dr jamal naim phd in orthodontics tissue of the teeth dentin
TRANSCRIPT

Dr Jamal NaimPhD in Orthodontics
Tissue of the teeth
Dentin

Age and functional changes
1. Physiologic regular secondary dentin2. Pathologic irregular secondary dentin3. Transparent (sclerotic) dentin

Physiologic regular secondary dentin
Secondary D
Primary D

Physiologic regular secondary dentin
• This is the type of dentin formed under Physiologic conditions after complete root formation.
• It is deposited continuously as long as the pulp is vital.
• It is formed at a lower rate and is separated by a darkly stained line from primary dentin
• It has less number of tubules.• It occurs in the entire pulpal surface.• Higher deposition at the roof and floor of the
pulp chamber.

Physiologic regular secondary dentin
CPD
Reparative D
CPD

Physiologic regular secondary dentin
• The size of the pulp cavity decreases and obliteration of the pulp horns
• The course of the dentin canals is more irregular

Pathologic irregular secondary dentin
• It is also known as tertiary or reparative dentin
• This type of dentin is formed as a protection for the pulp against severe stimulus (pathological conditions or irritations), such as
• Attrition• Caries• Preparations
• It is formed at a localized area (e.g. pulp horn) • Some UMC in the subodontoblastic layer
differentiate to new odontoblast to form dentin.

Pathologic irregular secondary dentin
• The number of the tubules is reduced.
• Tertiary dentin has frequently twisted tubules
• Some areas doesn’t contain tubules
• Reparative dentin is separated from other types by a darkly stained line.

Pathologic irregular secondary dentin
Tertiary dentin
secondary dentin

Types of reparative dentin• Osteodentin: The odontoblasts (cells) are
included in the formed dentin

Types of reparative dentin• Atubular dentin: areas without tubules

Types of reparative dentin• Vasodentin: entrapped blood vessels

Types of secondary dentinRegular
Cause: mild stimuli (slow attrition, slowly progressing caries)
Site of formation: entire pulpal surface (thicker on pulp roof and floor)
Tubules: wavy course, decrease in number
irregularCause: severe stimuli,
severe attrition, erosion, deep caries,
Site of formation: located (eg pulp horn)
Tubules: wavy and twisted course, decrease in number or atubular

Types of secondary dentinRegular
Line of demarcation: stain dark
Clinically:The increase of the
dentin thickness and the closure of the pulp horns make it much less possible to expose the pulp chamber during preparation.
IrregularLine of demarcation:
stain dark
Clinically:Functions as a barrier
for against caries.

Transparent (Sclerotic) dentin• Sclerotic dentin can be seen as physiological
change (elderly dentin) or pathological change (caries, attrition, deep fillings, ) in primary or secondary dentin.
• Partial or complete obliteration of the dentin tubules, at first thickining of peritubular dentin, then complete obliteration of the tubules with intertubular d.
• Higher mineralized, harder and denser than normal dentin
• Appears light in transmitted light and dark in reflected light.
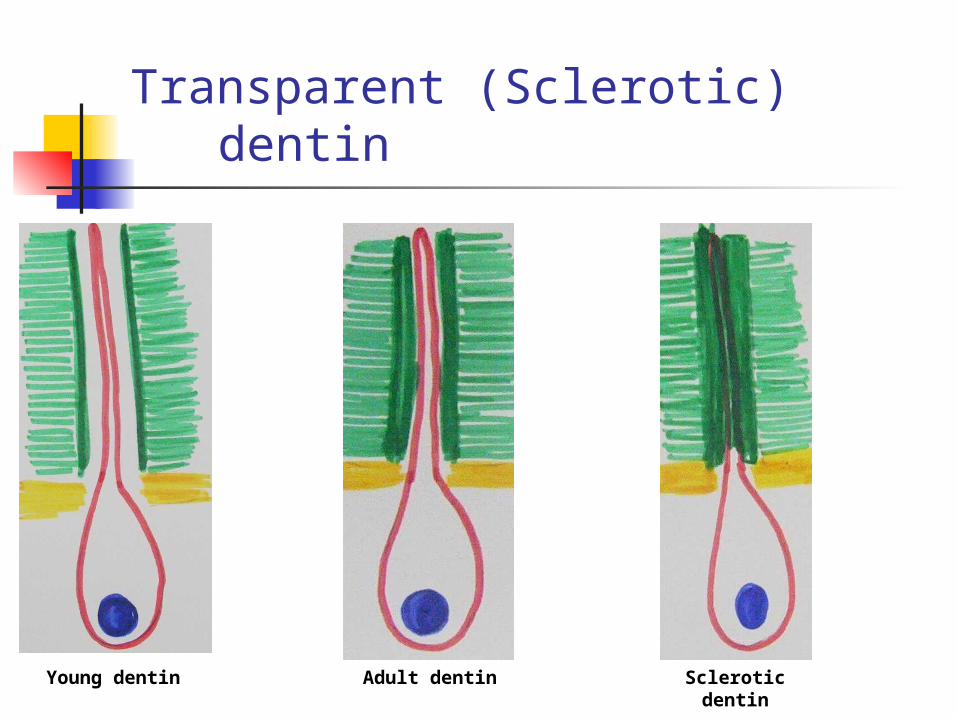
Transparent (Sclerotic) dentin
Young dentin
Adult dentin Sclerotic dentin

Transparent (Sclerotic) dentin

Dead tracts• Severe stimulation to dentin leads to
destruction or disintegration of the odontoblastic process and odontoblasts.
• The dentin tubules are empty and filled with air.
• Most often in areas of narrow pulp horns due to odontoblastic crowding. In ground section they appear black.
• Often surrounds with sclerotic dentin.

Dead tracts

Dead tracts

Dead tracts

Vitality and sensitivity of dentin
Vitality of dentin is its ability to react following physiological or pathological stimuli.
Forming secondary or tertiary dentin, feeling pain are signs of being vital.
Several theories have been cited to explain the mechanism involved in dentinal sensitivity & vitality:
The transducer theory, the conduction theory, the modulation theory the Brännström's hydrodynamic theory.

The transducer theory contend that the odontoblast and its process are capable to mediate neural impulse in the same way as nerve cells.
Contra:But investigations have proved that no pain is
experienced in exposed dentin by application of substance known to bare nerve endings.
The measurement of membrane potential of the odontoblasts shows clearly that this potential is very low to contribute in the pain excitation.
The transducer theory

The transducer theory

The conduction theory (intratubular innervation theory) contend that dentin is richly innervated and those nerves mediate the impulse to the brain.
Some new studies show that predentin and the first layer of circumpulpal dentin (0.2mm) is innervated with nerve fiber from the raschkows plexus.
The fibers run parallel ro the tomes fiber in the dentin tubules.
The density of those fiber is much higher in the coronal dentin than cervical dentin. Root dentin doesn’t include such fibers.
The conduction theory

The conduction theory

Some authors contend that those fibers end at the DEJ, but can not be seen in histological slides.
Contra:It is uncapable to explain the higher sensitivity at
the cemento-enamel junction than that felt at other areas.
The conduction theory

The conduction theory

The hydrodynamic theory
The “hydrodynamic theory”, developed in the 1960’s is the widely accepted physiopathological theory of Dentin Sensitivity.
Temperature, physical osmotic changes or electrical and chemical stimuli and dehydration are the most pain-inducing stimuli.
According to this theory, those stimuli increase centrifugal fluid flow within the dentinal tubules, giving rise to a pressure change throughout the entire dentine.
The hydrodynamic theory
The movement stimulates intradentinal nerve receptors sensitive to pressure (BARORECEPTORS), which leads to the transmission of the stimuli .
This simulation generates pain.

The hydrodynamic theory
Berman describes this reaction as: “The coefficient of thermal expansion of the
tubule fluid is about ten times that of the tubule wall. Therefore, heat applied to dentin will result in expansion of the fluid and cold will result in contraction of the fluid, both creating an excitation of the 'mechano-receptor'.”

Vitality and sensitivity of dentin