
WORLD COPD DAYNovember 20, 2013
WORLD COPD DAYNovember 20, 2013
Raising COPD Awareness WorldwideRaising COPD Awareness Worldwide© 2013 Global Initiative for Chronic Obstructive Lung Disease

Chronic Obstructive Pulmonary Disease (COPD): Improving Fiscal and Health
Impact through Accountable Care
Guy W. Soo Hoo, MD, MPHPulmonary and Critical Care Section
West Los Angeles VA Healthcare CenterLos Angeles, CA

WORLD COPD DAY 2013: It’s not too late
How many people have COPD?Worldwide, one in 10 adults over age 40 may have COPD. COPD is most common in countries where cigarette smoking has been, or still is, very widespread. How many lives are lost to COPD?Worldwide, nearly 3 million people die from COPD every year.According to a report commissioned by the World Bank, COPD is the third leading cause of death worldwide, surpassed only by heart attack and stroke.
In the United States in 2005, the direct costs of COPD were $21.8 billion and the indirect costs totaled $17 billion.
World COPD Day 2013 is organized by the Global Initiative for Chronic Obstructive Lung Disease (www.goldcopd.org).

COPD: perceptions of disease• COPD is a disease of smokers• COPD is a disease of men • COPD is a disease of elderly adults• COPD only affects the lungs• COPD is diagnosed too late for any treatment• COPD results an progressive decline• COPD results in permanent disability• COPD is unmanageable• COPD is untreatable

Pauwels R, Rabe K:. Lancet 2004; 304: 613-20
Death rates of major cardiopulmonary diseases


Global Strategy for Diagnosis, Management and Prevention of COPD
Definition of COPD COPD, a common preventable and
treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases.
Exacerbations and comorbidities contribute to the overall severity in individual patients.© 2013 Global Initiative for Chronic Obstructive Lung Disease

Petty T. Chest 2002: 1219(S):116S

Prevalence of COPD in the US 2007-2009
Akinbami L , Liu X. NCHS Data brief; 2011 (6): 1-8
Most people with COPD are < 75 years of ageMost undiagnosed patients with COPD are < 65 years of age

Prevalence of COPD in the US 2007-2009
Akinbami L , Liu X. NCHS Data brief; 2011 (6): 1-8
There are more women with COPD than menCOPD in more common among women than men

Global Strategy for Diagnosis, Management and Prevention of COPD
Risk Factors for COPD
GenesGenes
InfectionsInfections
Socio-economic Socio-economic statusstatus
Aging PopulationsAging Populations© 2013 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD
Diagnosis and Assessment: Key Points
A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and a history of exposure to risk factors for the disease.
Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD.
© 2013 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD
Combined Assessment of COPD
Assess symptoms Assess degree of airflow limitation
using spirometry Assess risk of exacerbations
Combine these assessments for the purpose of improving management of
COPD© 2013 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD
Classification of Severity of Airflow Limitation in COPD*
In patients with FEV1/FVC < 0.70:
GOLD 1: Mild FEV1 > 80% predicted
GOLD 2: Moderate 50% < FEV1 < 80% predicted
GOLD 3: Severe 30% < FEV1 < 50% predicted
GOLD 4: Very Severe FEV1 < 30% predicted
*Based on Post-Bronchodilator FEV1
© 2013 Global Initiative for Chronic Obstructive Lung Disease
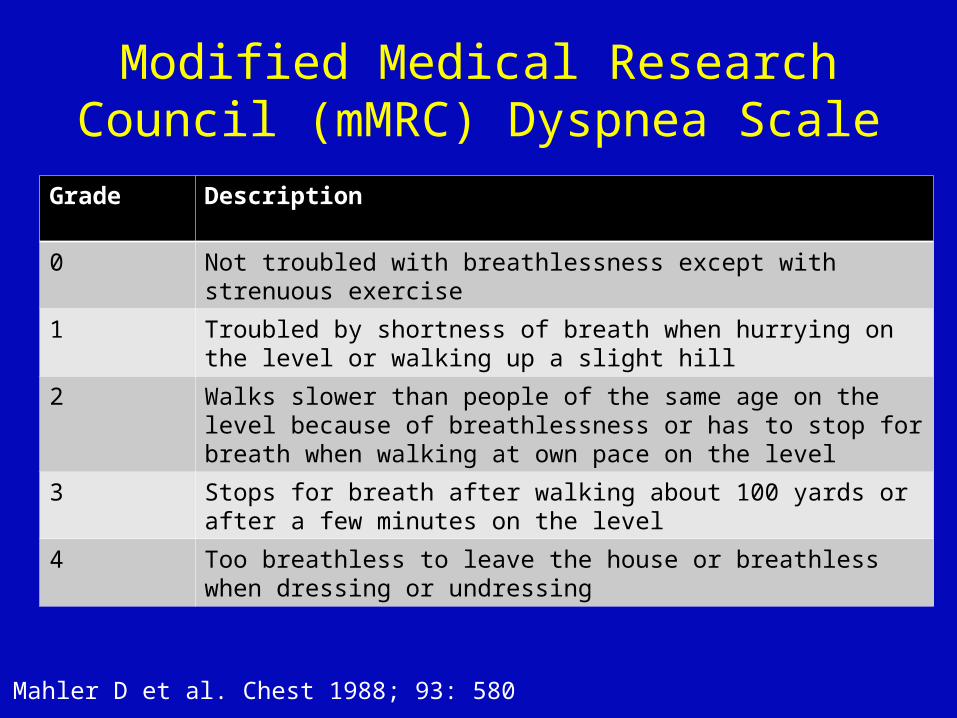
Modified Medical Research Council (mMRC) Dyspnea Scale
Grade Description
0 Not troubled with breathlessness except with strenuous exercise
1 Troubled by shortness of breath when hurrying on the level or walking up a slight hill
2 Walks slower than people of the same age on the level because of breathlessness or has to stop for breath when walking at own pace on the level
3 Stops for breath after walking about 100 yards or after a few minutes on the level
4 Too breathless to leave the house or breathless when dressing or undressing
Mahler D et al. Chest 1988; 93: 580

Patient Characteristic Spirometric Classification
Exacerbations per year
mMRC CAT
ALow Risk
Less SymptomsGOLD 1-2 ≤ 1 0-1 < 10
BLow Risk
More SymptomsGOLD 1-2 ≤ 1 > 2 ≥ 10
CHigh Risk
Less SymptomsGOLD 3-4 > 2 0-1 < 10
DHigh Risk
More SymptomsGOLD 3-4 > 2 > 2
≥ 10
Global Strategy for Diagnosis, Management and Prevention of COPD
Combined Assessment of COPD
When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. One or more hospitalizations for COPD exacerbations should be considered high risk.)
© 2013 Global Initiative for Chronic Obstructive Lung Disease

Relieve symptoms Improve exercise tolerance Improve health status
Prevent disease progression Prevent and treat exacerbations Reduce mortality
Relieve symptoms Improve exercise tolerance Improve health status
Prevent disease progression Prevent and treat exacerbations Reduce mortality
Reducesymptoms
Reducerisk
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Goals of Therapy
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Goals of Therapy
© 2013 Global Initiative for Chronic Obstructive Lung Disease

Identification and reduction of exposure to risk factors are important steps in prevention and treatment.
Individualized assessment of symptoms, airflow limitation, and future risk of exacerbations should be incorporated into the management strategy.
All COPD patients benefit from rehabilitation and maintenance of physical activity.
Pharmacologic therapy is used to reduce symptoms, reduce frequency and severity of exacerbations, and improve health status and exercise tolerance.
Identification and reduction of exposure to risk factors are important steps in prevention and treatment.
Individualized assessment of symptoms, airflow limitation, and future risk of exacerbations should be incorporated into the management strategy.
All COPD patients benefit from rehabilitation and maintenance of physical activity.
Pharmacologic therapy is used to reduce symptoms, reduce frequency and severity of exacerbations, and improve health status and exercise tolerance.
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Key Points
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Key Points
© 2013 Global Initiative for Chronic Obstructive Lung Disease

The natural history of lung function: smoker and non-smokers
Fletcher C, Peto R. BMJ 1997; 1: 1645-8
Smoking cessation decreases the decline in lung function

Avoidance of risk factors
- smoking cessation
- reduction of indoor pollution
- reduction of occupational exposure
Influenza vaccination
Avoidance of risk factors
- smoking cessation
- reduction of indoor pollution
- reduction of occupational exposure
Influenza vaccination
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: All COPD Patients
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: All COPD Patients
© 2013 Global Initiative for Chronic Obstructive Lung Disease

Options in COPD management• Increasing options for treatment
Medications Oxygen therapy Preventive vaccinations Pulmonary rehabilitation Surgical options Lung transplantation
• Biomarkers and genes (ECLIPSE, COPD Gene, SPIROMICS)
• Targeted therapy

COPD: World COPD Day 2013• COPD is a disease of inhaled irritants• COPD is a disease of men and women• COPD is a disease of working adults• COPD is a systemic disease• COPD diagnosis important for treatment• COPD progression is variable• COPD patients are functional• COPD is manageable• COPD is treatable

Patient Protection and Affordable Care Act (PPACA); Affordable Care Act
Enacted 2010; Upheld 2012• Most significant overhaul of US healthcare system
since Medicare and Medicaide (1965)
• Goals of legislation• Increase quality and affordability of health insurance• Lower uninsured rate, expanding insurance coverage• Minimum standards, eliminate exclusion from pre-existing
conditions• Reforms by shifting system towards quality over quantitiy
• Expanding Medicaid and establishing state based health insurance exchanges

Health care providers Heath care plans
Accountable care organizations
What is the impact on COPD?

It’s not too late




The changing face of COPD

Mannino, D et al MMWR 2002: 51: 1-16; Rennard S, et al. Eur Resp J 2002;20: 799-805
Under-diagnosis and unfamiliarity with COPD
Public not aware of “COPD”, ~ 15% aware
Diagnosis on queryCOPD 23%Emphysema 26%Chronic bronchitis 36%
Only about half of patients with COPD diagnosed

How do you know you have COPD?







