dr juzar hooker , consulting neurologist, aga khan ... juzar hooker, consulting neurologist, aga...
TRANSCRIPT

Dr Juzar Hooker, Consulting Neurologist, Aga Khan University Hospital

Common and burdensome Can be serious Important cause of disability (WHO) Burden of referral Treatment available, effective, under-utilised
Use a case-based approach
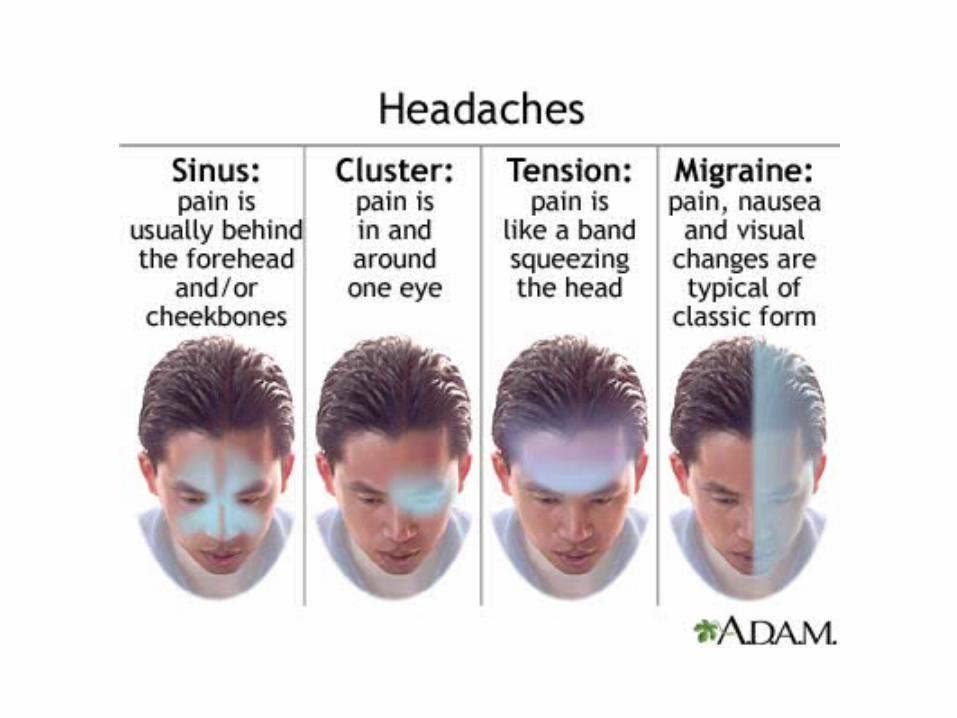
Discuss common headache types Migraine Tension-type headache
Emphasise important principles

A 28 year old housewife with 2 small children presents with increasingly frequent headaches, in the setting of a long-standing history of occasional headaches.


Unilateral Throbbing Nausea Worse with activity Disabling Rests
6-7 hours 7-10/10
Paracetamol
No aura
Some premenstrual
1 y 3 m old baby – 2-3
awakenings at night

A. At least 5 attacks fulfilling criteria B-D B. Headache attacks lasting 4-72 h (untreated or
unsuccessfully treated) C. Headache has ≥2 of the following characteristics:
1. unilateral location 2. pulsating quality 3. moderate or severe pain intensity 4. aggravation by or causing avoidance of routine
physical activity (eg, walking, climbing stairs) D. During headache ≥1 of the following:
1. nausea and/or vomiting 2. photophobia and phonophobia
E. Not better accounted for by another ICHD-3 diagnosis

AAN

(1) Has a headache limited your activities for a day or more in the last three months?
(2) Are you nauseated or sick to your stomach when you have a headache?
(3) Does light bother you when you have a headache?
High accuracy Sensitivity 0.81 (95%
CI,0.77 to 0.85) specificity 0.75 (95% CI,
0.64 to 0.84) In the primary care
setting, ID Migraine Screener had a positive predictive value of 93.3% (95% CI, 89.9 to 95.8)
NEUROLOGY 2003;61:375–382



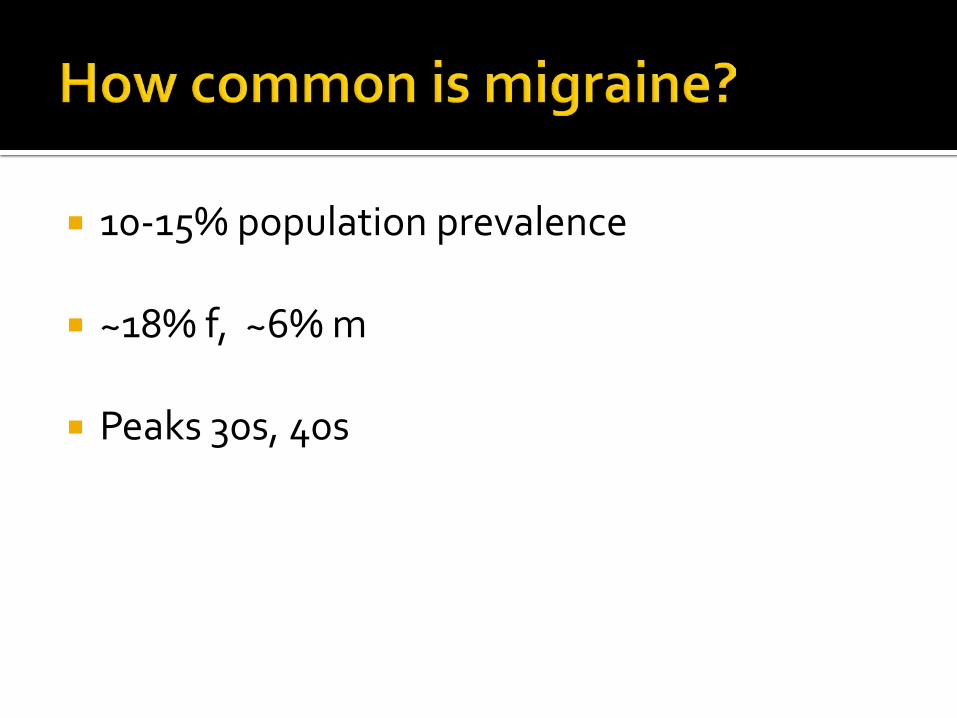
10-15% population prevalence
~18% f, ~6% m
Peaks 30s, 40s

Lipton et al

88% of 711 medical students reported at least one episode of headache in preceding 6 months
38.4% migraine 29% migraine with aura m:f ratio 1:1.3 43% had 2-3 episodes per month 43.6% had a family history
Amayo et al, 1996


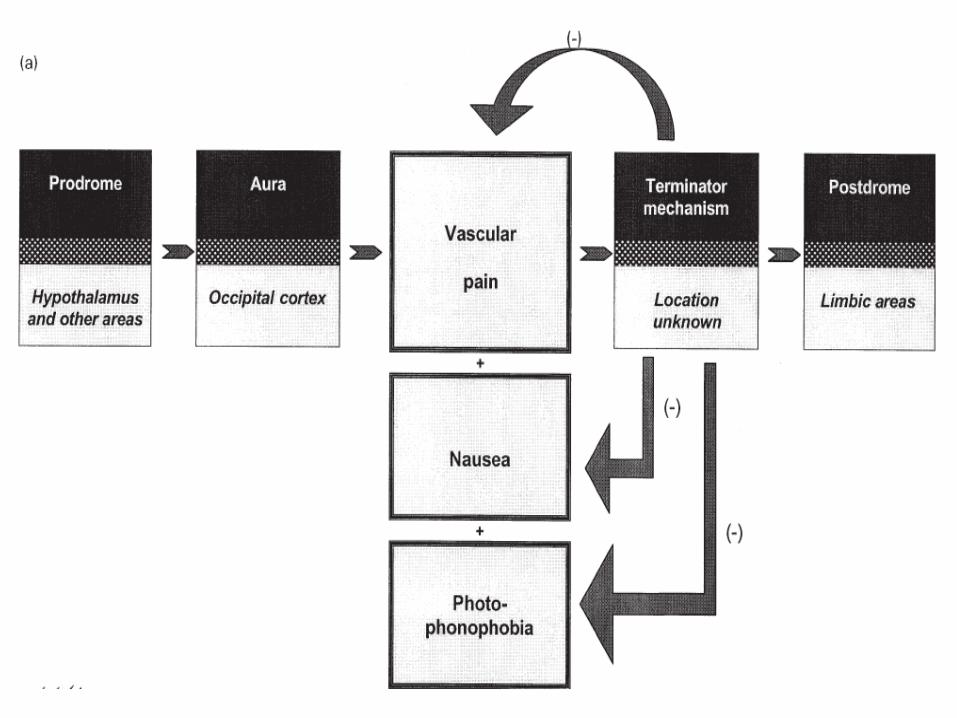
Disorder of the brain involving neural hyperexcitability/hypersynchronicity resulting in activation or perception of activation of the nociceptive trigeminovascular system and pain, together with a state of hypersensitivity to various stimuli
after Peter Goadsby
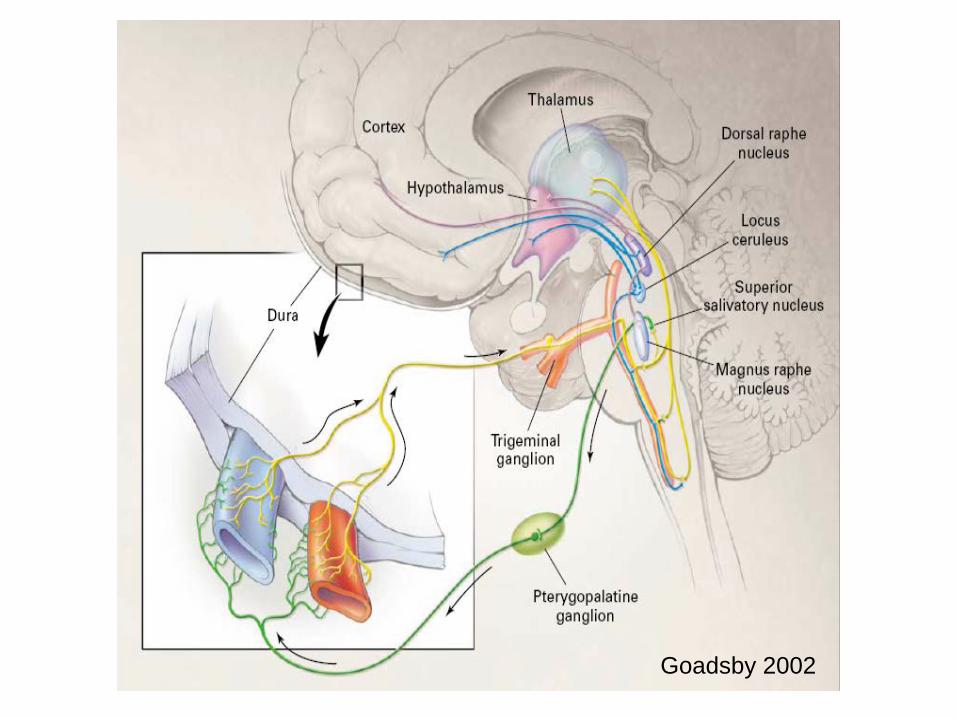
Goadsby 2002
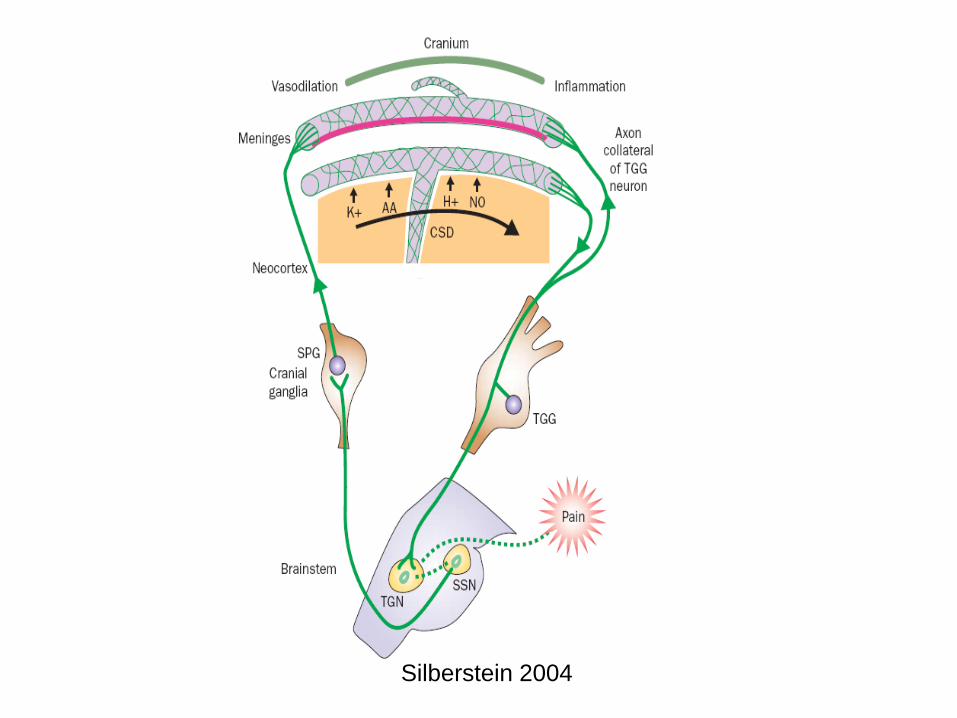
Silberstein 2004

A 47 year old lady has been having episodic severe unilateral throbbing headaches lasting up to a day, with associated nausea, vomiting, photo-, phono-, and osmophobia. They stop her from working or playing tennis. Over the last 10 days, she has developed a different left frontal headache.

Headache features First-ever headache Worst-ever headache Subacute worsening Persistent headache Different headache Always on one side Disturbs sleep Present on awakening Vomiting precedes headache Exacerbated by head position Onset with head trauma Onset with Valsalva
manoeuvre, exercise Onset after age 50 years
Associated features Focal neurological signs Altered consciousness Fever Nuchal rigidity Seizure Papilloedema or (pre)retinal
haemorrhage History of
AIDS or HIV risk factors Bleeding diathesis Hypercoagulable state Vascular disease Connective tissue disease Cancer Trauma

ESR/CRP/PCT Complete blood count Coagulation profile HIV serology Septic screen
Neuroradiology CT scan brain MRI, MRV, MRA Angiography
Lumbar puncture and CSF studies
EEG



Acute treatment
Avoid triggers/non-pharmacologic management
Prevention of attacks

Paracetamol
AAC
NSAID Ibuprofen 400-800 mg Naproxen 500 mg
Aspirin 900 mg

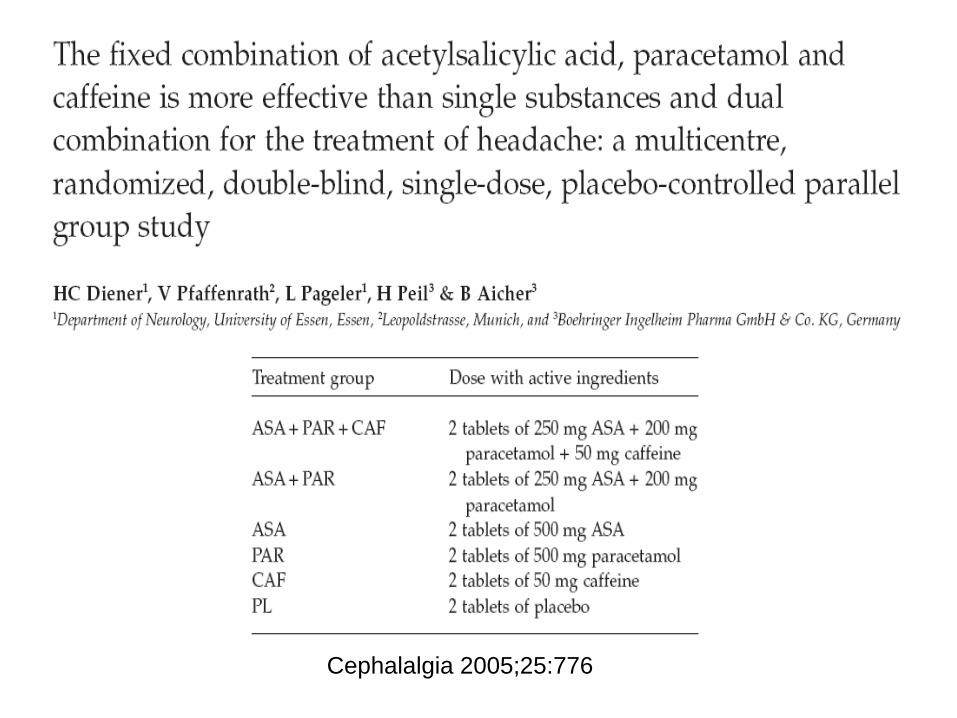
Cephalalgia 2005;25:776

Cephalalgia 2005;25:776
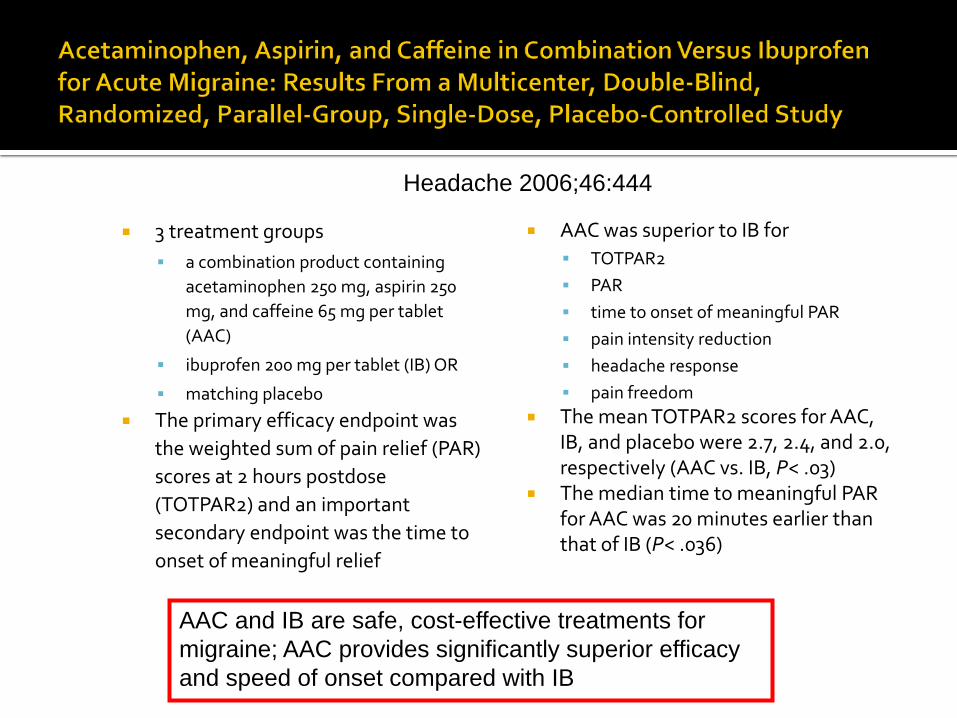
3 treatment groups a combination product containing
acetaminophen 250 mg, aspirin 250 mg, and caffeine 65 mg per tablet (AAC)
ibuprofen 200 mg per tablet (IB) OR
matching placebo The primary efficacy endpoint was
the weighted sum of pain relief (PAR) scores at 2 hours postdose (TOTPAR2) and an important secondary endpoint was the time to onset of meaningful relief
AAC was superior to IB for TOTPAR2 PAR time to onset of meaningful PAR pain intensity reduction headache response pain freedom
The mean TOTPAR2 scores for AAC, IB, and placebo were 2.7, 2.4, and 2.0, respectively (AAC vs. IB, P< .03)
The median time to meaningful PAR for AAC was 20 minutes earlier than that of IB (P< .036)
AAC and IB are safe, cost-effective treatments for migraine; AAC provides significantly superior efficacy and speed of onset compared with IB
Headache 2006;46:444

Goadsby 2002

Cephalalgia 2004;24:321
Dichotomy Triptans and non-triptans almost equi-efficacious
in trials Triptans considered more effective in clinical
practice
Why?
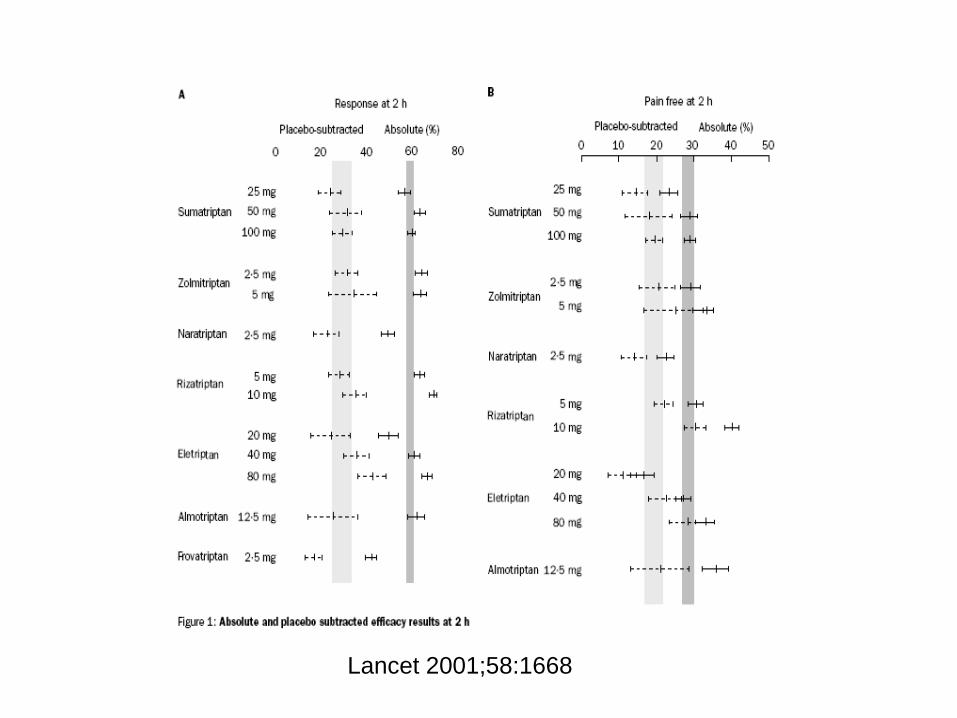
Lancet 2001;58:1668

Lancet 2001;58:1668

Headache 2005;45:983


Sumatriptan Nasal spray 20 mg SC injection 6 mg Transdermal
Ergotamine
Dihydroergotamine nasal spray 2 mg


38 year old doctor’s wife brought to A+E with very severe headache, unresponsive to analgesics. Blood pressure high – 160/100. This is the 4th such episode. Was once started on antihypertensive, and was to be investigated for a secondary cause for hypertension.

BMJ 2004;329:1369

Neuroleptics Chlorpromazine 0.1 mg/kg IV Prochlorperazine 10 mg IV Droperidol 2-75-8.25 mg IM
Dexamethasone 10-25 mg IV or IM Prevents migraine recurrence

Ketorolac 60 mg IM or 30 mg IV or 20 mg PO
Can give 30 mg q4-6 h IV or IM (maximum 120 mg/d) OR 10 mg q4-6 h (maximum 40 mg/d)

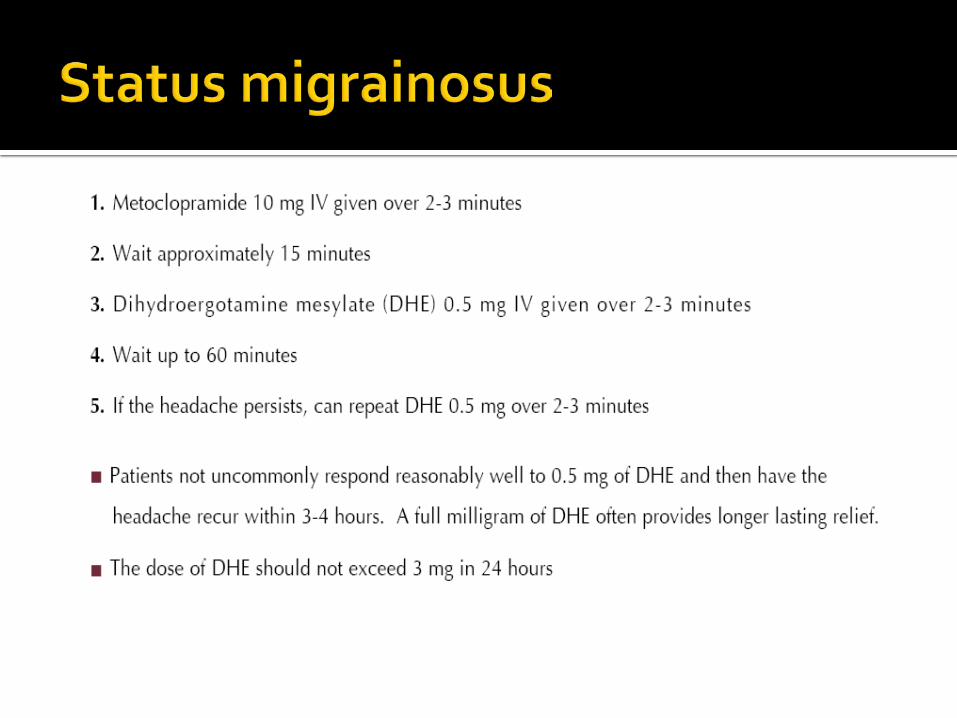
35 year old lawyer with known migraine presents with a 1 week history of persistent severe headache, which is unrelenting even with usual analgesics.




27 year old banker has 12 headache days a month. She is finding it difficult to cope at work and at home. Her family is worried.

Sleep hygiene Regular meals, good breakfast Adequate fluids 35 minutes on, 5 minutes off for computer
use Avoid precipitants
Graded exercise
Yoga (Cognitive behavioural therapy)

5-HT2 stimulation >2 disabling attacks/month Intensity * frequency * duration of
headache Start low, go slow Review therapy after 6 months, taper

Beta blockers Propranolol A Metoprolol A Timolol A Atenolol B Nadolol B Nebivolol C Pindolol C
Anticonvulsants Topiramate A Divalproex and valproate A (Gabapentin) U (Carbamazepine) C

Antidepressants Amitriptyline B Venlafaxine B
Antihypertensives Verapamil U Lisinopril C Candesartan C Clonidine C
Flunarizine A
Cyproheptadine C
Pizotifen
Naturals Butterbur A Riboflavin B Coenzyme Q10 C

Botox
Acupuncture
Occipital nerve blocks


Selective muscle resections
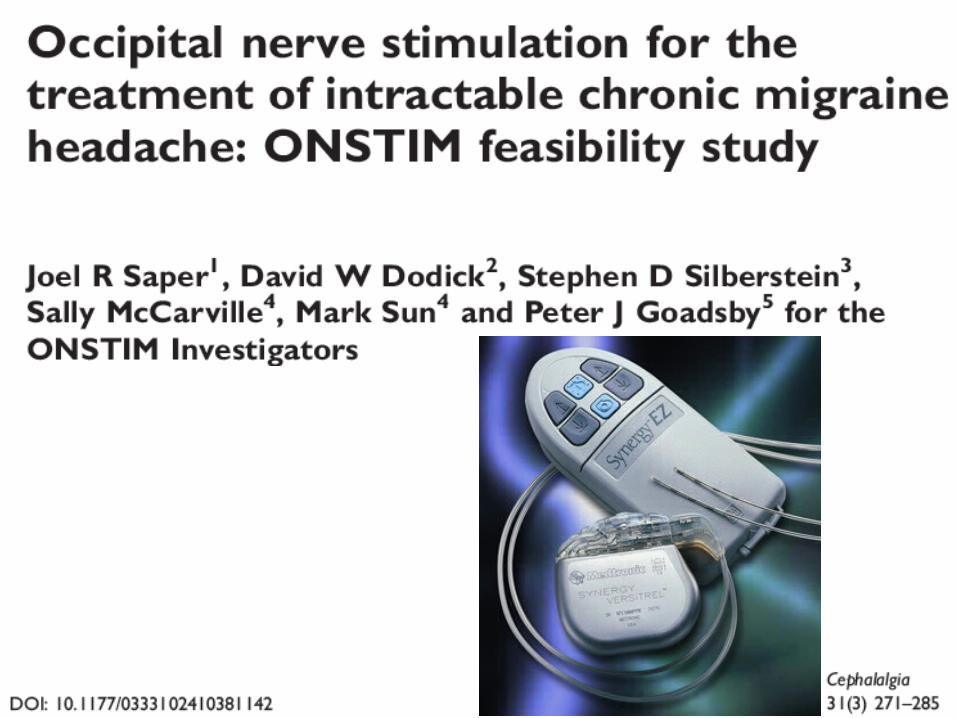
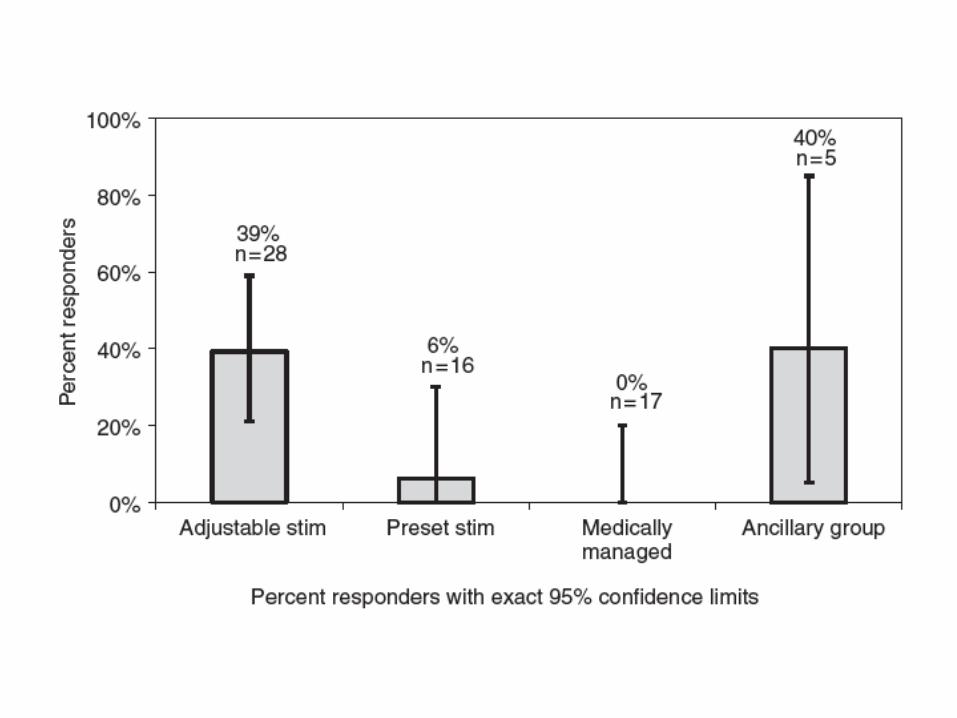
Neuromodulatory devices

36 year old humanitarian worker has 4 days of severe headache a month, causing her to miss work. She travels a lot. The headaches tend to occur from 2 days before her periods begin. The periods are regular.


Perimenstrual Triptans ▪ Frovatriptan ▪ Zolmitriptan ▪ Naratriptan
Naproxen/NSAID Oestrogen

A 40 year old chef suffers from moderately severe daily headache for 8 months. He previously had episodic throbbing severe headaches. He requires daily painkillers.

Previous episodic migraine without aura
Now Chronic/transformed migraine Medication overuse headache

NEMJ 2006;354:158
Withdraw analgesics
Effective pain management
Prophylaxis

Lancet Neurology 2004;3:475
26 year old businessman develops visual disturbance involving one half of the visual field, usually on the left, lasting about 15 minutes, followed by severe headache. Since the last episode, when the visual problem lasted over an hour, he has remained with a spot of absent vision while reading.

Migraine with aura
Migrainous infarction


A. At least 2 attacks fulfilling criteria B and C B. ≥1 of the following fully reversible aura symptoms: 1.visual; 2. sensory; 3. speech and/or language;
4. motor ; 5. brainstem; 6. retinal C. ≥2 of the following 4 characteristics: 1. ≥1 aura symptom spreads gradually over ≥5 min,
and/or ≥2 symptoms occur in succession 2. each individual aura symptom lasts 5-60 min 3. ≥1 aura symptom is unilateral 4. aura accompanied or followed in <60 min by
headache D. Not better accounted for by another ICHD-3 diagnosis,
and TIA excluded

A. At least 2 attacks fulfilling criteria B and C B. Aura of visual, sensory and/or speech/language
symptoms, each fully reversible, but no motor, brainstem or retinal symptoms
C. ≥2 of the following 4 characteristics: 1. ≥1 aura symptom spreads gradually over ≥5 min,
and/or ≥2 symptoms occur in succession 2. each individual aura symptom lasts 5-60 min 3. ≥1 aura symptom is unilateral 4. aura accompanied or followed in <60 min by
headache D. Not better accounted for by another ICHD-3 diagnosis,
and TIA excluded

A. Fulfils criteria for 1.2.1 Migraine with typical aura B. Headache, with or without migraine characteristics,
accompanies or follows the aura within 60 min

A. Fulfils criteria for 1.2.1 Migraine with typical aura B. No headache accompanies or follows the aura within
60 min
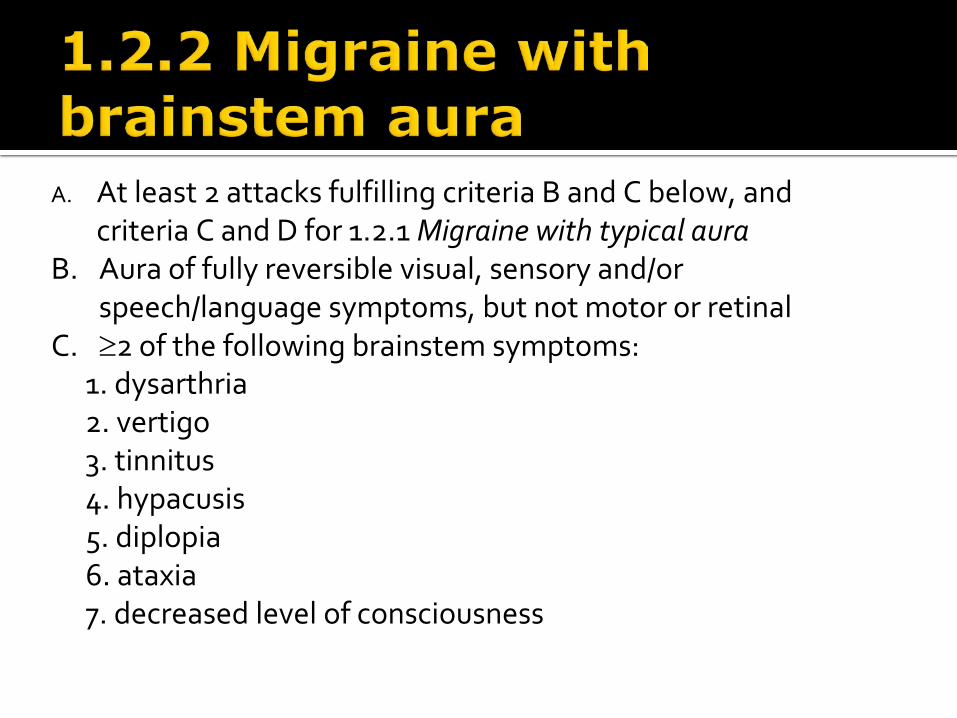
A. At least 2 attacks fulfilling criteria B and C below, and criteria C and D for 1.2.1 Migraine with typical aura
B. Aura of fully reversible visual, sensory and/or speech/language symptoms, but not motor or retinal
C. ≥2 of the following brainstem symptoms: 1. dysarthria 2. vertigo 3. tinnitus 4. hypacusis 5. diplopia 6. ataxia 7. decreased level of consciousness

1.4.1 Status migrainosus 1.4.2 Persistent aura without infarction 1.4.3 Migrainous infarction 1.4.4 Migraine aura-triggered seizure

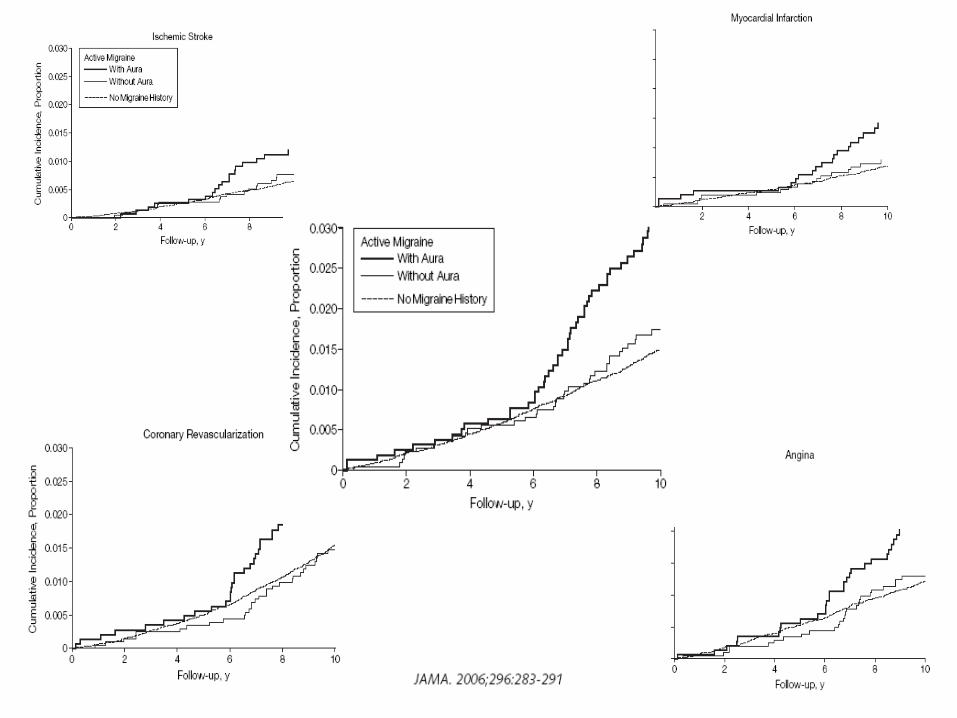


Risk factor OR Smokers 1.43 (1.1-1.8) Dyslipidaemia 1.64 (1.1-2.4) ↑BP 1.76 (1.04-3) Premature stroke/CAD 3.96 (1.1-14.3)
Neurology 2005;64:614

Aspirin
Lamotrigine
Verapamil or flunarizine for hemiplegic migraine

42 year gentleman with chronic daily headache. Pressing pain, back of head, continuous, worse at the end of the day.


2.1 Infrequent episodic tension-type headache 2.2 Frequent episodic tension-type headache 2.3 Chronic tension-type headache 2.4 Probable tension-type headache
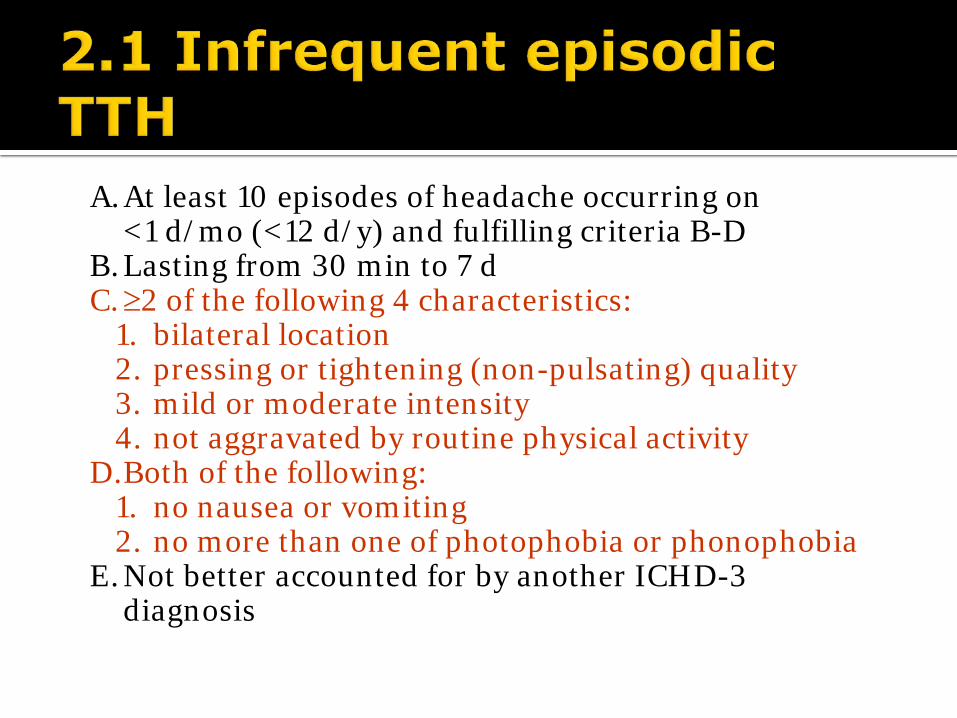
A. At least 10 episodes of headache occurring on <1 d/mo (<12 d/y) and fulfilling criteria B-D
B. Lasting from 30 min to 7 d C. ≥2 of the following 4 characteristics:
1. bilateral location 2. pressing or tightening (non-pulsating) quality 3. mild or moderate intensity 4. not aggravated by routine physical activity
D. Both of the following: 1. no nausea or vomiting 2. no more than one of photophobia or phonophobia
E. Not better accounted for by another ICHD-3 diagnosis
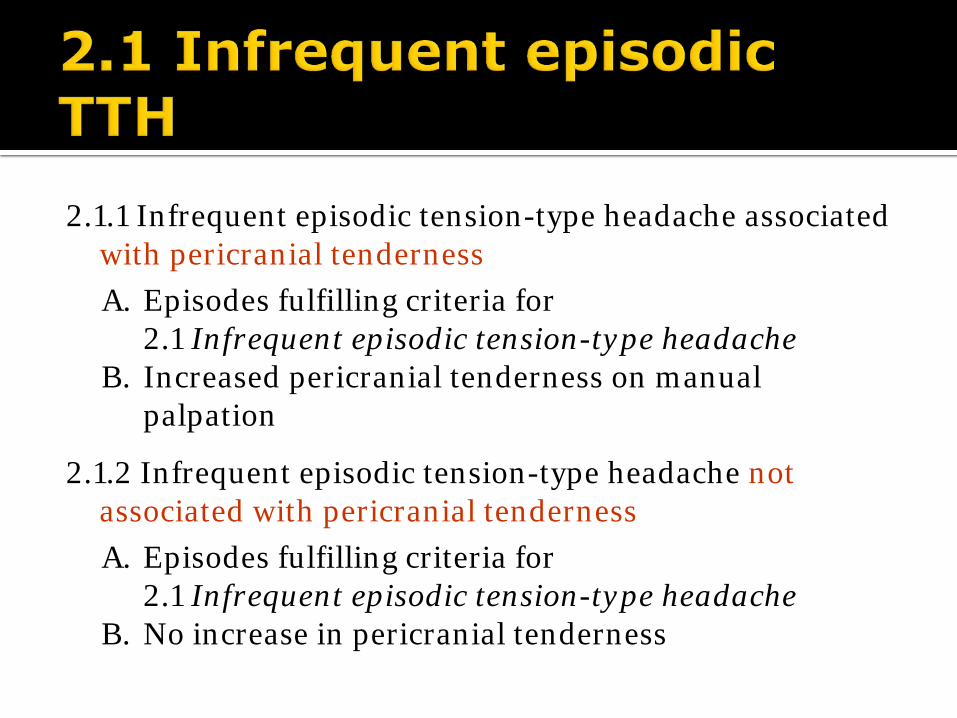
2.1.1 Infrequent episodic tension-type headache associated with pericranial tenderness A. Episodes fulfilling criteria for
2.1 Infrequent episodic tension-type headache B. Increased pericranial tenderness on manual
palpation
2.1.2 Infrequent episodic tension-type headache not associated with pericranial tenderness A. Episodes fulfilling criteria for
2.1 Infrequent episodic tension-type headache B. No increase in pericranial tenderness
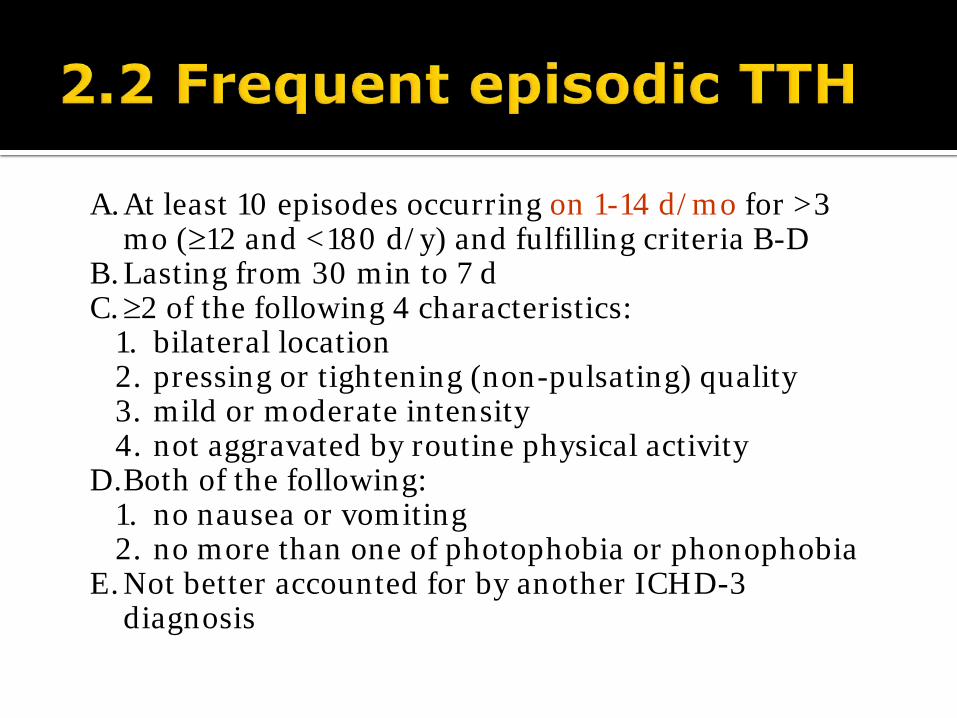
A. At least 10 episodes occurring on 1-14 d/mo for >3 mo (≥12 and <180 d/y) and fulfilling criteria B-D
B. Lasting from 30 min to 7 d C. ≥2 of the following 4 characteristics:
1. bilateral location 2. pressing or tightening (non-pulsating) quality 3. mild or moderate intensity 4. not aggravated by routine physical activity
D. Both of the following: 1. no nausea or vomiting 2. no more than one of photophobia or phonophobia
E. Not better accounted for by another ICHD-3 diagnosis

2.2.1 Frequent episodic tension-type headache associated with pericranial tenderness A. Episodes fulfilling criteria for
2.2 Frequent episodic tension-type headache B. Increased pericranial tenderness on manual
palpation
2.2.2 Frequent episodic tension-type headache not associated with pericranial tenderness A. Episodes fulfilling criteria for
2.2 Frequent episodic tension-type headache B. No increase in pericranial tenderness
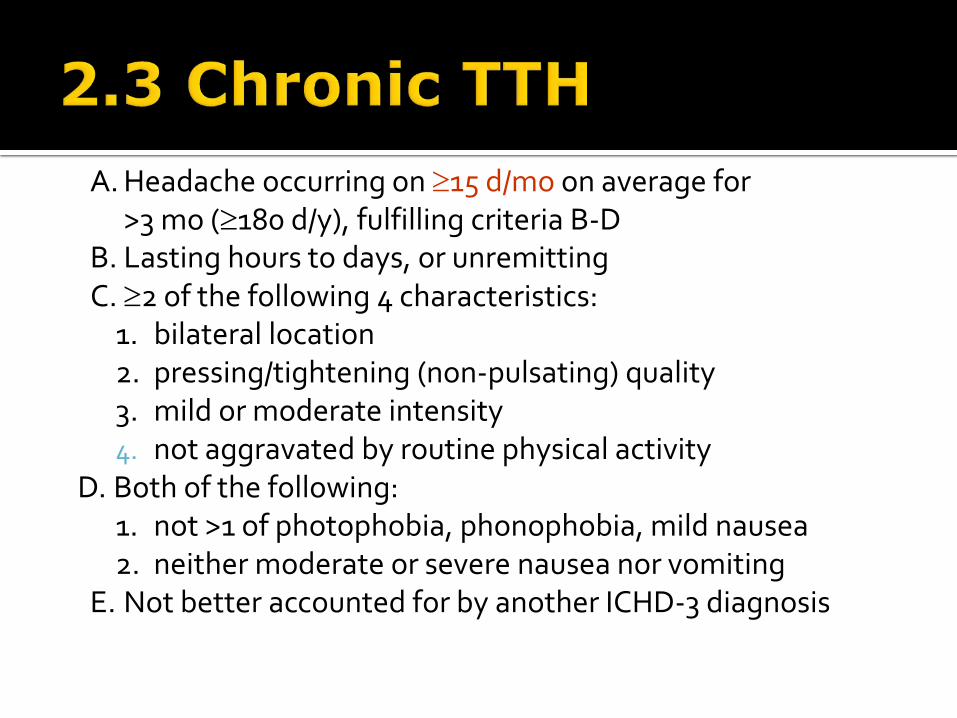
A. Headache occurring on ≥15 d/mo on average for >3 mo (≥180 d/y), fulfilling criteria B-D
B. Lasting hours to days, or unremitting C. ≥2 of the following 4 characteristics:
1. bilateral location 2. pressing/tightening (non-pulsating) quality 3. mild or moderate intensity 4. not aggravated by routine physical activity
D. Both of the following: 1. not >1 of photophobia, phonophobia, mild nausea 2. neither moderate or severe nausea nor vomiting
E. Not better accounted for by another ICHD-3 diagnosis

2.3.1 Chronic tension-type headache associated with pericranial tenderness A. Headache fulfilling criteria for
2.3 Chronic tension-type headache B. Increased pericranial tenderness on manual
palpation
2.3.2 Chronic tension-type headache not associated with pericranial tenderness A. Episodes fulfilling criteria for
2.3 Chronic tension-type headache B. No increase in pericranial tenderness

2.4.1 Probable infrequent episodic TTH A. One or more episodes fulfilling all but one of criteria
A-D for 2.1 Infrequent episodic tension-type headache B. Not fulfilling ICHD-3 criteria for any other headache
disorder C. Not better accounted for by another ICHD-3 diagnosis
2.4.2 Probable frequent episodic TTH A. Episodes fulfilling all but one of criteria A-D for
2.2 Frequent episodic tension-type headache B. Not fulfilling ICHD-3 criteria for any other headache
disorder C. Not better accounted for by another ICHD-3 diagnosis

2.4.3 Probable chronic TTH A. Headache fulfilling all but one of criteria A-D for
2.3 Chronic tension-type headache B. Not fulfilling ICHD-3 criteria for any other headache
disorder C. Not better accounted for by another ICHD-3 diagnosis

NSAID
AAC
Ketorolac 60 mg IM
Non-pharmacologic Heat Ice Massage Rest Biofeedback

Amitriptyline
Stress management/relaxation techniques
Physical therapy

History gives the clues Examination is important Imaging will clarify when necessary Management is worthwhile Treatment is available, safe and effective

"I'm very brave generally," he went on in a low voice: "only today I happen to have a headache." - Lewis Carroll
http://quotes.dictionary.com/search/migraine_headache?page=1#Zs22kI0pCbdBe0vl.99