
Welcome to WKD in the EU parliament
Norbert Lameire
Chair of the EKHA
Brussels March, 7, 2013
Objectives of EKHA EKHA articulates its mission around five fundamental objectives: 1. Raising awareness of the importance of kidney health and of the need for action to improve the early detection of chronic kidney disease so that preventative strategies can be introduced to minimize its consequences. 2. Promoting a uniformly high standard of care for those with kidney disease throughout Europe by developing consistent strategies for educating and training throughout the EU. 3. Supporting the development of novel strategies and therapeutic approaches for the detection and management of kidney disease through research and its translation into clinical practice. 4. Cooperating with EU health organisations addressing areas linked to kidney disease. 5. Facilitating exchange of information between the European Kidney Community, the EU institutions and organisations in charge of health policy throughout the EU.

STRATEGY FOR ENGAGEMENT 2013-2017
European Chronic Disease Alliance
Confidential - for internal use only

World Kidney Day 2013
The relation AKI-CKD-AKI Norbert Lameire, MD, PhD
Em Prof of Medicine University Hospital
Gent, Belgium Chairman EKHA
EU Parliament, Brussels
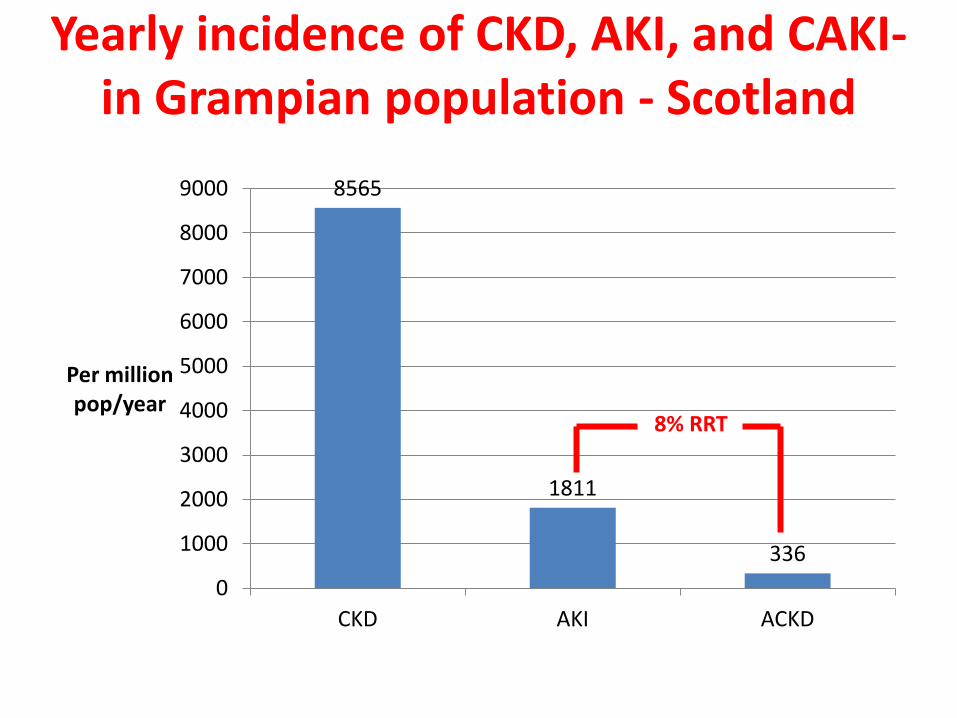
Yearly incidence of CKD, AKI, and CAKI- in Grampian population - Scotland
8565
1811
336 0
1000
2000
3000
4000
5000
6000
7000
8000
9000
CKD AKI ACKD
Per million pop/year
8% RRT

Prognosis of AKI in population-Grampian area-Scotland
7,8 12,5
32,7
39,8 41,4
48,9 49,8
62,5
0
10
20
30
40
50
60
70
AKI CAKI
Percentage
RRT inhospit mortality 90 d mortality 6 mo mortality

Competing “epidemics” of kidney diseases
Disease incidence, 2003 per million person years
Annual mortality rate
ESRD (requiring dialysis) 343 ( 0-1 % per year) 24 %
AKI (requiring dialysis) 295 ( > 7% per year) > 28 %
Modified from Hsu C-Y, J Am Soc Nephrol, 21: 1607-1611, 2010

Immediate and delayed mortality of AKI patients admitted to an ICU
Van Berendoncks et al, Clin J Am Soc Nephrol 5: 1755–1762, 2010
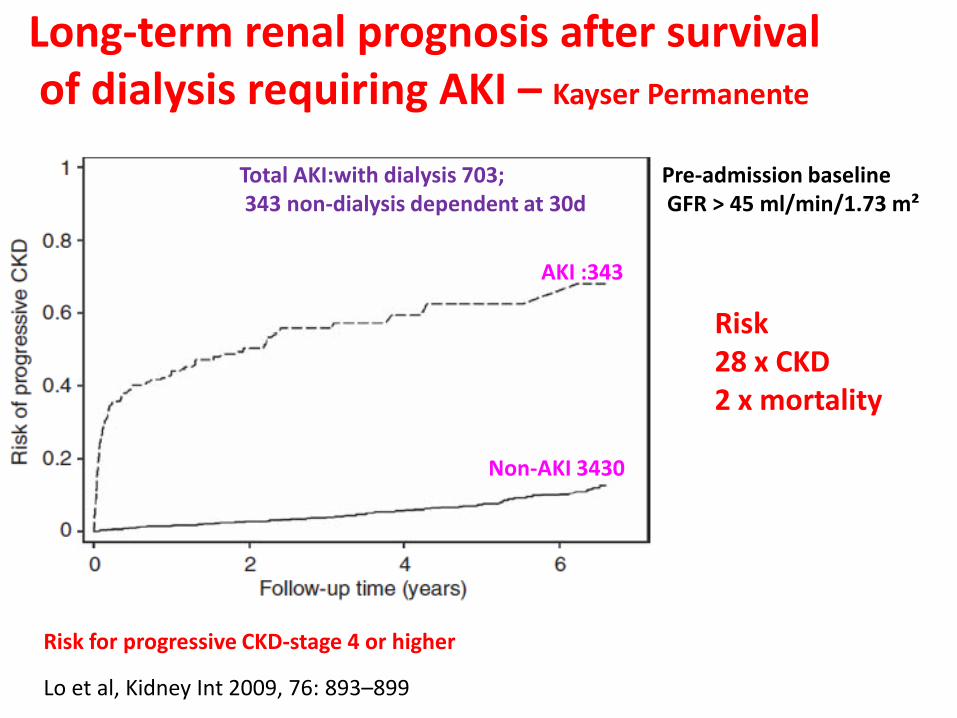
Lo et al, Kidney Int 2009, 76: 893–899
AKI :343
Non-AKI 3430
Long-term renal prognosis after survival of dialysis requiring AKI – Kayser Permanente
Total AKI:with dialysis 703; 343 non-dialysis dependent at 30d
Risk for progressive CKD-stage 4 or higher
Risk 28 x CKD 2 x mortality
Pre-admission baseline GFR > 45 ml/min/1.73 m²

CKD
ESRD
Coca et al, Kidney Int (2012) 81, 442–448
CKD after AKI-a systematic review and meta-analysis

Risk of chronic dialysis, all-cause mortality and rehospitalization among hospitalized patients with AKI
versus hospitalized patients with no AKI
Wald et al, Am J Med, 2012, 125, 585-593

Albuminuria and eGFR Independently Associate with Acute Kidney Injury
Grams et al, J Am Soc Nephrol, 21: 1757-1764, 2010

AKI AKD CKD
Conceptual Model For AKI, AKD and CKD








