mortality in AFFIRM Trial

Asymptomatic or not?
Check with spouse 6 min walk test-300m-NYHA class I Treadmill DCCV to SR & note if any improvement
in symptoms

Rhythm Maintenance: 1) AAD

Issues with these Guidelines
These guidelines are based NOT on efficacy but by limiting side effects/proarrhythmia
E.G. sotalol/propafenone/flecanide above amiodarone and ablation

William Vaughn Classification

Class Ic: Flecanide & Propafenone Can be started in an out patient setting as long
as sinus node and AV conduction normal Avoid in conduction blocks, SHD: ischemia,
significant LVH (1.4cm) Ideal for pill in pocket: flecanide 300mg or
propafenone 600mg x 1 dose with verapamil 80mg (unless already on an AV blocking agent)
Can also be used to “top off” if chronically on Ic agent (as long max daily dose not reached 400/900)
Effective in converting to SR 70-80% (within 4hours) in maintaining SR in~40% (exception RAFT trial-70%)

Class III: Sotalol/Amiodarone/Dofetilide/Dronedarone Can be initiated as an out patient if: not
bradycardic, baseline borderline QTc, hypokalemia, hypomagnesemia, female gender
Efficacy 40% Main issue prolonged QTc and TdP, especially if
QTc >500ms+bradycardia+ K or Mg Risk of TdP was <1% in trials Renal excreated not used if GFR <40ml/min Beta blocking effects plateau at a lower dose
(≤240/day) than class III effects Not effective for pharmacological conversion

Class III: Sotalol/Amiodarone/Dofetilide/Dronedarone Most effective, efficacy of 50-60% 2nd line in structurally normal hearts 1st
in patients with CHF Maintenance dose in AF should be no
more than 200mg/day: even at this dose 15% may have thyroid abnormalities (usually hypo), 2% pulmonary toxicity annually
Monitor 2 x a year lft, tsh and eye exam, x-ray once a year

Class III: Sotalol/Amiodarone/Dofetilide/Dronedarone Efficacy 40% better with paroxysmal
60% High risk of TdP, requires initiation
hospitalization Renal elimination Can be used in CHF Well tolerated

Class III: Sotalol/Amiodarone/Dofetilide/Dronedarone Like amiodarone but no iodine Less effective Only drug shown to reduce cv mortality
and hospitalization

Dronedarone
O
CH3
OI
I
O
N
CH3
CH3
Dronedarone does not contain iodine, and has the addition of a methane-sulfonyl group that reduces lipophilicity to decrease accumulation in tissue.
dronedarone
amiodarone

New developments in AAD therapy---Dronedarone
The Good—Athena The Bad---Andromeda---Black Box
---Dionysos The Ugly—Pallas—Black Box





Dronedarone current state
Avoid in Permanent AF Avoid in Class III/IV heart failure Monitor LFT’s at least in 6 weeks and then
as needed Consider dronedarone to avoid toxicities
such as thyroid dysfunction or pulmonary toxicities
Caution with Dabigatran Keep cost and formulary issues in mind

Dronedarone….JAMA Feb17th 2014
5 trials measured mortality: 13 more deaths per 1000 treated than placebo
3 trials measured adverse effects: 46 more 1000 treated
1 trial vs amio: 214 more AF recurrences per 1000
Athena trial: only “positive” trial driven by hospital admissions
Guidelines: faulty management of COI, inadequate composition of writing group, lack of systematic reviews etc.
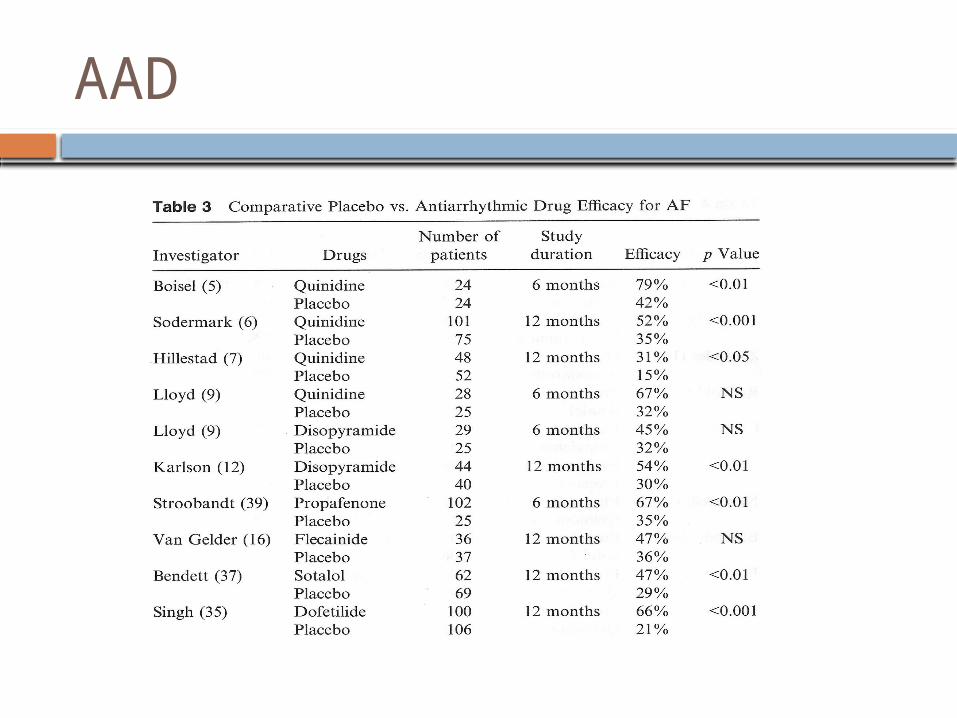
AAD

W/u needed prior to initiation of AAD H & P: CAD, PCTA, CABG, severe
uncontrolled HTN, valve disorders EKG:(2/3 deg block, LBBB, RBBB+hb,
QRS/QT) Echo: EF, valve, wall motion/thickness
± Ischemic evaluation: at initiation and at regular intervals or if symptoms develop

Rhythm Maintenance: 2) Ablation
Class IIa

Rate control plusanticoagulation preferred
Rhythm controlpreferred
• No or lesser AF symptoms
• Longer AF Hx• More SHD• Toxicity Risk• Elderly• Greater risk of
proarrhythmia• Greater AF symptoms• Symptoms despite rate control• Younger age• No or lesser SHD
In anticoagulation candidates, continue anticoagulation indefinitely
APPROACH TO AFIB THERAPY

Digoxin 2015 update

VA physician guidelines..

Thank you

ANY QUESTIONS?