
WELCOME TO THE CALIFORNIA CHAPTER
EDUCATION PROGRAM
IPPS FY2017 UPDATE
September 28th, 2016

Speaker
• Gloryanne Bryant, RHIA, CDIP, CCS, CCDS
• AHIMA Approved ICD-10-CM/PCS Trainer
• Nationally recognized HIM Coding professional, leader and
advocate
• Past-President of CHIA
• Former ACIDS Board Member
• California ACDIS Leadership Team
• Currently: National Director Coding Quality, Education, Systems and Support
• National Revenue Cycle for an Integrated Healthcare System
Goals/Objectives
• Review of top MS-DRG changes
• Learn key aspects of POA, HAC and Discharge
disposition under IPPS
• Enhance understanding of IPPS MS-DRG LOS
& Relative Weight Changes
• Discuss steps and action to enhance MS-DRG
accuracy and compliance with FY 2017
requirements
• Question and Answer Period
Disclaimer
• This material is designed and provided to communicate information about IPPS FY2017 in an educational format and manner. The presenter is not providing or offering legal advice, but rather practical and useful information and tools to achieve compliant results in the area of coding, clinical documentation, and data quality.
• Every reasonable effort has been taken to ensure that the educational information provided is accurate and useful.
• This presentation is an accumulation of the IPPS information and does not include ALL aspects and details thus attendee’s should review the final rule in addition.
• Participants are cautioned that information contained in this presentation is not a substitute for informed coding professional judgment.
NOTE: the program content, views, and opinions of the
speaker are not those of ACDIS or Kaiser Permanente.

Inpatient Prospective Payment
System (IPPS)
• Generally, Medicare IPPS payment is on a per discharge or per case basis for Medicare patients with inpatient stays.
• The claim for the patient’s inpatient stay must include all outpatient diagnostic services and admission-related outpatient nondiagnostic services provided by the admitting hospital or an entity that is wholly owned or operated by the admitting hospital on the date of a patient’s inpatient admission or within 3 days immediately preceding the date of a patient’s inpatient admission.
– In addition, you must not separately bill these services to Medicare Part B.
• Discharges are assigned to diagnosis-related groups (DRGs), a classification system that groups similar clinical conditions (diagnoses) and the procedures furnished by the hospital during the stay. The patient’s principal diagnosis and up to 24 secondary diagnoses that may include comorbidities or complications will determine the DRG assignment. Similarly, DRG assignment can be affected by up to 25 procedures furnished during the stay.
• Other factors that may influence DRG assignment include a patient’s gender, age, or discharge status disposition.
Inpatient Prospective Payment
System (IPPS)
• MS-DRG Changes
• Discharge Disposition
• Documentation and Coding adjustment
• Changes for the inpatient quality reporting
program
• Key updates on P4P programs: VBP,
readmissions, and HAC
6
Published in the Federal Register on August 22, 2016.

IPPS FY2017
7
MS-DRG FY2017
• The ICD-10 Medicare Severity Diagnosis Related Groups (MS-DRGs) Grouper software v34.0 classifies hospital case types into groups expected to have similar hospital resource use.
• Medicare uses this classification to pay for inpatient hospital care. Hospitals are paid a fixed price by Diagnosis Related Group (DRG) for treating Medicare patients.
• The groupings are based on diagnoses, procedures, other demographic information, and the presence of complications or co-morbidities, gender, and discharge disposition.
NOTE: Check with your IT and Grouper Vendor (Coding/DRG Software)
on installing the updates.
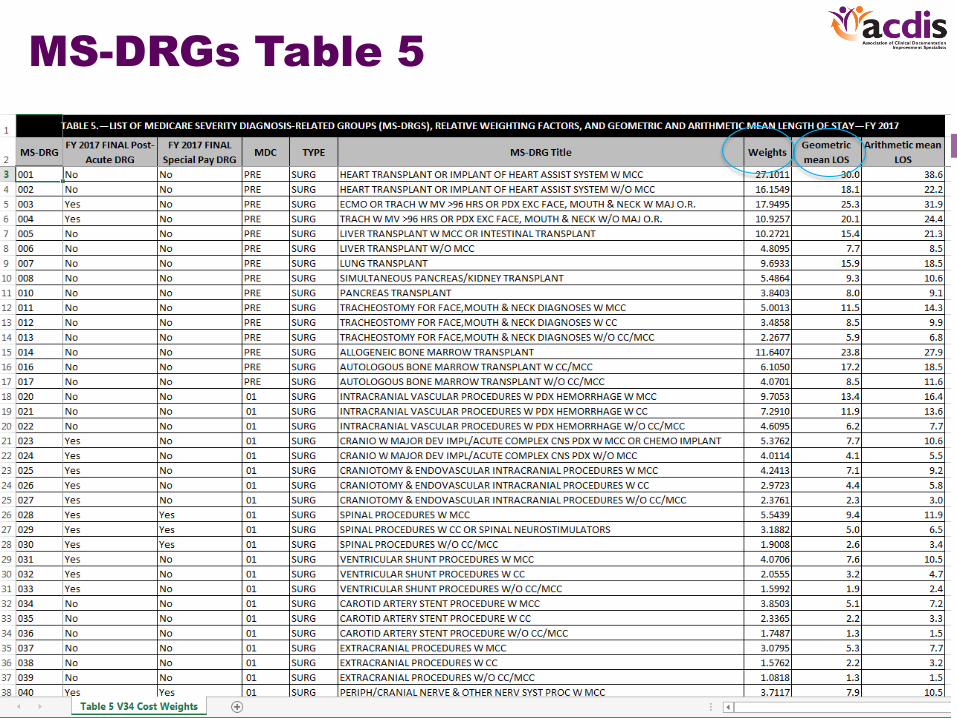
MS-DRGs Table 5
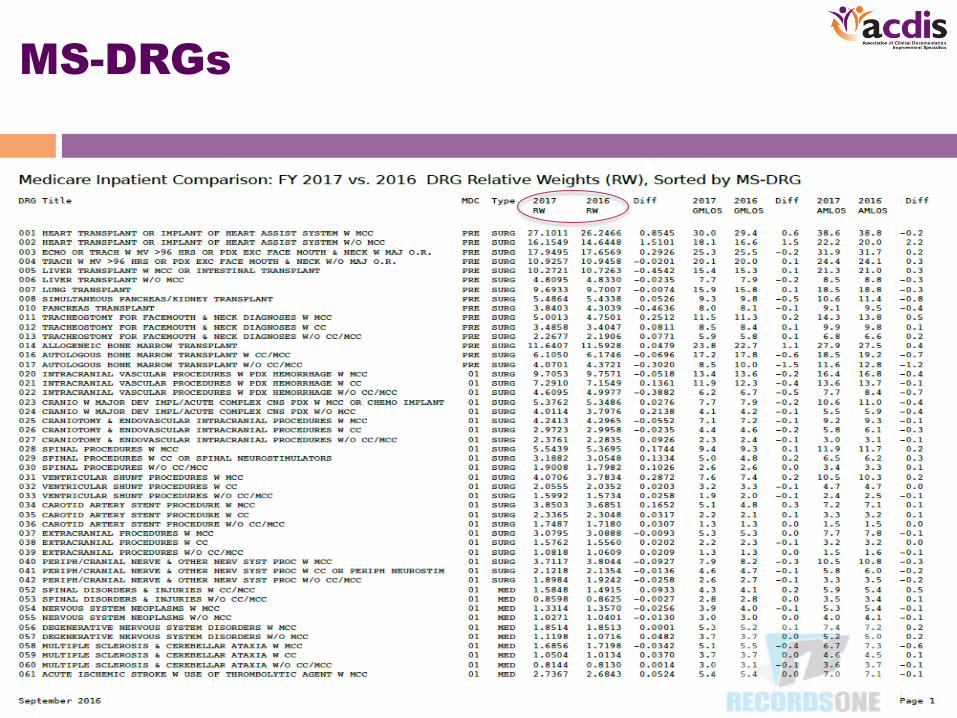
MS-DRGs
MS-DRG Changes
• The title for MS–DRG 884 in FY 2017 ICD–10 MS–DRGs Version 34 is
“MS–DRG 884 (Organic Disturbances and Intellectual Disability),”
effective October 1, 2016 changing the word “mental retardation”.
• Reassign ICD–10–CM diagnosis codes T85.610A, T85.620A,
T85.630A, and T85.690A from MDC 21 under MS–DRGs 919, 920,
and 921 to MDC 1 under MS–DRGs 091, 092, and 093. The official
code titles for these four codes were revised after publication of the
proposed rule. Effective October 1, 2016, the revised code titles are as
follows (and are reflected in Table 6E).
– T85.610A (Breakdown (mechanical) of cranial or spinal infusion catheter, initial
encounter);
– T85.620A (Displacement of cranial or spinal infusion catheter, initial encounter);
– T85.630A (Leakage of cranial or spinal infusion catheter, initial encounter); and
– T85.690A (Other mechanical complication of cranial or spinal infusion catheter, initial
encounter)

MS-DRG Changes (cont.)
• No change in assignments for endovascular
embolization or occlusion of head and neck procedures
and other endovascular procedures in MS–DRGs 020
through 027.
• Assign ICD–10–PCS procedure codes 02RK0JZ
(Replacement of right ventricle with synthetic substitute,
open approach) and 02RL0JZ (Replacement of left
ventricle with synthetic substitute, open approach) as a
code cluster to MS–DRGs 001 and 002 (Heart
Transplant or Implant of Heart Assist System with and
without MCC, respectively) effective October 1, 2016 for
ICD–10 MS–DRGs Version 34.

MS-DRG changes (cont.)
• Reassigning 18 ICD–10–CM diagnosis codes from MDC 21
(Injuries, Poisonings and Toxic Effects of Drugs)under MS–DRGs 919,
920, and 921(Complications of Treatment with MCC, with CC, and
without CC/MCC, respectively) to MDC 1 (Diseases and Disorders of
the Nervous System) under MS–DRGs 091, 092, and 093 (Other
Disorders of the Nervous System with MCC, with CC, and without
CC/MCC, respectively) effective October 1, 2016.
• MS-DRGs 919-921 (Mechanical Complications): Mechanical
complications of the nervous system including devices, implants,
grafts, implanted electronic neurostimulator of the brain will be moved
from MS-DRGs 919 – 921 to MS-DRG 91 – 93 (Other Disorders of the
Nervous System).
• Reassigned ICD–10–CM diagnosis code R22.2 Localized Swelling,
Mass and Lump, Trunk) from MDC 4 to MDC 9 under MS–DRGs 606
and 607 (Minor Skin Disorders with and without MCC, respectively).

MS-DRGs Changes (Cardiac
Focus)
• MDC 5 (Diseases and Disorders of the Circulatory System)
• Implantable Loop Recorder
– CMS finalized its proposal to include 4 of the 6 requested ICD-10 procedure codes related to ILRs as OR procedures, which will result in these procedures mapping to higher paying MS-DRGs
• Pacemaker Implants, Replacements and Revisions
– CMS finalized its proposals to eliminate the code combinations, and instead provide lists of codes for each category (i.e. Implant, Revision, Replacement) – if the appropriate codes appear on the claim from these lists, they will map to MS-DRGs 242-244
• MitraClip System Implants
– CMS finalized its proposal to map MitraClip procedures to MS-DRGs 228, 229
• MS-DRGs 228-230 Other Cardiothoracic Procedures: CMS finalized its proposal to move transcatheter mitral valve repair (i.e. the MitraClip® System) from current MS-DRG 273-274 to MS-DRG 228 and 229.
– MS-DRG 230 has been eliminated based on claims data and the rules governing splitting MS-DRGs. These cases will be included with MS-DRG 229 C
– Current MS-DRG 228 description will be Other Cardiothoracic Procedures with MCC and MS-DRG 229 without MCC or CC.
• AICD Procedures
– CMS is finalizing its proposal for no changes to MS-DRG 245 based on their analysis
– Implantable Medical Device Credits
• CMS policy states that if a hospital received a credit for a recalled device equal to 50 percent or more of the cost of the device, CMS would reduce a hospital’s IPPS payment for those MS-DRGs
• No changes were made to this policy for FY 2017 – this policy impacts 48 MS-DRGs
• Implantable Medical Device Credits
– CMS policy states that if a hospital received a credit for a recalled device equal to 50 percent or more of the cost of the device, CMS would reduce a hospital's IPPS payment for those MS-DRGs
– No changes were made to this policy for FY 2017 – this policy impacts 48 MS-DRGs

MS-DRG Changes (cont.)
• Collapse MS–DRGs 228, 229, and 230 from three severity levels to
two severity levels by deleting MS–DRG 230 and revising MS–DRG
229.
• Finalizing our proposal to reassign ICD–9–CM procedure code
35.97 and the cases reporting ICD–10–PCS procedure code
02UG3JZ (Supplement mitral valve with synthetic substitute,
percutaneous approach) from MS–DRGs 273 and 274 to MS–DRG
228 and revised MS–DRG 229. The title of revised MS–DRG 229 is
finalized as follows to reflect the ‘‘without MCC’’ designation, ‘‘Other
Cardiothoracic Procedures without MCC’’. The title for MS–DRG
228 is finalized as ‘‘MS–DRG 228 (Other Cardiothoracic Procedures
with MCC)’’.
MS-DRG Changes (cont.)
• Modify the MS–DRG logic for MS–DRGs 242, 243, and 244 to
establish that cases reporting one ICD–10–PCS code from the list
of procedure codes describing procedures involving pacemaker
devices and one ICD–10–PCS code from the list of procedure
codes describing procedures involving pacemaker leads in
combination with one another will qualify the case for assignment to
MS– DRGs 242, 243, and 244.
• Modify the MS–DRG logic for MS–DRGs 258 and 259 (Cardiac
Pacemaker Device Replacement with and without MCC,
respectively) to establish that a case reporting one ICD–10–PCS
procedure code describing procedures involving pacemaker device
insertions without any other procedure codes describing procedures
involving pacemaker leads reported is assigned to MS–DRGs 258
and 259 for FY 2017.
• Updated ICD-10-PCS code titles for these procedures.
MS-DRG Changes (cont.)
• MS–DRG 245 (AICD Generator Procedures) criteria
were not met to support the subdivision of MS–DRG
245 into severity levels for FY 2017.
– CMS will continue to monitor MS–DRG 245 claim
data as we analyze issues for the FY 2018
IPPS/LTCH PPS proposed rule.
• Reclassify the bypass of the portal vein to lower
vein with transluminal device, percutaneous
approach (06183DY) from 270 – 272 (Other Major
• Cardiothoracic Procedures) to MSDRGs 405 – 407.
– Also known as TIPS procedure.

MS-DRGs (cont.)
• MS-DRG 270-272 Endovascular Thrombectomy of the Lower Limbs: CMS finalized assignment of procedures describing endovascular thrombectomy of the lower limbs be assigned to MS-DRGs 270, 271 and 272 .
– (long list of ICD-10-PCS codes . . .)
– 04CK3ZZ .......... Extirpation of matter from right femoral artery, percutaneous approach.
– 04CL3ZZ ........... Extirpation of matter from left femoral artery, percutaneous approach.
– 04CM3ZZ .......... Extirpation of matter from right popliteal artery, percutaneous approach.
– 04CN3ZZ .......... Extirpation of matter from left popliteal artery, percutaneous approach.
– 04CP3ZZ .......... Extirpation of matter from right anterior tibial artery, percutaneous approach.
– 04CQ3ZZ .......... Extirpation of matter from left anterior tibial artery, percutaneous approach.
– 04CR3ZZ .......... Extirpation of matter from right posterior tibial artery, percutaneous approach.
– 04CS3ZZ .......... Extirpation of matter from left posterior tibial artery, percutaneous approach.
– 04CV3ZZ .......... Extirpation of matter from right foot artery, percutaneous approach.
– 04CW3ZZ ......... Extirpation of matter from left foot artery, percutaneous approach.
– 04CY3ZZ .......... Extirpation of matter from lower artery, percutaneous approach.
– 06CM3ZZ .......... Extirpation of matter from right femoral vein, percutaneous approach.

MS-DRG Changes (cont.)
• MS-DRGs 268 and 269 (Aortic and Heart
Assist Procedures Except Pulsation Balloon)
• Move procedure codes 06CV3ZZ and 06CY3ZZ
from DRGs 268 and 269 to 270, 271, and 272
(Other Major Cardiovascular Procedures)
–Adjustment to Relative Weights
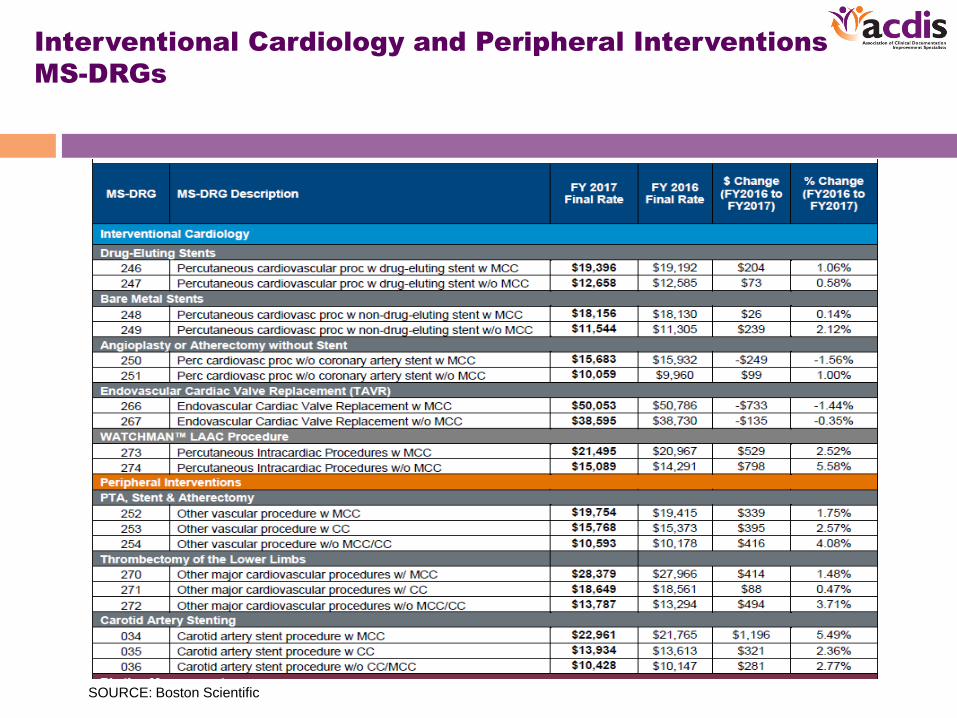
Interventional Cardiology and Peripheral Interventions
MS-DRGs
SOURCE: Boston Scientific

Rhythm Management MS-DRGs
MS-DRG Changes (cont.)
• MS-DRGs 456 - 458 (Spinal Fusion Except
Cervical)
• These diagnoses will be removed from the
secondary diagnosis list from MS-DRGs 456 –
458.
– M40.50 (Lordosis, unspecified, unspecified site)
– M40.55 (Lordosis, unspecified, thoracolumbar)
– M40.56 (Lordosis, unspecified, lumbar)
– M40.57 (Lordosis, unspecified, lumbosacral)
MS-DRG Changes (cont.)
• Designate the following four ICD–10–PCS
codes as O.R. procedures Version 34 ICD–10
MS–DRG Definitions Manual:– 0JH602Z (Insertion of monitoring device into chest subcutaneous
tissue and fascia, open approach);
– 0JH632Z (Insertion of monitoring device into chest subcutaneous
tissue and fascia, percutaneous approach);
– 0JWT02Z (Revision of monitoring device in trunk subcutaneous
tissue and fascia, open approach); and
– 0JWT32Z (Revision of monitoring device in trunk subcutaneous
tissue and fascia, percutaneous approach).

MS-DRG Changes (cont.)
• MDC 6 (Diseases and Disorders of the Digestive
System): Excision of Ileum
• Reassign ICD–10–PCS procedure codes 0DBB0ZZ
(Excision of ileum, open approach) and 0DBA0ZZ
(Excision of jejunum, open approach) from MS–DRGs
347, 348, and 349 (Anal and Stomal Procedures with
MCC, with CC, and without CC/MCC, respectively) to
MS–DRGs 329, 330, and 331 (Major Small and Large
Bowel Procedures with MCC, with CC, and without
CC/MCC, respectively) effective with the ICD–10 MS–
DRGs Version 34 on October 1, 2016.

MS-DRG Changes (cont.)
• MDC 7 (Diseases and Disorders of the Hepatobiliary
System and Pancreas): Bypass Procedures of the Veins
• Assign ICD–10–PCS code 06183DY (Bypass portal vein
to lower vein with intraluminal device, percutaneous
approach) to MDC 7 (Diseases and Disorders of the
Hepatobiliary System and Pancreas) under MS–DRGs
405, 406, and 407 (Pancreas Liver and Shunt
Procedures with MCC, with CC, and without CC/ MCC,
respectively).
MS-DRG Changes (cont.)
• MDC 8 (Diseases and Disorders of the Musculoskeletal System and
Connective Tissue).
• Total Ankle Replacement (TAR) Procedures: Maintain the current MS–
DRG assignment for total ankle replacements in MS–DRGs 469 and 470
and not create a new MS–DRG for total ankle replacements.
• Hip Replacement Procedures With Principal Diagnosis of Hip Fracture:
maintain the MS–DRG assignment for hip replacements with a principal
diagnosis of hip fractures in MS– DRGs 469 and 470 and not create a
new MS–DRG for hip replacements with a principal diagnosis of hip
fractures.
– Removal of spacer and replacement of joint procedures added to the
methodology.
• Add 58 new codes for the removal and replacement of knee joint
combinations that capture the joint revisions to the Version 34 MS DRG
structure for MS– DRGs 466, 467, and 468, effective October 1, 2016.

MS-DRGs with no changes
• MS-DRGs 515 – 517 (Other Musculoskeletal
System Procedures)
• – Decompressive Laminectomies will not
change
• MS-DRGs 945 – 946 (Rehabilitation)
• – Logic will not change

Documentation & Coding
• “This also reflects a 1.5 percentage point
reduction for documentation and coding
required by the American Taxpayer Relief Act of
2012 (section 631) and an increase of
approximately 0.8 percentage points to remove
the adjustment to offset the estimated costs of
the two-midnight policy and address its effects
in FYs 2014, 2015, and 2016,” said CMS.
CC List
• A92.5 Zika Virus
• C49.A- Gastrointestinalstromal tumor (Multiple)Allvariants of postprocedural hematoma
• H34.81- Central retinal vein occlusion
• K04.0- Pulpitis
• K59.3- Megacolon
• K90.4- Malabsorption due to intolerance
• L03.213 Periorbital cellulitis
• M50.02- Cervical disc disorders of mid-cervical region with myelopathy
• M84.75- Atypical femoral fractures*
• M97- Periprosthetic fractures**
• N13.0 Hydronephrosis with UPJ obstruction
• N83.5- Torsion of ovary, ovarian pedicle and fallopian tube
*Except sequela (S), or subsequent encounters with routine healing (D) or delayed healing (G)
**Except sequela (S), or subsequent encounters with routine healing (D)
CC List (cont.)
• O.00- Ectopic pregnancy
• O44.2- Partial placenta previa without hemorrhage
• O44.4- Low lying placenta NOS without hemorrhage
• Q25.2- Atresia of aorta
• Q25.4- Other congenital malformations of the aorta
• S02.1- Closed skull and facial bone fractures*
• S02.3- Open and closed orbital floor fractures*
• S02.4- Open and closed fractures of malar, maxillary, and zygoma*
• S02.6- Open and closed fractures of mandible*
• S02.8- Open and closed fractures of other specified skull and facial bones*
• S92.81- Open and closed fractures of feet*
*Except sequela (S), or subsequent encounters with routine healing (D) or
delayed healing (G)
CC List (cont.)
• T82.855A Stenosis of coronary artery stent, initial encounter*
• T82.856A Stenosis of peripheral vascular stent, initial encounter*
• T83.113A Breakdown (mechanical) of other urinary stents, initial encounter
• T83.123A Displacement of other urinary stents, initial encounter
• T83.193A Other mechanical complication of other urinary stent, initial encounter
• T83.24XA Erosion of graft of urinary organ, initial encounter
• T83.25XA Exposure of graft of urinary organ, initial encounter
• T83.51- Infection and inflammatory reaction due to indwelling urinary catheter*
• T83.59- Infection and inflammatory reaction due to prosthetic device, implant and graft in the urinary system*
• T83.6- Infection and inflammatory reaction due to prosthetic device, implant and graft in the genital tract*
• T83.71- Erosion of implanted mesh and other prosthetic materials to surrounding organ or tissue
• T83.72- Exposure of implanted mesh and other prosthetic materials to surrounding organ or tissue
*Except sequela (S), or subsequent encounters (D)

CC List (cont.)
• T83.79- Other specified complications due to other prosthetic materials*
• T85.113A Breakdown (mechanical) of implanted electronic neurostimulator, generator, initial encounter
• T85.123A Displacement of implanted electronic neurostimulator, generator, initial encounter
• T85.193A Other mechanical complication of implanted electronic neurostimulator, generator, initial encounter
• T85.615A Breakdown (mechanical) of other nervous system device, implant or graft, initial encounter
• T85.625A Displacement of other nervous system device, implant or graft, initial encounter
• T85.635A Leakage of other nervous system device, implant or graft, initial encounter
• T85.695A Other mechanical complication of other nervous system device, implant or graft, initial encounter
• T85.73- Infection and inflammatory reaction due to implanted nervous system device (e.g. shunt, neurostimulator)*
• T85.81- Embolism due to nervous system prosthetic devices, implants and grafts**
• T85.82- Fibrosis due to nervous system prosthetic devices, implants and grafts**
• T85.83- Hemorrhage due to nervous system prosthetic devices, implants and grafts**
*Except sequela (S), or subsequent encounters (D)
**Except sequela (S)
CC List (cont.)
• T85.84- Pain due to nervous system prosthetic devices, implants and grafts**
• T85.85- Stenosis due to nervous system prosthetic devices, implants and grafts**
• T85.86- Thrombosis due to nervous system prosthetic devices, implants and grafts**
• T85.89- Other specified complication of nervous system prosthetic devices, implants and grafts**
*Except sequela (S), or subsequent encounters (D)
**Except sequela (S)
MCC List
• I60.2 Non-traumatic subarachnoid hemorrhage from anterior communicating artery
• I63._ _3 Cerebral infarctions involving bilateral cerebral or precerebral arteries
• I77.70 Dissection of unspecified artery
• I77.75 Dissection of other precerebral arteries
• I77.76 Dissection of artery of upper extremity
• I77.77 Dissection of artery of lower extremity
• J95.81 Mediastinitis
• J95.89 Other diseases of mediastinum, not elsewhere classified
• K55.0- Acute vascular disorders of intestine
• K55.30 Necrotizing enterocolitis, unspecified
• K55.31 Stage 1 necrotizing enterocolitis
• K55.32 Stage 2 necrotizing enterocolitis
• K55.33 Stage 3 necrotizing enterocolitis

MCC List (cont.)
• K85._0 Acute pancreatitis without necrosis or infection
• K85._1 Acute pancreatitis with uninfected necrosis
• K85._2 Acute pancreatitis with infected necrosis
• O44.3- Partial placenta previa with hemorrhage
• O44.5- Low lying placenta NOS with hemorrhage
• S02.10_B Fracture of base of skull, Initial encounter for open fracture
• S02.11_B Occipital condyle fractures, Initial encounter for open fracture

ICD-10-PCS
• There are 49 ICD-10-PCS code additions
pertaining to insertion and infusion devices,
which are shown in table 6P.3c and
available on CMS’s website at:
• https://www.cms.gov/Medicare/Medicare-Fee-for- Service-
Payment/AcuteInpatientPPS/Downloads/ FY2017-CMS-1655-FR-
Table-6.zip

New Technology Add-on Payment
• Technology criteria for newness, high cost threshold, and
substantial clinical improvement.
– Add-on payment is provided
• CMS evaluated seven new technologies for FY2017, four of
which are for medical device technologies and three for drugs.
• Blinatumomab (BLINCYTO) used to treat Acute Lymphoblastic
Leukemia (est. $27,017.85)
– ICD-10-PCS codes: XW03351, XW04351
• Awarded new technology status to: Defitelio ® (est. $75,900),
VISTOGARD™ (est. $37,500), Praxbind®, GORE®
EXCLUDER® Iliac Branch Endoprosthesis, and MAGEC®
Spinal Bracing and Distraction System (est. $15,750)
New Technology Add-on Payment
(cont.)
• In the cardiovascular area:
• GORE® EXCLUDER® Iliac Branch
Endoprosthesis (IBE) – est. $5,250
– a device that consists of both the Iliac Branch
Component (IBC) and the Internal Iliac Component
(IIC) and each endoprosthesis is pre-mounted on a
customized delivery and deployment system
allowing for controlled endovascular delivery via
bilateral femoral access for the treatment of patients
requiring repair of common iliac or aortoiliac
aneurysms was approved for NTAP status.
New Technology Add-On Payment
(cont.)
39
https://www.goremedical.com/products/excludereu---ibe?locale=mpd_euro
New Technology Add-on Payment
(cont.)
• CMS will continue new technology add-on payments (NTAP) in FY2017 for:
– CardioMEMS™ HF (Heart Failure) Monitoring System
– LUTONIX® Drug-Coated Balloon (DCB) Percutaneous Transluminal Angioplasty (PTA) Catheter (Approx. $1,035.72)
– IN.PACT™ Admiral™ Paclitaxel Coated Percutaneous Transluminal Angioplasty (PTA) Balloon Catheter.
• CMS will discontinue new technology add-on payments in FY 2017 for MitraClip® System.
– MitraClip (02UG3JZ) will be reassigned from 273/274 to 228/229

New Technology Add-on Payments
(cont.)
• All NTAP procedures will be assigned a
Section “X” code (New Technology) within the
structure of the ICD-10-PCS.
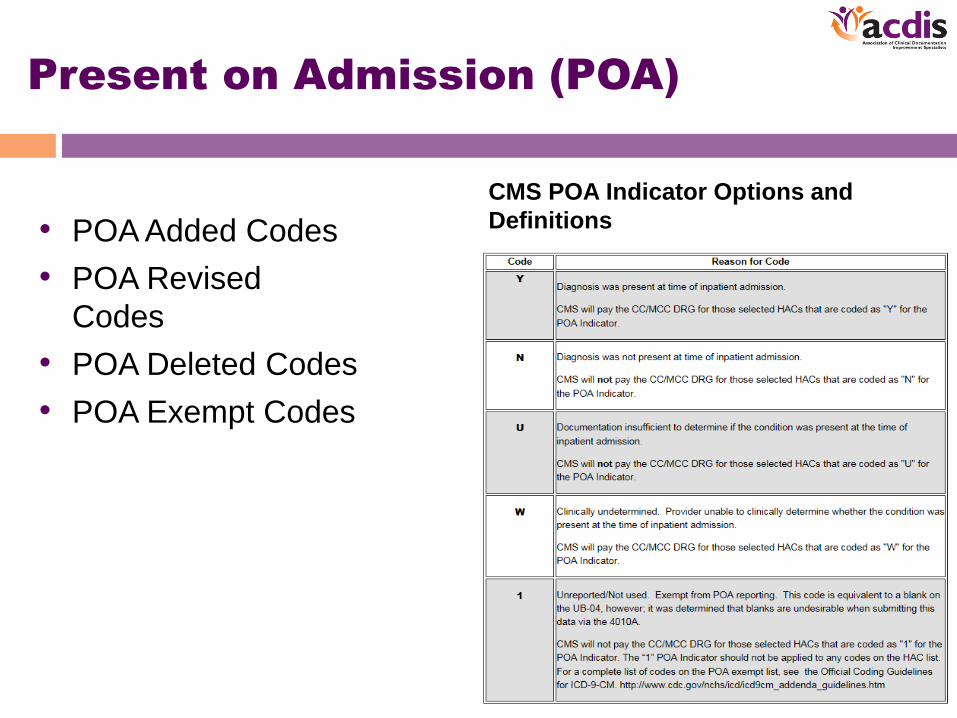
Present on Admission (POA)
• POA Added Codes
• POA Revised
Codes
• POA Deleted Codes
• POA Exempt Codes
CMS POA Indicator Options and
Definitions
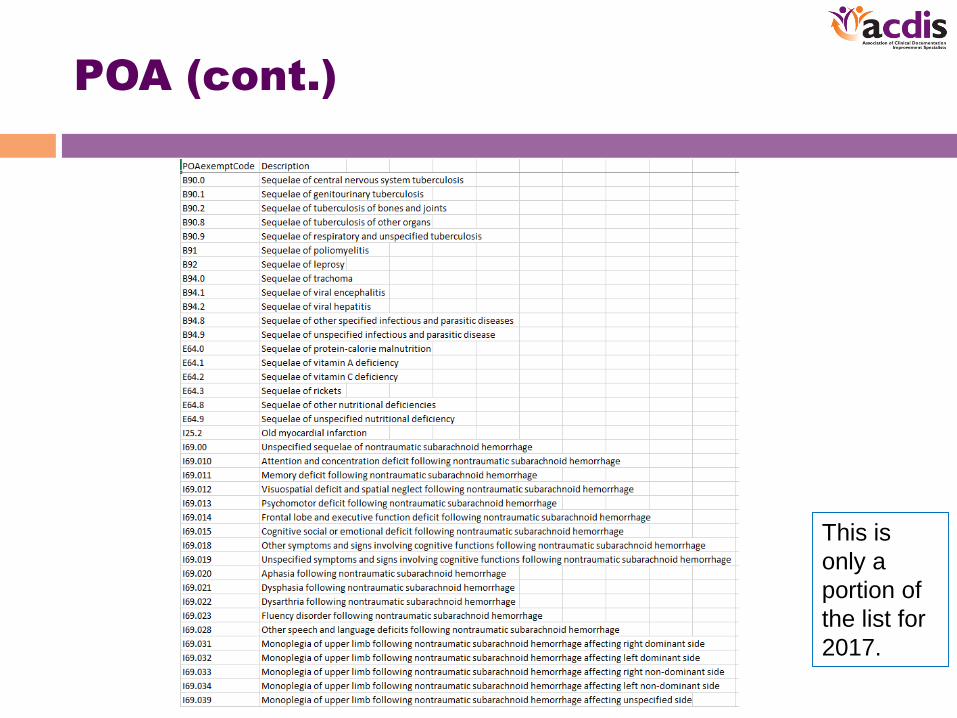
POA (cont.)
This is
only a
portion of
the list for
2017.
IPPS FY2017: HAC
• Hospitals in the lowest performing quartile for HACs are
penalized 1% of their total Medicare MS-DRG payments. In
2016, 75% of the performance in HACs will be in the abstracted
measure domain, and central line-associated bloodstream
infections (CLABSI), catheter-associated urinary tract infections
(CAUTI), and SSIs will be targeted.
• Thus far, the results have been:
– Approximately 1.3 million fewer patients were harmed in U.S.
hospitals between 2010-2013, which is a 17% decline in
HACs.
– Approximately 50,000 fewer patients died in the hospital as a
result of this reduction in HACs.
– Approximately $12 billion in healthcare costs was saved from
2010-2013 due to this reduction.44

HAC (cont.)
• HAC 01 – Foreign Object Retained After Surgery ICD-10-CM diagnosis code list
• HAC 02 – Air Embolism ICD-10-CM diagnosis code list
• HAC 03 – Blood Incompatibility ICD-10-CM diagnosis code list
• HAC 04 – Stage III and IV Pressure Ulcers ICD-10-CM diagnosis code list
• HAC 05 – Falls and Trauma ICD-10-CM diagnosis code list
• HAC 06 – Catheter-Associated Urinary Tract Infection (UTI) ICD-10-CM diagnosis code list
• HAC 07 – Vascular Catheter-Associated Infection ICD-10-CM diagnosis code list
• HAC 08 - Surgical Site Infection (SSI)-Mediastinitis Following Coronary Artery Bypass Graft (CABG) ICD-10-CM
diagnosis and ICD-10-PCS procedure code lists
• HAC 09 – Manifestations of Poor Glycemic Control ICD-10-CM diagnosis code list
• HAC 10 – Deep Vein Thrombosis (DVT)/Pulmonary Embolism (PE) with Total Knee or Hip Replacement ICD-10-
CM diagnosis and ICD-10-PCS procedure code lists
• HAC 11 – Surgical Site Infection (SSI) Following Bariatric Surgery ICD-10-CM diagnosis and ICD-10-PCS
procedure code lists
• HAC 12 – Surgical Site Infection (SSI) Following Certain Orthopedic Procedures of Spine, Shoulder or Elbow
ICD-10-CM diagnosis and ICD-10-PCS procedure code lists
• HAC 13 - Surgical Site Infection (SSI) Following Cardiac Implantable Electronic Device (CIED) Procedures ICD-
10-CM diagnosis and ICD-10-PCS procedure code lists
• HAC 14 – *Iatrogenic Pneumothorax with Venous Catheterization ICD-10-CM diagnosis and ICD-10-PCS
procedure code lists

HAC (cont.)
IPPS FY2017 Discharge
Disposition – No Changes
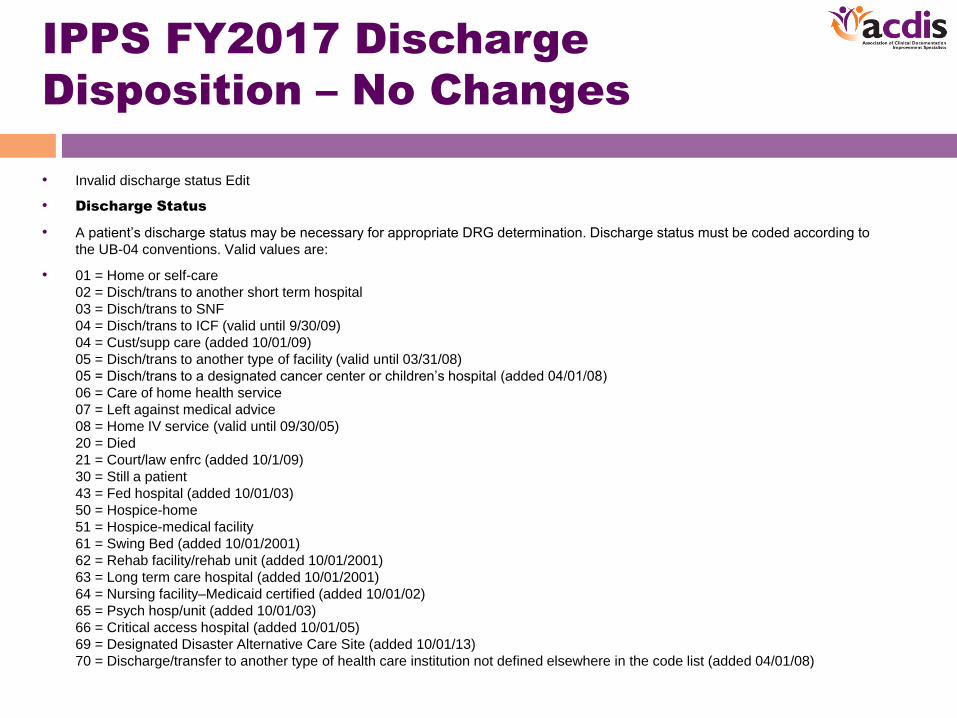
• Invalid discharge status Edit
• Discharge Status
• A patient’s discharge status may be necessary for appropriate DRG determination. Discharge status must be coded according to
the UB-04 conventions. Valid values are:
• 01 = Home or self-care
02 = Disch/trans to another short term hospital
03 = Disch/trans to SNF
04 = Disch/trans to ICF (valid until 9/30/09)
04 = Cust/supp care (added 10/01/09)
05 = Disch/trans to another type of facility (valid until 03/31/08)
05 = Disch/trans to a designated cancer center or children’s hospital (added 04/01/08)
06 = Care of home health service
07 = Left against medical advice
08 = Home IV service (valid until 09/30/05)
20 = Died
21 = Court/law enfrc (added 10/1/09)
30 = Still a patient
43 = Fed hospital (added 10/01/03)
50 = Hospice-home
51 = Hospice-medical facility
61 = Swing Bed (added 10/01/2001)
62 = Rehab facility/rehab unit (added 10/01/2001)
63 = Long term care hospital (added 10/01/2001)
64 = Nursing facility–Medicaid certified (added 10/01/02)
65 = Psych hosp/unit (added 10/01/03)
66 = Critical access hospital (added 10/01/05)
69 = Designated Disaster Alternative Care Site (added 10/01/13)
70 = Discharge/transfer to another type of health care institution not defined elsewhere in the code list (added 04/01/08)

Discharge Status (cont.)
• 65 = Psych hosp/unit (added 10/01/03)66 = Critical access hospital (added 10/01/05)69 = Designated Disaster Alternative Care Site (added 10/01/13)70 = Discharge/transfer to another type of health care institution not defined elsewhere in the code list (added 04/01/08)71 = Outpatient services-other facility (10/01/01–09/30/03 only)72 = Outpatient services-this facility (10/01/01–09/30/03 only)81 = Home-Self care w Planned Readmission (added 10/01/13)82 = Short Term Hospital w Planned Readmission (added 10/01/13)83 = SNF w Planned Readmission (added 10/01/13)84 = Cust/supp care w Planned Readmission (added 10/01/13)85 = Canc/child hosp w Planned Readmission (added 10/01/13)86 = Home Health Service w Planned Readmission (added 10/01/13)87 = Court/law enfrc w Planned Readmission (added 10/01/13)88 = Federal Hospital w Planned Readmission (added 10/01/13)89 = Swing Bed w Planned Readmission (added 10/01/13)90 = Rehab Facility/ Unit w Planned Readmission (added 10/01/13)91 = LTCH w Planned Readmission (added 10/01/13)92 = Nursg Fac-Medicaid Cert w Planned Readmiss (added 10/01/13)93 = Psych Hosp/Unit w Planned Readmission (added 10/01/13)94 = Crit Acc Hosp w Planned Readmission (added 10/01/13)95 = Oth Institution w Planned Readmission (added 10/01/13)

Post Acute Care Transfer
(PACT)
• CMS evaluates whether the postacute care transfer
policy applies to that assignment using the following
criteria:
– Whether the MS-DRG’s total number of discharges to
postacute care equals or exceeds the 55th percentile
for all MS-DRGs; and
– Whether the proportion of (i) short-stay discharges to
postacute care to (ii) total discharges in the MS-DRG
exceeds the 55th percentile for all MS-DRGs.
• If the MS-DRG satisfies both criteria, CMS applies the
postacute care transfer policy to that MS-DRG as well
as to any other MS-DRG that shares the same base
MS-DRG.

PACT cont.
• The discharge status code is assigned by the hospital based on the
expected treatment, if any, planned after the patient leaves the care
of the hospital. The proper discharge status code is determined
after consultation with the patient and the patient’s family, their
physician and hospital personnel. It can indicate, among other
scenarios, that a patient will be discharged to:
– • Home
– • A nursing home
– • Home health care
– • A rehabilitation facility
– • A psychiatric facility, or
– • Another acute care hospital
• Only certain discharge status codes are impacted by the Transfer
Rule.
PACT cont.
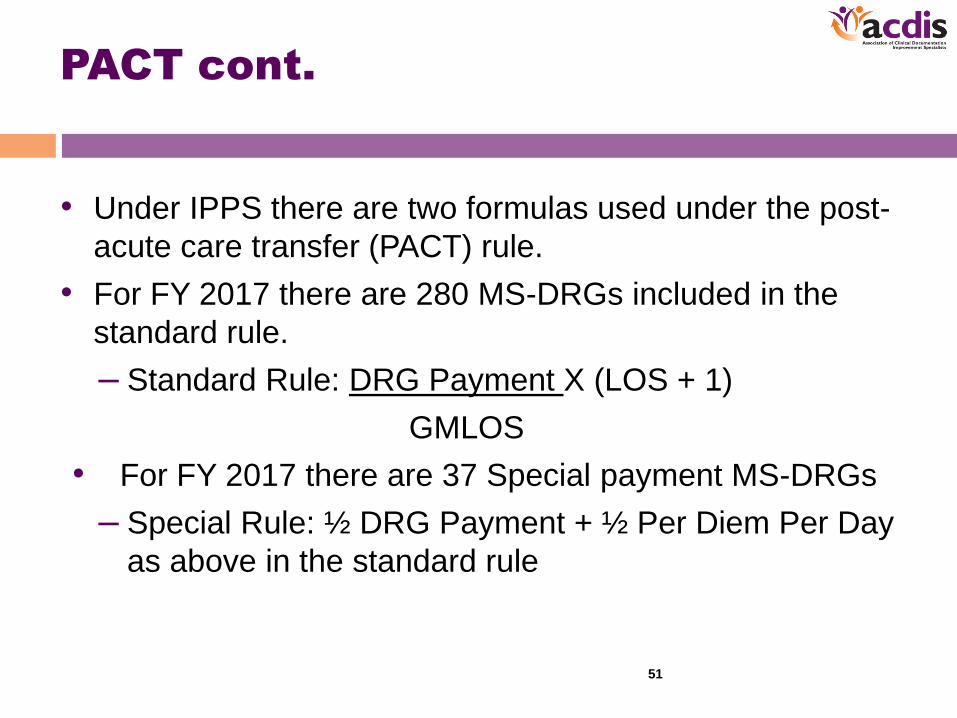
• Under IPPS there are two formulas used under the post-
acute care transfer (PACT) rule.
• For FY 2017 there are 280 MS-DRGs included in the
standard rule.
– Standard Rule: DRG Payment X (LOS + 1)
GMLOS
• For FY 2017 there are 37 Special payment MS-DRGs
– Special Rule: ½ DRG Payment + ½ Per Diem Per Day
as above in the standard rule
51
Medicare Code Editor
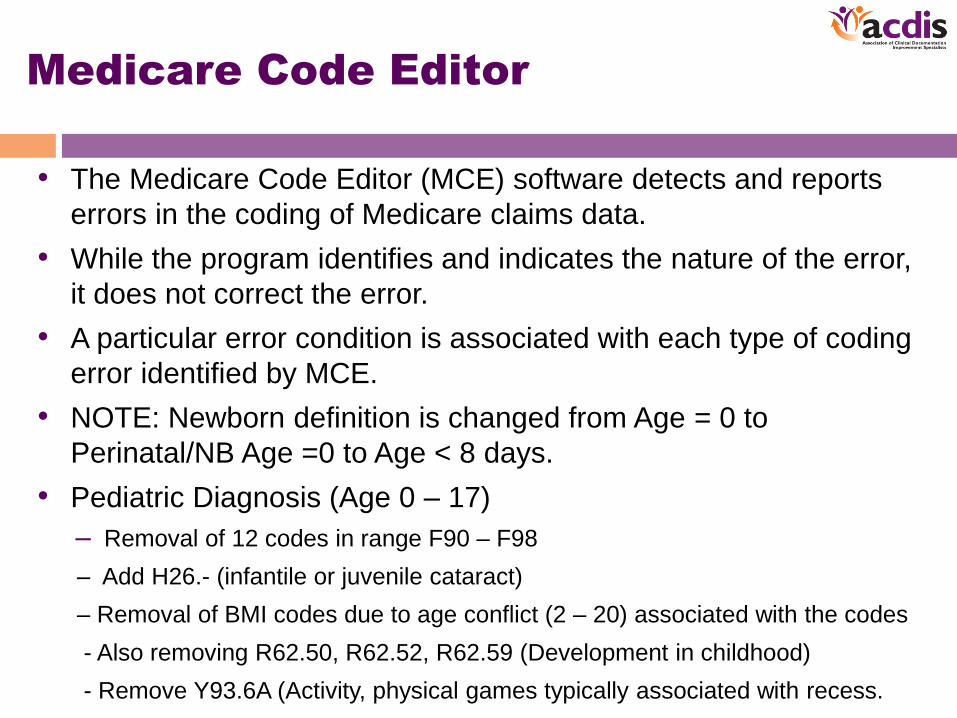
• The Medicare Code Editor (MCE) software detects and reports
errors in the coding of Medicare claims data.
• While the program identifies and indicates the nature of the error,
it does not correct the error.
• A particular error condition is associated with each type of coding
error identified by MCE.
• NOTE: Newborn definition is changed from Age = 0 to
Perinatal/NB Age =0 to Age < 8 days.
• Pediatric Diagnosis (Age 0 – 17)
– Removal of 12 codes in range F90 – F98
– Add H26.- (infantile or juvenile cataract)
– Removal of BMI codes due to age conflict (2 – 20) associated with the codes
- Also removing R62.50, R62.52, R62.59 (Development in childhood)
- Remove Y93.6A (Activity, physical games typically associated with recess.

MCE: Edit code lists
• Below is a list of edits:
• 1. Invalid diagnosis or procedure code
• 2. External causes of morbidity codes as principal diagnosis
• 3. Duplicate of PDX
• 4. Age conflict
• 5. Sex conflict
• 6. Manifestation code as principal diagnosis
• 7. Non-specific principal diagnosis (Discontinued as of 10/01/07)
• 8. Questionable admission
• 9. Unacceptable principal diagnosis
• 10. Non-specific O.R. procedure (Discontinued as of 10/01/07)
• 11. Non-covered procedure
• 12. Open biopsy check (Discontinued as of 10/01/10)
• 13. Bilateral procedure (Discontinued as of ICD-10 implementation)
• 14. Invalid age
• 15. Invalid sex
• 16. Invalid discharge status
• 17. Limited coverage
• 18. Wrong procedure performed
• 19. Procedure inconsistent with LOS
Questionable Admissions - removed
– T81.81XA (Complication of inhalation therapy)
– T88.4XXA (Failed or difficult intubation)
– T88.7XXA (Unspecified drug adverse effect)
– T88.8XXA (Other specified complications of medical care)
– T88.9XXA (Complication of medical/surgical care, unspecified)

MCE (cont.)
• Example – not all inclusive
• 1. Invalid diagnosis or procedure code
• The Medicare Code Editor checks each diagnosis including the admitting diagnosis and each procedure against a table of valid ICD codes. If an entered code does not agree with any code on the internal list, it is assumed to be invalid.
• For a list of all valid ICD-10-CM and ICD-10-PCS codes, see the International Classification of Diseases list.
• 2. External causes of morbidity codes as principal diagnosis
• External cause codes (V, W, X or Y codes (ICD-10-CM), E codes (ICD-9-CM)) describe the circumstance causing an injury, not the nature of the injury, and therefore should not be used as a principal diagnosis.
• For a list of all external causes of morbidity codes, see the International Classification of Diseases list.
• 3. Duplicate of PDX
• Whenever a secondary diagnosis is coded the same as the principal diagnosis, the secondary diagnosis is identified as a duplicate of the principal diagnosis.
Readmission
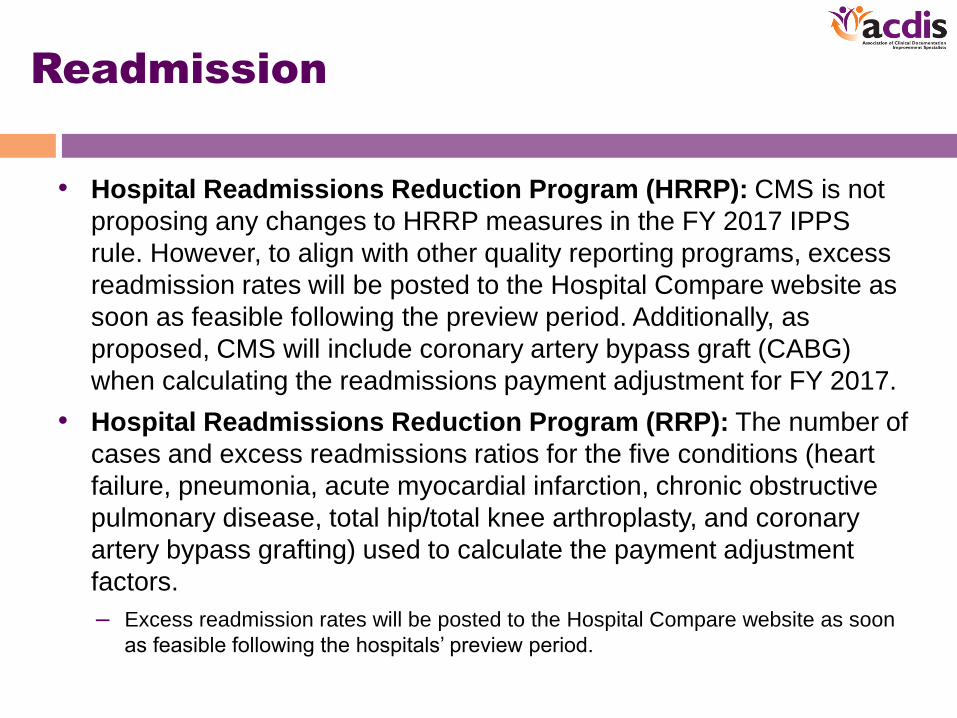
• Hospital Readmissions Reduction Program (HRRP): CMS is not
proposing any changes to HRRP measures in the FY 2017 IPPS
rule. However, to align with other quality reporting programs, excess
readmission rates will be posted to the Hospital Compare website as
soon as feasible following the preview period. Additionally, as
proposed, CMS will include coronary artery bypass graft (CABG)
when calculating the readmissions payment adjustment for FY 2017.
• Hospital Readmissions Reduction Program (RRP): The number of
cases and excess readmissions ratios for the five conditions (heart
failure, pneumonia, acute myocardial infarction, chronic obstructive
pulmonary disease, total hip/total knee arthroplasty, and coronary
artery bypass grafting) used to calculate the payment adjustment
factors.
– Excess readmission rates will be posted to the Hospital Compare website as soon
as feasible following the hospitals’ preview period.
Two-Midnight Rule
• Two-Midnight Rule: CMS will remove the 0.2% reduction from the two midnight rule.
• In FY2017, CMS will make a one-time increase of 0.8% to offset the payment reductions that occurred in FY2014, FY2015, and FY2016.
• Note while the two-midnight timeframe remains in effect, CMS will recognize exceptions based on documentation of the clinical need of the patient.

Two-Midnight Rule (cont.)
• CMS is finalizing regulations to implement the NOTICE Act, which requires hospitals to provide patients receiving more than 24 hours of observation services as an outpatient both written notice and oral explanation of the implications of this status
– Standard written notice needs to be provided, called the Medicare Outpatient Observation Notice (MOON) – this must be signed by patient or person acting on their behalf.
• The MOON is currently going through the Paperwork Reduction Act process, and comments on the MOON will be accepted for 30 days after the final rule is published.
• The draft MOON is available at https://www.cms.gov/Regulations-and-Guidance/Legislation/PaperworkReductionActof1995/PRA-Listing-Items/CMS-10611.html
• Hospitals and CAHs must fully implement use of the MOON no later than 90 calendar days from the date of PRA approval of the MOON, which will be 120 days after the publication of the final rule (including the 30 day comment period).
– CMS will provide oral explanation guidance in forthcoming manual provisions.

Two-Midnight Rule (cont.)
• Notice must be given to Medicare patients no later than 36 hours after observation services begin. However, the MOON can be provided before the patient has received more than 24 hours of observation services, and be in compliance with the written requirement.
• Please note – CMS is not proposing changes to the “Two-Midnight Rule” policy. The only changes CMS is proposing regarding this policy is the payment adjustment tied to it, and this is reflected in the overall 0.9% adjustment described above.

IPPS FY2017: P4P & VBP
• Hospital Value-Based Purchasing (VBP)
Program. CMS is adding 2 condition-specific
payment measures (for acute myocardial
infarction and heart failure) beginning with the
FY 2021 program year and a 30-day mortality
measure following CABG surgery beginning with
the FY 2022 program year.
59

Value-Based Purchasing (VBP)
–Percentage in play for hospitals rises to 2%.
–CMS estimates that $1.8 billion will be
redistributed among hospitals through VBP.
–CMS provides a summary of previously
adopted and recently base lined performance
periods for program year 2018-2022, including
adding AMI and HF payment measures for
2021. These will be calculated in the same
manner as CMS calculates the MSPB
measure.

Hospital IQR Program
• CMS will add 4 new claims-based measures for the FY
2019 payment determination and subsequent years:
Aortic Aneurysm Procedure Clinical Episode-Based
Payment Measure; Cholecystectomy and Common Duct
Exploration Clinical Episode-Based Payment Measure;
Spinal Fusion Clinical Episode-Based Payment
Measure; and Excess Days in Acute Care After
Hospitalization for Pneumonia.
• CMS is also removing 15 measures for the FY 2019
payment determination and subsequent years.

Hospital Acquired Conditions
(HAC) Program
• Hospital Acquired Conditions (HAC) Program:
– CMS is making five changes to existing HAC Reduction Program policies:
• Establishing National Healthcare Safety Network (NHSN) CDC
Healthcare Associated Infections (HAI) data submission requirements
for newly opened hospitals;
• Clarifying data requirements for Domain 1 scoring;
• Establishing performance periods for the FY 2018 and FY 2019 HAC
Reduction Program;
• Adopting the refined PSI 90: Patient Safety for Selected Indicators
Composite Measure (NQF # 0531); and
• Changing the Program scoring methodology from the current decile-
based scoring to a continuous scoring methodology
– HAC will reduce total IPPS payments by 1 percentage point to the top
quartile of ranked hospitals – no estimated dollar impact was provided.

Summary
• IPPS Changes take effect 10/1/2016.
• Work closely with Coding HIM on the MS-DRG
data.
• ICD-10-PCS operative changes to MS-DRGs.
• Accuracy of discharge disposition (PACT rule).
• Stay tuned on MOON and two mid-night.
• Quality, Quality and more Quality initiatives that
drive payment!
Next Steps
• Study your MS-DRG data and trends
• Run report of “Unspecified” codes
– Top 5 positions at least
• Review your top Physician Queries since 10/2016
• ICD-10-PCS may be a key for future aspects of CDI
– Enhance knowledge in the surgical documentation
area.
• Meet at least once a month with HIM Coding
– Dialog with HIM Coding on a regular basis.
– Q4 2016 AHA Coding Clinic.

Questions?

Thank you
References/Resources
• CMS IPPS Final Rule FY2017
• http://www.medaxiom.com/news/2016/08/10/news/how-
cms-final-rule-for-fiscal-year-2017-ipps-impacts-your-
business/
• http://www.besler.com/ipps2017/?utm_campaign=2016-
12+IPPS+2017&utm_source=hs_email&utm_medium=e
mail&utm_content=33340923&_hsenc=p2ANqtz-
_mmdnQo8y5ZwRIK4PmrLFShK2O0yPLN4YFjy8nD2V
X0HeJXcEAHYeyqIp9m-
w2wcwtgjYrdZagNAJAK4ggE3OrOJTOOw&_hsmi=3334
0923
ADDITIONAL INFORMATION REGARDING CEU CREDITS
if warranted.
Thank you. Questions?







