dr dewald behrens - modbury hospital - the target culture: friend or foe?
TRANSCRIPT

CLINICAL TARGETS – FRIEND OR FOE?
D C Behrens 2015
Difficult…
Primum non nocere
Take the UK
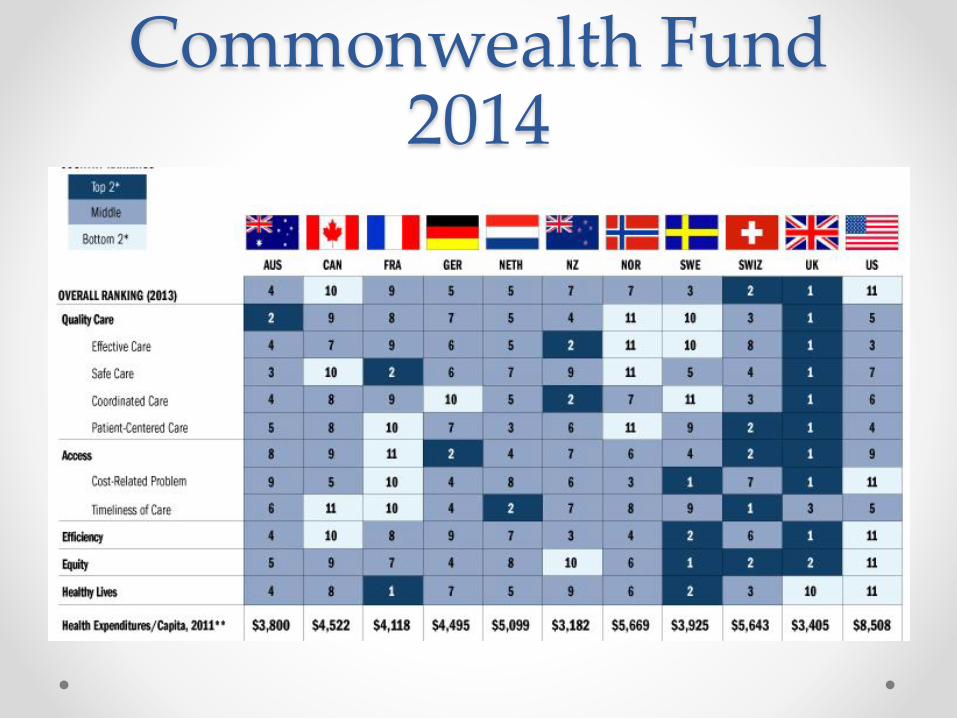
Commonwealth Fund 2014
NHS Target Culture• NHS target culture• A UK term of art referring to the f
ocusing by managers in NHS organisations on objective and tangible goals (targets), including financial targets (e.g., cutting an annual budget by £5 million) or time targets (e.g. being seen within 4 hours by a doctor or nurse in A&E or beginning defi-nitive cancer therapy within 31 days of urgent GP referral, etc.), often to the exclusion of non-objective measures of care quality, including changing of bed linen, responding to call alarms, etc.
1997
• Labour triumphs under
Tony Blair
• NHS reform promised
NHS disasters continue
• Third of buildings built prior to founding of NHS
• 1.8 doctors/1000 – EU average 3.1
• Overcrowding, delays
• Bodies in the chapel
• 1998 Bristol Heart Surgery
• 2000 Shipman murders

2000

Simon Stevens
Simon Stevens
• Medical Advisor to
Tony Blair 2001 – 2004
• Oxford graduate
• NHS manager
• Health policy advisor to
two Labour Health
secretaries 1997 - 2001
• Reform Strategies For The English NHS
•Scarcity Gives Way To Munificence
• One-Dimensional Reform: Support For Providers
• Two-Dimensional Reform: Hierarchical Challenge
• Three-Dimensional Reform: Localist Challenge
• The Search For ‘Constructive Discomfort’
‘Constructive Discomfort’• The past five years have arguably seen three tectonic
shifts in the postwar health policy settlement: an end to the bipartisan political consensus on the role of tax funding; a new bipartisan consensus on the value of a more mixed supply side; and increased challenge to the medical profession’s power. In part this is because of an increasing appreciation of the fact that health care improvement requires a source of tension to overcome the inertia inherent in all human systems.24 The past five years have seen England searching for the optimal policy mix to generate that constructive discomfort. In doing so, it has entered a relatively pragmatic phase compared with its more traditional “path dependency.”25

‘Constructive Discomfort’ continued
• “…important critiques of the notion of clinical freedom
have arisen as a result of the increasingly team-based
nature of clinical care, the greater capital intensity of
services, the costlier nature of health care and the
attendant demands for accountability from payers, the
availability of information showing wide variations in
clinical quality and practice, evidence that professionals
and institutions are sometimes organized for their own
convenience without regard to patients’ preferences,
and consequent pressure from consumer organizations.
Top-down challenge is therefore likely to have an
ongoing place in the English health reform pantheon.”

• The result will be that, at least on the supply side, the
era of English “exceptionalism” in health care is over.

An ED Consequence

Another consequence
Mid Staffs• Catastrophic failings
• More than a thousand people needlessly died
• Yet it was a ‘Foundation trust’
• Data is only as good as the feed
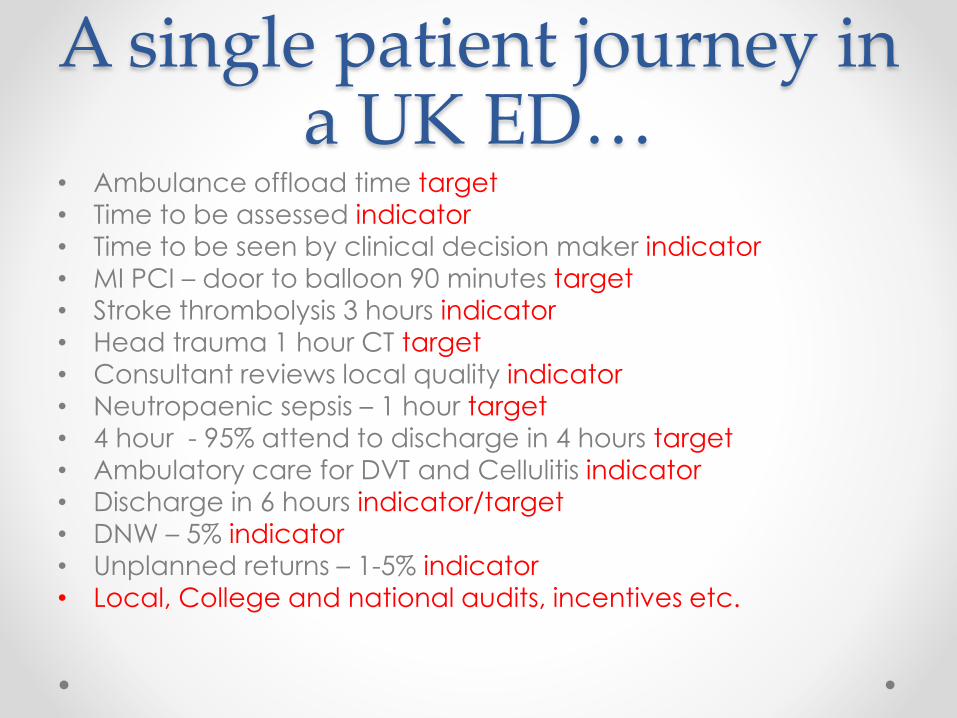
A single patient journey in a UK ED…
• Ambulance offload time target
• Time to be assessed indicator
• Time to be seen by clinical decision maker indicator
• MI PCI – door to balloon 90 minutes target
• Stroke thrombolysis 3 hours indicator• Head trauma 1 hour CT target
• Consultant reviews local quality indicator
• Neutropaenic sepsis – 1 hour target
• 4 hour - 95% attend to discharge in 4 hours target
• Ambulatory care for DVT and Cellulitis indicator
• Discharge in 6 hours indicator/target
• DNW – 5% indicator
• Unplanned returns – 1-5% indicator• Local, College and national audits, incentives etc.
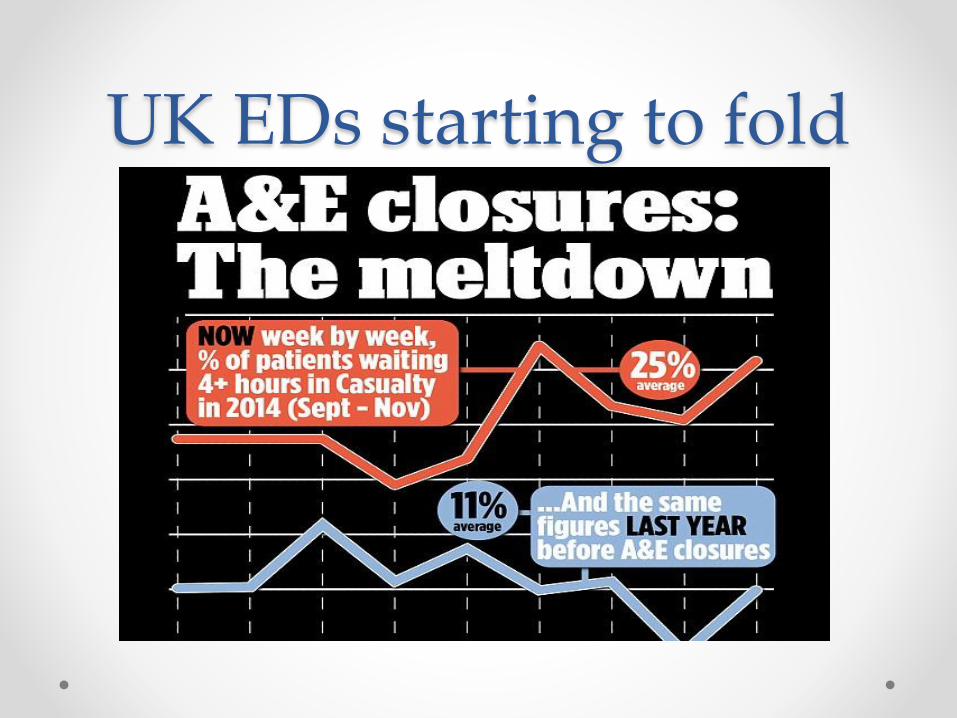
UK EDs starting to fold

So how is it going in Australia?

Targets• Australian triage score is a time based target –
popularly misused data.
• WA adopted 4 hour rule to help with bed block in
2008.
• Chris Baggoley Australian CMO coined the term
NEAT.
• NEST
• Lately NSQHS Clinical standards – not targets!
• Or are they?
• ACEM Quality Framework

So what do we think of targets?

Potential foe
• Potential lack of
professional control
and therefore
responsibility
• Perverse incentives
• Unintended
consequences
• Goalodicy
Friend
• Timeliness is crucial – both in assessment and flow.
• Patients need more multi disciplinary input – this
needs replicable coordination.
• Standardisation through best practice needs a
structured approach with expectations.
What are our future challenges?
• Evidence is not always
what it is cracked up to
be…
• Health remains non linear and complex.
• There is a huge swing between innovation and traditionalism, sometimes in the same service.
• Changes in health happen quickly and on many fronts – this makes proper health programme studies difficult.

Suggestions• The devil is in the detail!
• Ask the right questions
• Challenge perceptions
• Support your colleagues
• Always remember it is about patients
• Engage other specialities – it is a hospital approach
• Make targets work for you!
• My bottom line is that NEAT is the one hospital owned timeliness tool we in the ED can utilise to improve flow. We should be harnessing this, as correctly applied, it has shown to improve patient outcomes and satisfaction, and staff morale.
What happened to the NHS plan 2000?
• Life expectancy – progress
• Health inequalities – deterioration
• Smoking – met
• Mortality rates from heart disease – met
• Inequalities gap in rates of death from heart disease –progress
• Suicide – progress
• Four hour wait – met
• 18 week wait from referral to treatment – met
• Mortality from cancer – met
• Inequality gap in rates of death from cancer – met
• Access to GP services – progress
• Under 18 conception rate - progress

Questions?