dr. mahesh patwardhan complications of laparoscopic surgery
TRANSCRIPT

www.slh.nhs.uk
Complica)onsoflaparoscopicsurgery
Mr Mahesh Patwardhan M.D., F.R.C.O.G.
Consultant Laparoscopic Surgeon South East London NHS Healthcare
London, U.K.

What is a complication? l A Complication is a concurrence of various
causes and conditions in the course of surgical procedure, which do not normally form part of it and which usually make it more serious.
l Historical Evolution of the risks of complications
Period Laparoscopic Surgery
Complications
’70 – ’85
Initial Period Due to Technique
’85-’90 Development Due to indications ’90- date
Globalisation Due to Surgeon

Patterns of Risk factors
l The use of incorrect or unfamiliar instruments.
l First and subsequent access routes. l Surgical Technique and alternative route. l Electrosurgical applications. l Level of proficiency of the surgical team.

Learning the correct technique – the governance side!
l Successful results of laparoscopic surgery are essentially accomplished by good technique and application of ergonomic principle.
l .

System in U.K.
l U.K. – Single standardising body (R.C.O.G.)
l Advising bodies – B.S.G.E., NICE. l Advanced and intermediate level
certification. l Training period – Minimum number. l Private sector – Practices have to be
consistent with NHS practice. l Compulsory approved training courses. l G.M.C.

Complications related to Access entry
l Veress needle or direct entry?
l Umbilical port or Palmer’s point.
l Metal ports or newer ports?
l Correct entry and placement of the second port.
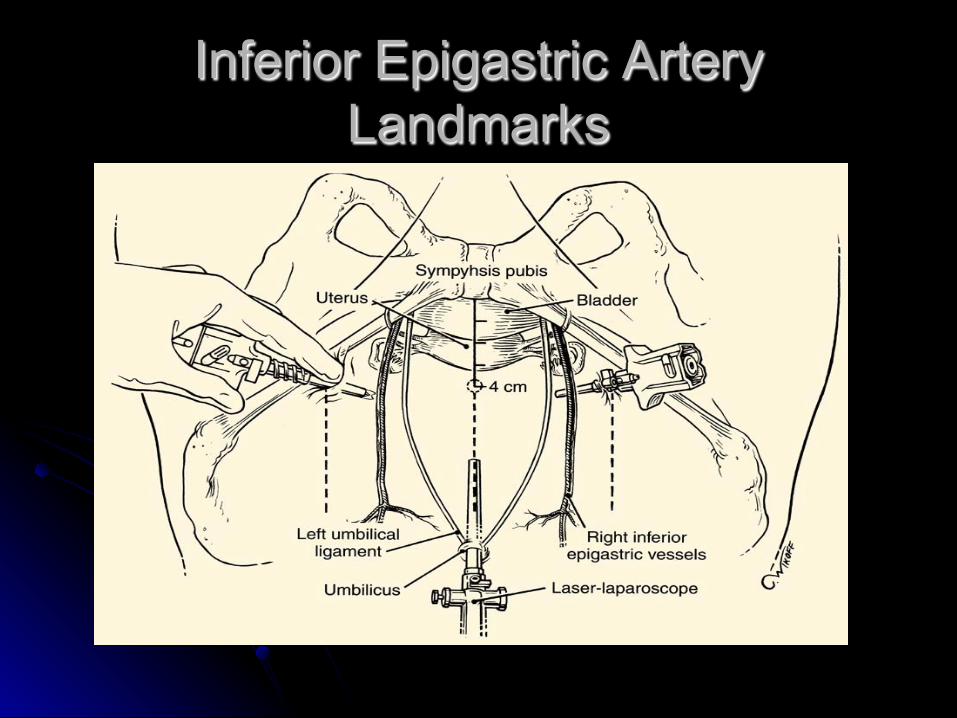
Inferior Epigastric Artery Landmarks

Inferior epigastric - Anatomy

Inferior epigastric artery

Phipp’s Needle

What to do?
l Phipp’s Needle. l Endocatch. l Deep Suture. l Foley’s catheter. l Suturing under direct
vision.

Injury due to port entry
l Injury to bowel – serosal, complete, small / large bowel.
l Injury to major vessel such as aorta, common iliac, external iliac etc.
l Surgical emphysema.

What to do?
l Bowel Injury – Most important – identification.
l Laparoscopic suturing only if proficient. l Major Vessel Injury - call for help. l Pressure to stop the loss. l Always a multidisciplinary approach. l Correct documentation and
communications.

Port Hernias l Larger Ports –
Morcellator. l What to do? l Prevention – Phipp’s
Needle, Endocatch, J Shaped Needle.
l If Recognised early, - Jet wash to separate, check viability
l Multidisciplinary approach
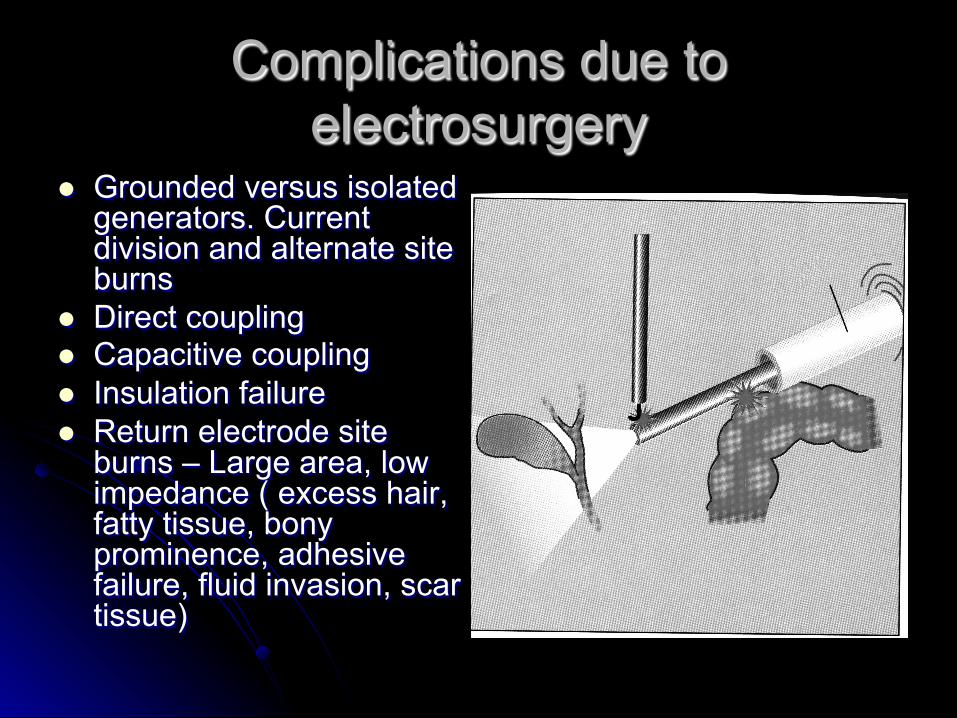
Complications due to electrosurgery
l Grounded versus isolated generators. Current division and alternate site burns
l Direct coupling l Capacitive coupling l Insulation failure l Return electrode site
burns – Large area, low impedance ( excess hair, fatty tissue, bony prominence, adhesive failure, fluid invasion, scar tissue)

ACTIVE SURGICAL TEMPERATURES
Vaporization of water dessicates tissues
Eschar forms when tissues burn
Eschar (oxidation)
Protein Coagulation
Proteins disorganize to form a coagulum
HARMONIC Electrosurgery/Laser Surgery
50º C 100º C 150º C 400º C+
Tissue Dessication

Amaral JF, Chrostek CA. SAGES, 1995.
0
10
20
30
40
50
60
70
Time (sec)
Lateral spread
(cc²)
Electrosurgery
UltraCision
0 1 2 3 4 5 6 7 8 9 10
LATERAL SPREAD OF COAGUALTION

What to do?
l Many of these are unrecognised at the time.
l Awareness. l Risk reporting. l Use of disposable instruments wherever
possible. l Knowledge of electrosurgical principles.

Unfamiliar tools in inexperienced hands!
l Morcellator. – Paediatric complication in Oxford.
l Lap Loop. l Unnecessary use of
traumatic graspers l Advanced laparoscopic
surgery – should it be allowed without proper training?

Complications due to procedure.
l Cauterisation of endometriosis – ureteric injuries. l Adhesiolysis – Bowel injuries. l Myomectomy – Bleeding l Colposuspension – Bladder injuries. l Laparoscopic Hysterectomy – Bleeding form the
uterine arteries, bladder injuries. l Laparoscopic sacropexy, pelvic lymph node
dissection – Injury to major vessels, bowel, ureter

Intra operative resolution of complications
l Correct diagnosis l Knowledge of the limits of laparoscopic
surgery – Avoiding cowboy approach! l Maximum coordination of surgical team l Appropriate complexity of the admitting
hospital l Multidisciplinary approach.

Causing awareness!
l Those who do not have complications either do not operate or they conceal them and therefore do not publish them!
Causing awareness
l The best way to treat the complications is to recognise them and the best way to recognise is to show it to the medical community.

Prevention
l Balance between indications, technical abilities and instruments
l Team work l Safety standards valid during surgery l Awareness that the complications exist! l Training and education. l Informed consent and appropriate
documentation

Role of responsible bodies
l Standardisation across the country.
l Certification. l Mandatory training
courses. l Regular auditing of
practices. l Revalidation.

Thank you
… any questions?