dr. l. telisinghe - who
TRANSCRIPT

PICO4 – preliminary results V1.7- 16th April 2014 1
Systematic review of the effect of antibiotics and/or vaccination in preventing subsequent disease among household contacts
of cases of meningococcal disease
Report for the WHO Meningitis Guideline Revision
May 2014
Dr. L. Telisinghe
Current position: The WHO control of epidemic meningococcal disease; practical guidelines 2nd edition
1998 (http://www.who.int/csr/resources/publications/meningitis/WHO_EMC_BAC_98_3_EN/en/) states that
1) Vaccination – mass vaccination campaigns can halt epidemics

PICO4 – preliminary results V1.7- 16th April 2014 2
2) Chemoprophylaxis – of contacts of cases of meningitis is not recommended during epidemics. In non-
epidemic settings, chemoprophylaxis is recommended to close contacts of a case including household
contacts.
However, recently during a large outbreak of serogroup W meningococcal meningitis in the Gambia, ciprofloxacin
was administered as chemoprophylaxis to close contacts of cases of meningococcal disease. In addition with
the use of the serogroup A polysaccharide-tetanus toxoid conjugated vaccine, the scale and frequency of
serogroup A meningococcal disease outbreaks in the meningitis belt is likely to decrease. Given these, the
WHO recommendation for the use of chemoprophylaxis and vaccination for the region needs to be reviewed and
updated, to ensure up to date, evidence based practice in the region.
Recommendation question: Should prophylaxis (antibiotics and/or vaccination) be recommended for
household contacts of cases of meningococcal meningitis in epidemic and non-epidemic settings?
PICO question: Among household contacts of a case, what is the risk of meningococcal meningitis during
the month after disease onset among close contacts given and not given prophylaxis?
Populations: Household contacts of cases of meningococcal meningitis
Intervention: Prophylaxis to household contacts
Comparator: No prophylaxis to household contacts
Outcome: Attack rate among household contacts within one month after disease onset in index case
Aim: To determine the effect of antibiotics and/or vaccination, in preventing subsequent meningococcal
disease in household contacts of cases of meningococcal meningitis, in epidemic and non-epidemic settings.
Objectives:
1) Conduct a systematic review of the literature using an appropriate search strategy.
2) Determine a combined estimate of the effect of appropriate antibiotics on the risk of subsequent
meningococcal disease among household contacts of cases of meningococcal disease at 30 days and 1 year
following the index case.
3) Determine a combined estimate of the effect of appropriate vaccination on the risk of subsequent
meningococcal disease among household contacts of cases of meningococcal disease at 30 days and 1 year
following the index case.
PICO4 – preliminary results V1.7- 16th April 2014 3
4) Determine a combined estimate of the effect of appropriate antibiotics and vaccination on the risk of
subsequent meningococcal disease among household contacts of cases of meningococcal disease at 30 days
and 1 year following the index case.
5) Determine the number needed to treat with antibiotics, vaccination, and, antibiotics and vaccination to prevent
one subsequent case of meningococcal disease among household contacts of cases of meningococcal disease
at 30 days and 1 year.
6) Explore drug resistance in isolates of Neisseria meningitidis from subsequent cases of meningococcal disease
given chemoprophylaxis.
7) Explore the proportion of household contacts given prophylaxis (both antibiotics and vaccination), who
develop side effects due to prophylaxis.
Methods: See protocol v1.6; 7th March 2014 for details of the study methods. Where methods differ from
proposed methods in the protocol – this is indicated in the document.

PICO4 – preliminary results V1.7- 16th April 2014 4
Results
Systematic review search
Figure 1: Search for systematic reviews (undertaken by LT, TW and JS)
*n=27(39.7%) had no abstracts; SR=systematic review
Records identified through
database search N=906
Records remaining after
duplicates removed n=718
Number of duplicates removed
n=188
Number of records excluded
following abstract screen n=128 Abstracts screened n=196
For full text screen n=68+12=80
Number of records excluded
following title screen n=522
Full texts screened n=64
Titles screened n=718
Unable to find articles n=16 3rd
review by RJS
Additional articles reviewed
based on reference search
n=12
Number of articles considered
n=4
Excluded
Not SR (i.e. reviews only) n=58
Older version of SR n=2

PICO4 – preliminary results V1.7- 16th April 2014 5
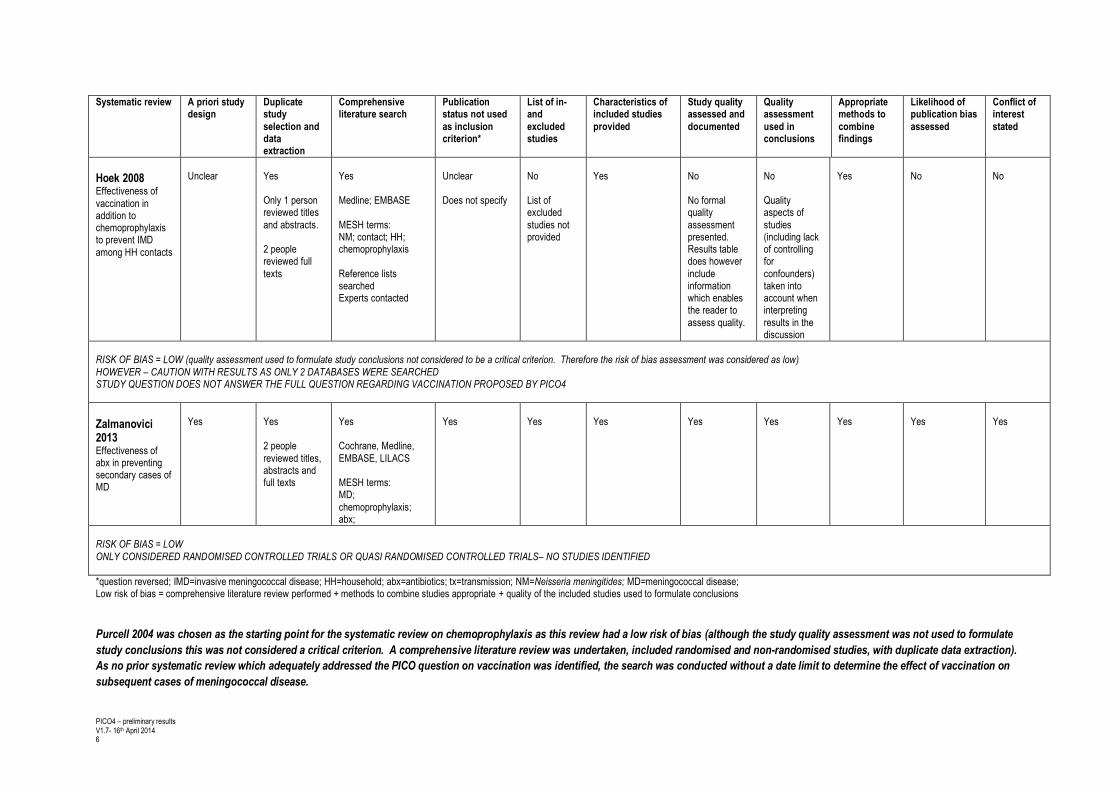
Table 1: Methodological quality assessment of systematic reviews using the AMSTAR tool
Systematic review A priori study design
Duplicate study
selection and data extraction
Comprehensive literature search
Publication status not used
as inclusion criterion*
List of in- and
excluded studies
Characteristics of included studies
provided
Study quality assessed and
documented
Quality assessment
used in conclusions
Appropriate methods to
combine findings
Likelihood of publication bias
assessed
Conflict of interest
stated
Purcell 2004 Effectiveness of chemoprophylaxis
Unclear
Yes 2 independent
data extractors
Yes Cochrane, HTA and
national research register (UK); Medline; EMBASE; CAB heath
Mesh terms for NM; chemoprophylaxis; abx; HH; outbreak; tx;
control Reference search Contacted experts
Unclear Does not specify
Did not exclude based on language, date,
country
No List of
excluded studies not provided
Yes
No No formal
quality assessment presented. However,
information is provided on the included studies, which
enables the reader to assess quality.
No Quality aspects
of studies (including lack of controlling for
confounders) taken into account when interpreting
results in the discussion
Yes
No
No
RISK OF BIAS = LOW (while study quality assessment was not formerly used in conclusions, this was not considered to be a critical criterion as there was duplicate study selection and data extraction and a comprehensive literature search performed, with studies not excluded based on language, country or date. Therefore the risk of bias assessment was considered low)
ECDC 2010 Guidelines: Public health management
of sporadic cases of invasive meningococcal disease and their contacts
Yes
No
Yes
Medline; EMBASE; Cochrane; Global Health
Mesh terms: NM; tx; outbreak; HH; chemoprophylaxis; abx
Reference search Contacted experts
Unclear
Does not specify
No
List of excluded studies not provided
Yes
No
No
Quality aspects of studies (including lack
of controlling for confounders) taken into
account when interpreting results in the discussion
Yes
No
Yes
RISK OF BIAS = NOT LOW (the risk of bias was considered as not low as duplicate study selection and data extraction was not performed)
PICO4 – preliminary results V1.7- 16th April 2014 6
Systematic review A priori study design
Duplicate study
selection and data extraction
Comprehensive literature search
Publication status not used
as inclusion criterion*
List of in- and
excluded studies
Characteristics of included studies
provided
Study quality assessed and
documented
Quality assessment
used in conclusions
Appropriate methods to
combine findings
Likelihood of publication bias
assessed
Conflict of interest
stated
Hoek 2008 Effectiveness of
vaccination in addition to chemoprophylaxis to prevent IMD
among HH contacts
Unclear
Yes Only 1 person reviewed titles
and abstracts. 2 people reviewed full
texts
Yes Medline; EMBASE
MESH terms: NM; contact; HH; chemoprophylaxis
Reference lists searched Experts contacted
Unclear Does not specify
No List of excluded
studies not provided
Yes
No No formal quality
assessment presented. Results table does however
include information which enables the reader to
assess quality.
No Quality aspects of
studies (including lack of controlling for
confounders) taken into account when interpreting
results in the discussion
Yes
No
No
RISK OF BIAS = LOW (quality assessment used to formulate study conclusions not considered to be a critical criterion. Therefore the risk of bias assessment was considered as low)
HOWEVER – CAUTION WITH RESULTS AS ONLY 2 DATABASES WERE SEARCHED STUDY QUESTION DOES NOT ANSWER THE FULL QUESTION REGARDING VACCINATION PROPOSED BY PICO4
Zalmanovici 2013 Effectiveness of abx in preventing secondary cases of MD
Yes
Yes 2 people
reviewed titles, abstracts and full texts
Yes Cochrane, Medline,
EMBASE, LILACS MESH terms: MD;
chemoprophylaxis; abx;
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
RISK OF BIAS = LOW
ONLY CONSIDERED RANDOMISED CONTROLLED TRIALS OR QUASI RANDOMISED CONTROLLED TRIALS– NO STUDIES IDENTIFIED
*question reversed; IMD=invasive meningococcal disease; HH=household; abx=antibiotics; tx=transmission; NM=Neisseria meningitides; MD=meningococcal disease; Low risk of bias = comprehensive literature review performed + methods to combine studies appropriate + quality of the included studies used to formulate conclusions
Purcell 2004 was chosen as the starting point for the systematic review on chemoprophylaxis as this review had a low risk of bias (although the study quality assessment was not used to formulate
study conclusions this was not considered a critical criterion. A comprehensive literature review was undertaken, included randomised and non-randomised studies, with duplicate data extraction).
As no prior systematic review which adequately addressed the PICO question on vaccination was identified, the search was conducted without a date limit to determine the effect of vaccination on
subsequent cases of meningococcal disease.

PICO4 – preliminary results V1.7- 16th April 2014 7
Primary study search
Figure 2: Search for primary articles (undertaken by LT, TW and JS)
‡Grey literature included from 2002 onwards; *45(63.4%) had no abstract;
Chemoprophylaxis – from 2004 onwards; Vaccination – no date limit
Records identified through
database search‡ N=2936
Records remaining after
duplicates removed n=2381
Number of duplicates removed
n=555
Number of records excluded
following abstract screen
n=562
Abstracts screened n=627
For full text screen*
n=65+12=77
Number of records excluded
following title screen n=1754
Full texts screened** n=77
Titles screened n=2381
Additional articles reviewed
based on reference search
n=12
Articles included n=2
1=chemoprophylaxis; 1=vaccines
Excluded
No relevant information for PICO n = 72
(Includes studies/reviews of vaccine/antibiotic effectiveness in non-household setting; outbreak reports; antibody response
studies; carriage studies; acceptability studies; economic evaluations)
Information on clusters only n=2 In Purcell review n=1

PICO4 – preliminary results V1.7- 16th April 2014 8
Table 2: Chemoprophylaxis: description of studies considered (from Purcell 2004 + primary articles identified since 2004)
Author Year
Design
Setting Country Region
Date from -
to
Index cases
(N)
Serogp of
cases
Household contact definition
Number of
contacts
Total follow
up time Intervention Comparator
Exposed (N)
Exposed subsequent
cases (n)
Unexposed (N)
Unexposed subsequent
cases (n)
Stefanoff*
2008 Cohort
Endemic; Poland;
National (surveillance
data)
2003 to 2006
635 -
person living in the same HH as the case
in the 7 days before onset of illness in the
case
1905
at least
2 months
Rifampicin
no antibiotics 629 1
(>30 days) 1276
3 (≤30 days)
Samuelsson 2000
Cohort
Endemic (3-4/100,000);
Denmark; National
(surveillance data)
Oct-95 to Apr-
97 172 -
person sleeping in the
same HH/room or kissing/saliva
exchanging contact with the case in the 10
days before onset of illness in the case
802
>24 hours (upper
limit not
clear)
ciprofloxacin no antibiotics 724 0 72 2
(≤30 days)
Scholten 1993
Cohort
Endemic
(4/100,000), Netherlands;
National (surveillance
data)
Apr-89 to Apr-
90 502
mostly B; C; A
HH member living in
the same house as the case in the week
before hospitalization of the case
1102 At least 30 days
rifampicin or minocycline
no antibiotics or antibiotics other
than rifampicin or minocycline
276 1
(>30 days) 826
4 (≤30 days)
Kristiansen
1992 Time series
Endemic (1986:
6.7/100,000);
Norway; Telemark
(surveillance data)
Jan-84
to Dec-89
13
8B;
4C; 1Y
441
(during 1987-1989)
rifampicin if harbouring
disease
causing strain and penicillin in <15years (1987-1989)
penicillin if <15
years only (1984-1987)
441 0
16**
MDSG 1976
Cohort
Endemic (0.23/100,000);
USA;
27 states & Washington DC
period 1; 17 states &
Washington DC in period 2
Nov-73 to mar-
74 & Jan-75 to Apr-
75
512 (324
serogr)
45%B;
32%C; 18%Y; 2%A
person that lived in the
same HH/dorm room with a case in the
week prior to onset of illness in the case
1872 30 days
rifampicin,
sulphonamide or
minocycline
no antibiotics or
antibiotics other than sulfonamide,
minocycline or rifampicin
693 0 1179 5
(≤30 days)
Kaiser 1974
Randomised
trial
Outbreak USA;
Dade country,
Florida
Apr-70 to Dec-
70
N/A C People who slept/ate in the same dwelling
as the case
54 9
months rifampicin none specified 35 0 19 0
HH=household; Serogp=serogroup; MDSG=meningococcal disease surveillance group; info=information. *Data obtained from study authors. **Text of article: 11 bacteriologically verified and 4 clinically suspected cases. Table in article shows 12 bacteriologically verified and 4 clinically suspected cases

PICO4 – preliminary results V1.7- 16th April 2014 9
Table 3: Vaccination – description of study considered (primary article)
Author Year
Design
Setting Country Region
Date from -
to
Serogp of
cases
Household contact definition
Number of
contacts
Total follow up
time Intervention Comparator
Exposed (N)
Exposed subsequent
cases (n)
Unexposed (N)
Unexposed subsequent
cases (n)
Greenwood
1978
Epidemic
Nigeria, Zaria
Mar-77
to May-77
A
Small compound – all people; large
compound – close family; Koranic
school – all Average size of compounds and
Koranic school - 17
1043
Until the
end of the epidemic
Meriuex (A&C
vaccine) Tetanus toxoid 520
0 definite; 1
probable 523
5 definite; 4
probable

PICO4 – preliminary results V1.7- 16th April 2014 10
Chemoprophylaxis at ≤30days
Studies excluded from the meta-analysis
Kaiser 1974 – no cases in exposed and unexposed groups
Kristiansen 1992 – no contact data during 1984-1987
Table 4: Meta-analysis of included studies – risk of subsequent meningococcal disease among household contacts given and not given chemoprophylaxis at ≤30days Study Intervention
group (n/N) Comparator group (n/N)
Risk ratio
95% confidence interval
% Weight
Stefanoff 2008 0/629 3/1276 0.29 0.01 - 5.60 17.54 Samuelsson 2000 0/724 2/72 0.02 0.00 - 0.42 34.45 Scholten 1993 0/276 4/826 0.33 0.02 - 6.14 17.12 MDSG 1976 0/693 5/1179 0.16 0.01 - 2.79 30.89 M-H pooled RR (fixed effect) 0/2322 14/3353 0.16 0.04 - 0.64 100.00 n=number of subsequent cases; N=number of contacts Chi squared test for heterogeneity p=0.543;I2 (variation in RR attributable to heterogeneity)=0.0%; Test of RR=1: p=0.008
Figure 3: Forest plot of the risk of subsequent cases of meningococcal disease among household contacts given and not given chemoprophylaxis at ≤30days
Table 5: Meta-analysis of included studies – risk difference of meningococcal disease among household contacts given and not given chemoprophylaxis at ≤30days Study Intervention
group (n/N) Comparator group (n/N)
Risk difference
95% confidence interval
% Weight
Stefanoff 2008 0/629 3/1276 -0.002 -0.006 to 0.001 37.28 Samuelsson 2000 0/724 2/72 -0.028 -0.070 to 0.014 5.79 Scholten 1993 0/276 4/826 -0.005 -0.012 to 0.002 18.31 MDSG 1976 0/693 5/1179 -0.004 -0.009 to 0.000 38.62 M-H pooled risk difference 0/2322 14/3353 -0.005 -0.009 to -0.001 100.00 NNT 200 111 to 1000 n=number of subsequent cases; N=number of contacts; NNT=number needed to treat; Chi squared test for heterogeneity p=0.34; I2=10.3%; Test of RD=0:
p=0.005
Overall (I-squared = 0.0%, p = 0.531)
Stefanoff 2008
Scholten 1993
Samuelsson 2000
Study
MDSG 1976
0.16 (0.04, 0.64)
Risk
0.29 (0.01, 5.60)
0.33 (0.02, 6.14)
0.02 (0.00, 0.42)
Ratio (95% CI)
0.15 (0.01, 2.79)
0/2322
Events,
0/629
0/276
0/724
Treatment
0/693
14/3353
Events,
3/1276
4/826
2/72
Control
5/1179
100.00
%
17.54
17.12
34.45
Weight
30.89
0.16 (0.04, 0.64)
Risk
0.29 (0.01, 5.60)
0.33 (0.02, 6.14)
0.02 (0.00, 0.42)
Ratio (95% CI)
0.15 (0.01, 2.79)
0/2322
Events,
0/629
0/276
0/724
Treatment
0/693
Favours chemoprophylaxis Favours no chemoprophylaxis
1.001 .01 .04 .16 .64 2 6
Risk Ratio

PICO4 – preliminary results V1.7- 16th April 2014 11
Chemoprophylaxis at ≤1year
Studies excluded from the meta-analysis
Kaiser 1974 – no cases in exposed and unexposed groups
Kristiansen 1992 – no contact data during 1984-1987
MDSG 1976 – follow up for only 30days
Table 6: Meta-analysis of included studies – risk of subsequent meningococcal disease among household contacts given and not given chemoprophylaxis at ≤1year* Study Intervention
group (n/N) Comparator group (n/N)
Risk ratio
95% confidence interval
% Weight
Stefanoff 2008 1/629 3/1276 0.68 0.07 - 6.49 23.23 Samuelsson 2000 0/724 2/72 0.02 0.00 - 0.42 53.27 Scholten 1993 1/276 4/826 0.75 0.08 - 6.67 23.50 M-H pooled RR (fixed effect) 2/1629 9/2174 0.34 0.11 - 1.06 100.00 n=number of subsequent cases; N=number of contacts; Chi squared test for heterogeneity p=0.12;I2 (variation in RR attributable to heterogeneity)=52.4%; Test of RR=1: p=0.06 *The total duration of follow-up of the entire cohort is unclear in the included studies. Therefore denominators may be inaccurate.
Figure 4: Forest plot of the risk of subsequent cases of meningococcal disease among household contacts given and not given chemoprophylaxis at ≤1year
Table 7: Meta-analysis of included studies – risk difference of meningococcal disease among household contacts given and not given chemoprophylaxis at ≤1year* Study Intervention
group (n/N) Comparator group (n/N)
Risk difference
95% confidence interval
% Weight
Stefanoff 2008 1/629 3/1276 -0.001 -0.005 to 0.003 60.74 Samuelsson 2000 0/724 2/72 -0.028 -0.070 to 0.014 9.44 Scholten 1993 1/276 4/826 -0.001 -0.010 to 0.007 29.82 M-H pooled risk difference 2/1629 9/2174 -0.003 -0.009 to 0.002 100.00 n=number of subsequent cases; N=number of contacts; Chi squared test for heterogeneity p=0.20; I2=37.9%; Test of RD=0: p=0.21. *The total duration of follow-up of the entire cohort is unclear in the included studies. Therefore denominators may be inaccurate.
Overall (I-squared = 52.4%, p = 0.122)
name
samuelsson
Scholten
stefanoff
0.34 (0.11, 1.06)
Ratio (95% CI)
0.02 (0.00, 0.42)
0.75 (0.08, 6.67)
0.68 (0.07, 6.49)
Risk
2/1629
Treatment
0/724
1/276
1/629
Events,
9/2174
Control
2/72
4/826
3/1276
Events,
100.00
Weight
53.27
23.50
23.23
%
0.34 (0.11, 1.06)
Ratio (95% CI)
0.02 (0.00, 0.42)
0.75 (0.08, 6.67)
0.68 (0.07, 6.49)
Risk
2/1629
Treatment
0/724
1/276
1/629
Events,
Favours chemoprophylaxis Favours no chemoprophylaxis
1.001 .01 .11 .34 2 6
Risk Ratio

PICO4 – preliminary results V1.7- 16th April 2014 12
Table 8: Chemoprophylaxis - risk of bias assessment for observational studies Item Stefanoff 2008 Samuelsson 2000 Scholten 1993 MDSG 1976 Kristiansen 1992
Study design Cohort
(national) Cohort
(national) Cohort
(national) Cohort
Cohort (time series in
one county)
Allocation of intervention Treatment decision
specific to area Treatment decision specific
to area Treatment decision
specific to area Treatment decision
specific to area Treatment decision
specific to area Comments
Selection Cohort exposed representative of all household contacts of a case of meningococcal disease
+ - + + +
Cohort not given chemoprophylaxis from the same population as the exposed cohort
+ + + + -
Comparability of exposed and unexposed assessed - - - - - Baseline demographic details given - - - - -
Comments Fatal cases excluded
Control group from a different time period to
intervention group but from
the same area.
Outcomes Objective sources used to ascertain outcome + ? + - + Adequate duration of follow up for outcome ascertainment
? ? + + +
Losses to follow up/no information ? 32% 25% ? ?
Comments Data obtained from
author – need to contact to obtain details
Notification systems used to
identify cases. Households interviewed. Unclear if
subsequent cases determined by notification or interview.
172/252 eligible households participated
378/502 eligible households included. Valid information
only on 1102/1130 (97.5%) of included contacts.
Households contacted to
enquire on secondary cases, at least 30days after
hospitalization of index case. No information to assess
losses to follow-up
Follow up 7-31months
during the intervention period. For 84-87 (control period) some cases were
followed up for at least 300
days.
Analysis Adequate control for confounders - - - - - Comments

PICO4 – preliminary results V1.7- 16th April 2014 13
Table 9: Chemoprophylaxis - risk of bias assessment for trials (Kaiser 1974)
Domain Judgement Justification
Selection bias Random sequence generation Low risk of bias Allocation by dice throw Allocation concealment Unclear risk of bias Not stated
Performance bias Blinding Low Not specified, but it is unlikely that
blinding would have influenced the outcome.
Detection bias Blinding of outcome assessment Low Unclear if investigators assessing
outcome status of study participants were blinded. However, it is unlikely that assessment of this objective outcome would have been influenced (and there were no subsequent cases in the study)
Attrition bias Incomplete outcome data Unclear risk of bias Not stated
Reporting bias Selective reporting Unclear risk of bias Protocol not available to determine
main objectives of study

PICO4 – preliminary results V1.7- 16th April 2014 14
Vaccination
Table 10: Risk of subsequent meningococcal disease among household contacts who were and were not vaccinated Study Intervention
group (n/N) Comparator group (n/N)
Risk ratio 95% confidence interval
p -value
Greenwood 1978 Definite only 0/520 5/523 0.09 0.01-1.65 0.11 Definite & probable 1/520 9/523 0.11 0.01-0.88 0.04 n=number of subsequent cases; N=number of contacts; Definite case=proven meningitis and positive culture or antigen test; Probable case (intervention
group) = acute febrile illness but died on the way to hospital with no clinical samples takes; Probable cases (comparator group) = proven meningitis (with
negative cultures and antigen test) or septicaemia and high baseline antibody titre (≥1 in 32) or rise in titre of >4 fold.
Table 11: Risk of bias assessment for vaccination study
Domain Judgement Justification
Selection bias Random sequence generation Unclear risk of bias Alternative compounds allocated
to intervention and comparator group. Unclear if allocation could have been predicted in advance
Allocation concealment
Unclear risk of bias
Not specified
Performance bias Blinding Low Not specified, but it is unlikely that
blinding would have influenced the outcome.
Detection bias Blinding of outcome assessment Low / Unclear risk of bias Unclear if investigators assessing
outcome status of study participants were blinded. However it is unlikely that blinding would influence the outcome assessment for definite cases. For probable cases, the risk of bias is unclear
Attrition bias Incomplete outcome data Low risk of bias Study does not appear to have
any missing data for outcomes
Reporting bias Selective reporting Unclear risk of bias Protocol not available to determine
main objectives of study

PICO4 – preliminary results V1.7- 16th April 2014 15
Development of resistance to antibiotics used as chemoprophylaxis
Not reported in studies included in this systematic review and meta-analysis.
A systematic review undertaken by the Cochrane Collaboration (Zalmanovici 2013, page 10) reported the
following:
“Eleven trials reported the susceptibility of persistent isolates to at least one of the studied antibiotics
(Blakebrough 1980; Deal 1969a; Deal 1969b; Devine 1971b; Dworzack 1988; Guttler 1971; Kaiser 1974;
Munford 1974; Pugsley 1987; Renkonen 1987; Simmons 2000). No development of resistance was detected for
any antibiotic drug other than rifampin. Six trials assessed resistance development to rifampin (Blakebrough
1980; Deal 1969a; Guttler 1971; Kaiser 1974; Munford 1974; Simmons 2000). In Guttler 1971 rifampin-resistant
isolates requiring minimal inhibitory concentrations (MICs) of 100 to 200 μg/ml of rifampin were seen in 20 of 75
post-treatment isolates, while MICs increased from pre-treatment values of less than 0.25 μg/ml to 2 to 6 μg/ml in
37 additional isolates. All resistant isolates were detected among patients treated with rifampin. In Munford
1974, seven resistant isolates were detected out of 37 isolates among 67 patients treated with rifampin (MICs of
16 to 256 μg/ml). All pre-treatment isolates were susceptible to rifampin and no resistance to rifampin developed
among patients randomised to rifampin in addition to minocycline in this study. The meningococci identified in
these two studies were serogroup B or C and all resistant isolates were identified as group C. One additional
study assessing group A meningococci (Blakebrough 1980) found an increase in rifampin MICs from less than
0.1 μg/ml to 3.2 μg/ml (three isolates) and 6.4 μg/ml (one isolate) post treatment. In all trials seven eradication
failures were assessed for resistance development, which was not found.”
11 studies; variety of setting (most from North America; South America; sub-Saharan Africa [1]; New
Zealand); variety of populations (household contacts, students; army recruits, volunteers)
Antibiotics used: rifampicin, ciprofloxacin, sulphonamides, minocycline, cephalexin, ampicillin, ceftriaxone
Follow up time: 5 to 130days
Primary outcomes: eradication/morbidity

PICO4 – preliminary results V1.7- 16th April 2014 16
Table 12: Details of studies assessing resistance development to rifampicin
Munford 1974 Guttler 1971 Blakebrough 1980 Simmons 2000 Deal 1969 Kaiser 1974
Main serogroup B/C B/C A B B C
Resistant serogroup C C A
Follow-up (weeks) 2 5 7 6 days 2-3 3-4
Rifampin dose 600mgX2 for 2days 600mgX1 for 4days 600mgX2 for 2days 600mgX2 for 2days 600mgX1 for 4days 600mgX1 for 4days
Population Families+children
(Brazil) Army recruits
(USA) Household+children
(Nigeria) Household+children
(New Zealand) Students
(USA) Household+children
(USA)
Resistance testing method Agar dilution Agar dilution Agar dilution E test Plate dilution Plate dilution
Number treated with rifampicin 67 147 48 82 15 13
Number of treatment failures 6 13 11 4 2 1
Initial MICs of isolates (µg/ml) <0.25 <0.25 <0.1 Not reported <1 <0.12
Final MICs of isolates (µg/ml) 1=16; 1=32; 1=64;
1=125; 1=256 37=2-6; 20=100-
200 3=3.2; 1=6.4 <2 <1 <0.12
Comments
No resistance in rifampin-
minocycline combination arm; 7 resistant isolates
detected out of 37 tested
75 isolates tested 11 isolates tested 7 isolates tested 4 isolates tested
Proportion of isolates with raised MICs
18.9% 76.0% 36.4% - - -
(Data received from Professor Paul and Professor Leibovici, authors of the Cochrane Review Zalmanovici et al. Antibiotics for preventing meningococcal infections 2013)

PICO4 – preliminary results V1.7- 16th April 2014 17
Adverse effects of antibiotics and/or vaccination used as prophylaxis
Not reported in studies included in this systematic review and meta-analysis.
A systematic review undertaken by the Cochrane Collaboration (Zalmanovici 2013, page 9, 36 and 38) reported the following:
“Eighteen trials provided quantitative data regarding the occurrence of adverse effects. These were all mild in nature and included nausea, diarrhoea, abdominal pain,
headaches, dizziness, skin rash and pain at injection site. One study comparing rifampin to ceftriaxone yielded an overall risk ratio (RR) for any clinical adverse effects of 1.39
(95% confidence interval (CI) 1.10 to 1.75) (Analysis 1.1). Two studies comparing rifampin to ciprofloxacin yielded an overall non-significant RR of 0.75 (95% CI 0.36 to 1.56)
(Analysis 1.2).”
18 trials; variety of settings (North & South America, sub-Saharan Africa [1], North Africa, Asia); variety of populations (household contacts, children, students, army
recruits, volunteers, patients with gonorrhoea)
Antibiotics used: rifampicin, ciprofloxacin, cephalexin, minocycline, sulphadiazine, amoxicillin, coumermycin, azithromycin, spectinomycin, ceftriaxone
Follow up time: 5 to 30days
Primary outcome: eradication/morbidity

PICO4 – preliminary results V1.7- 16th April 2014 18

PICO4 – preliminary results V1.7- 16th April 2014 19

PICO4 – preliminary results V1.7- 16th April 2014 20
GRADE profile
Question: Should chemoprophylaxis be used for subsequent meningococcal disease among household contacts of cases of meningococcal disease?
Quality assessment Summary of findings
Importance No of patients Effect
Quality No of studies
Design Limitations Inconsistency Indirectness Imprecision Other considerations Chemoprofylaxis control Relative (95% CI)
Absolute
Subsequent case of meningococcal disease (30 days) (follow-up 30 days; clinical judgement or PCR/culture)
4 observational studies
serious1 no serious inconsistency
serious2 serious3 none
0/2322 (0%) 14/3353 (0.42%)
RR 0.16 (0.04 to
0.64)
4 fewer per 1000 (from 2
fewer to 4 fewer)
VERY LOW
CRITICAL
Subsequent case of meningococcal disease (1 year) (follow-up 1 year; clinical judgement or PCR/culture)
3 observational studies
serious1 no serious inconsistency
serious2 serious3 none
2/1629 (0.1%) 9/2174 (0.4%)
RR 0.34 (0.11 to
1.06)
3 fewer per 1000 (from 4
fewer to 0 more)
OOO VERY LOW
CRITICAL
Resistance to antibiotics (follow-up 14+ days)
3 randomised trials
serious4 serious5 no serious indirectness
serious3 Resistance development was not detected for any antibiotic other than rifampicin. In 3 studies
undertaken in a variety of settings, raised MICs to rifampicin used developed in 18.9%, 36.4% and 76.0% of the isolates tested.
- - - - OOO VERY LOW
CRITICAL
Adverse effects: rifampicin vs ceftriaxone (follow-up 6+ days)
1 randomised trials
serious4 no serious inconsistency
no serious indirectness
serious3 none
129/440 (29.3%) 88/416 (21.2%)
RR 1.39 (1.10 to
1.75)
83 more per 1000 (from 21 more to 159
more)
OO LOW
IMPORTANT
Adverse effects: rifampicin vs ciprofloxacin (follow-up 2 weeks)
2 randomised trials
serious4 no serious inconsistency
no serious indirectness
very serious3,6
none
13/861 (1.5%) 15/737 (2%)
RR 0.75 (0.36 to
1.56)
5 fewer per 1000 (from 13
fewer to 11 more)
OOO VERY LOW
IMPORTANT
1 No baseline demographic details provided; no adjustment for confounding in all studies; 2 All studies carried out in US or Western Europe (non-epidemic situations); 3 Optimal Information Size (OIS) not met; 4 All
studies high risk of bias; 5 One study in army recruits with very high percentage of rifampicin resistance; 6 CI includes both benefit and harm

PICO4 – preliminary results V1.7- 16th April 2014 21
Question: Should vaccination be used for subsequent meningococcal disease among household contacts of cases of meningococcal disease?
Quality assessment Summary of findings
Importance Number of patients Effect
Quality No of studies
Design Limitations Inconsistency Indirectness Imprecision Other
considerations An appropriate
vaccine control
Relative (95% CI)
Absolute
Subsequent definite meningococcal disease (clinical features, culture, antibody and antigen test)
1 trial serious1 no serious inconsistency
no serious indirectness
serious2 None 0/520 (0%)
5/523 (0.96%)
RR 0.09 (0.01 to 1.65)
9 fewer per 1000 (from 9 fewer to 6 more)
LOW
CRITICAL
Adverse effects
0 - - - - - None - - - -
IMPORTANT 1 Unclear risk of selection, performance and detection bias; 2 Optimal Information Size (OIS) not met; No=Number
Question: Should chemoprophylaxis and vaccination be used for subsequent meningococcal disease among household contacts of cases of meningococcal disease?
Quality assessment Summary of findings
Importance Number of patients Effect
Quality No of studies Design Limitations Inconsistency Indirectness Imprecision Other considerations Chemoprophylaxis and vaccination control
Relative (95% CI)
Absolute
Subsequent case of meningococcal disease at ≤30days
0 - - - - - none - - - -
CRITICAL
Subsequent case of meningococcal disease at ≤1 year
0 - - - - - none - - - -
CRITICAL
Resistance to antibiotics
0 - - - - - none - - - -
CRITICAL
Adverse effects
0 - - - - - none - - - -
IMPORTANT
No=number

PICO4 – preliminary results V1.7- 16th April 2014 22
Conclusions:
There is limited evidence on the effect of chemoprophylaxis (4 observational studies) and vaccination (1 quasi-
randomised trial) on the risk of subsequent meningococcal disease among household contacts of a case of
meningococcal disease. Data on risk of meningococcal disease among household contacts, including risk over
time in the African setting would be useful to guide decision making.
Chemoprophylaxis
All four included studies were from non-epidemic settings in Europe and USA (annual disease incidence
ranging from 0.23 – 4.0 per 100,000 population)
Data suggests an 84% reduction in the risk of subsequent cases of meningococcal disease among
household contacts given chemoprophylaxis at ≤30days (p=0.008).
Using the pooled estimate, 200 (95%CI 111-1000) household contacts would need to be treated to
prevent 1 subsequent case of meningococcal disease at ≤30days.
Data suggests a 66% reduction in the risk of subsequent cases of meningococcal disease among
household contacts given chemoprophylaxis at ≤1 year (P=0.06).
However, the quality of the evidence (at ≤30days and ≤1year) was very low.
Vaccination
Single trial from Africa
While data suggests a 91% reduction in the risk of subsequent cases of definite meningococcal disease
among household contacts given vaccine, there is insufficient evidence to rule out a chance finding
(p=0.11).
When both definite and probable cases were taken into consideration, the data suggests an 89%
reduction in the risk of subsequent cases of meningococcal disease (p=0.04)
Resistance to antibiotics used as chemoprophylaxis
Not reported on in the studies included in this systematic review.
Evidence from a previous systematic review suggests that resistance only developed when rifampicin
was used (raised MICs were found to 18.9% to 76.0% of isolates tested from 3 studies)
Adverse effects of antibiotics used
Not reported on in the studies included in this systematic review

PICO4 – preliminary results V1.7- 16th April 2014 23
Evidence from a previous systematic review suggests that there is no difference in adverse effects
reported when rifampicin or ciprofloxacin were used, but more adverse effects were found after
rifampicin compared to ceftriaxone.

PICO4 – preliminary results V1.7- 16th April 2014 24
References:(1-12)
1. World Health Organization. Control of epidemic meningococcal disease; WHO practical gudielines 1998. Available from: http://www.who.int/csr/resources/publications/meningitis/WHO_EMC_BAC_98_3_EN/en/index.html. 2. Hossain MJ, Roca A, Mackenzie GA, Jasseh M, Hossain MI, Muhammad S, et al. Serogroup W135 meningococcal disease, The Gambia, 2012. Emerging infectious diseases. 2013;19(9):1507-10. PubMed PMID: 23965435. Pubmed Central PMCID: 3810914. 3. Purcell B, Samuelsson S, Hahne SJ, Ehrhard I, Heuberger S, Camaroni I, et al. Effectiveness of antibiotics in preventing meningococcal disease after a case: systematic review. Bmj. 2004 Jun 5;328(7452):1339. PubMed PMID: 15178612. Pubmed Central PMCID: 420283. 4. European Centre for Disease prevention and Control. Public health management of sporadic cases of invasive meningococcal disease and their contacts 2010. Available from: http://www.ecdc.europa.eu/en/publications/publications/1010_gui_meningococcal_guidance.pdf. 5. Hoek MR, Christensen H, Hellenbrand W, Stefanoff P, Howitz M, Stuart JM. Effectiveness of vaccinating household contacts in addition to chemoprophylaxis after a case of meningococcal disease: a systematic review. Epidemiology and infection. 2008 Nov;136(11):1441-7. PubMed PMID: 18559124. Pubmed Central PMCID: 2870749. 6. Zalmanovici Trestioreanu A, Fraser A, Gafter-Gvili A, Paul M, Leibovici L. Antibiotics for preventing meningococcal infections. The Cochrane database of systematic reviews. 2013 Oct 25;10:CD004785. PubMed PMID: 24163051. 7. Samuelsson S, Hansen ET, Osler M, Jeune B. Prevention of secondary cases of meningococcal disease in Denmark. Epidemiology and infection. 2000 Jun;124(3):433-40. PubMed PMID: 10982067. Pubmed Central PMCID: 2810929. 8. Scholten RJ, Bijlmer HA, Dankert J, Valkenburg HA. [Secondary cases of meningococcal disease in The Netherlands, 1989-1990; a reappraisal of chemoprophylaxis]. Nederlands tijdschrift voor geneeskunde. 1993 Jul 24;137(30):1505-8. PubMed PMID: 8366938. Secundaire gevallen van meningokokkenziekte in Nederland, 1989-1990; chemoprofylaxe opnieuw bezien. 9. Kristiansen BE, Tveten Y, Ask E, Reiten T, Knapskog AB, Steen-Johnsen J, et al. Preventing secondary cases of meningococcal disease by identifying and eradicating disease-causing strains in close contacts of patients. Scandinavian journal of infectious diseases. 1992;24(2):165-73. PubMed PMID: 1641593. 10. Analysis of endemic meningococcal disease by serogroup and evaluation of chemoprophylaxis. The Journal of infectious diseases. 1976 Aug;134(2):201-4. PubMed PMID: 823273. 11. Kaiser AB, Hennekens CH, Saslaw MS, Hayes PS, Bennett JV. Seroepidemiology and chemoprophylaxis disease due to sulfonamide-resistant Neisseria meningitidis in a civillian population. The Journal of infectious diseases. 1974 Sep;130(3):217-24. PubMed PMID: 4213375. 12. Greenwood BM, Hassan-King M, Whittle HC. Prevention of secondary cases of meningococcal disease in household contacts by vaccination. British medical journal. 1978 May 20;1(6123):1317-9. PubMed PMID: 417754. Pubmed Central PMCID: 1604678.