dr. michael power, national clinical lead, critical care programme, csp hse
TRANSCRIPT

M Power National Clinical Lead Critical Care Programme National Clinical Programmes Clinical Strategy and Programmes Division
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
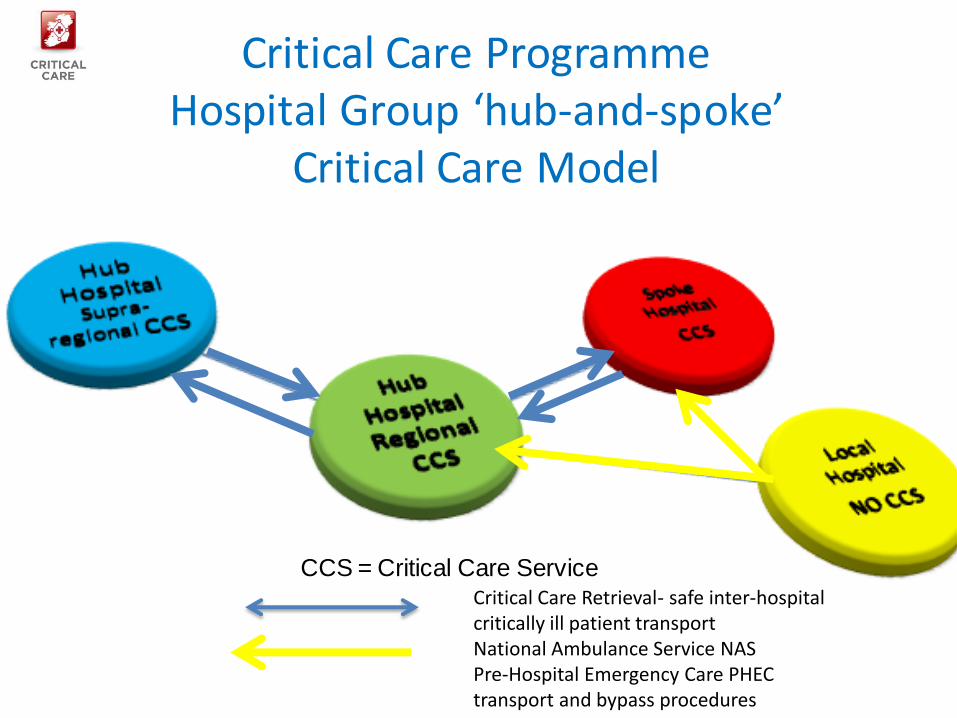
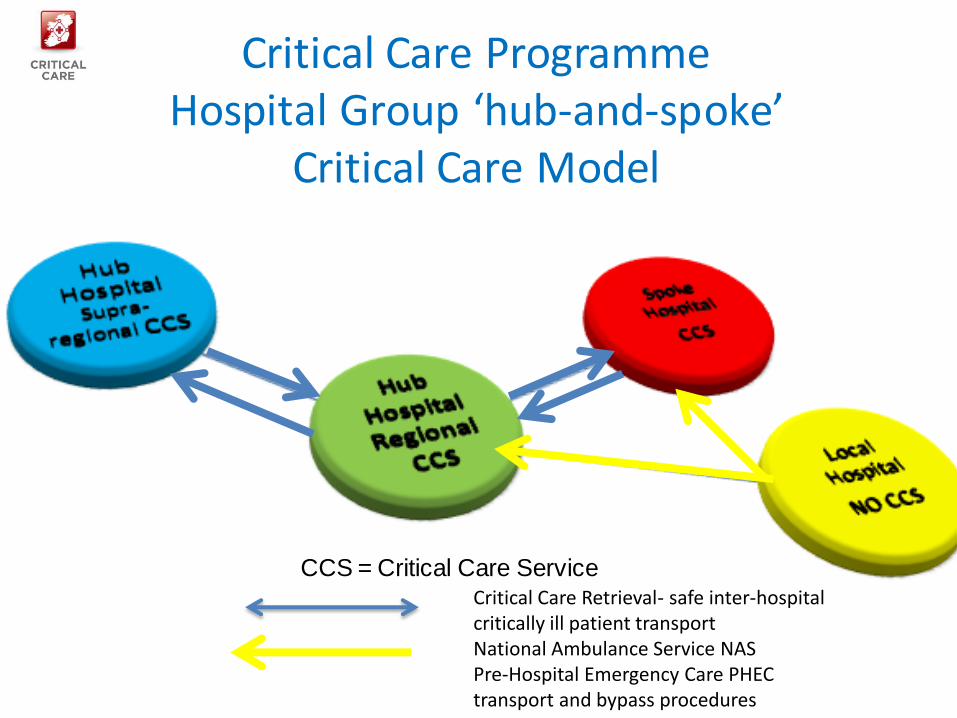
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
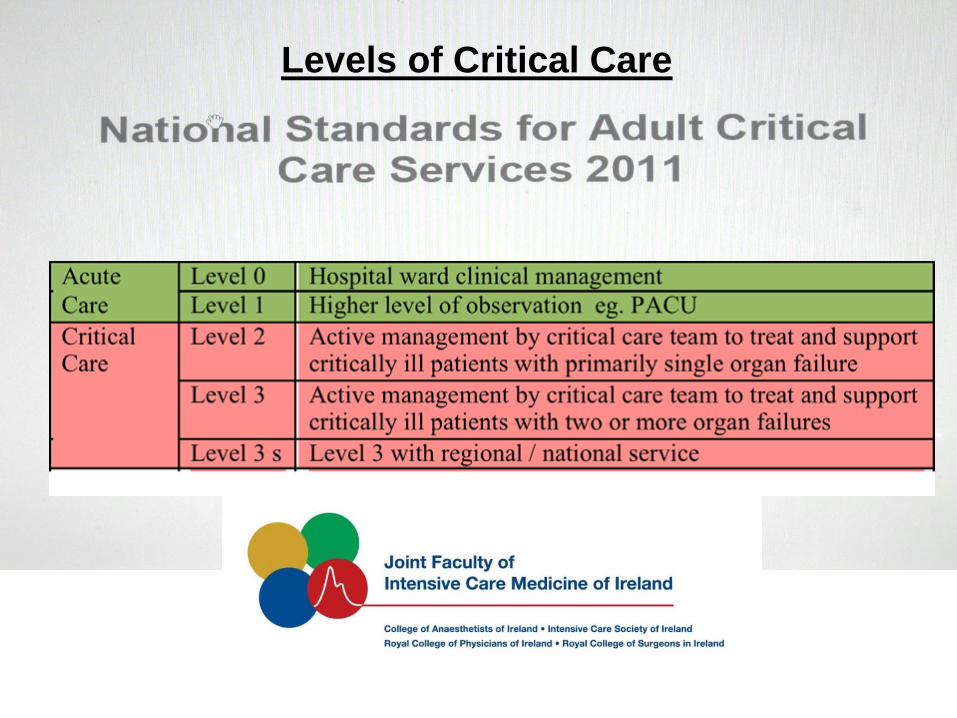
Levels of Critical Care
Joint Faculty of Intensive Care Medicine of Ireland (JFICMI) National Standards define
Critical Care Service
ldquoappropriate for the care of patients requiring Level 2 3 and 3(s) critical carehellipgenerally delivered within a High-Dependency Unit (HDU) or Intensive Care Unit (ICU)rdquo
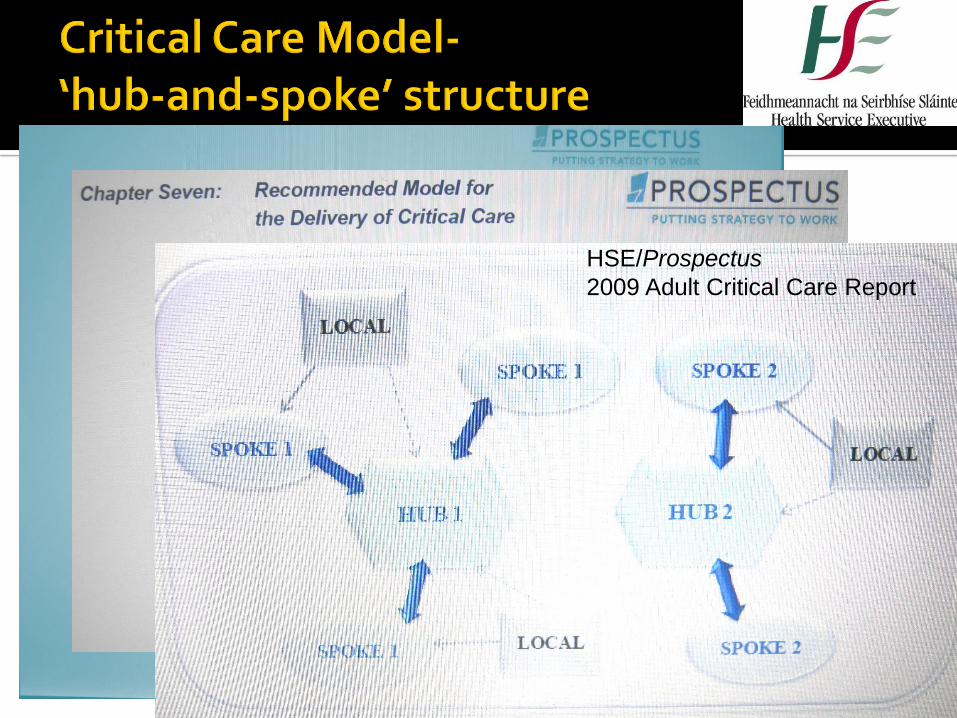
HSEProspectus
2009 Adult Critical Care Report
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Levels of Critical Care
Joint Faculty of Intensive Care Medicine of Ireland (JFICMI) National Standards define
Critical Care Service
ldquoappropriate for the care of patients requiring Level 2 3 and 3(s) critical carehellipgenerally delivered within a High-Dependency Unit (HDU) or Intensive Care Unit (ICU)rdquo
HSEProspectus
2009 Adult Critical Care Report
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Levels of Critical Care
Joint Faculty of Intensive Care Medicine of Ireland (JFICMI) National Standards define
Critical Care Service
ldquoappropriate for the care of patients requiring Level 2 3 and 3(s) critical carehellipgenerally delivered within a High-Dependency Unit (HDU) or Intensive Care Unit (ICU)rdquo
HSEProspectus
2009 Adult Critical Care Report
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Levels of Critical Care
Joint Faculty of Intensive Care Medicine of Ireland (JFICMI) National Standards define
Critical Care Service
ldquoappropriate for the care of patients requiring Level 2 3 and 3(s) critical carehellipgenerally delivered within a High-Dependency Unit (HDU) or Intensive Care Unit (ICU)rdquo
HSEProspectus
2009 Adult Critical Care Report
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Joint Faculty of Intensive Care Medicine of Ireland (JFICMI) National Standards define
Critical Care Service
ldquoappropriate for the care of patients requiring Level 2 3 and 3(s) critical carehellipgenerally delivered within a High-Dependency Unit (HDU) or Intensive Care Unit (ICU)rdquo
HSEProspectus
2009 Adult Critical Care Report
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
HSEProspectus
2009 Adult Critical Care Report
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Critical Care Programme Hospital Group lsquohub-and-spokersquo
Critical Care Model
CCS = Critical Care ServiceCritical Care Retrieval- safe inter-hospital critically ill patient transportNational Ambulance Service NAS Pre-Hospital Emergency Care PHEC transport and bypass procedures
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Ennis Mallow Tallaght Galway
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
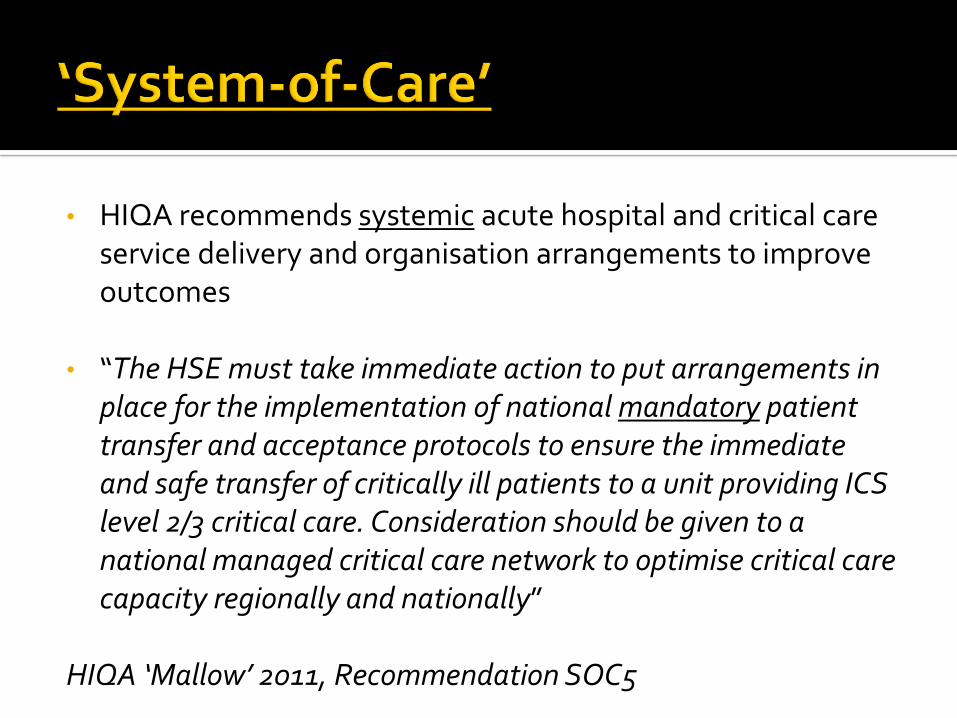
bull HIQA recommends systemic acute hospital and critical care service delivery and organisation arrangements to improve outcomes
bull ldquoThe HSE must take immediate action to put arrangements in place for the implementation of national mandatory patient transfer and acceptance protocols to ensure the immediate and safe transfer of critically ill patients to a unit providing ICS level 23 critical care Consideration should be given to a national managed critical care network to optimise critical care capacity regionally and nationallyrdquo
HIQA lsquoMallowrsquo 2011 Recommendation SOC5
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
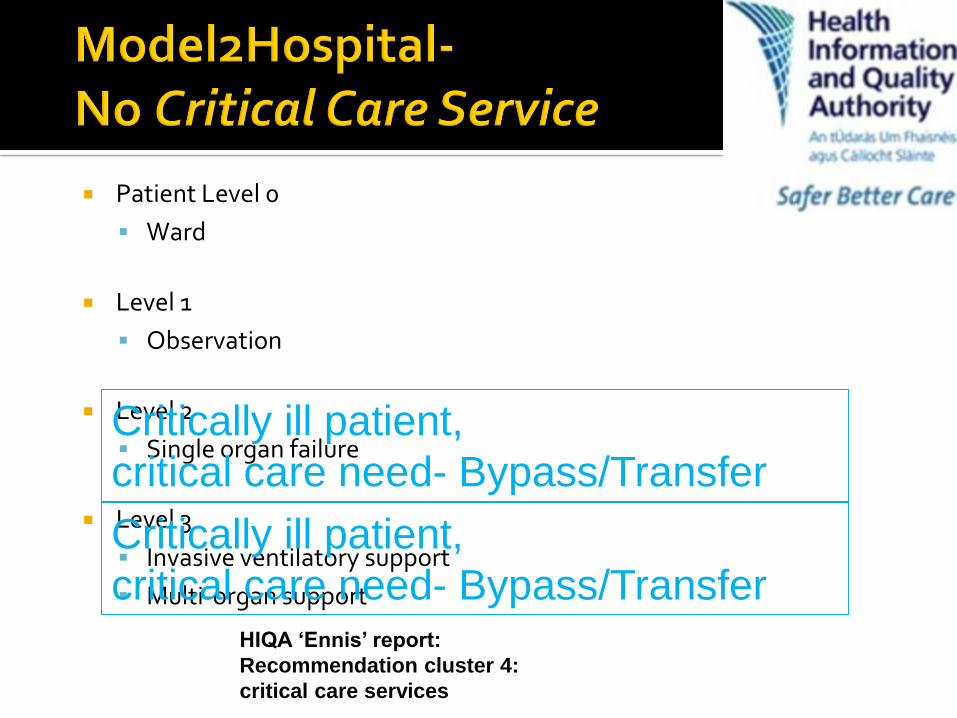
Patient Level 0
Ward
Level 1
Observation
Level 2
Single organ failure
Level 3
Invasive ventilatory support
Multi-organ support
Critically ill patient
critical care need- BypassTransfer
Critically ill patient
critical care need- BypassTransferHIQA lsquoEnnisrsquo report
Recommendation cluster 4
critical care services
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
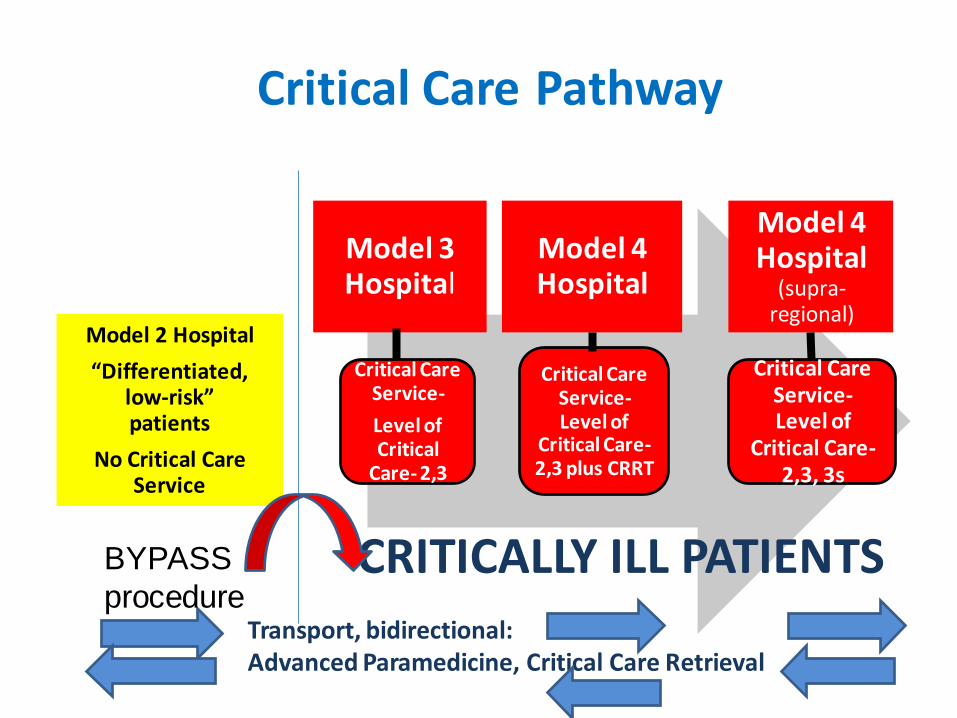
Critical Care Pathway
Critical Care Service-
Level of Critical
Care- 23
Critical Care Service-Level of
Critical Care-23 plus CRRT
Critical Care Service-Level of
Critical Care-23 3s
Model 3 Hospital
Model 4 Hospital
Model 4 Hospital
(supra-regional)
Model 2 Hospital
ldquoDifferentiated low-riskrdquo patients
No Critical Care Service
Transport bidirectional Advanced Paramedicine Critical Care Retrieval
CRITICALLY ILL PATIENTSBYPASS
procedure
Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

Fragmentation
ldquoAll politics is localrdquo Senator Thomas P ldquoTiprdquo OrsquoNeill Speaker US House of Representatives 1977-86
Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

Public policy- decentralisation or lsquosubsidiarityrsquo
bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

bull lsquoThe Health Service Reform Programme announced in June 2003 represents the most ambitious programme of change for the Irish health system in over 30 yearsrsquo
bull lsquomain elementrsquo ndash lsquomajor rationalisation of existing health service agencies to reduce fragmentationrsquo
bull Should the Government Statement not read lsquoin over 75 yearsrsquo
bull Does lsquorationalisationrsquo mean integration or centralisation
These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

These are my principles
If you donrsquot like themhellip
Wellhellip I have others
Groucho Marx
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Centralisation and decentralisation public policies can impact greatly on critical care delivery
Acute healthcare systemlsquoCounty jerseyrsquo fragmentation -v- andRationality integration centralisation
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
ldquoToo many institutions must not be allowed to specialise along the same lines to the neglect of other less popular branches of curative medicine The central specialised hospitals must be made available for all and the poor must get the use of them free The local hospitals must be developed to afford the maximum of utility without a high degree of specialisation and their geographical organisation must be carefully plannedrdquo
Dr FC Ward Parliamentary Secretary [Junior Minister for Health] to the Minister for Local Government and Public Health Second (Committee) Stage Public Hospitals Bill Daacuteil Debate 28th April 1933
Strategy- Commissioning access affordability tiering geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Hospitalsrsquo Commission
1936 (published)
Rare Book Archive TCD
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
lsquoDISTRICT HOSPITALSrsquo
lsquoCOUNTY HOSPITALSrsquo
lsquoREGIONAL HOSPITALSrsquo
lsquoMAIN HOSPITAL CENTRESrsquo
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
1968 lsquoFitzgeraldrsquo Report
ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

ldquoReforming the organisation of hospital servicesrdquo
ldquoThere is convincing evidence that the best results in treatment are achieved when patients are treated by staff working as part of a multi-disciplinary specialist team and that better clinical outcomes are achieved in units with appropriate numbers of specialist staff with relevant skills and experience high volumes of activity and access to appropriate diagnostic and treatment facilitiesrdquo
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
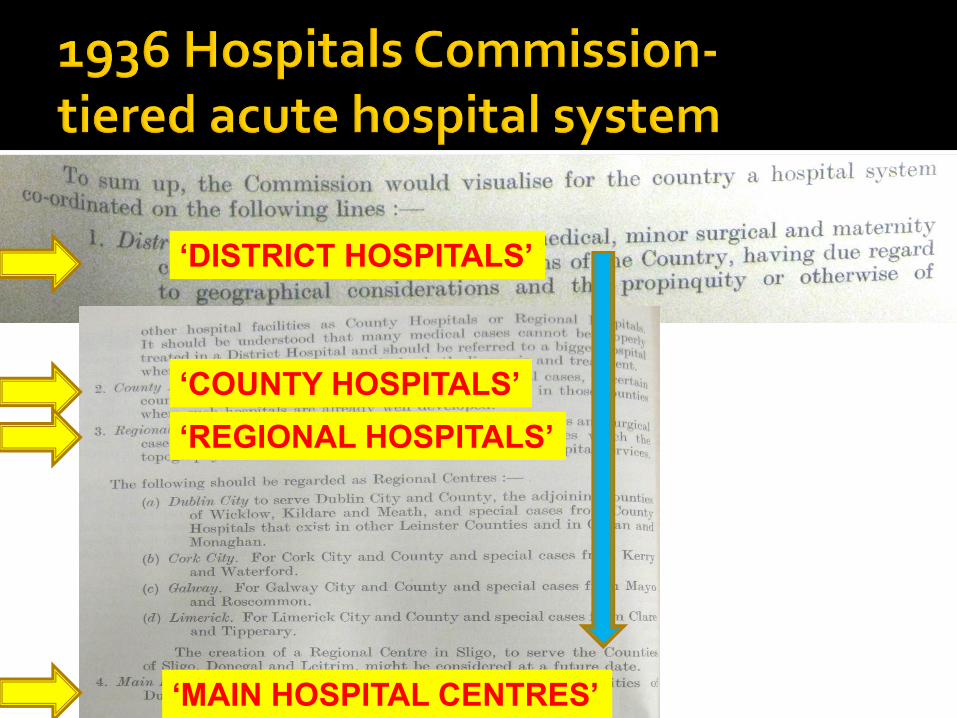
Acute hospital emergency care
No
Yes
Yes
Yes
1 1936 Hospitals Commission
2 1968 lsquoFitzgeraldrsquo Report
3 2003 lsquoHanlyrsquo Report
4 2013 HospitalModels and Smaller Hospital Framework
lsquoDistrict Hospitalrsquo
lsquoDistrict Hospitalrsquo
lsquoLocal Hospitalrsquo Model 2
lsquoCounty Hospitalrsquo
lsquoGeneralHospitalrsquo
lsquoGeneral Hospitalrsquo
Model 3
lsquoRegionalHospitalrsquo
lsquoRegional Hospitalrsquo
lsquoMajor Hospitalrsquo Model 4
lsquoMain hospital centrersquo
lsquoMedical teaching centrersquo
lsquoNational and supraregionalservicesrsquo Major Hospital
Model 4 supraregional national
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Countervailing local political forces
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Crowds protest closure of Bantry General
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Thousands protest cuts at Navan Hospital
2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

2000 protest against Portlaoise hospital cutbacks
Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

Big bang
MosaicIncremental
Blueprint
SimultaneousGradual PACE
SCALE
2012 HSCA2003-2013-
1936
1947
1953
1970
2003
1991-2010
Tuohy lsquoaccidental logicrsquo of healthcare organisation
Large
Small
2010 PPACA
Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

Out-of-hospital cardiac arrest Trauma Acute stroke care Critical care
London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

London Ambulance Service LAS- pop 8m Clinical pathways ldquoChain-of-Survivalrdquo and
ldquoHeart Attack Hospitalrdquo
Bystander CPR AED deployment
Fast pre-hospital emergency care response and hospital bypass procedure
Extra 222 patients ldquosurvived to hospital dischargerdquo in 5 years (VF survival- 12 increased to 32)
Editorial- ldquoIt takes a system to save a victimrdquoFothergill Resuscitation 2013
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Stages Advanced Paramedicine
for life-threatening conditions inc home field workplace nursing home urban rural and remote locations
Resuscitation Bystander and Early CPR Early defibrillation AED
Transport Acute Hospital- ED
ICU and critical care Therapeutic hypothermia
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
If a public access defibrillation programme is introduced in Ireland it should be considered in conjunction with measures to increase the utilisation of publicly accessible AEDs such as increased public awareness expanded CPR and AED training and an EMS-linked AED register Any prospective programme should start by targeting the mandatory deployment of AEDs to locations with the highest incidence of out-of-hospital cardiac arrest
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Hyper-acute
stroke unit
HASU
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Mortality at RLH decreased from 2000 to 2005 by 48 from 342 to 179
specialist trauma service 2003
direct local hospital ED referral to RLH trauma service was associated with a 53 decrease in mortality
Davenport BJS 2010
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
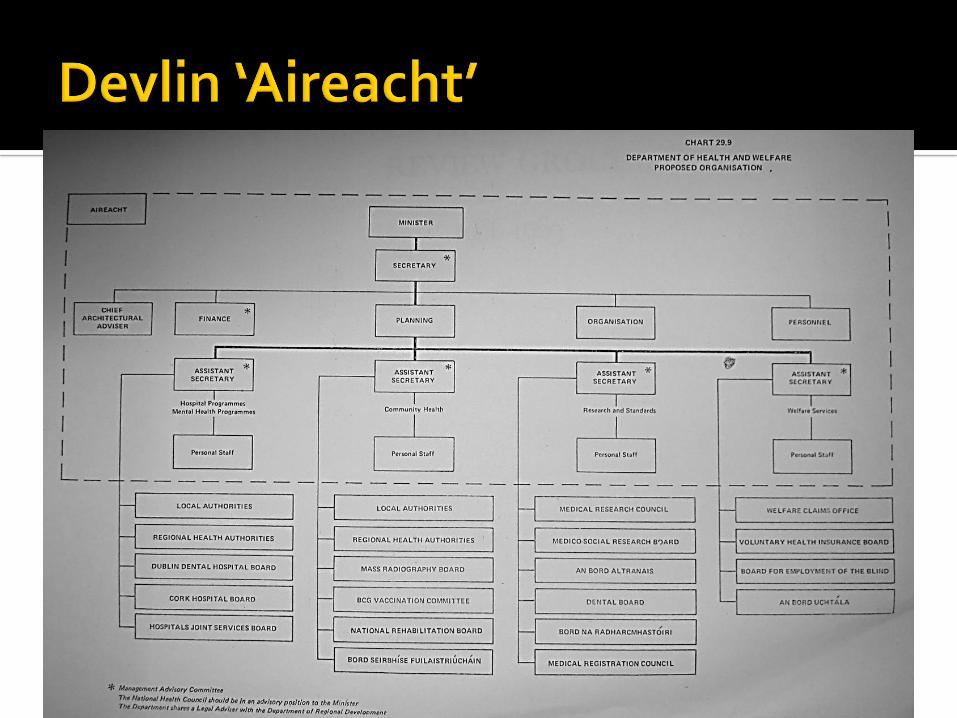
Performance improvement
The use of data and information Process and practice changes Planning Communication and engagement Leadership and Governance
DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

DGH District General Hospital
NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

NHS FIVE YEAR FORWARD VIEW 2015
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
Radical upgrade in prevention and public health
When people do need health services patients will gain far greater control of their own health care
The NHS will take decisive steps to break down the barriers in how care is provided
Multispecialty community provider
Primary and Acute Care Systems
Urgent and emergency care services
Smaller hospitals Primary Care National Leadership Meaningful local flexibility Innovation
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
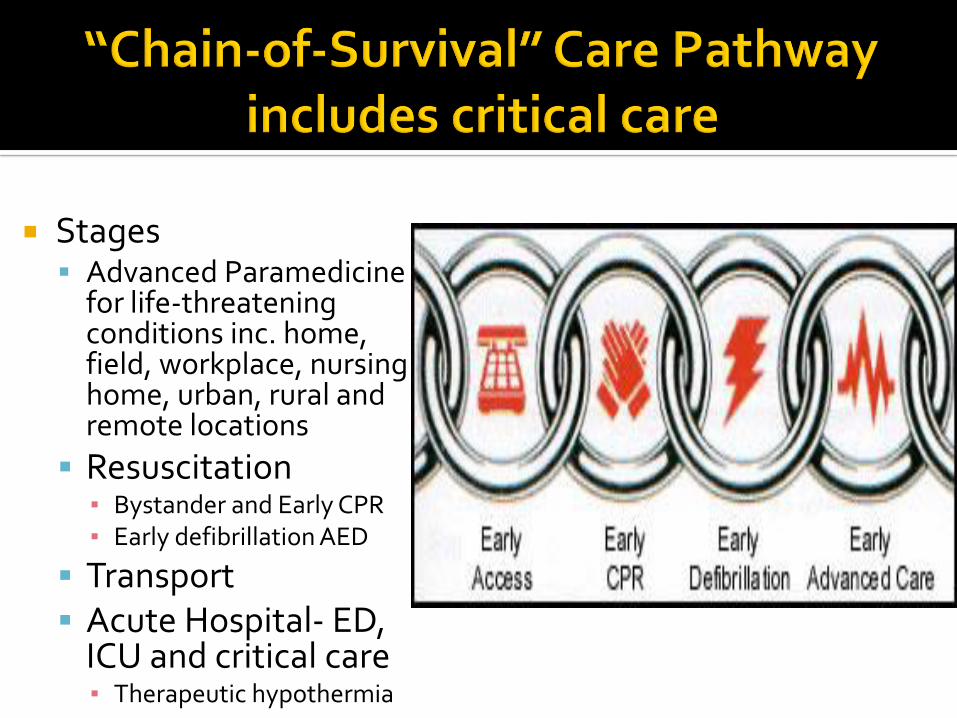
Smaller Hospitals
ldquoEngland is too diverse for a one size fits all care model to apply everywhere But nor is the answer to let lsquoa thousand flowers bloomrsquo Different local health communities will instead be supported by the NHSrsquo national leadership to choose from amongst a small number of radical new care delivery options and then given the resources and support to implement them where that makes senserdquo
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
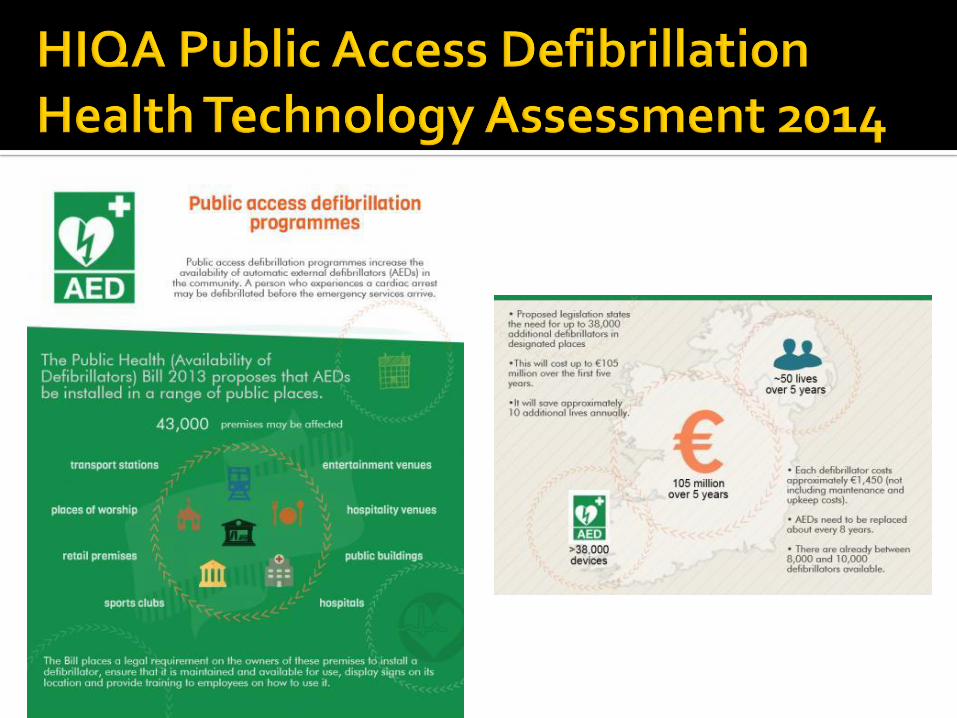
ldquoMajor trauma which is dealt with regionally
Emergency intervention most commonly associated with the 999 ambulance service and
Urgent care Out of Hours care where a difficulty exists but it does not initially present as life threatening and includes minor injuriesrdquo
Transforming Your Care TYC 2011
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
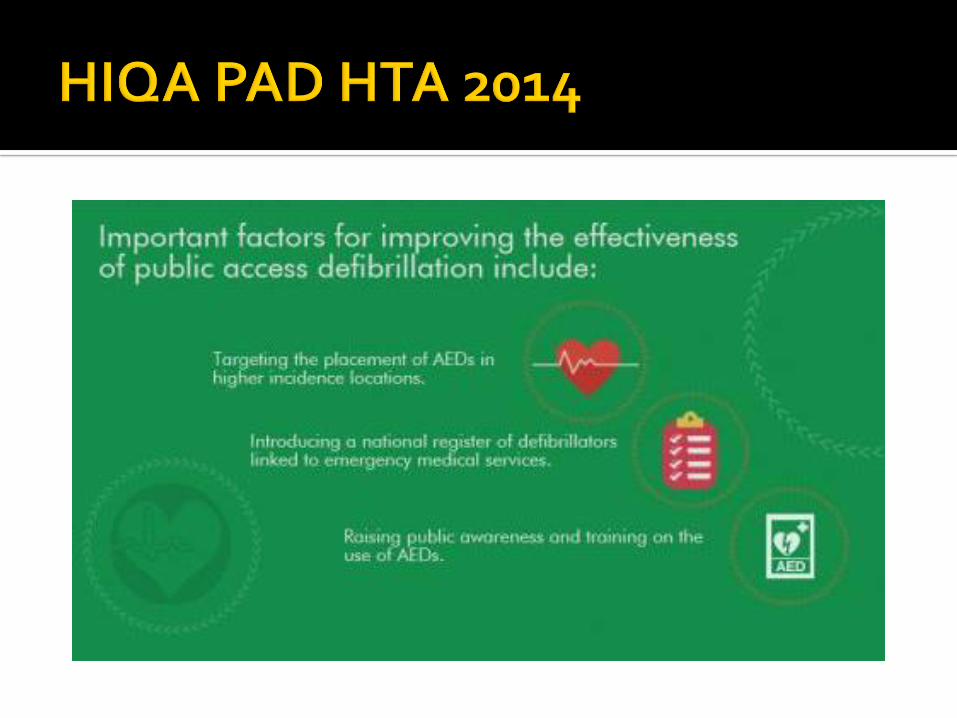
bull 1 Critical Care Model
bull 2 Irish healthcare politics
bull 3 lsquoMacrorsquo delivery evidence
bull 4 lsquoMacrorsquo delivery policy elsewhere
Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography

Evidence
Learning
Knowledge
Innovation
Design
Commissioner
Model
Context
Voluntary sector
Decentralisation legacy
Finance mechanisms
Organisation hierarchy
Capacity Capability
bull Funding
bull Communication Engagement
bull Governance
bull Leadership
bull Process
Activity
Outputs
Outcome
bull Survival
bull Impact
bull Performance
bull Accountability
bull Legitimation
bull Data Information
bull Value
bull Improvement
bull Ethic
bull Equity
GovernmentRegulationLegislation
Inputs
Structure- INTEGRATOR
Process- TRANSFORMATION
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
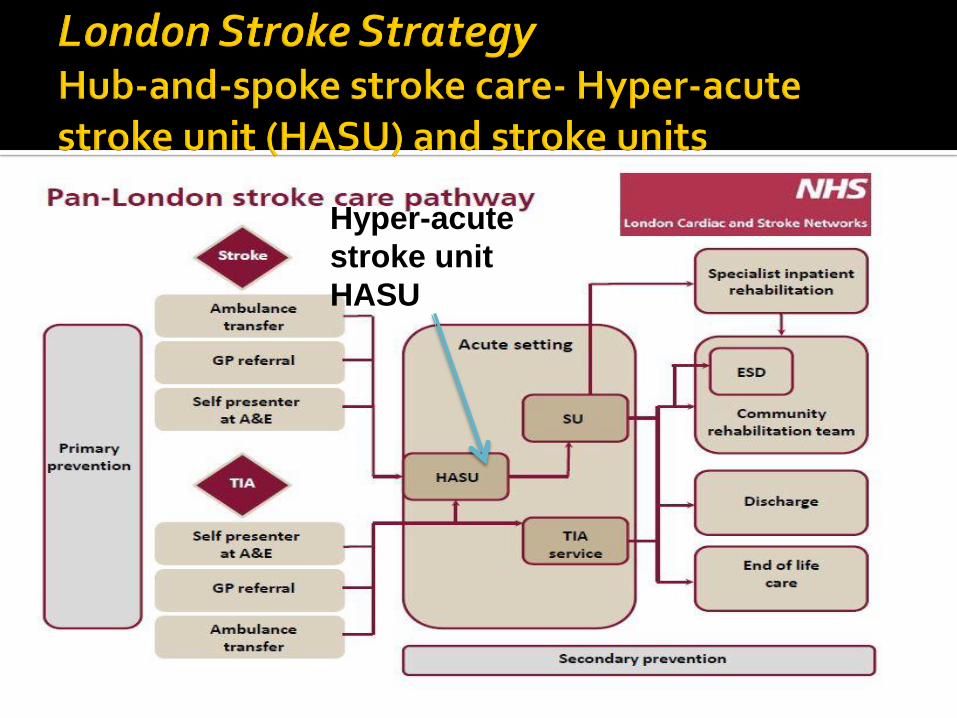
Different hospital site
System Transport Retrieval
Elective surgeryAmbulatory (lsquobasketrsquo) surgery
Same hospital centre
EmergencyUrgent
Major deferred complex surgery
Sametime-criticalunscheduled
Different time
Space
Time
Towill 2005
Hospital Chain structure
Johari window
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
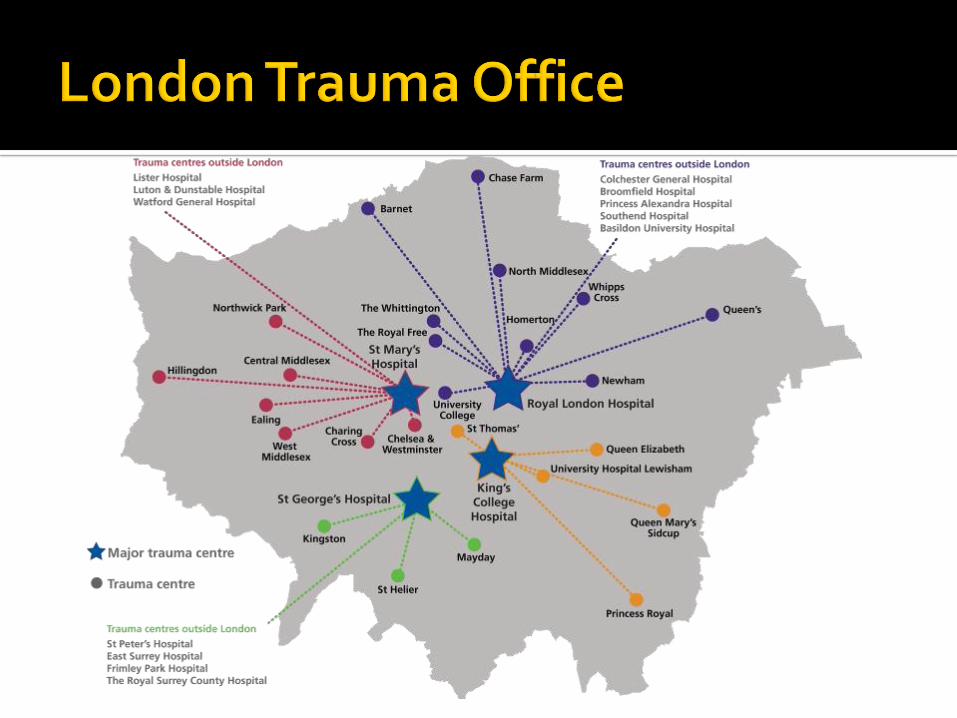
Organisation
integration
Service
integration
Functional
integration
Clinical
integration
Clinical and service integration
The route to improved outcomes
Curry amp Ham 2010
Integrated care
to the patient
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
lsquoThe health reforms introduced by DH
showed a clear determinationhellip
to decentralise healthcarersquo (p9)
Financial Secretary to the Treasury
Minister of State at Communities and Local Government
with responsibilities for Decentralisation and Planning Policy
Director of Policy for the Conservative Party 2012
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography
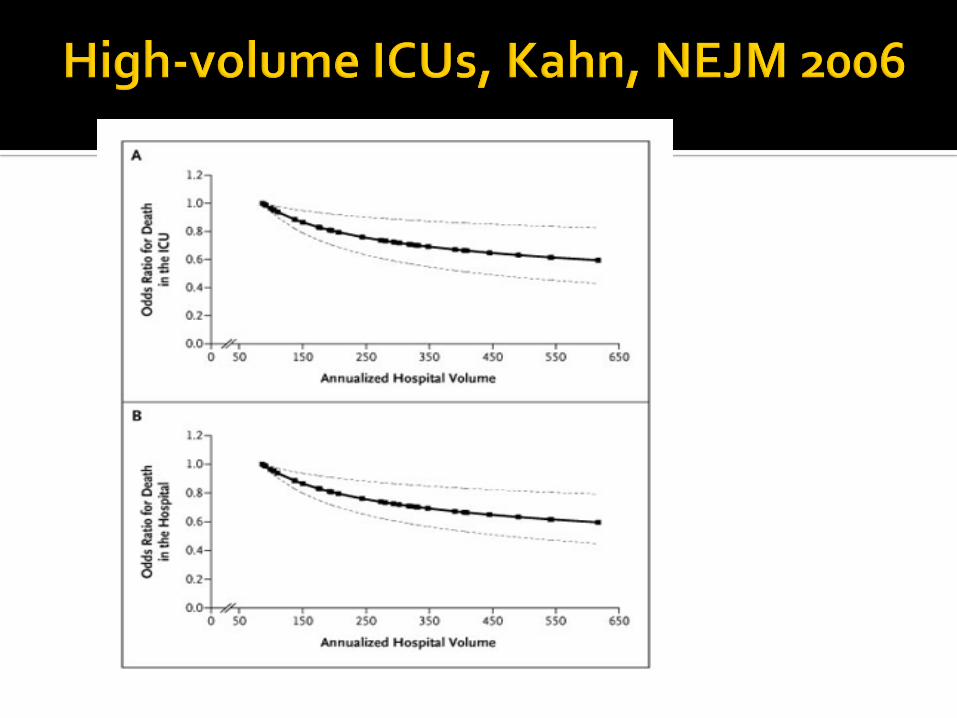
Integration is a coherent set of methods and models on the funding administrative organisational service delivery and clinical levels designed to create connectivity alignment and collaboration within and between the cure and care sectors The goal of these methods and models is to enhance quality of care and quality of life consumer satisfaction and system efficiency for patients with complex long term problems cutting across multiple services providers and settings The result of such multipronged efforts to promote integration for the benefit of these special patient groups is called lsquointegrated carersquo
Kodner et al 2002
Integration crosses the boundaries of healthcare
governance delivery finance professions and geography