dr liz mcdonald dr katy brett - gp cme south/sat_room7_0830_macdonald_liz... · please see this 34...
TRANSCRIPT

Dr Liz McDonaldPerinatal Psychiatrist
University of Otago Senior
Researcher
Canterbury DHB
8:30 - 9:25 WS #69: Perinatal Mental Health: Changing the Face of the Future
9:35 - 10:30 WS #79: Perinatal Mental Health: Changing the Face of the Future
(Repeated)
Dr Katy BrettChristchurch

Perinatal Mental Health for GPs
Dr Liz Macdonald Perinatal Psychiatrist/Clinical Head
Dr Katy Brett Perinatal Psychiatrist
Mother and Baby Service
South Island Perinatal Mental Health Service

“Helping mothers of
young families with
psychiatric problems, is
one of the main
challenges for the
mental health services:
it also provides one of
the best opportunities
for a preventive
approach.”
Brockington, 1996.

Perinatal Mental Health for GPs
• Mothers and Babies Service – who are we?
• Why Perinatal Mental health is important
• Management in primary care including medications
• Who , when and how to refer
• Bipolar Disorder
• Remembering the infant…..
• Some useful resources

Mothers and Babies Service Who are we?
• Specialised Mental Health Service – South Island
• Multidisciplinary
• Mothers/ caregivers with complex moderate to severe mental illness
• Pregnant women from second trimester , and women with babies up to one year old.
• Women with severe illness considering pregnancy
• Not for women where substance abuse is the primary difficulty (GAP!)
• Referrals from GPs, Other mental health services in Canterbury and SI, hospital doctors e.g. obstetricians, paediatricians.

Treatments offered…….
• Preconception counselling • Phone prescribing advice• Assessment - diagnostic clarification• Case management • Mental health Birth Plans • Psychological therapies/ medication/ Physio• Support with Bonding and Attachment - some limited resource for
specialised mother infant therapy• 5/6 bedded Mother Baby Unit for South Island • Regional – consultation/ admission/ education via local Mental Health
Service

Up to 20% of women will develop a mental illness around pregnancy and postpartum

Why is perinatal mental health important..
• All mental health disorders can present during pregnancy and postpartum.
• The risk of suffering a psychiatric illness is higher after childbirth than at any other stage of life
• Anxiety and depression rates elevated
• Impact of maternal illness on infant and children both in pregnancy and postpartum
• Suicide is the leading cause of maternal death in NZ

Pregnancy
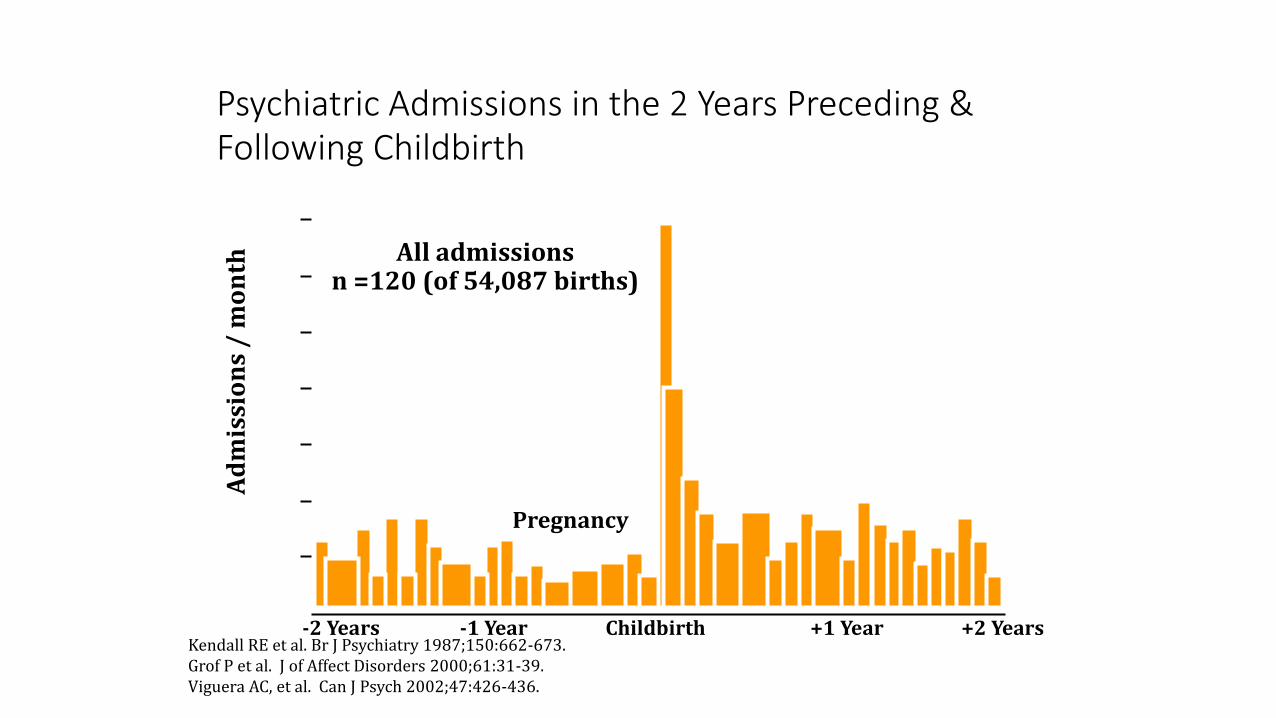
Psychiatric Admissions in the 2 Years Preceding & Following Childbirth
-2 Years -1 Year Childbirth +1 Year +2 Years
Ad
mis
sio
ns
/ m
on
th All admissionsn =120 (of 54,087 births)
70
60
50
40
30
20
10
Kendall RE et al. Br J Psychiatry 1987;150:662-673. Grof P et al. J of Affect Disorders 2000;61:31-39. Viguera AC, et al. Can J Psych 2002;47:426-436.

Specific Disorders
• Postnatal depression 10-15%
• Antenatal depression 10%
• Anxiety 15%
• Panic disorder/OCD/tokophobia 5-10%
• PTSD 1.5-6%
• Personality disorders 15-20%
• Eating disorders
• Bipolar Disorder – 50% relapse in postpartum
• Serious postpartum disorder 2-4% (psychosis 0.5% )
• Chronic Enduring Serious Mental Illness e.g. Schizophrenia

Primary Care Management
• Assessment inc rating scales e.g. Edinburgh Postnatal Depression Scale
• Psycho -Education – e.g. PADA website
• Counselling – e.g Brief Intervention Counselling , low cost community options, private psychology
• Community supports
• Collaborate with LMC and other providers
• Medication
• Consult / refer Mothers and Babies…..
Community Services
• Mother : Referral to Post Natal Adjustment Programme ( Plunket) , Peer Support PND Canterbury
• Parenting support : Early Start ( Canterbury), Waipuna ( mothers up to 24 yrs old)
• Mother infant relationship - PPAIRS ( Circle of security programme Plunket) , Infant Mental Health Service at Child and Family Service
• Practical supports – e.g. Bellyful
• Community Support worker

Maori community resources
• Pura Pura Whetu Counselling and whanau ora servies including TeOriori ( parenting support for whanau with children up to age 7)
• Te Runanga O Nga Mataawaka - Mother & Pepi : Maori mothers with children 0-2 with no support networks
• Te Puna Oranga – 24 hour manaaki ( crisis/ support), Counselling incACC, parenting , treatment relating to sexual abuse, whanau mediation 0800 222 042

Prescribing in pregnancy / breastfeeding

Effect of illness on pregnancy outcome
Prescribing…
• Case by case basis
• Indications – complex moderate to severe depression - NOT mild
• Full documented discussion of potential risk and benefits inc written material
• Lowest effective dose
• Avoid polypharmacy
• Consult – websites e.g. mothertobaby.org , BUMPS medicinesinpregnancy.org
• Medicines Information 0800 DRUGINFO (378446)
• Mothers and Babies 033377708

Local guidelines for managing psychotropics during pregnancy and breastfeeding …..
• Covers basic prescribing principles
• How to manage antidepressants and benzodiazepines around birth
• Neonatal adaptation syndrome
• Table on specific medications with reference to antenatal / newbornand feeding
• Will be on Health Pathways – draft copy as handout
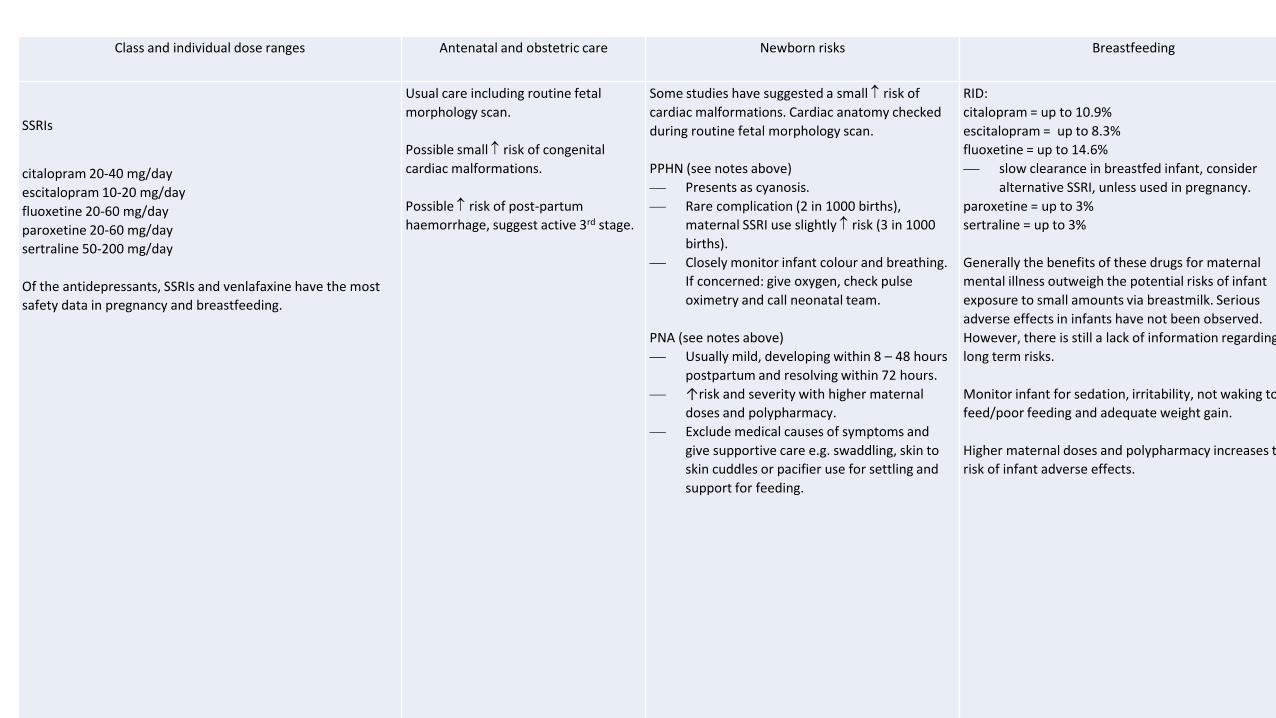
Class and individual dose ranges Antenatal and obstetric care Newborn risks Breastfeeding
SSRIs
citalopram 20-40 mg/day
escitalopram 10-20 mg/day
fluoxetine 20-60 mg/day
paroxetine 20-60 mg/day
sertraline 50-200 mg/day
Of the antidepressants, SSRIs and venlafaxine have the most
safety data in pregnancy and breastfeeding.
Usual care including routine fetal
morphology scan.
Possible small risk of congenital
cardiac malformations.
Possible risk of post-partum
haemorrhage, suggest active 3rd stage.
Some studies have suggested a small risk of
cardiac malformations. Cardiac anatomy checked
during routine fetal morphology scan.
PPHN (see notes above)
⎯ Presents as cyanosis.
⎯ Rare complication (2 in 1000 births),
maternal SSRI use slightly risk (3 in 1000
births).
⎯ Closely monitor infant colour and breathing.
If concerned: give oxygen, check pulse
oximetry and call neonatal team.
PNA (see notes above)
⎯ Usually mild, developing within 8 – 48 hours
postpartum and resolving within 72 hours.
⎯ ↑risk and severity with higher maternal
doses and polypharmacy.
⎯ Exclude medical causes of symptoms and
give supportive care e.g. swaddling, skin to
skin cuddles or pacifier use for settling and
support for feeding.
RID:
citalopram = up to 10.9%
escitalopram = up to 8.3%
fluoxetine = up to 14.6%
⎯ slow clearance in breastfed infant, consider
alternative SSRI, unless used in pregnancy.
paroxetine = up to 3%
sertraline = up to 3%
Generally the benefits of these drugs for maternal
mental illness outweigh the potential risks of infant
exposure to small amounts via breastmilk. Serious
adverse effects in infants have not been observed.
However, there is still a lack of information regarding
long term risks.
Monitor infant for sedation, irritability, not waking to
feed/poor feeding and adequate weight gain.
Higher maternal doses and polypharmacy increases the
risk of infant adverse effects.

Starting an antidepressant in pregnancy
• Choice of antidepressant - what has worked in past?
• First line - Sertraline or Escitalopram
• Others:Venlafaxine, Paroxetine relatively higher risk neonatal withdrawal
• Fluoxetine higher amounts in BM and long half life
• TCAs Nortriptyline – effective but not well tolerated and less data
• Avoid MAOIs in pregnancy and breastfeeding

If already on antidepressant…
• Preconception counselling ideally…..
• Don’t stop suddenly! Relapse 68%
• What's the indication? Diagnosis and severity
• Response?
• Have they tried to come off it in past?
• If come off - gradually (months)and moniter
• To switch or not to switch…… EgFluoxetine - not necessarily
• Do not advise dose reduction around delivery 0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 12 24 36
Pro
pro
tio
n o
f P
atie
nts
R
em
ain
ing
We
ll
Gestational Age
Maintained (N=82)
Increased (N=20)
Decreased (N=34)
Discontinued (N=65)
Cohen et al. JAMA. 2006

Stopping antidepressants Horowitz MA, Taylor D
Tapering of SSRI treatment to mitigate withdrawal symptoms.
Lancet Psychiatry. 2019; 6: 538-546
• Withdrawal symptoms potentially much more severe for some people…Electric shock symptoms, flu like, mood changes - link to duration of treatment
• Taper antidepressants over much more extended periods of time than previously recommended for some people
• Follow patient’s symptoms
• Half the dose – wait until all symptoms subside before further reduction - can take weeks to years!
Night sedation
• Zopiclone - low dose. No evidence of increased effect above 7.5mg. Most data.
• Temazepam (avoid first trimester)
• Small doses 12.5-25mg quetiapine
• Antihistamines e.g. Promethazine
• Caution use late pregnancy - infant withdrawal/ adaptation syndrome
• Melatonin ?

Mood stabilisers – Sodium Valproate
• Sodium Valproate - malformations and developmental problems
• Contraindicated in pregnancy !!
• Should be avoided in women of child bearing age
• EMA 2018 - If used , should be on highly effective contraception (EU Pregnancy Prevention Programme)
• Folic acid 5mg daily

40 year old woman on sodium valproate 1000mg daily – diagnosis bipolar disorder but stable for over ten yearsHas just found out she is pregnant – what do we do?
• Taper and stop sodium valproate
• Start Folic acid 5mg daily
• Consider starting replacement mood stabiliser e.g. Olanzapine 5mg daily or wait and close moniter
• Refer to maternal mental health 2nd trimester
• Ensure LMC aware
• High risk obstetric clinic
• Detailed morphology scan at 16 and 20 weeks gestation at CWH through Maternal FetalMedicine

When to refer and how….

Who should definitely be referred?
• Mothers with major mental illness - even if currently well (Bipolar 1 disorder, schizophrenia, schizoaffective disorder, post partum psychosis, severe depression (i.e. prolonged hospital admission, psychotic symptoms, ECT)
• Refer from 2nd trimester onwards
• Mental Health Birth Plan – early 3rd trimester LMC/family/GP
• Women with severe mental illness or complex medication regimes for pre-natal counselling

“Alice had a severe post partum psychosis 2 weeks after the delivery of her first child. She
is pregnant again EDD x/x/x. She is in a much better space than she was at the time of
her sons birth. She is enjoying mother hood and is seeking IVF for a second child but has
conceived naturally this time. I understand that you recommended Alice be referred to
the unit when she became pregnant again”
Who else should be referred?
• Mothers with severe mental illness mood /anxiety/eating disorders with current symptoms.
• Mothers with moderate to severe mental illness and disrupted relationship with their baby
• Mothers on complicated medication regimes including mood stabilisers e.g. lithium , atypical antipsychotics

“please see this 34 yr old woman pregnant for the first time. She was diagnosed
as having Bipolar II disorder in the US and was commenced on lamotrigine which
she has been taking at a dose of 150 mg since then. Prior to that she was on a
number of medications but they were ineffective. Please advise re management
of lamotrigine in pregnancy…..”

Who might you refer?
Mothers with moderately severe mental illness that is complex e.g. • Dual diagnosis – E.g Concurrent diagnosis of Other mental health disorder,
Personality Disorder, Substance abuse (Not primary problem), History of trauma, low IQ….
• Disrupted Mother infant bonding /relationship
• Poor response to treatment or other medication issues

“Thank you for seeing this 29 yr old woman who is now in her second
trimester. She has a history of major depression starting as a teenager. After
being on venlafaxine for a time she has been on mirtazapine with good effect
since 2011. There have been times of more mild depressive episodes since,
including at times of trail of dose reduction. However since becoming
pregnant ( first time) she has struggled with low mood , tearfulness and
irritability. She has managed to continue work as a hairdresser but is
struggling. Her partner also suffers from depression.
She has continued on 45mg mirtazapine throughout pregnancy so far, and is
now 17 weeks. She has started BIC with no benefit. “

• “This lovely mother has presented to talk to me about her low mood and anxiety. This has been present since her baby was born 5 months ago. She at first thought it was hormonal but the symptoms seem to be worsening and persisting. She had some thoughts of harm to herself earlier on but this has settled now. She would really benefit from supports and some counselling please………”
• “LMC wants us to refer to mothers and Babies……..”
• “Feeling anxious and depressed – happened last pregnancy. Was worse then – felt
suicidal. Did not see psychiatrist and was not started on meds. Anxious husband will
leave her. Not currently suicidal. Sleeping well, appetite and energy normal – looking
forward to family visit……”

What needs to be in a referral to maternal mental health to get your patient seen?• Advice, assessment or treatment?
• Presenting Symptoms
• Has a trial of treatment been tried and failed?
• Past Psych History
• Family history
• Medications
• A&D
• Social situation
• Supports
• Ethnicity
• Bonding/attachment concerns
• RISK to self/others/baby

When you need to refer urgently….Urgent same day assessment by mental health services of
• Active Suicidal ideation / attempts
• Active thoughts of harm to baby
• Psychotic symptoms
• Mania
• Refer to Crisis resolution - 0800-477-792 (0800-GP-PSYC) during working hours Monday to Friday or 0800-920-092 and ask for Crisis Resolution.
• Tip: Emphasise vulnerability and risk to baby
Bipolar / Post Partum Psychosis
• 1 in 500 births
• Can be very predictable !
• At least 30- 50% chance relapse in first 4-6 weeks postpartum if Bipolar 1
• Risk increased if previous postpartum episodes or family history
• Elevated risk following first birth, infant mortality, obstetric complications
• Psychiatric emergency as risks very high
• Usually need hospitalised. Preferably in MB unit, will need close monitoring
• Preconception counselling and mental health birth plan required
• Trigger of sleep deprivation


What can the GP do?
• Identification of high risk women early on – refer preconception counselling with Mothers and Babies
• Women who are at high risk i.e.Bipolar 1 should be referred to MHS even if currently well
• Will need active medication management
• Mental health birth plan and close moniteringpostpartum
• If become involved in postpartum in acute onset of illness – treat as emergency and refer urgently
• Sleep!!!! - short term sleeping tabs, xpress milk, etc

And don’t forget the baby……

Pregnancy stress and pregnancy outcomes?
• Slightly shorter gestation, smaller head circumference
• Mixed handedness
• Increased childhood anxiety
• Increase in ADHD symptoms
(Glover et al, J.Child Psychology and Psychiatry,2007)
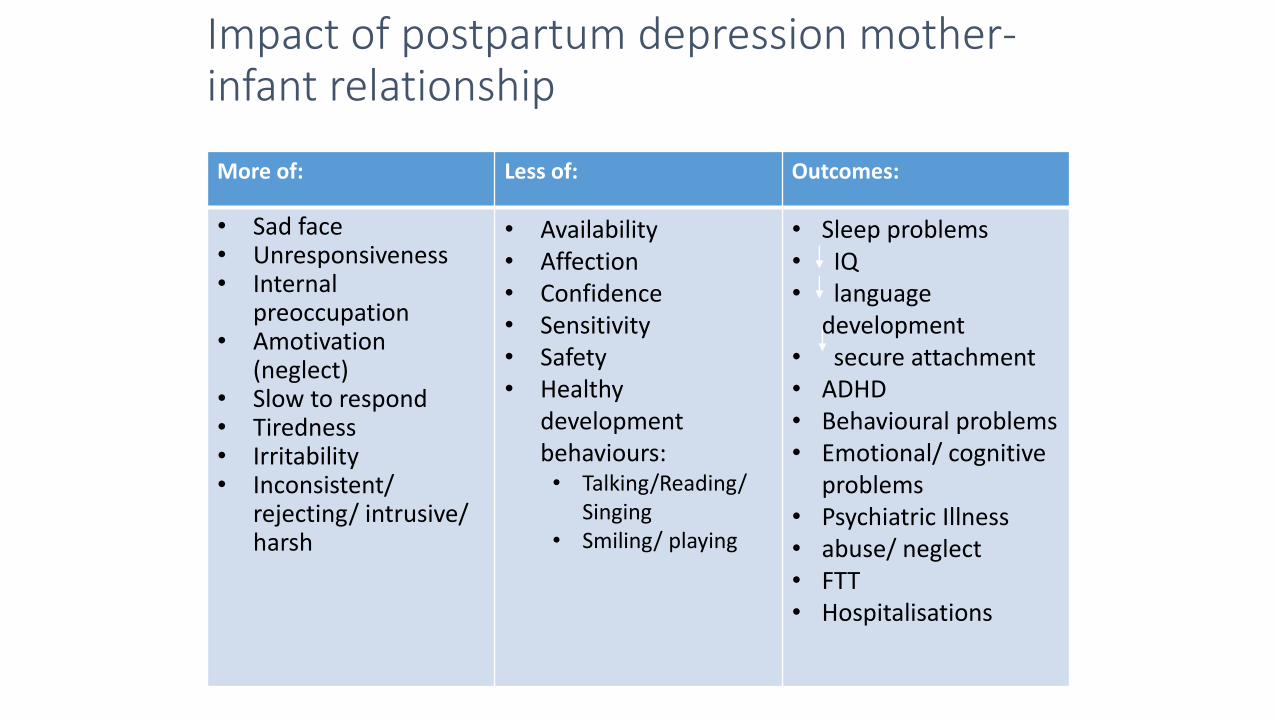
Impact of postpartum depression mother-infant relationship
More of: Less of: Outcomes:
• Sad face• Unresponsiveness• Internal
preoccupation• Amotivation
(neglect)• Slow to respond• Tiredness• Irritability• Inconsistent/
rejecting/ intrusive/ harsh
• Availability• Affection• Confidence• Sensitivity• Safety• Healthy
development behaviours:• Talking/Reading/
Singing• Smiling/ playing
• Sleep problems• IQ• language
development• secure attachment• ADHD• Behavioural problems• Emotional/ cognitive
problems• Psychiatric Illness• abuse/ neglect• FTT• Hospitalisations

What you might see / hear in your practice
• Mothers or cargiver rejecting or not bonding with their babies
• Frequent presentations with physical concerns
• Parents concerned about their toddler having a disorder e.g. autism / ADHD
• Presenting with infants / toddlers with e.g. feeding difficulties, sleep problems, anxiety…
• Child you can’t engage with / Overly familiar child

Christchurch Infant Mental Health Service
• ‘Fledgling Service’
• Referrals to CAF Link
• Under 5’s
• Thorough assessment inc preschool observations
• Currently receive most of referrals from GP
• Therapies include Theraplay, VIG, PCIT as well as parent education and support.

FATHERS
• Depression in fathers in the postnatal period is common, ( 8-10%.)
• High co-occurrence of mental health difficulties in partners of unwell women.
• Fathers reactions to partners illness and stress
• Relationships stresses and risks
• Paternal depression also has implications for children

Resources
• Guidelines on psychotropic medications during pregnancy and breastfeeding ( Draft)
• Contacts and referrals used by Mothers and Babies inc Maori organisations
• Apps and websites
