dr. roy philip
TRANSCRIPT

Clinical LeadershipClinical Leadership
Maternity and Child HealthMaternity and Child Health
Dr. Roy K PhilipConsultant Paediatrician & Neonatologist
University Hospital LimerickLimerick, Ireland
[email protected] @roykphilip

DisclaimerDisclaimer• Conflicts of interest: Nil to declare • Clinical Bias: Actively promote breastfeeding among
premature infants
• Communications: Voice views through Social / Professional media including

FormatFormat• Clinical leadershipClinical leadership• Value in healthcareValue in healthcare• Positive developmentsPositive developments• Clinical innovationsClinical innovations
• Some storiesSome stories• Personal viewsPersonal views

Clinical leadershipClinical leadership
• Clinical governancegovernance. • InitiatingInitiating and implementing changechange.• Clinical performanceperformance enhancement. • Healthcare professionals leading innovationinnovation.• Reform of healthcare and patient services.• Buy-inBuy-in and creation of effective teamseffective teams. • ProcessProcess improvement. • (Availability), accountability and authority.

HSE Corporate Plan- sets out an ambition for the Health Services over the three years ‘15–’17. Delivery of the vision of a ‘high quality health service valued by all’‘high quality health service valued by all’

““Value” is not a bad wordValue” is not a bad word
• Michael PorterMichael Porter, Harvard Business School, and others have been pointing out for years that in health care, “value” in health care, “value” means something else: achieving good means something else: achieving good outcomes as efficiently as possibleoutcomes as efficiently as possible.
• It may never be expressible as a numerical ratio numerical ratio (quality divided by costs) that allows meaningful comparisons among providers.
• But measuring outcomes and costs measuring outcomes and costs does allow providers to push for improvement—and to learn from their competitors.

MaternityMaternity
• Key clinical guidelines - sepsis management, management of a critically ill women, clinical handoverhandover, labour ward huddlehuddle.
• Implementation of Maternity Early Warning System (IMEWSIMEWS) in the 19 maternity units.
• Development of Cardiotocography (CTGCTG) trace training modules.
• Clinical governance and senior clinical decision making senior clinical decision making in all of the units. • Reporting by the 19 maternity units on 30 quality assurance indicatorsquality assurance indicators.
More to do......More to do......• Standards of care-adverse outcomes / miscarriage.• Service user Service user feedback integration.• Optimisation of patient to clinical workforce ratio. • Primary care Primary care and maternity services.• National maternity strategy. • Clinical business informationClinical business information.• Activity based funding in maternity services.• MN-CMSMN-CMS (Maternal & newborn clinical management system)
• New maternity hospitals (Dublin & Limerick)

Child health – acute careChild health – acute care• National clinical programmes in Paediatrics and
Neonatology.• Timely, safe and efficient retrieval retrieval services.• Infants and children with surgicalsurgical needs.• Integration with child health in primary care.• Implementation of PEWSPEWS. • New Children’s Hospital.• How the NCH integrate and interact effectively
with regional centres to create a seamless model create a seamless model of ‘hub and spoke’of ‘hub and spoke’.
Clinical innovationsClinical innovations• Service developments linked to innovation.
• Projects underpinning access, equity and costaccess, equity and cost.
• Projects on paper (presentations) to patient.
• Learn and adaptadapt from successful small countries.
• Effective clinical leadership Effective clinical leadership is critical.
• DataData and evidenceevidence as the ‘fuel’ to drive.
• ArticulateArticulate your vision and (collectivecollective) mission well.

True story 1 True story 1 – service development– service development• Development of first paediatric high dependency
unit (critical care level II) outside of Dublin.• Pooling of resources to care locally with safetyto care locally with safety.• Reduction of critical care transfers by 50%• Reduction of ICU admissions by over 70%• Considerable cost savings over the five years.• Future model for NCH ‘hub and spoke’.• NoNo ward level ‘crashes’ or ‘cod blue’.• National level awards – benefit to community.

PAEDIATRIC HIGH DEPENDENCY UNIT AT LIMERICK REGIONAL HOSPITAL WIN COMMUNITY FUND
The Limerick-based Paediatric High Dependency Unit bet off strong competition from organisations representing other counties and received the majority of the 30,000 votes cast by the public to help it win the competition.
PHDU PHDU
G. Reddin, A. Hannigan, R. PhilipGraduate Entry Medical School, University of Limerick

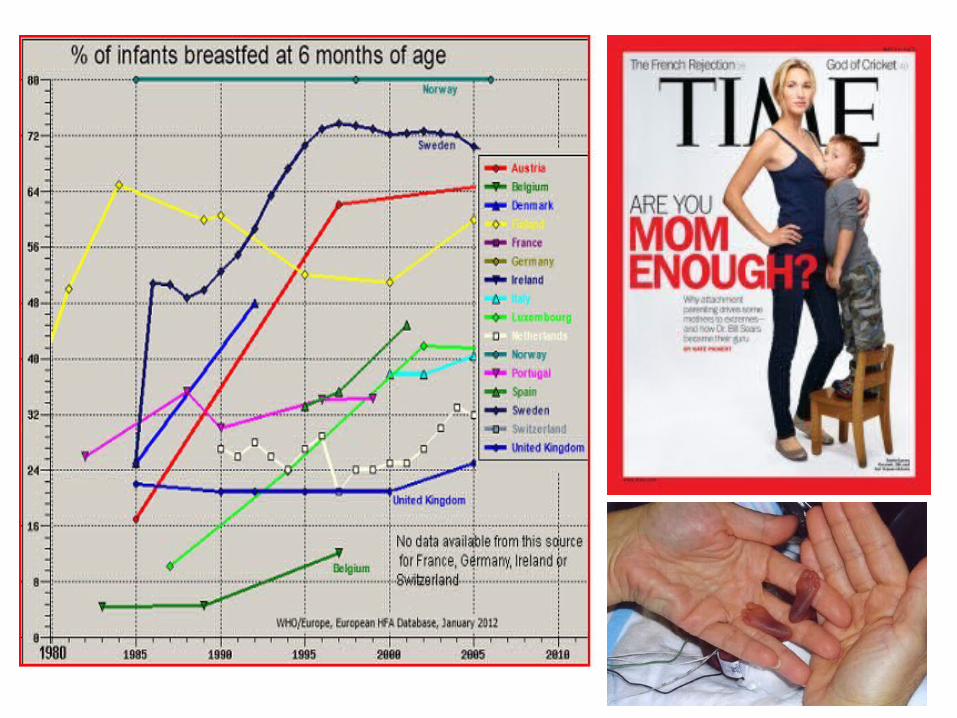
IRELANDIn 2013, 55.8% 55.8% of mothers were breastfeeding on discharge from hospital, 46.6% exclusively.
Figures for 2012 showed that five out of every 10 babies born in Ireland were being breastfed on leaving hospital.
This compares with eight out of every 10 in the UK.
Across Europe on average nine out of every 10 babies born are breastfed, with almost all babies born in Norway, Denmark and Sweden being breastfed.
Less than 10% at 6 months of age.

True story 2 True story 2 - QIP- QIP
• Breast milk for premature babies.• From below 20% to 100%• ZeroZero Necrotising enterocolitis (NECNEC) at UMHL.• Maintenance of success for the third year.• Saving of over €250,000• Through QIP, buy-in, parent in the treating team.• International black spot to hot spot in breastfeeding.• International acclaim – awards & publications.
• A 'NEC free NICU' through breastfeeding A 'NEC free NICU' through breastfeeding quality improvement project (QIP)quality improvement project (QIP)
• RK Philip, A Ismail, C Quinn, M Dunworth, A Hannigan, M O'Leary
• Pediatrics 2015; 135:Supplement 1 135S1; doi:10.1542/peds.2014-330W

Excellence in Pediatrics (EiP) – world congress. Excellence in Pediatrics (EiP) – world congress.
Best educational project award – 70 countries and over 2000 participants. Best educational project award – 70 countries and over 2000 participants.

Breast milk: the best lovebioticlovebiotic
• Crealey MR, Ludusan E, Philip RK.• J Perinatol. 2015 Aug;35(8):665. PMID: 26219700
True story 3 True story 3 - audit- audit
• Bed utilisation study.• How are we utilising our scarce bed-stockscarce bed-stock.• First paediatric review with input from public health .• To audit own practices and compare internationallycompare internationally.• Paediatric appropriateness evaluation protocol (PAEP).
• Children’s Ark at UHL – 96.6%96.6% appropriateness.• ParityParity in public, private and out-of-hours.• International recognition.

Original Article. Published: 10 May 2016
Bed Utilisation in an Irish Regional Paediatric Unit – A Cross-Sectional Study Using the Paediatric Appropriateness Evaluation Protocol (PAEP)
Coilín ÓhAiseadha1, Mai Mannix1, Jean Saunders2, Roy K. Philip3*
Increasing demand for limited healthcare resources raises questions about appropriate use of inpatient beds. In the first paediatric bed utilisation study at a regional university centre in Ireland, we conducted a cross-sectional study to audit the utilisation of inpatient beds at the Regional Paediatric Unit (RPU) in University Hospital Limerick (UHL), Limerick, Ireland and also examined hospital activity data, to make recommendations for optimal use of inpatient resources.
Conclusion: At a mean bed occupancy of 84.1%, an Irish RPU can achieve 96.6% appropriate admissions.
Citation: Int J Health Policy Manag. 2016;5(x):x–x. doi: 10.15171/ijhpm.2016.53

5 Simple tips – our experience5 Simple tips – our experience• Goal-setting - make you feel proud
(If the goal, when achieved, won’t make you proud, don’t bother to go for it!)
• Break it down - break your goal into the smallest possible granule.
• Every single day – ‘work’ on your goal every single day.
• Celebrate small victories – may be small for you.
• Process matters - no marathon is done or won by just thinking.(Instead focus on its process)

Clinical Leadership Competency Framework (CLCF) NHS
2011 NHS Leadership Academy.

Generally speaking, the number of people an organization needs to train in process improvementtrain in process improvement is the square root of the total number of personnel.
Rule of ThumbRule of Thumb
Thomas H Lee, MD, chief medical officer at Press Ganey Associates. Engaging doctors in the health care revolution ... HRB 2010
Turning Doctors into LeadersThomas H. Lee, MD

Clinical leadershipClinical leadership
• Initiating change• Effective clinical leadership• Clinical innovation• Value in healthcare• Adapt, Articulate, Buy-in• Collective mission• Goal – feel proud• Break it down - process
Dr Roy Philip Clinical Leaders Summit 26th May 2016
