downloaded from on june 2, 2015
TRANSCRIPT

A short history of Camp BastionHospital: part 2—Bastion’s catalyticrole in advancing combat casualty careDavid Vassallo
INTRODUCTIONIt’s all about the casualties“They took me to Camp Bastion, the fieldhospital, which took about twentyminutes. Once I reached it, they took medirectly into the operating theatre and thelast thing I remember was a nurse talkingto me. She said to me, ‘Derek, be strong,you’re going to be OK.’”—a personalaccount of ‘right turn resuscitation’ byPrivate Derek Derenalagi, blown up by animprovised explosive device (IED) on 19July 2007, suffering a bilateral transfe-moral amputation, and subsequently clas-sified as an ‘unexpected survivor’.1
A remarkable and inspiring photo-essaybook appeared in 2013, featuring the per-sonal accounts of 36 severely injured sol-diers and marines who, in the words ofGeneral the Lord Dannatt, have “risenabove the hurt their enemies thought theyhad inflicted on them”. 2
Twenty-seven of these servicemen wereinjured in Afghanistan and had been evac-uated from the battlefield to Bastion,where they were managed for less thanone day or two at most, before beingevacuated to Birmingham. It is obviousfrom their stories that by all rights manyof them should not have lived to tell theirtale, but their recollections from Bastionare tantalisingly hazy as most weresedated or anaesthetised en route or onarrival there, waking up days or weekslater in the intensive therapy unit (ITU) inBirmingham.
This article covers the care these ser-vicemen and others would have receivedin that 24 h gap in their testimonials,during their extraction from the battlefieldand after arrival in Bastion, the care thatin those crucial few hours enabled themto join that unique fraternity—the unex-pected survivors of Afghanistan.
COMBAT CASUALTY CAREThe doctrinal revolution underpinningcasualty care in HelmandThe paradigm shift in combat casualtycare that occurred in 2005 shortly before
British troops deployed into HelmandProvince and which was to underpinevery aspect of casualty care there was theformal recognition that catastrophichaemorrhage, designated as <C>, wasthe major killer on the battlefield andneeded to be attended to immediately,even ahead of managing the airway.3 Thisled to the concept of <C> ABC, theacceptance of tourniquets in the militarysetting, which were introduced widelyfrom Op HERRICK 4 in 2006 onwards,novel haemostatic dressings and the devel-opment of the ‘damage control resuscita-tion—damage control surgery’ sequence.Importantly, the rapid spread of concep-tual knowledge and experience across theDMS soon resulted in a critical mass ofhighly motivated individuals who coulddrive further change, and their provingground was Bastion. A whole raft of otherinnovations ensued, such as near pointcoagulation testing in the form of throm-boelastometry (ROTEM), introduced toBastion on a feasibility study in 2009,4
and soon fully integrated into damagecontrol resuscitation,5 followed by doctri-nal and organisational changes.6
Casualty retrieval: Bastion’s MedicalEmergency Response Teams“Then the Chinook helicopter came in totry and get me. It was a huge relief to seeit, but then a rocket-propelled grenade wasfired at it. You’re not allowed to landunder fire, so it withdrew and circled over-head. That’s when I thought, ‘I’m actuallygoing to die here.’… Then the Apacheturned up, and rained fire down on thelocation, taking out the Taliban so thatthe Chinook could come back in andland.”—a personal account by PrivateStringer, blown up by an IED on 19January 2011. He is a triple amputee and‘unexpected survivor’.7
Camp Bastion Hospital was the princi-pal link in the evacuation chain from thebattlegrounds of Helmand, pivotal towhich from the outset were the iconicBritish Medical Emergency ResponseTeams (MERT) based at the hospital. Forspeed of evacuation, and because roadtransport was fraught with the risks ofIEDs, almost all patients were brought to
Bastion Hospital by helicopter, landing atits aptly named Helicopter Landing Site‘Nightingale’.
The MERT was a revolutionaryconcept, taking the most experiencedhealthcare professionals directly to themost critically wounded on the battlefield,which was introduced to Afghanistan onOp HERRICK 4. It had evolved from theIncident Response Teams of the Balkanconflicts of the 1990s and the Iraqcampaign.
The larger capacity of the Royal AirForce’s (RAF) sturdy CH-47 Chinook,which could accommodate 8 stretcherpatients and 20 walking wounded, carrymore equipment and a force protectionteam, and still have space to provide careto casualties, meant it was preferred forcasualty evacuation over all other helicop-ters (Figure 1).8 The Chinook allowed thespecially developed MERT, consisting of aconsultant in anaesthesia or emergencymedicine, a nurse and two paramedics, tobe carried forward of the hospital toprovide in-flight casualty care andadvanced resuscitation. This eventuallyincluded in-flight blood transfusion,which was perhaps the most criticalinnovation.
American medevac flights, which sup-plemented British medevac missions from2009 onwards, were carried out by USArmy UH-60A Blackhawk helicopters(known as DUSTOFF) and USAF HH-60Pave Hawk helicopters (known asPEDRO). These had a quicker responsetime, better night operability and couldfly into ‘hot zones’ at less collective risk,but they had limited capacity and signifi-cantly only carried one or two paramedicsrespectively, so the US Department ofDefense recognised that they could notmatch the MERT’s capability.9
Intelligent tasking of these three differ-ent aeromedical assets contributed to thephysician-led MERT transporting a higherproportion of critically injured casualties,a decision justified by the MERTachievinggreater than predicted survival rates(Figure 2).10
Trauma teams and human factors atBastionThe large multidisciplinary ‘ComplexTrauma Teams’ at Bastion allowedconsultant-delivered care from the ‘frontdoor’ of the emergency department (ED)(Figures 3 and 4), ensuring experienced,early, robust decision-making for thesecritically injured casualties.
There would typically be at least 17members in the trauma team with all themedical roles filled by consultants
Correspondence to Col David Vassallo, Army MedicalDirectorate, Camberley, Surrey GU15 4NP, UK;[email protected]
160 Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from

excepting the primary survey doctor whowas usually the ED specialist registrar(Figure 5). The team consisted of a TeamLeader who was the ED consultant, aPrimary Survey Doctor, two anaesthetistsfor airway and central venous access, anoperating department practitioner, scribe,trauma nurse coordinator, four ED nursesfor intravenous access and first bloodsample, drugs and rapid infuser (×2), arunner, orthopaedic, general and plasticsurgeons, a radiologist and radiographerand the deployed medical director(DMD). Logistic support would be pro-vided by the laboratory technician, theatremanager and Ward Master, while ‘front ofhouse’ support would be provided by aninterpreter, the Squadron Sergeant Majorand the Padre.11
Much of the success of these teams wasdue to exemplary human factors (non-
technical skills) rehearsed and consoli-dated in pre-deployment training andhoned at Bastion, with emphasis on com-munication, situational awareness, leader-ship, followership and teamwork.12 13
Deployed medical directorsAdvances in prehospital medicine anddamage control resuscitation and surgery,the rapid evacuation of critically and mas-sively wounded personnel to BastionHospital, the multinational and interdis-ciplinary challenges of clinical innova-tions, and the high-intensity workload atthis specialist trauma hospital led to theformal development of the role of theDMD in 2009. The DMD worked withinthe administrative command structure,alongside the Commanding Officer andthe Senior Nursing Officer.14
DMDs played a crucial coordinatingrole in meeting these many challenges,smoothing professional interactions, main-taining and developing clinical standardsand addressing ethical dilemmas and gov-ernance issues from one roulement ofhospital staff to another. Moreover, theDMD was the interface between the ‘firstworld’ facilities at Bastion and the severalAfghan civilian, charitable and militarymedical facilities. The movement of localnational casualties and patients, in andout of Bastion, posed significant ethicaland logistic challenges for the DMD andthe military medical command teams(Figure 6).
The DMD was also the interface withother allied hospitals in theatre, especiallywhen it came to transferring casualties forurgent specialist care. Camp BastionHospital was but one component (albeitthe busiest) in a complex and inter-dependent multinational network ofcentres of excellence that included theCanadian/US Hospital at Kandahar forthe treatment of neurosurgical and max-illofacial casualties (a facility that includedBritish surgeons),15 the American hospitalin Bagram and the French Hospital inKabul for eye casualties.
Damage control radiologyWhile CT scanning had been part ofBastion Hospital’s armamentarium sinceJune 2007, consultant radiology input toBastion had initially been limited to tele-radiology support from the UK. In 2009,consultant radiologists became part of thecomplement of British field hospitals. AnAmerican consultant radiologist deployedto Bastion with the first US contingent onOp HERRICK 10A (2009), and in Maythat year a British radiologist was alsoadded to the establishment, with radiolo-gists being included in the traumateam. Consultant-performed Focussed
Figure 1 In Safe Hands Medical Emergency Response Team in action (Stuart Brown).
Figure 2 Medical EmergencyResponse Team with casualty arrivingat Nightingale helipad, Camp BastionHospital (Graeme Lothian).
Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2 161
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from
Abdominal Sonography for Trauma, anddirect digital X-ray facilities (Figure 7),soon added their contribution to traumaresuscitation.
The first CT scanner ever to bedeployed in a British field hospital hadbeen installed at British Military HospitalShaibah in Iraq in 2005. When one rea-lises that the first 100 CT scans at BMHShaibah were taken over a 13-monthperiod, followed by 66 scans in July2007, and then compares this with the100 trauma CT scans performed atBastion in a 10-day period alone in July2010, one can better appreciate both thevastly different tempo of war fightingbetween the two theatres and the clinical
utility of rapid CT in the evaluation oftrauma (Figure 8).16
Damage control resuscitation anddamage control surgery at BastionGunshot wounds accounted for themajority of trauma patients received atBastion Hospital in 2006–2007.Thereafter, the Taliban insurgencyadapted its modus operandi to deployincreasingly sophisticated and effectiveIEDs, which became the signature weaponof the Afghan conflict.17 IEDs caused>60% of all UK fatalities in Afghanistan.The high (often bilateral) transfemoralamputation with mutilating perineal andsignificant pelvic injury became the
signature injury pattern, with the surgicalworkload changing considerably as aresult. 18
Rapid helicopter evacuation of casual-ties with MERT resuscitation en routeresulted in such patients usually arrivingalive in Bastion, but at the limits of theirphysiological reserve. Critical decision-making by experienced consultants inemergency medicine, anaesthesia andsurgery, coupled with damage controlresuscitation, with massive transfusionaccording to strict protocols,11 includingthe novel and effective use of tranexamicacid and cryoprecipitate,19 damagecontrol surgery and radiology, all contrib-uted to achieve unprecedented survivalrates for these hugely traumatised casual-ties. Overall 98% of those who made italive to Bastion survived.20 Between April2006 and July 2008, there were 75 unex-pected survivors out of nearly 300 severetrauma cases presenting to Iraq andAfghanistan,21 22 this 25% ratio being instark contrast to the best National HealthService ratio of 6%, and this remarkableratio was maintained in Bastion throughlater years. By the end of 2011, SurgeonVice-Admiral Raffaelli, the SurgeonGeneral, could report to the House ofCommons that there had been some 210‘unexpected survivors’ in the previous fiveyears,23 and by the end of conflict opera-tions in 2014 it is estimated that therehave been some 300 in all.
Right turn resuscitationThe concept of selective ‘right turn resus-citation’ was introduced in Bastion on OpHERRICK 7 in 2007 and refined there-after.24 It was the process whereby critic-ally unstable casualties identified en routeto hospital would bypass the emergencyroom altogether, going directly into theoperating theatre for surgical control ofproximal haemorrhage, followed by rapidCT imaging, ongoing resuscitation and ashort period of ITU stabilisation. Thiswould usually be followed by a return totheatre for further damage controlsurgery (Figure 9). The ‘right turn’reflected the geographical location of theBastion theatres on the right side of theED corridor, but its ethos symbolisedtaking the right decision for the rightpatient at the right time followed by theright response.
Casualties under 16 years oldOnly those who have never deployed towar could assume that casualties dealtwith by a military hospital are all adultcombatants. Civilians—men and women,the elderly, children and babies—formed a
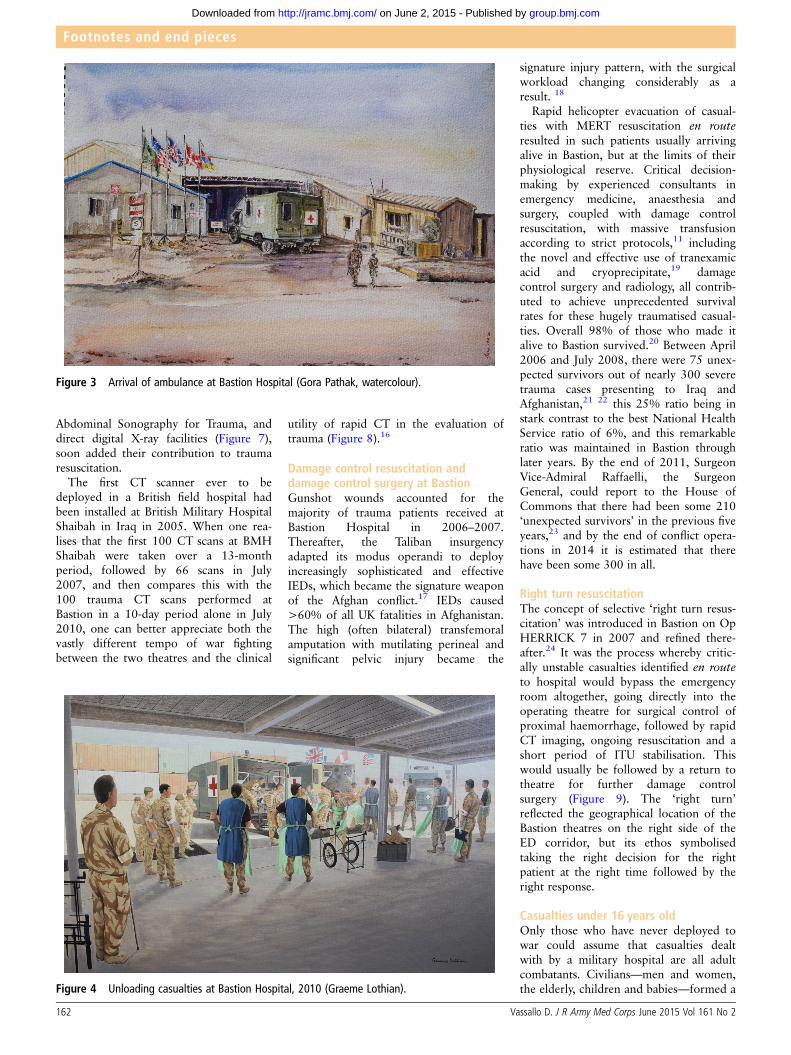
Figure 3 Arrival of ambulance at Bastion Hospital (Gora Pathak, watercolour).
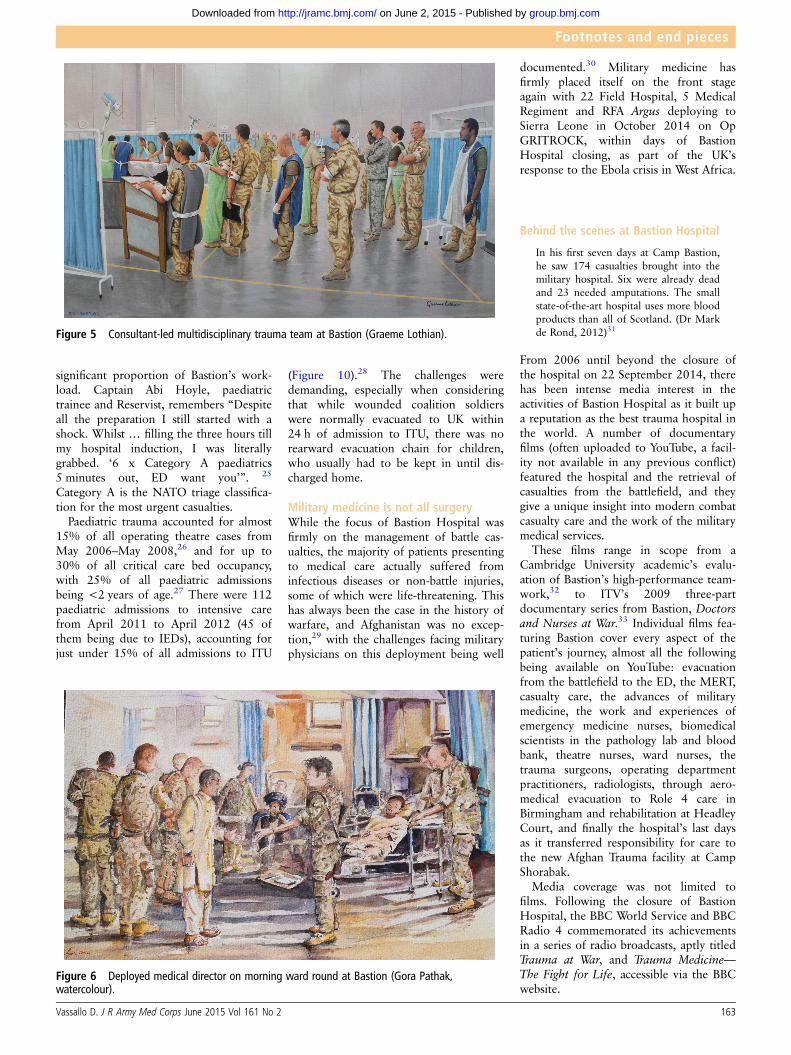
Figure 4 Unloading casualties at Bastion Hospital, 2010 (Graeme Lothian).
162 Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from
significant proportion of Bastion’s work-load. Captain Abi Hoyle, paediatrictrainee and Reservist, remembers “Despiteall the preparation I still started with ashock. Whilst … filling the three hours tillmy hospital induction, I was literallygrabbed. ‘6 x Category A paediatrics5 minutes out, ED want you’”. 25
Category A is the NATO triage classifica-tion for the most urgent casualties.
Paediatric trauma accounted for almost15% of all operating theatre cases fromMay 2006–May 2008,26 and for up to30% of all critical care bed occupancy,with 25% of all paediatric admissionsbeing <2 years of age.27 There were 112paediatric admissions to intensive carefrom April 2011 to April 2012 (45 ofthem being due to IEDs), accounting forjust under 15% of all admissions to ITU
(Figure 10).28 The challenges weredemanding, especially when consideringthat while wounded coalition soldierswere normally evacuated to UK within24 h of admission to ITU, there was norearward evacuation chain for children,who usually had to be kept in until dis-charged home.
Military medicine is not all surgeryWhile the focus of Bastion Hospital wasfirmly on the management of battle cas-ualties, the majority of patients presentingto medical care actually suffered frominfectious diseases or non-battle injuries,some of which were life-threatening. Thishas always been the case in the history ofwarfare, and Afghanistan was no excep-tion,29 with the challenges facing militaryphysicians on this deployment being well
documented.30 Military medicine hasfirmly placed itself on the front stageagain with 22 Field Hospital, 5 MedicalRegiment and RFA Argus deploying toSierra Leone in October 2014 on OpGRITROCK, within days of BastionHospital closing, as part of the UK’sresponse to the Ebola crisis in West Africa.
Behind the scenes at Bastion Hospital
In his first seven days at Camp Bastion,he saw 174 casualties brought into themilitary hospital. Six were already deadand 23 needed amputations. The smallstate-of-the-art hospital uses more bloodproducts than all of Scotland. (Dr Markde Rond, 2012)31
From 2006 until beyond the closure ofthe hospital on 22 September 2014, therehas been intense media interest in theactivities of Bastion Hospital as it built upa reputation as the best trauma hospital inthe world. A number of documentaryfilms (often uploaded to YouTube, a facil-ity not available in any previous conflict)featured the hospital and the retrieval ofcasualties from the battlefield, and theygive a unique insight into modern combatcasualty care and the work of the militarymedical services.
These films range in scope from aCambridge University academic’s evalu-ation of Bastion’s high-performance team-work,32 to ITV’s 2009 three-partdocumentary series from Bastion, Doctorsand Nurses at War.33 Individual films fea-turing Bastion cover every aspect of thepatient’s journey, almost all the followingbeing available on YouTube: evacuationfrom the battlefield to the ED, the MERT,casualty care, the advances of militarymedicine, the work and experiences ofemergency medicine nurses, biomedicalscientists in the pathology lab and bloodbank, theatre nurses, ward nurses, thetrauma surgeons, operating departmentpractitioners, radiologists, through aero-medical evacuation to Role 4 care inBirmingham and rehabilitation at HeadleyCourt, and finally the hospital’s last daysas it transferred responsibility for care tothe new Afghan Trauma facility at CampShorabak.
Media coverage was not limited tofilms. Following the closure of BastionHospital, the BBC World Service and BBCRadio 4 commemorated its achievementsin a series of radio broadcasts, aptly titledTrauma at War, and Trauma Medicine—The Fight for Life, accessible via the BBCwebsite.
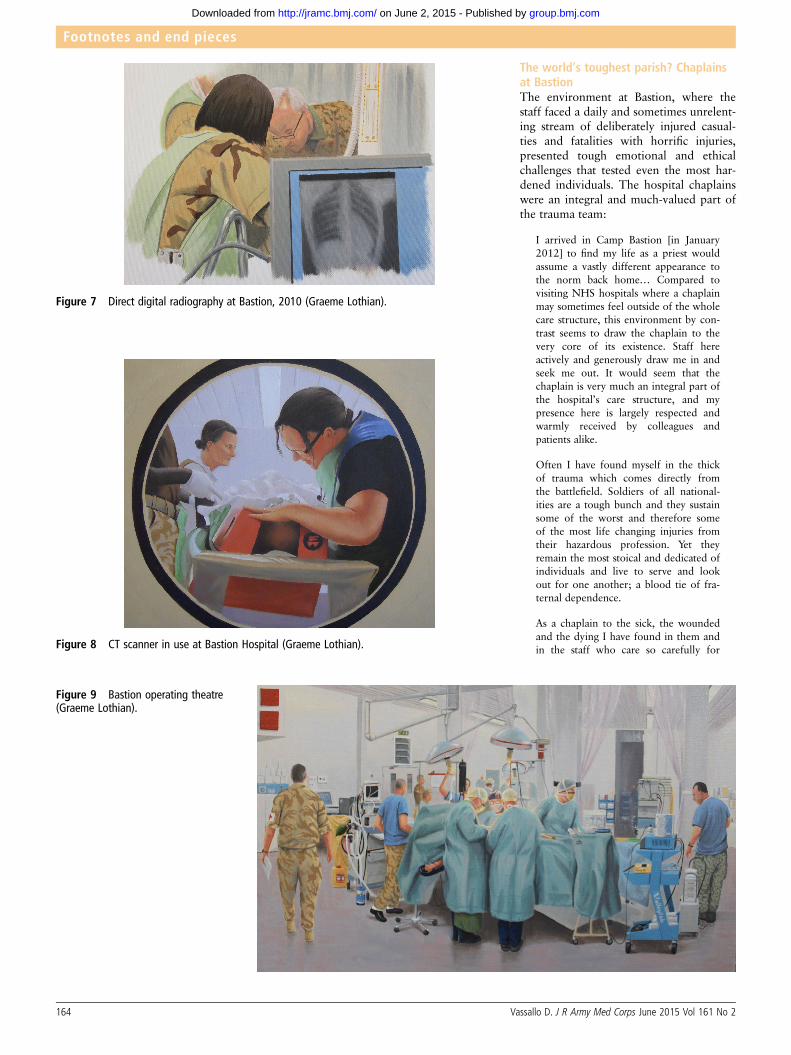
Figure 5 Consultant-led multidisciplinary trauma team at Bastion (Graeme Lothian).
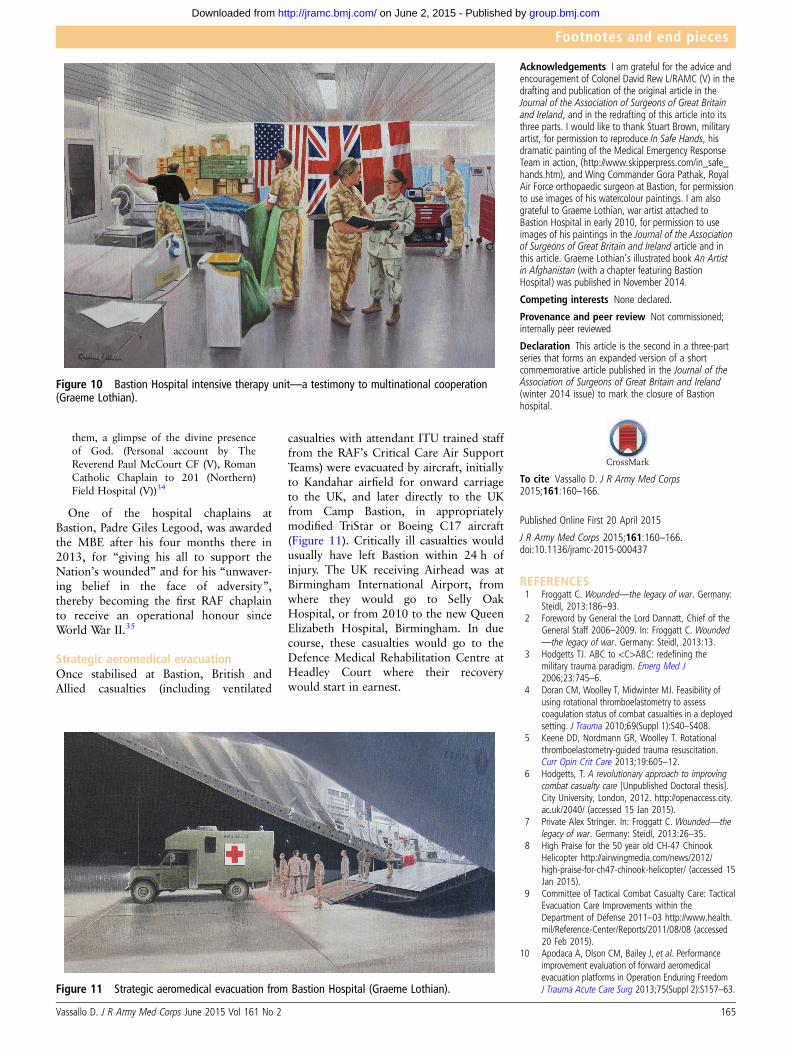
Figure 6 Deployed medical director on morning ward round at Bastion (Gora Pathak,watercolour).
Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2 163
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from
The world’s toughest parish? Chaplainsat BastionThe environment at Bastion, where thestaff faced a daily and sometimes unrelent-ing stream of deliberately injured casual-ties and fatalities with horrific injuries,presented tough emotional and ethicalchallenges that tested even the most har-dened individuals. The hospital chaplainswere an integral and much-valued part ofthe trauma team:
I arrived in Camp Bastion [in January2012] to find my life as a priest wouldassume a vastly different appearance tothe norm back home… Compared tovisiting NHS hospitals where a chaplainmay sometimes feel outside of the wholecare structure, this environment by con-trast seems to draw the chaplain to thevery core of its existence. Staff hereactively and generously draw me in andseek me out. It would seem that thechaplain is very much an integral part ofthe hospital’s care structure, and mypresence here is largely respected andwarmly received by colleagues andpatients alike.
Often I have found myself in the thickof trauma which comes directly fromthe battlefield. Soldiers of all national-ities are a tough bunch and they sustainsome of the worst and therefore someof the most life changing injuries fromtheir hazardous profession. Yet theyremain the most stoical and dedicated ofindividuals and live to serve and lookout for one another; a blood tie of fra-ternal dependence.
As a chaplain to the sick, the woundedand the dying I have found in them andin the staff who care so carefully for
Figure 7 Direct digital radiography at Bastion, 2010 (Graeme Lothian).
Figure 8 CT scanner in use at Bastion Hospital (Graeme Lothian).
Figure 9 Bastion operating theatre(Graeme Lothian).
164 Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from
them, a glimpse of the divine presenceof God. (Personal account by TheReverend Paul McCourt CF (V), RomanCatholic Chaplain to 201 (Northern)Field Hospital (V))34
One of the hospital chaplains atBastion, Padre Giles Legood, was awardedthe MBE after his four months there in2013, for “giving his all to support theNation’s wounded” and for his “unwaver-ing belief in the face of adversity”,thereby becoming the first RAF chaplainto receive an operational honour sinceWorld War II.35
Strategic aeromedical evacuationOnce stabilised at Bastion, British andAllied casualties (including ventilated
casualties with attendant ITU trained stafffrom the RAF’s Critical Care Air SupportTeams) were evacuated by aircraft, initiallyto Kandahar airfield for onward carriageto the UK, and later directly to the UKfrom Camp Bastion, in appropriatelymodified TriStar or Boeing C17 aircraft(Figure 11). Critically ill casualties wouldusually have left Bastion within 24 h ofinjury. The UK receiving Airhead was atBirmingham International Airport, fromwhere they would go to Selly OakHospital, or from 2010 to the new QueenElizabeth Hospital, Birmingham. In duecourse, these casualties would go to theDefence Medical Rehabilitation Centre atHeadley Court where their recoverywould start in earnest.
Acknowledgements I am grateful for the advice andencouragement of Colonel David Rew L/RAMC (V) in thedrafting and publication of the original article in theJournal of the Association of Surgeons of Great Britainand Ireland, and in the redrafting of this article into itsthree parts. I would like to thank Stuart Brown, militaryartist, for permission to reproduce In Safe Hands, hisdramatic painting of the Medical Emergency ResponseTeam in action, (http://www.skipperpress.com/in_safe_hands.htm), and Wing Commander Gora Pathak, RoyalAir Force orthopaedic surgeon at Bastion, for permissionto use images of his watercolour paintings. I am alsograteful to Graeme Lothian, war artist attached toBastion Hospital in early 2010, for permission to useimages of his paintings in the Journal of the Associationof Surgeons of Great Britain and Ireland article and inthis article. Graeme Lothian’s illustrated book An Artistin Afghanistan (with a chapter featuring BastionHospital) was published in November 2014.
Competing interests None declared.
Provenance and peer review Not commissioned;internally peer reviewed
Declaration This article is the second in a three-partseries that forms an expanded version of a shortcommemorative article published in the Journal of theAssociation of Surgeons of Great Britain and Ireland(winter 2014 issue) to mark the closure of Bastionhospital.
To cite Vassallo D. J R Army Med Corps2015;161:160–166.
Published Online First 20 April 2015
J R Army Med Corps 2015;161:160–166.doi:10.1136/jramc-2015-000437
REFERENCES1 Froggatt C. Wounded—the legacy of war. Germany:
Steidl, 2013:186–93.2 Foreword by General the Lord Dannatt, Chief of the
General Staff 2006–2009. In: Froggatt C. Wounded—the legacy of war. Germany: Steidl, 2013:13.
3 Hodgetts TJ. ABC to <C>ABC: redefining themilitary trauma paradigm. Emerg Med J2006;23:745–6.
4 Doran CM, Woolley T, Midwinter MJ. Feasibility ofusing rotational thromboelastometry to assesscoagulation status of combat casualties in a deployedsetting. J Trauma 2010;69(Suppl 1):S40–S408.
5 Keene DD, Nordmann GR, Woolley T. Rotationalthromboelastometry-guided trauma resuscitation.Curr Opin Crit Care 2013;19:605–12.
6 Hodgetts, T. A revolutionary approach to improvingcombat casualty care [Unpublished Doctoral thesis].City University, London, 2012. http://openaccess.city.ac.uk/2040/ (accessed 15 Jan 2015).
7 Private Alex Stringer. In: Froggatt C. Wounded—thelegacy of war. Germany: Steidl, 2013:26–35.
8 High Praise for the 50 year old CH-47 ChinookHelicopter http://airwingmedia.com/news/2012/high-praise-for-ch47-chinook-helicopter/ (accessed 15Jan 2015).
9 Committee of Tactical Combat Casualty Care: TacticalEvacuation Care Improvements within theDepartment of Defense 2011–03 http://www.health.mil/Reference-Center/Reports/2011/08/08 (accessed20 Feb 2015).
10 Apodaca A, Olson CM, Bailey J, et al. Performanceimprovement evaluation of forward aeromedicalevacuation platforms in Operation Enduring FreedomJ Trauma Acute Care Surg 2013;75(Suppl 2):S157–63.
Figure 10 Bastion Hospital intensive therapy unit—a testimony to multinational cooperation(Graeme Lothian).
Figure 11 Strategic aeromedical evacuation from Bastion Hospital (Graeme Lothian).
Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2 165
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from
11 Mercer SJ, Tarmey NT, Woolley T, et al. Haemorrhageand coagulopathy in the Defence Medical Services.Anaesthesia 2013;68(Suppl 1):49–60.
12 Midwinter MJ, Mercer S, Lambert AW, et al. Makingdifficult decisions in major military trauma: a crewresource management rerspective. J R Army MedCorps 2011;157(Suppl 1):S299–304.
13 Mercer S, Arul GS, Pugh HEJ. Performanceimprovement through best practice teammanagement: human factors in complex trauma. J RArmy Med Corps 2014;160:105–8.
14 Mahoney PF, Hodgetts TJ, Hicks I. The deployedmedical director: managing the challenges of acomplex trauma system. J R Army Med Corps2011;157(3 Suppl 1):S350–6.
15 Eisenburg MF, Christie M, Mathew P. Battlefieldneurosurgical care in the current conflict in southernAfghanistan. Neurosurg Focus 2010;28:1–6.
16 Gay DAT, Miles RM. Use of Imaging in TraumaDecision-Making. J R Army Med Corps 2011;157(3Suppl 1):S289–92.
17 Johnson TH. Taliban adaptations and innovations.Small Wars & Insurgencies 2013;24:3–27.
18 Jacobs N, Taylor DM, Parker PJ. Changes in surgicalworkload at the JF Med Gp Role 3 Hospital, CampBastion, Afghanistan, November 2008–November2010. Injury 2012;43:1037–40.
19 Morrison JJ, Ross JD, Dubose JJ, et al. Association ofcryoprecipitate and tranexamic acid with improvedsurvival following wartime injury—findings fromthe MATTERs II Study. JAMA Surg 2013;148:218–25.
20 NHS adopts trauma skills developed at militaryhospital in Afghanistan. The Independent, 2November 2014. http://www.independent.co.uk/life-style/health-and-families/health-news/nhs-adopts-trauma-skills-developed-at-military-hospital-in-afghanistan-9833603.html (accessed 17 Jan 2015).
21 Russell R, Hodgetts T, McLeod J. et al. The role oftrauma scoring in developing trauma clinicalgovernance in the Defence Medical Services PhilTrans Royal Society B 2011:366:171–91.
22 Emergency care on the battlefield. NHS Choiceshttp://www.nhs.uk/Livewell/Militarymedicine/Pages/Survivingbattlefield.aspx (accessed 17 Jan 2015).
23 House of Commons Defence Committee. Advances inmedical care resulting in more personnel survivinginjuries, in: The Armed Forces Covenant in Action?Part 1: Military Casualties, (HC 762). Seventh Reportof Session 2010–12, p.15, Q310. (London: TheStationery Office, 15 December 2011). http://www.parliament.uk/business/committees/committees-a-z/commons-select/defence-committee/inquiries/parliament-2010/the-military-covenant-in-action-part-1-military-casualies/ (accessed 8 Mar 2015).
24 Tai NRM, Russell R. Right turn resuscitation:frequently asked questions. J R Army Med Corps2011;157(3 Suppl 1):S310–4.
25 Hoyle A. Being a baby doctor in Bastion. The Medic2012;2:25–6.
26 Ramasamy A, Hinsley DE, Edwards DS, et al. Skillsets and competencies for the modern militarysurgeon: Lessons from UK military operationsin Southern Afghanistan. Injury 2010;41:453–9.
27 Nordmann GR, McNicholas JJ, Templeton PA, et al.Paediatric Trauma Management on Deployment.J R Army Med Corps 2011;157(3 Suppl 1):S334–43.
28 Inwald DP, Arul GS, Montgomery M, et al.Management of children in the deployed intensivecare unit at Camp Bastion, Afghanistan J R ArmyMed Corps 2014;160:236–40.
29 Bailey MS. A brief history of British militaryexperiences with infectious and tropical diseases. J RArmy Med Corps 2013;159:150–7.
30 Wilson DR. Highlights of this edition. J R Army MedCorps 2013;159:3.
31 Blood, sweat and. . .a game of cards: Inside CampBastion’s trauma clinic where lives of British soldiersrest in hands of elite medics. Daily Mail, 27 June2012 http://www.dailymail.co.uk/news/article-2165225/Photos-reveal-life-Camp-Bastions-trauma-.html (accessed 15 Jan 2015).
32 University of Cambridge. Mark de Rond—Welcometo Bastion: warzone ethnography with the combatsurgeons http://www.cam.ac.uk/research/news/welcome-to-bastion-warzone-ethnography-with-the-combat-surgeons (accessed 17 Jan 2015).
33 Doctors and Nurses at War http://www.qaranc.co.uk/doctors_and_nurses_at-war.php (accessed 25 Jan2015).
34 McCourt P. From Parish Priest to Camp Bastion. J RArmy Chaplains Department 2012;51:25.
35 Royal Air Force. The World’s Toughest Parish. http://www.raf.mod.uk/news/archive/the-worlds-toughest-parish-10112014 (accessed 25 Jan 2015).
166 Vassallo D. J R Army Med Corps June 2015 Vol 161 No 2
Footnotes and end pieces
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from
combat casualty careBastion's catalytic role in advancing−−part 2
A short history of Camp Bastion Hospital:
David Vassallo
doi: 10.1136/jramc-2015-00043720, 2015
2015 161: 160-166 originally published online AprilJ R Army Med Corps
http://jramc.bmj.com/content/161/2/160Updated information and services can be found at:
These include:
References #BIBLhttp://jramc.bmj.com/content/161/2/160
This article cites 22 articles, 10 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on June 2, 2015 - Published by http://jramc.bmj.com/Downloaded from