dr roselle herring centre for endocrinology, diabetes and
TRANSCRIPT
Dr Roselle Herring
Centre for Endocrinology,
Diabetes and Research
(CEDAR)
University of Surrey
Diabetes Mellitus: Advances in Treatment
New Advances in Diabetes
• Type 2 diabetes mellitus
• Type 2 diabetes management considerations
• Steroids and hyperglycaemia
• Monitoring guidelines
• End of life and hyperglycaemia
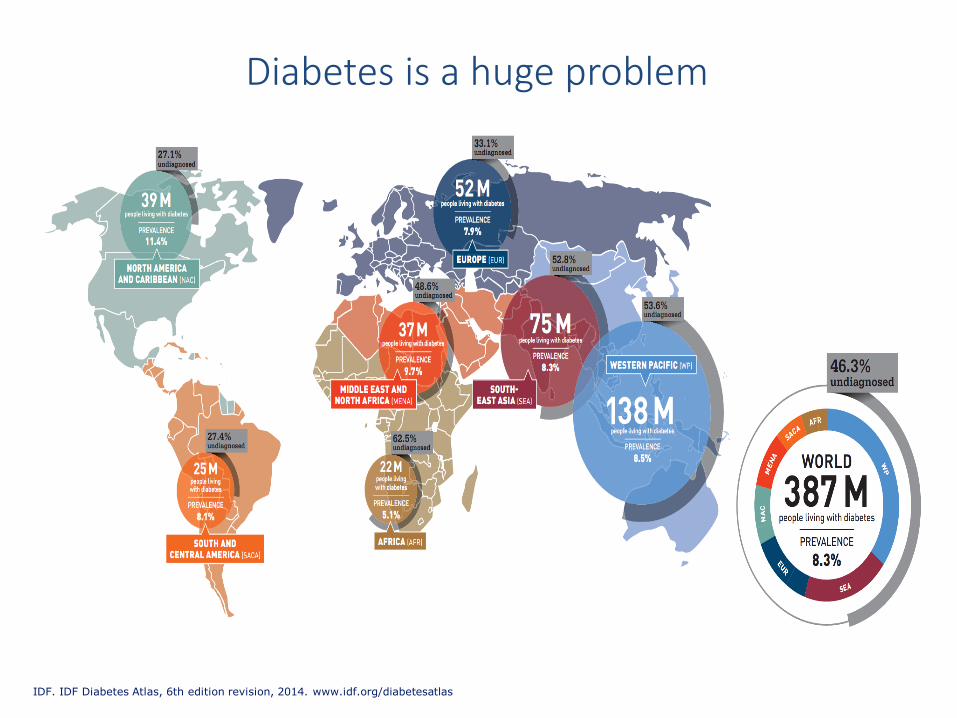
Diabetes is a huge problem
IDF. IDF Diabetes Atlas, 6th edition revision, 2014. www.idf.org/diabetesatlas
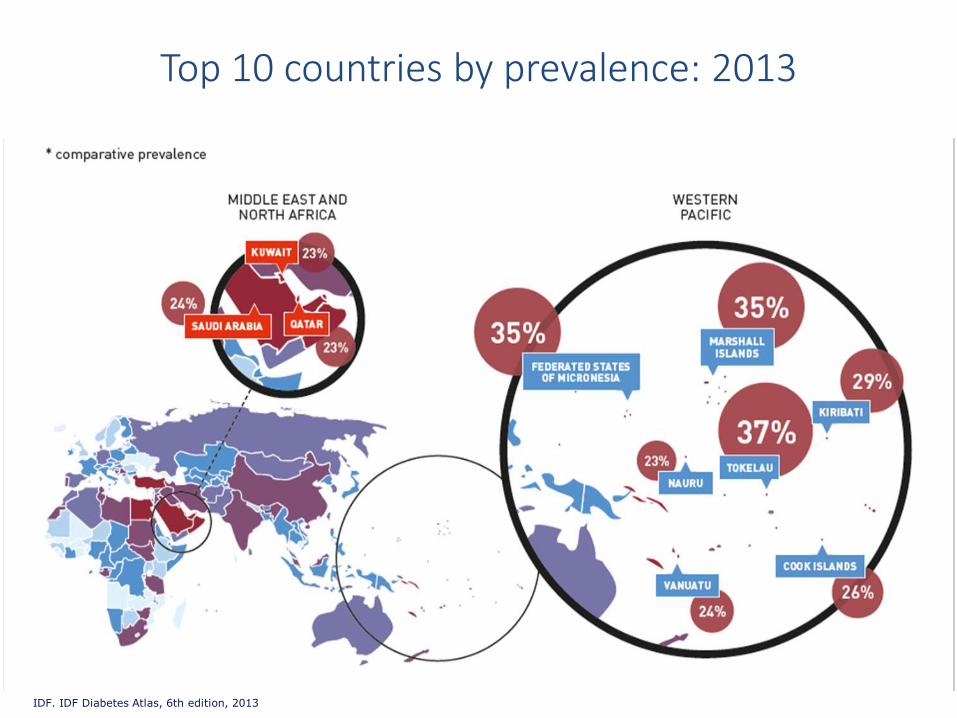
IDF. IDF Diabetes Atlas, 6th edition, 2013
Top 10 countries by prevalence: 2013
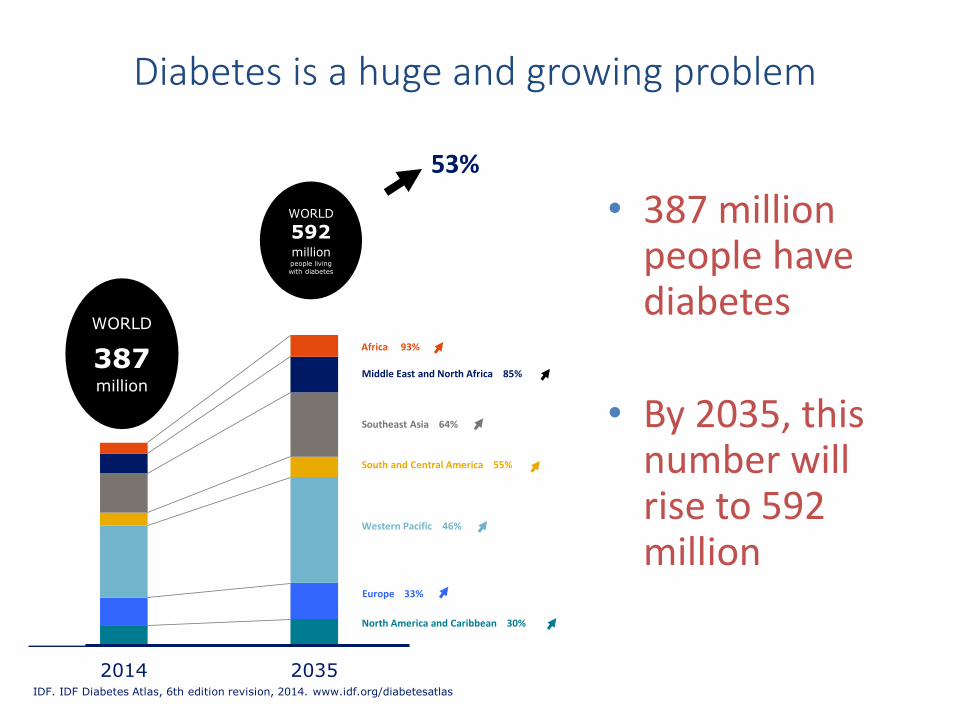
• 387 million people have diabetes
• By 2035, this number will rise to 592 million
Diabetes is a huge and growing problem
2014 2035
WORLD
387million
WORLD
592millionpeople living with diabetes
Middle East and North Africa 85%
Southeast Asia 64%
South and Central America 55%
Western Pacific 46%
Europe 33%
Africa 93%
53%
North America and Caribbean 30%
IDF. IDF Diabetes Atlas, 6th edition revision, 2014. www.idf.org/diabetesatlas

Classification of diabetes
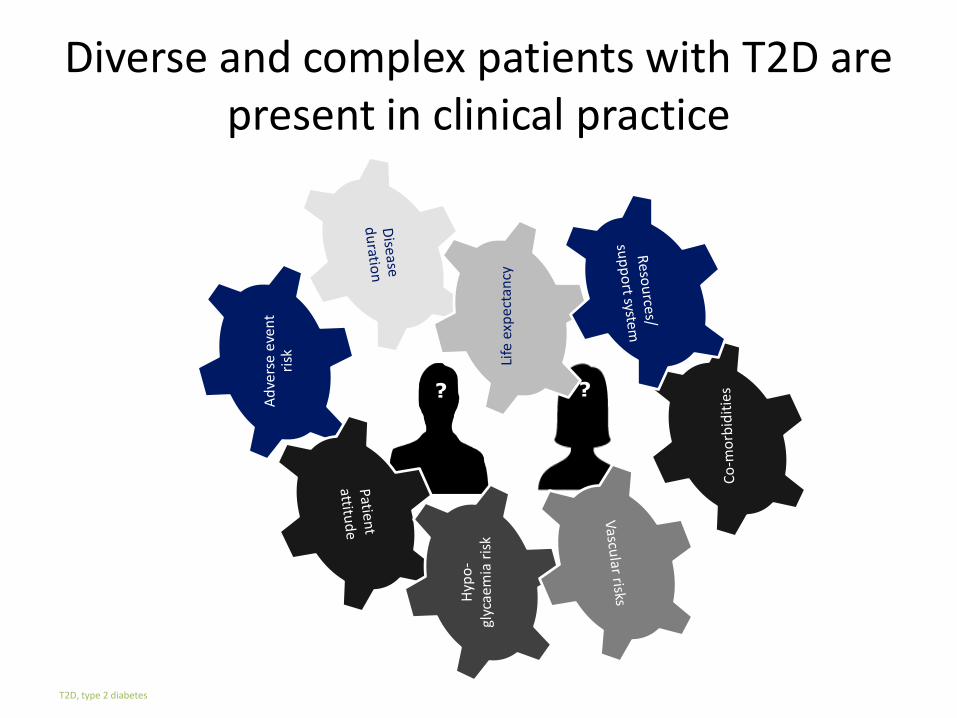
Diverse and complex patients with T2D are present in clinical practice
T2D, type 2 diabetes
? ?

Fasting plasma glucose
Postprandial glucose
Progression of Type 2 Diabetes
Diabetes
4–7 years
Diabetes Diagnosis
Impaired Glucose Tolerance
Hyperglycaemia
Adapted from Kendall DM et al. Am J Med 2009:122(6 Suppl):S37–S50

Insulin resistance
Insulin level
Fasting plasma glucose
Postprandial glucose
Beta-cell function
Progression of Type 2 Diabetes
Diabetes
4–7 years
Diabetes Diagnosis
Impaired Glucose Tolerance
Insulin dysfunction
Adapted from Kendall DM et al. Am J Med 2009:122(6 Suppl):S37–S50

HbA1c and Standardisation
• Laboratory methods are now well standardised and reliable
• National GlycohemoglobinStandardisation Programme
• A level ≥6% but <6.5% is sufficient to identify individuals at especially high risk for diabetes
Current
HbA1c
(%)
New HbA1c
(mmol/L)
6.0 42
6.5 48
7.0 53
7.5 59
8.0 64
9.0 75
Saudek C at el. A new look at Screening and Diagnosing Diabetes Mellitus. J Clin Endocrinol Metab.2008 93:2447-2453
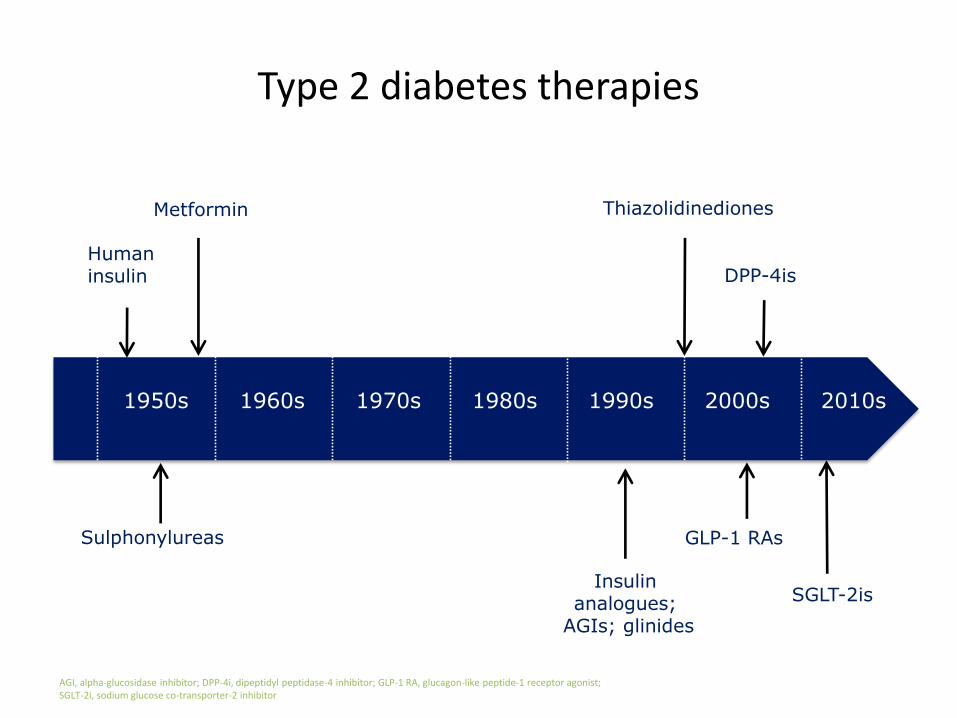
Type 2 diabetes therapies
AGI, alpha-glucosidase inhibitor; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist;SGLT-2i, sodium glucose co-transporter-2 inhibitor
1960s 1970s 1980s 1990s
Sulphonylureas
ThiazolidinedionesMetformin
1950s
Human insulin
GLP-1 RAs
DPP-4is
SGLT-2is
2000s 2010s
Insulin analogues;
AGIs; glinides
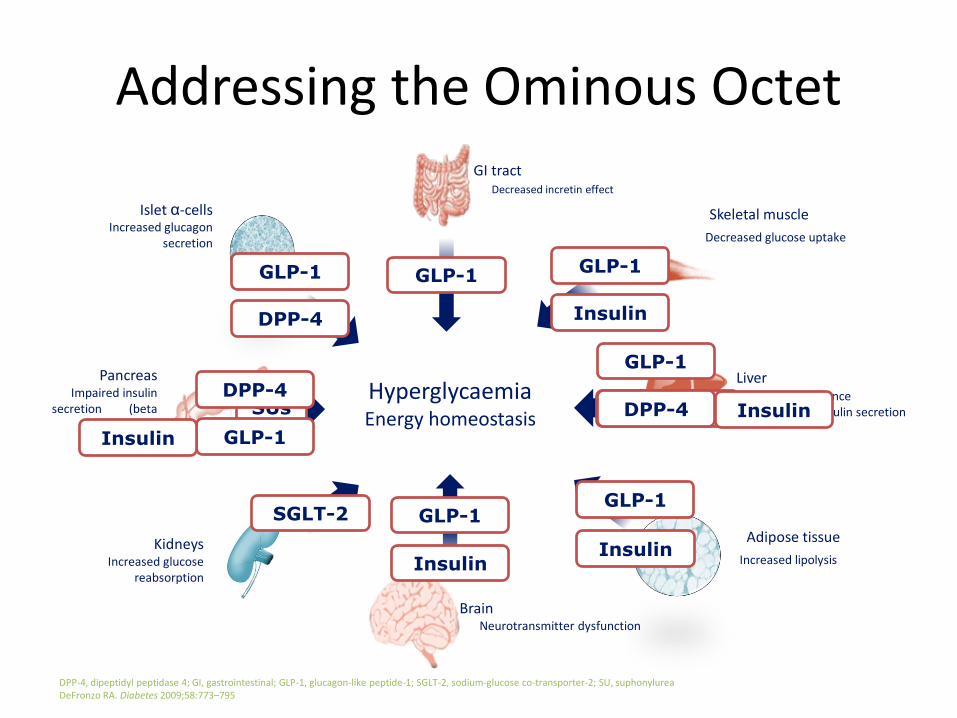
Addressing the Ominous Octet
DPP-4, dipeptidyl peptidase 4; GI, gastrointestinal; GLP-1, glucagon-like peptide-1; SGLT-2, sodium-glucose co-transporter-2; SU, suphonylureaDeFronzo RA. Diabetes 2009;58:773–795
Adipose tissue
Increased lipolysis
Skeletal muscle
Decreased glucose uptake
LiverInsulin resistanceDecreased insulin secretion
BrainNeurotransmitter dysfunction
PancreasImpaired insulin
secretion (beta cell decline)
GI tractDecreased incretin effect
KidneysIncreased glucose
reabsorption
Islet α-cellsIncreased glucagon
secretion
HyperglycaemiaEnergy homeostasis
SUs
GLP-1
DPP-4
Insulin
DPP-4
GLP-1 GLP-1GLP-1
Insulin
Metformin
GLP-1
DPP-4 Insulin
GLP-1
Insulin
GLP-1
Insulin
SGLT-2
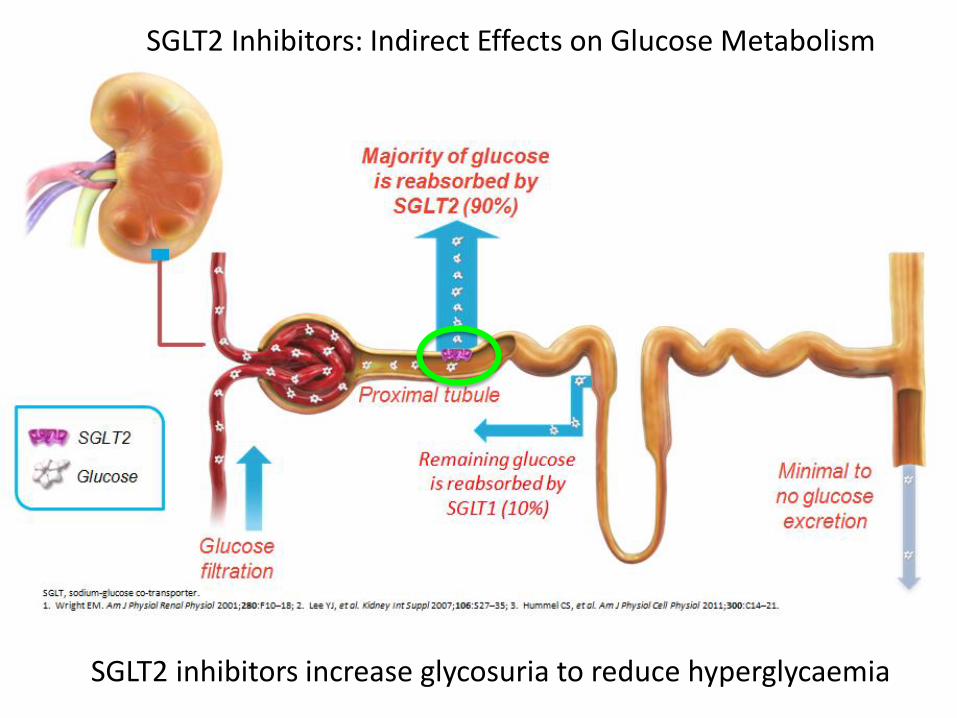
SGLT2 inhibitors increase glycosuria to reduce hyperglycaemia
SGLT2 Inhibitors: Indirect Effects on Glucose Metabolism
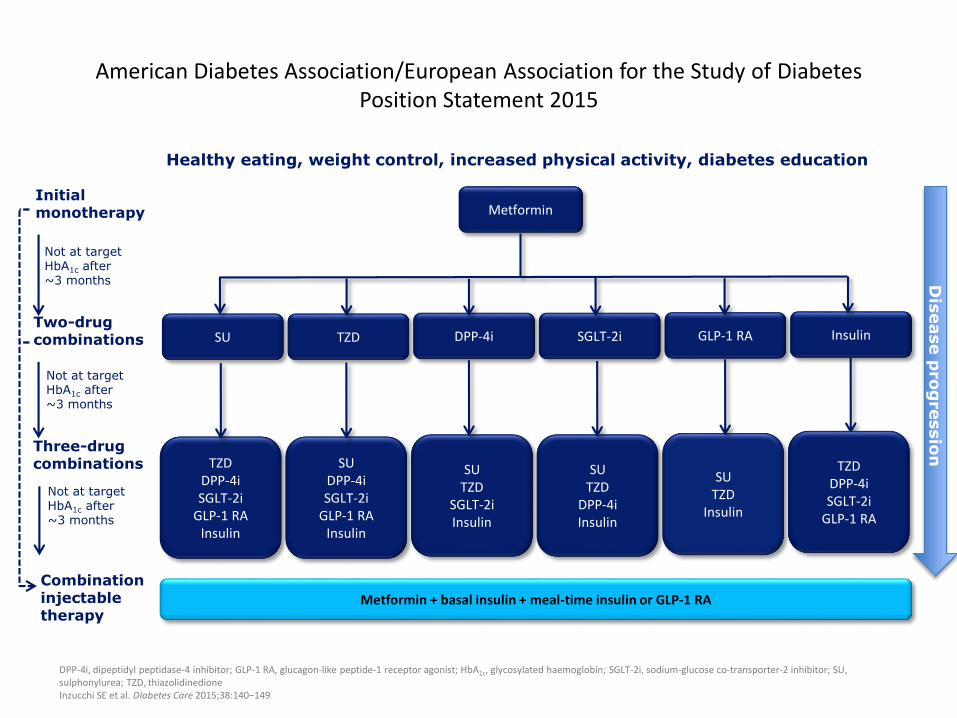
American Diabetes Association/European Association for the Study of Diabetes Position Statement 2015
DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylated haemoglobin; SGLT-2i, sodium-glucose co-transporter-2 inhibitor; SU, sulphonylurea; TZD, thiazolidinedioneInzucchi SE et al. Diabetes Care 2015;38:140−149
Healthy eating, weight control, increased physical activity, diabetes education
Not at target HbA1c after ~3 months
Two-drug combinations
Three-drug combinations
Combination injectable therapy
Initial monotherapy
Not at target HbA1c after ~3 months
Not at target HbA1c after ~3 months
GLP-1 RASGLT-2iDPP-4iTZDSU Insulin
Dis
ease p
rog
ressio
n
Metformin
SUTZD
Insulin
SUTZD
DPP-4iInsulin
SUTZD
SGLT-2iInsulin
SUDPP-4iSGLT-2i
GLP-1 RAInsulin
TZDDPP-4iSGLT-2i
GLP-1 RAInsulin
TZDDPP-4iSGLT-2i
GLP-1 RA
Metformin + basal insulin + meal-time insulin or GLP-1 RA

Considerations for individualised treatment
ADA/EASD position statement 2015
ADA, American Diabetes Association; AE, adverse event; EASD, European Association for the Study of Diabetes; HbA1c, glycated haemoglobin; T2D, type 2 diabetesAdapted from Inzucchi SE et al. Diabetes Care 2015;38:140−149
Hypoglycaemia and AE risks
Hyperglycaemia management approach
More stringent Less stringent
Long Short
Absent Severe
Important comorbidities
Highly motivated Less motivated
Resources and support system
Readily available Limited
HbA1c
7%
Life expectancy
Disease duration
Established vascular complications
Patient attitude and expectations
Few/mild
Absent SevereFew/mild
Newly diagnosed Long-standing
Low High
Usually
not
modifia
ble
Pote
ntia
lly
modifia
ble
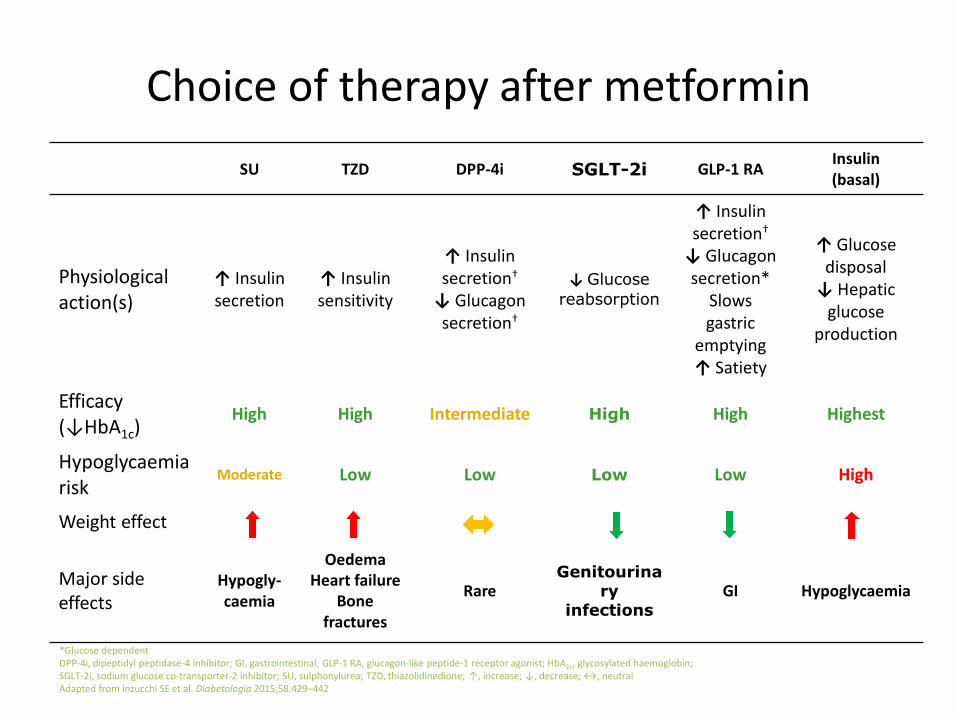
SU TZD DPP-4i SGLT-2i GLP-1 RAInsulin(basal)
Physiological action(s)
↑ Insulin secretion
↑ Insulin sensitivity
↑ Insulin secretion†
↓ Glucagon secretion†
↓ Glucose
reabsorption
↑ Insulin secretion†
↓ Glucagon secretion*
Slows gastric
emptying↑ Satiety
↑ Glucose disposal
↓ Hepatic glucose
production
Efficacy (↓HbA1c)
High High Intermediate High High Highest
Hypoglycaemia risk
Moderate Low Low Low Low High
Weight effect
Major side effects
Hypogly-caemia
OedemaHeart failure
Bone fractures
RareGenitourina
ry infections
GI Hypoglycaemia
Choice of therapy after metformin
*Glucose dependentDPP-4i, dipeptidyl peptidase-4 inhibitor; GI, gastrointestinal; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylated haemoglobin;SGLT-2i, sodium glucose co-transporter-2 inhibitor; SU, sulphonylurea; TZD, thiazolidinedione; ↑, increase; ↓, decrease; ↔, neutralAdapted from Inzucchi SE et al. Diabetologia 2015;58:429–442
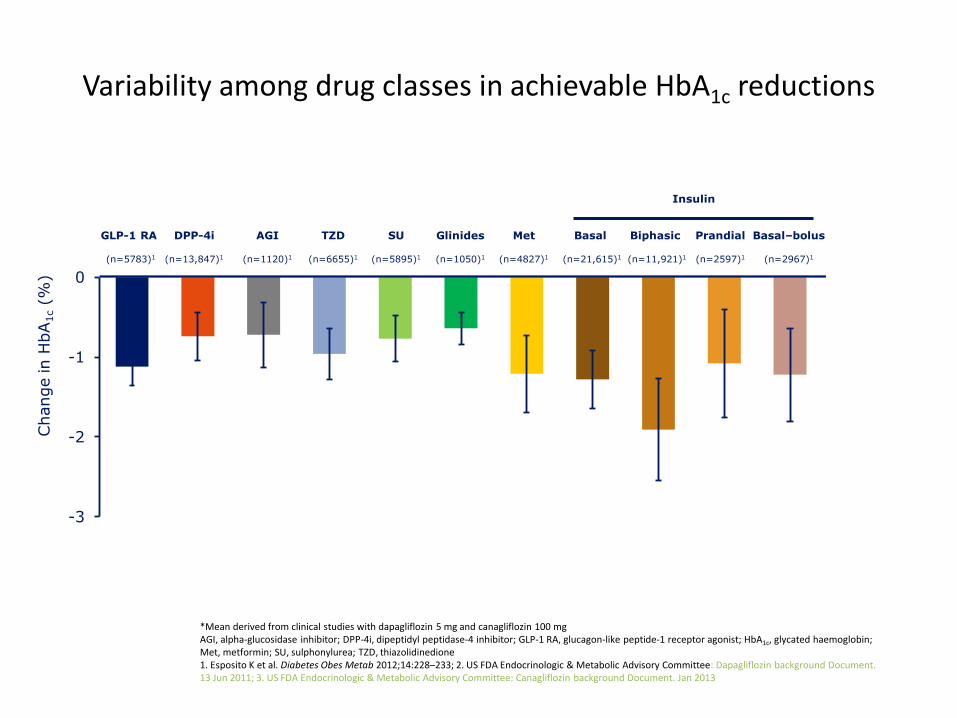
-3
-2
-1
0
Change in H
bA
1c(%
)
GLP-1 RA
(n=5783)1
DPP-4i
(n=13,847)1
AGI
(n=1120)1
TZD
(n=6655)1
SU
(n=5895)1
Glinides
(n=1050)1
Met
(n=4827)1
Basal
(n=21,615)1
Biphasic
(n=11,921)1
Prandial
(n=2597)1
Basal–bolus
(n=2967)1
SGLT-2i
(n=12,090)2,3*
Variability among drug classes in achievable HbA1c reductions
*Mean derived from clinical studies with dapagliflozin 5 mg and canagliflozin 100 mgAGI, alpha-glucosidase inhibitor; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycated haemoglobin; Met, metformin; SU, sulphonylurea; TZD, thiazolidinedione1. Esposito K et al. Diabetes Obes Metab 2012;14:228–233; 2. US FDA Endocrinologic & Metabolic Advisory Committee: Dapagliflozin background Document. 13 Jun 2011; 3. US FDA Endocrinologic & Metabolic Advisory Committee: Canagliflozin background Document. Jan 2013
Insulin
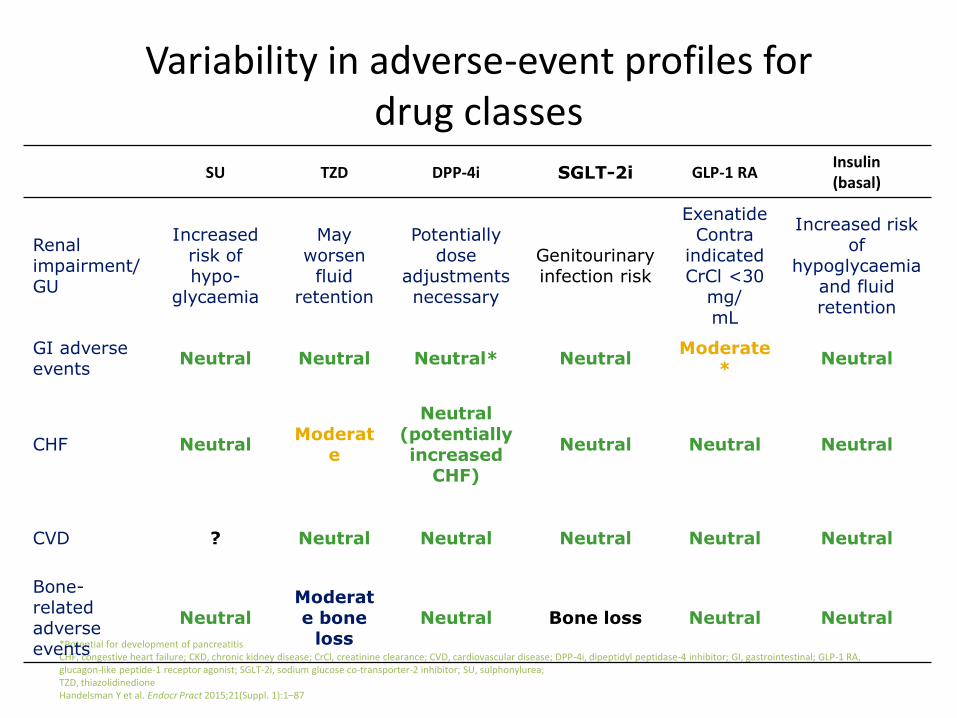
Variability in adverse-event profiles for drug classes
*Potential for development of pancreatitisCHF, congestive heart failure; CKD, chronic kidney disease; CrCl, creatinine clearance; CVD, cardiovascular disease; DPP-4i, dipeptidyl peptidase-4 inhibitor; GI, gastrointestinal; GLP-1 RA, glucagon-like peptide-1 receptor agonist; SGLT-2i, sodium glucose co-transporter-2 inhibitor; SU, sulphonylurea; TZD, thiazolidinedioneHandelsman Y et al. Endocr Pract 2015;21(Suppl. 1):1–87
SU TZD DPP-4i SGLT-2i GLP-1 RAInsulin(basal)
Renal impairment/GU
Increased risk of hypo-
glycaemia
May worsen
fluid retention
Potentially dose
adjustments necessary
Genitourinary infection risk
ExenatideContra
indicatedCrCl <30
mg/mL
Increased risk of
hypoglycaemia and fluid retention
GI adverse events
Neutral Neutral Neutral* NeutralModerate
*Neutral
CHF NeutralModerat
e
Neutral (potentially increased
CHF)
Neutral Neutral Neutral
CVD ? Neutral Neutral Neutral Neutral Neutral
Bone-related adverse events
NeutralModerate bone
lossNeutral Bone loss Neutral Neutral
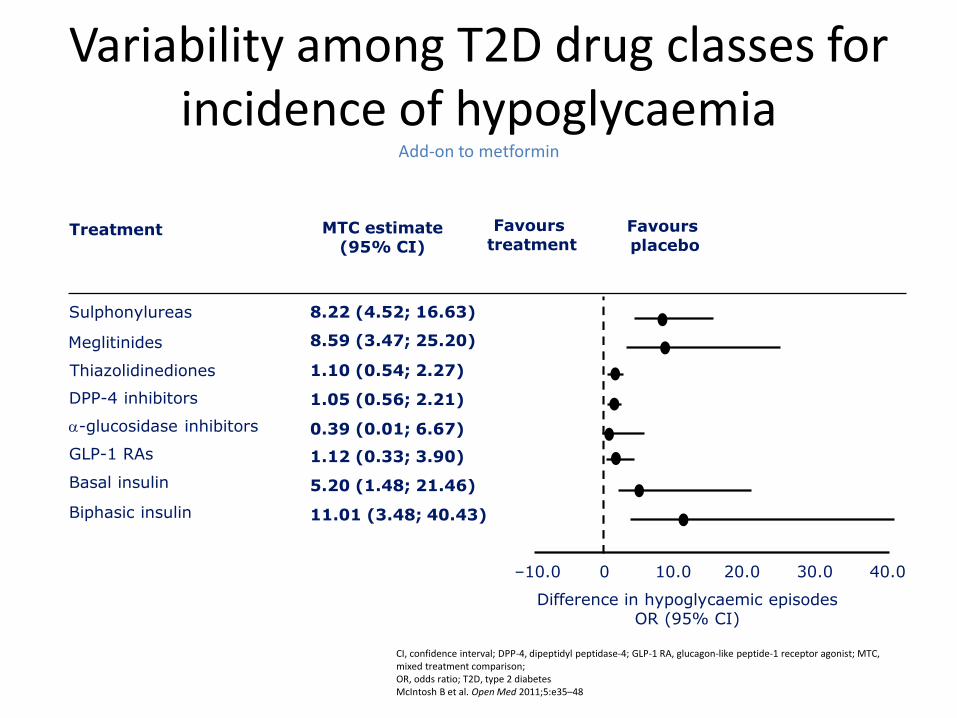
Variability among T2D drug classes for incidence of hypoglycaemia
Add-on to metformin
CI, confidence interval; DPP-4, dipeptidyl peptidase-4; GLP-1 RA, glucagon-like peptide-1 receptor agonist; MTC, mixed treatment comparison; OR, odds ratio; T2D, type 2 diabetesMcIntosh B et al. Open Med 2011;5:e35–48
GLP-1 RAs
Thiazolidinediones
Meglitinides
Sulphonylureas
DPP-4 inhibitors
Basal insulin
Biphasic insulin
-glucosidase inhibitors
Treatment MTC estimate(95% CI)
Favours treatment
Favours placebo
Difference in hypoglycaemic episodesOR (95% CI)
1.12 (0.33; 3.90)
11.01 (3.48; 40.43)
5.20 (1.48; 21.46)
0.39 (0.01; 6.67)
1.05 (0.56; 2.21)
1.10 (0.54; 2.27)
8.59 (3.47; 25.20)
8.22 (4.52; 16.63)
–10.0 0 10.0 30.020.0 40.0
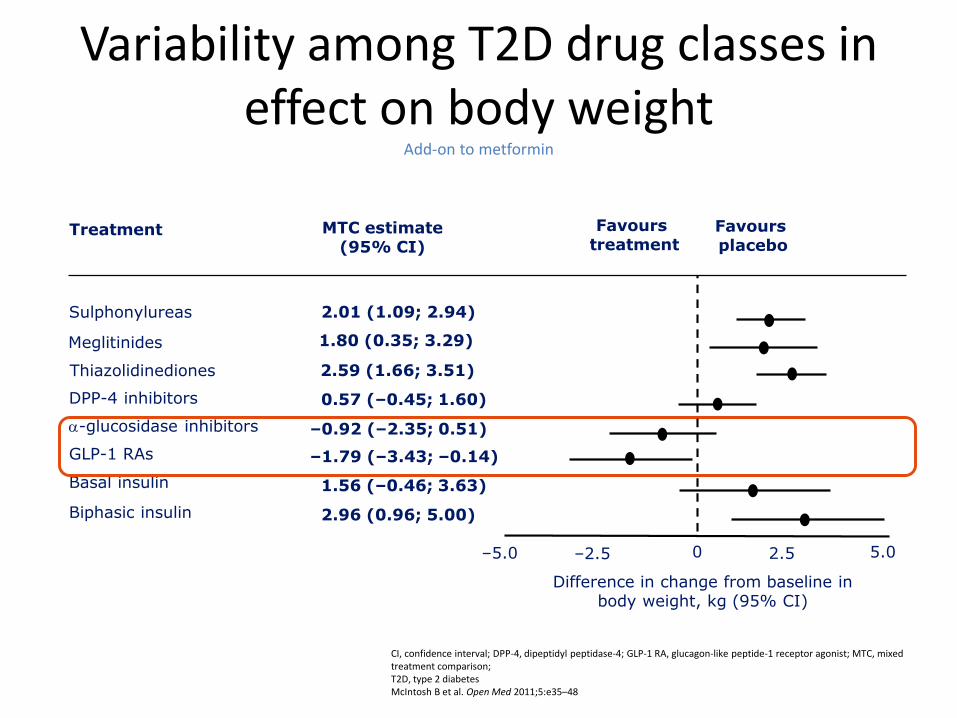
GLP-1 RAs
Thiazolidinediones
Meglitinides
Sulphonylureas
DPP-4 inhibitors
Basal insulin
Biphasic insulin
-glucosidase inhibitors
Treatment MTC estimate(95% CI)
Favours treatment
Favours placebo
Difference in change from baseline in body weight, kg (95% CI)
–1.79 (–3.43; –0.14)
2.96 (0.96; 5.00)
1.56 (–0.46; 3.63)
–0.92 (–2.35; 0.51)
0.57 (–0.45; 1.60)
2.59 (1.66; 3.51)
1.80 (0.35; 3.29)
2.01 (1.09; 2.94)
–5.0 –2.5 0 5.02.5
Variability among T2D drug classes in effect on body weight
Add-on to metformin
CI, confidence interval; DPP-4, dipeptidyl peptidase-4; GLP-1 RA, glucagon-like peptide-1 receptor agonist; MTC, mixed treatment comparison; T2D, type 2 diabetesMcIntosh B et al. Open Med 2011;5:e35–48

Case:61 year old female
Patient characteristics
PMH: Waldenstroms macroglobulinaemia (6/52 chemotherapy – ibrutinib / dexamethasone 10mg IV - 4 days last dose 03/06/2016)
Nephrotic syndrome:
Therapy Prednisolone 20mg
HbA1c 45mmol/mol
Random glucose 15mmol/L
BMI 34.2 kg/m2
BMI, body mass index; HbA1c, glycosylated haemoglobin; T2D, type 2 diabetes

What is the diagnosis?
Choose one
A.Type 2 diabetes mellitus
B.Impaired fasting hyperglycaemia
C.Steroid induced hyperglycaemia
D.Normoglycaemia
E.Steroid induced diabetes

Steroid treatment and diabetes
• The use of steroid treatment in people with pre-existing diabetes will undoubtedly result in worsening glucose control; this may be termed steroid induced hyperglycaemia. This will warrant temporary additional and more active glycaemic management.
• A rise in glucose, related to steroid therapy occurring in people without a known diagnosis of diabetes is termed steroid induced diabetes. This may or may not resolve when the steroids are withdrawn.
Steroid Therapy and Inpatient Glycaemic
Control
• Steroids raised blood glucose via a number of mechanisms including:
– Increased hepatic gluconeogenesis
– Decreased peripheral tissue glucose uptake
– Decreased sensitivity to insulin in cells in the extremities (thought to be linked with body fat redistribution)
24

Steroid dose equivalents
Steroid Potency (Equivalent dose)
Duration of action (1/2 life)
Hydrocortisone 20mg 8
Prednisolone 5mg 16-36
Methylprednisolone 4mg 18-40
Dexamethasone 0.75mg 36-54
Betamethasone 0.75mg 26-54
N.B: Potency relates to anti – inflammatory action, which may not equate to hyperglycaemic effect
JBDS-IP: Managament of hyperglycaemia and steroid therapy 2014
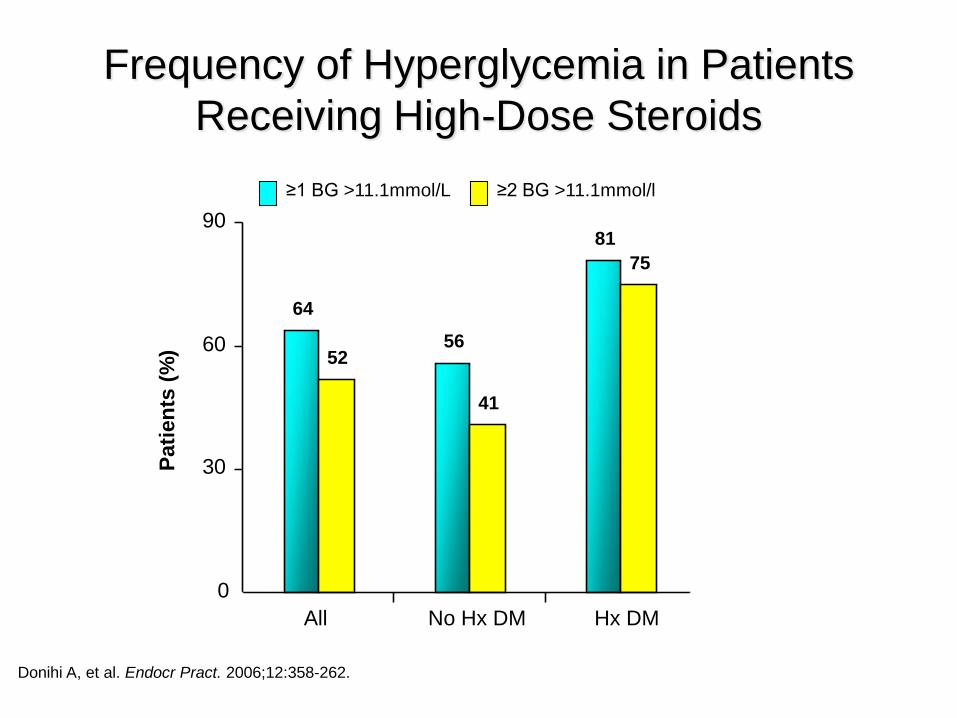
Frequency of Hyperglycemia in Patients
Receiving High-Dose Steroids
26Donihi A, et al. Endocr Pract. 2006;12:358-262.
≥1 BG >11.1mmol/L ≥2 BG >11.1mmol/l
64
56
81
52
41
75
0
30
60
90
All No Hx DM Hx DM
Pati
en
ts (
%)
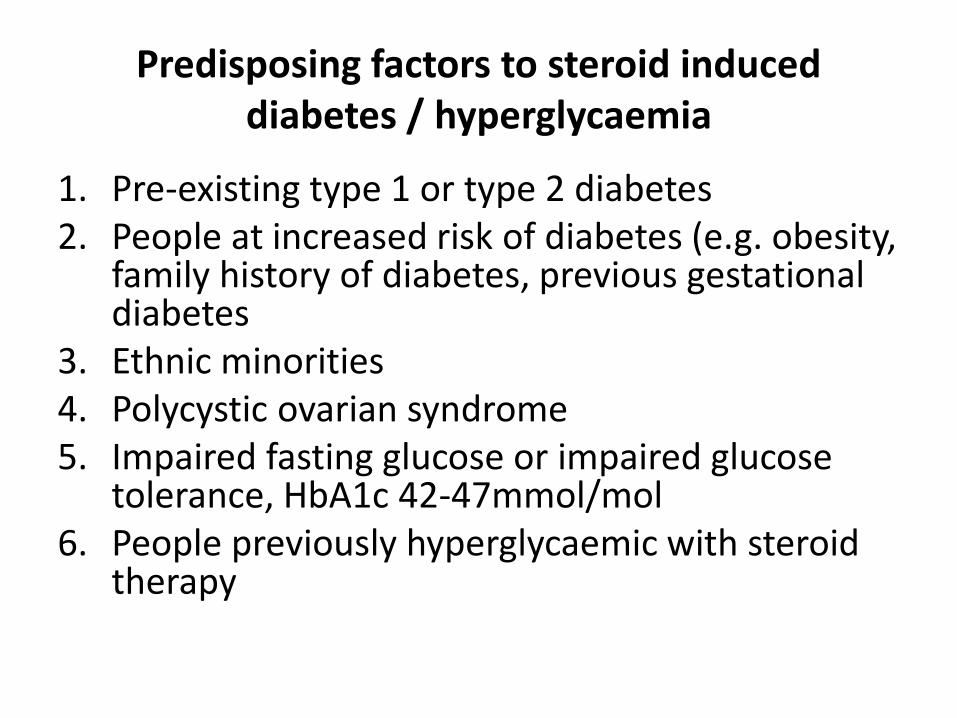
Predisposing factors to steroid induced diabetes / hyperglycaemia
1. Pre-existing type 1 or type 2 diabetes 2. People at increased risk of diabetes (e.g. obesity,
family history of diabetes, previous gestational diabetes
3. Ethnic minorities4. Polycystic ovarian syndrome5. Impaired fasting glucose or impaired glucose
tolerance, HbA1c 42-47mmol/mol6. People previously hyperglycaemic with steroid
therapy
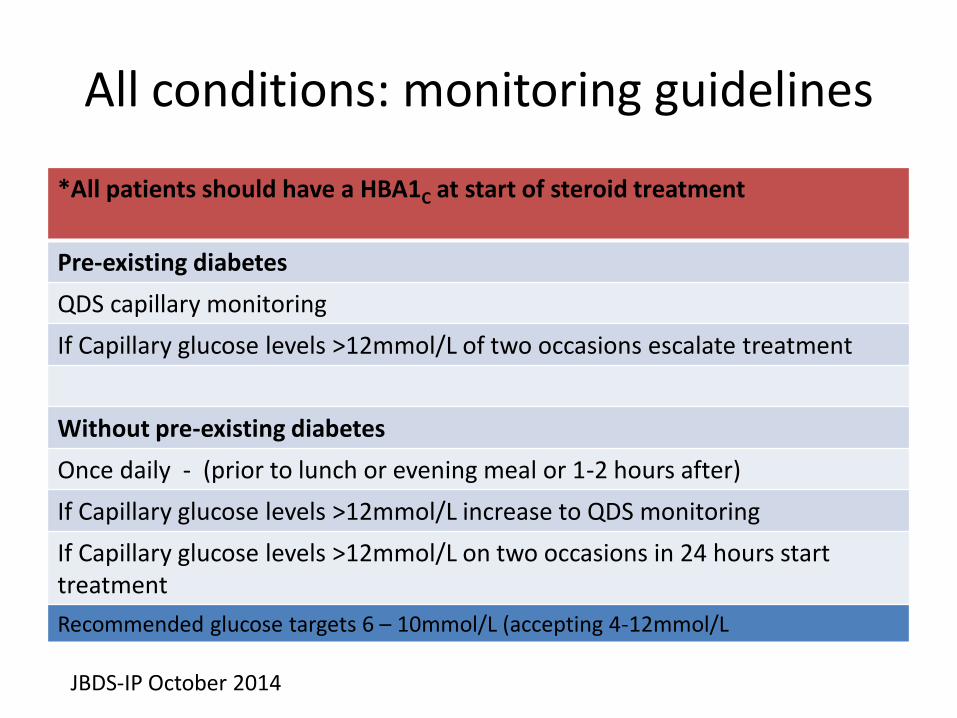
All conditions: monitoring guidelines
*All patients should have a HBA1C at start of steroid treatment
Pre-existing diabetes
QDS capillary monitoring
If Capillary glucose levels >12mmol/L of two occasions escalate treatment
Without pre-existing diabetes
Once daily - (prior to lunch or evening meal or 1-2 hours after)
If Capillary glucose levels >12mmol/L increase to QDS monitoring
If Capillary glucose levels >12mmol/L on two occasions in 24 hours start treatment
JBDS-IP October 2014
Recommended glucose targets 6 – 10mmol/L (accepting 4-12mmol/L

RSCH: STARTING HIGH DOSE STEROIDS IN ONCOLOGY OUTPATIENTS Care pathway
Many of these patients will develop hyperglycaemia which may adversely affect their wellbeing and outcomes
HbA1c >47 in the last 3 months?
Send blood for • random glucose
(grey) • HbA1c (purple)
Is random plasma Glucose >11.0mmol?
• Advice leaflet
• Start capillary monitoring premeals.
Do any of the following apply:• BMI>30• FH diabetes• Previous
gestational DM• Pancreatic lesion
or PMH pancreatitis
• Advice leaflet
• Urine glucose testing pre lunch
Daily for first 2 weeks and weekly after that while on steroids
Possible pre-existing diabetes/impaired glucose tolerance.
Pre-existing diabetes/impaired glucose tolerance. High probability of insulin treatment
Moderate risk of developing steroid induced hyperglycaemia
Is urine glucose positive on 2 consecutive tests?
Risk not increased above normal
Are 2 tests >12 mmol?
• Advice leaflet
• Start capillary monitoring premeals.
refer DSN for insulin start
If 2 tests >12-20Start gliclazide80mg om
Are 2 tests >20mmol or poor response to gliclazide
Y
Y
Y
RISK ASSESSMENT BEFORE STEROIDS STARTED
WHAT IS THE RISK?
NEW: SCREENING GLYCOSURIA
CAPILLARY MONITORING TREATMENT

Without pre-existing diabetes and steroid treatment
Set capillary glucose targets (6-10mmol/L)
Gliclazide – titrate to 320mg daily (240mg in am + 80mg pm)
If still no improvement: consider 10units human insulin (humulinI or insulatard) in the morning. Titrate in increments of 10 -20%
If uncontrolled hyperglycaemia or multiple dosing of steroidconsider switching to basal analogue insulin or alternative regimen for example basal bolus or bd
Beware of nocturnal and early morning hypoglycaemia
JBDS-IP October 2014
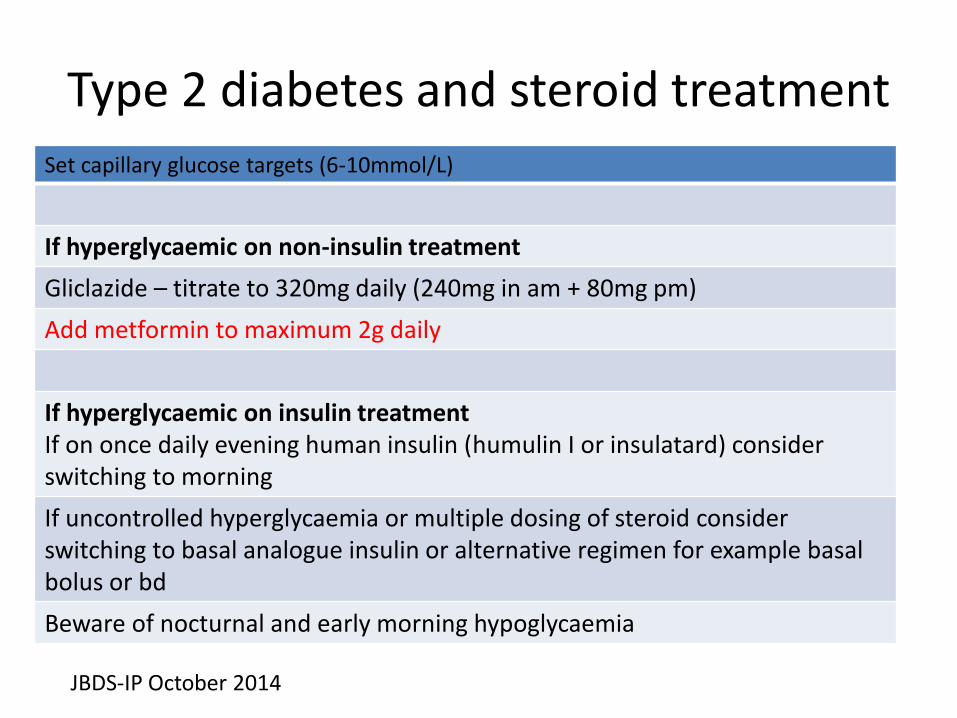
Type 2 diabetes and steroid treatmentSet capillary glucose targets (6-10mmol/L)
If hyperglycaemic on non-insulin treatment
Gliclazide – titrate to 320mg daily (240mg in am + 80mg pm)
Add metformin to maximum 2g daily
If hyperglycaemic on insulin treatmentIf on once daily evening human insulin (humulin I or insulatard) consider switching to morning
If uncontrolled hyperglycaemia or multiple dosing of steroid consider switching to basal analogue insulin or alternative regimen for example basal bolus or bd
Beware of nocturnal and early morning hypoglycaemia
JBDS-IP October 2014

End of life diabetes care
• Steroid therapy is frequently used in palliative care for symptom control, usually as dexamethasone or prednisolone
• Regardless of the indication, the impact of steroids on glucose control can cause additional hyperglycaemic symptoms

Goals of treatment
• Preserve quality of life via prevention of acute signs of (polyuria, nocturia and polydipsia)
• Prevention of sub-acute complications of sustained hyperglycaemia such as infections, hypercoagulability, catabolic weight loss and osmotic diuresis
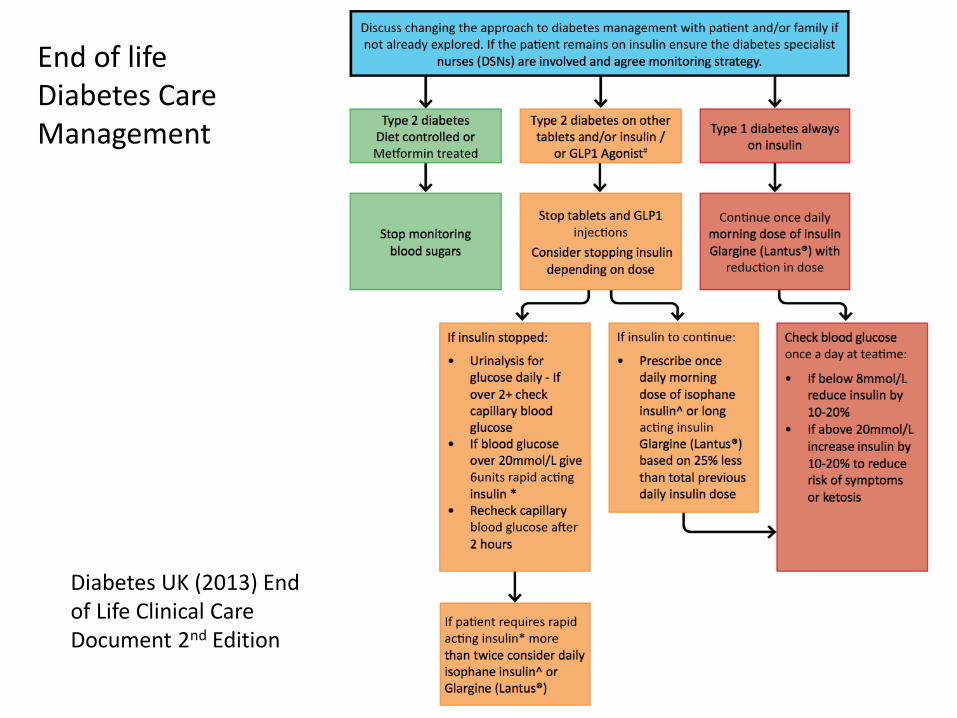
Diabetes UK (2013) End of Life Clinical Care Document 2nd Edition
End of life Diabetes Care Management

Summary
• Diabetes prevalence is increasing
• Considerations for individualised treatment
• HbA1c / risk assessment should be done on all patients starting high dose steroids
• Diabetes medication should be reduced towards end of life