
Vancomycin-Intermediate and Vancomycin-Resistant Staphylococcus aureus (VISA/VRSA) Investigation Form
Arizona Department of Health Services
MEDSIS Case No:_____________________ REPORT SOURCE
County:____________________________ Initial report date:_________
☐Confirmed ☐Suspect Reporter: _________________ Reporter phone:__________
☐Not a case ☐Lost to follow up Reporter organization:_________________________________
Outbreak Name:________________________ Provider name:_____________ Provider phone:___________
Part of National Outbreak ☐Yes Provider organization:__________________________________
Name (last, first)_______________________ Birthdate___/___/____ or age_____ Sex: ☐M ☐F ☐UK
Street address_________________________ City________________ State______ Zip____________
Occupation/school grade:_______________ Employer/school/other:_____________________________
Ethnicity: ☐Hispanic ☐Non-Hispanic
☐Unknown Country of birth:__________________________
Race: ☐White ☐African American
☐Native Hawaiian/Pac Islander ☐Asian
☐American Indian/ AK Native ☐Other_______________
Date of Onset of symptoms: ____/____/_____ Diagnosis Date:____/____/_____
Is the patient currently hospitalized ☐Yes ☐No ☐UK If yes, complete information below for current hospitalization: Name of hospital or healthcare facility_____________
Name of Physician treating_______________________
Physician Telephone number Admit date___/___/___ Discharge date ___/___/___
Outcome of illness
☐ Died Date of death:___/___/____ ☐ Unknown
_________________ Cause of death___________________
(check all that apply)
☐ Immunosuppressive therapy/Immunosuppressive condition ☐ HIV/AIDS
☐ Emphysema/COPD ☐ Renal disease
☐ Neurologic/neuromuscular disease ☐ Rheumatoid arthritis
☐ Other (specify)____________________________________
UK=Unknown
PATIENT DEMOGRAPHICS
CLINICAL INFORMATION
Clinical Diagnosis_____________________________________________________________________________
☐ Survived
If patient is deceased: Death Certificate Number:
Past Medical History and Underlying Conditions
☐ Current Smoker ☐ Cerebrovascular disease
☐ Other tobacco use ☐ Liver disease
☐ Alcohol abuse ☐ Diabetes mellitus
☐ IVDU ☐ Neoplastic disease
☐ Other drug use ☐ Cystic ŦƛōNJƻǎƛǎ ☐ Asthma
☐ Congestive heart failure
Y=Yes N=No
Clinical Diagnosis_____________________________________________________________________________
☐ Survived
If patient is deceased: Death Certificate Number:
Past Medical History and Underlying Conditions
☐ Current Smoker ☐ Cerebrovascular disease
☐ Other tobacco use ☐ Liver disease
☐ Alcohol abuse ☐ Diabetes mellitus
☐ IVDU ☐ Neoplastic disease
☐ Other drug use ☐ Cystic fibrosis
☐ Asthma
☐ Congestive heart failure
Y=Yes N=No
Revised 6/2016

In the past year did the patient have: ☐ Surgery ☐Dialysis ☐ Invasive device or catheter in place at least 1 day before Staphylococcus aureus collected
☐ Residence in a nursing home or other long-term care facility_________________________ Date of stay_____________
☐ Prior hospitalization _________________________________________________________ Date of stay_____________
Has patient received vancomycin in the past year? ☐Y ☐N ☐UK If yes, Dates received:___/___/____ to ___/____/____ ____/____/____ to ____/____/____
Does patient have prior history of methicillin-resistant Staphylococcus aureus (MRSA)?
☐Y ☐N ☐UK
If yes, Date of most recent MRSA Positive culture___/___/___ Culture Site________________________
Does patient have prior history of vancomycin-resistant enterococci (VRE)? ☐Y ☐N ☐UK
If yes, Date of most recent VRE Positive culture___/___/___ Culture Site________________________
Is the patient a healthcare worker? ☐Y ☐N ☐UK
Laboratory Name_____________________ Specimen ID_______________ Specimen Type__________ Collection Date ___/___/___ Result Date ___/____/_____ Organism isolated ☐ VISA ☐ VRSA
Susceptibility method used and MIC value: ☐ Automated susceptibility method (specify)________________________
☐ Non-automated MIC
☐ Kirby-Bauer
☐ E-test
☐ Vancomycin-screen plate
☐ Broth micro dilution
MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________
Was the MIC result repeated? ☐Y ☐N ☐UK Were the lab results confirmed by the Arizona State Laboratory? ☐Y ☐N ☐UK
If yes, Specimen ID# ______________________ Specimen Type____________________________ Collection Date ___/___/___ Result Date ___/____/_____ Organism isolated ☐ VISA ☐ VRSA Susceptibility method used and MIC value:
☐ Automated susceptibility method (specify)________________________
☐ Non-automated MIC
☐ Kirby-Bauer
☐ E-test
☐ Vancomycin-screen plate
☐ Broth micro dilution
MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________
Was the MIC result repeated? ☐Y ☐N ☐UK Were the lab results confirmed by the Centers for Disease Control and Prevention? ☐Y ☐N ☐UK If yes, Specimen ID# ______________________ Specimen Type____________________________ Collection Date ___/___/___ Result Date ___/____/_____ Organism isolated ☐ VISA ☐ VRSA Susceptibility method used and MIC value:
☐ Automated susceptibility method (specify)________________________
☐ Non-automated MIC
☐ Kirby-Bauer
☐ E-test
☐ Vancomycin-screen plate
☐ Broth micro dilution
MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________ MIC (µg/ml)_______________
Was the MIC result repeated? ☐Y ☐N ☐UK
LABORATORY INFORMATION
EXPOSURE HISTORY
Revised 6/2016

Were antibiotics prescribed? ☐Y ☐N ☐UK
List antibiotics prescribed before VISA/VRSA culture results known
_____________________________________________
List antibiotics prescribed after VISA/VRSA culture results known
_____________________________________________
Were other treatment modalities used (e.g. surgical intervention? ☐Y ☐N ☐UK
If yes, specify_________________________________________________________________________________________
DIAGNOSTIC CRITERIA ACTIONS TAKEN
Laboratory Criteria for Diagnosis
Isolation of Statphylococcus aureus from any body site AND
Intermediate or resistance of S. aureus isolate to vancomycin, detected and defined according to Clinical and Laboratory Standards Institute approved standard and recommendations
Case Classification CONFIRMED: A case of vancomycin-intermediate or vancomycin-resistant S. aureus that is laboratory confirmed
MIC≤ 2 µg/ml for VSSA MIC = 4 – 8 µg/ml for VISA MIC ≥ 16 µg/ml for VRSA
☐ No risk factors/exposures could be identified
☐ Patient could not be interviewed/LTF
☐ Infection control recommendations provided
☐ Epi-linked to confirmed case? MEDSIS ID of confirmed case:______________________
☐ Education provided to case/contacts/facilities
☐ Follow-up to ensure compliance with treatments
☐ Follow-up to contacts who may have been exposed
☐ Contact investigation conducted according to CDC guidelines http://www.cdc.gov/hai/pdfs/VRSA-Investigation-Guide-05_12_2015.pdf
☐ Laboratory results obtained from testing laboratory
☐ Medical records obtained on case(s)
☐ Other _________________________________________
Observed MIC Interpreted MIC VISA/VRSA
1.5 µg/ml 2 µg/ml VSSA
2 µg/ml 2 µg/ml VSSA
3 µg/ml 4 µg/ml VISA
4 µg/ml 4 µg/ml VISA
5 µg/ml 8 µg/ml VISA
6 µg/ml 8 µg/ml VISA
7 µg/ml 8 µg/ml VISA
8 µg/ml 8 µg/ml VISA
9 – 15 µg/ml 16 µg/ml VRSA
Organisms Identified:
☐ MRSA: If isolate is determined to have a MIC value ≤2, was obtained from a sterile site, and susceptibility pattern determined resistance to methicillin/oxacillin
☐ VISA: If isolate is determined to have a MIC value of 4-8 µg/ml ☐ VRSA: If isolate is determined to have a MIC value of 16 µg/ml from CDC
INVESTIGATOR(S):_____________________________ DATE:____/_____/_____ DATE CLOSED:____/____/____
TREATMENT
FOR PUBLIC HEALTH DEPARTMENT USE ONLY
Revised 6/2016
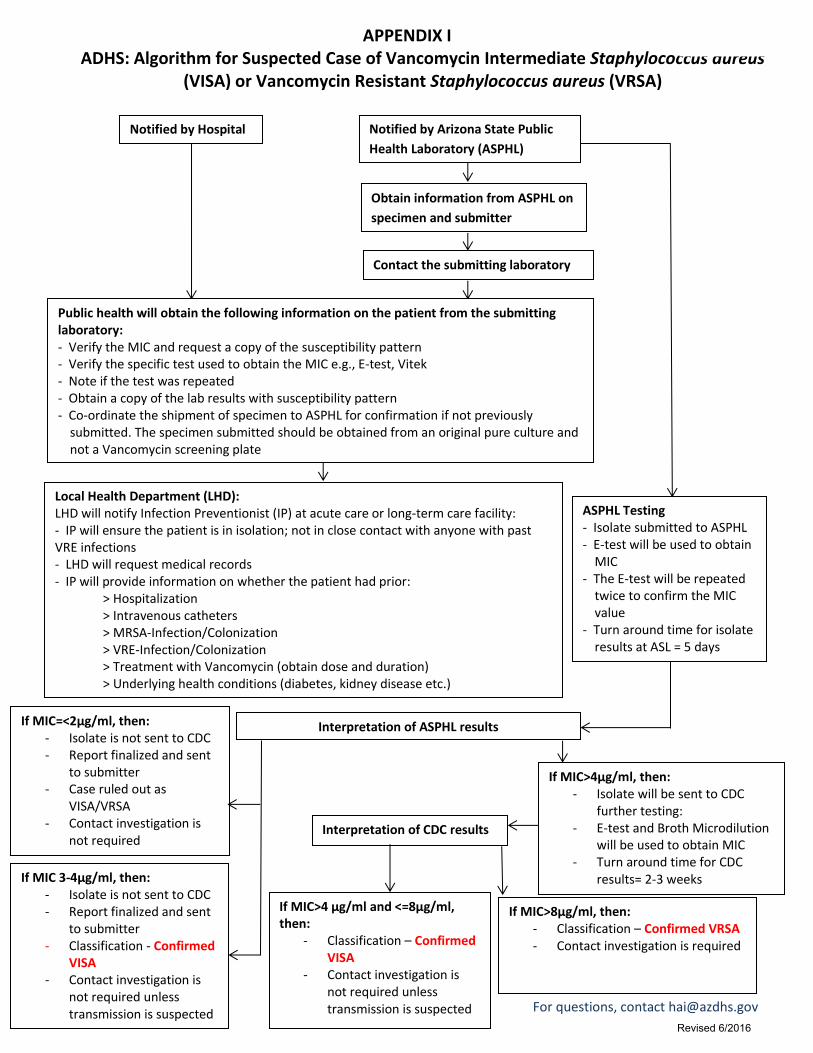
APPENDIX I ADHS: Algorithm for Suspected Case of Vancomycin Intermediate Staphylococcus aureus
(VISA) or Vancomycin Resistant Staphylococcus aureus (VRSA)
Notified by Hospital Notified by Arizona State Public
Health Laboratory (ASPHL)
Obtain information from ASPHL on
specimen and submitter
Contact the submitting laboratory
Public health will obtain the following information on the patient from the submitting laboratory: - Verify the MIC and request a copy of the susceptibility pattern - Verify the specific test used to obtain the MIC e.g., E-test, Vitek - Note if the test was repeated - Obtain a copy of the lab results with susceptibility pattern - Co-ordinate the shipment of specimen to ASPHL for confirmation if not previously
submitted. The specimen submitted should be obtained from an original pure culture and not a Vancomycin screening plate
Local Health Department (LHD): LHD will notify Infection Preventionist (IP) at acute care or long-term care facility: - IP will ensure the patient is in isolation; not in close contact with anyone with past VRE infections - LHD will request medical records - IP will provide information on whether the patient had prior:
> Hospitalization > Intravenous catheters > MRSA-Infection/Colonization > VRE-Infection/Colonization > Treatment with Vancomycin (obtain dose and duration) > Underlying health conditions (diabetes, kidney disease etc.)
Interpretation of ASPHL results If MIC=<2µg/ml, then: - Isolate is not sent to CDC - Report finalized and sent
to submitter - Case ruled out as
VISA/VRSA - Contact investigation is
not required
If MIC>4µg/ml, then: - Isolate will be sent to CDC
further testing: - E-test and Broth Microdilution
will be used to obtain MIC - Turn around time for CDC
results= 2-3 weeks
Interpretation of CDC results
If MIC>4 µg/ml and <=8µg/ml, then:
- Classification – Confirmed VISA
- Contact investigation is not required unless transmission is suspected
If MIC 3-4µg/ml, then: - Isolate is not sent to CDC - Report finalized and sent
to submitter - Classification - Confirmed
VISA - Contact investigation is
not required unless transmission is suspected
If MIC>8µg/ml, then: - Classification – Confirmed VRSA - Contact investigation is required
ASPHL Testing - Isolate submitted to ASPHL - E-test will be used to obtain
MIC - The E-test will be repeated
twice to confirm the MIC value
- Turn around time for isolate results at ASL = 5 days
For questions, contact [email protected]
Revised 6/2016
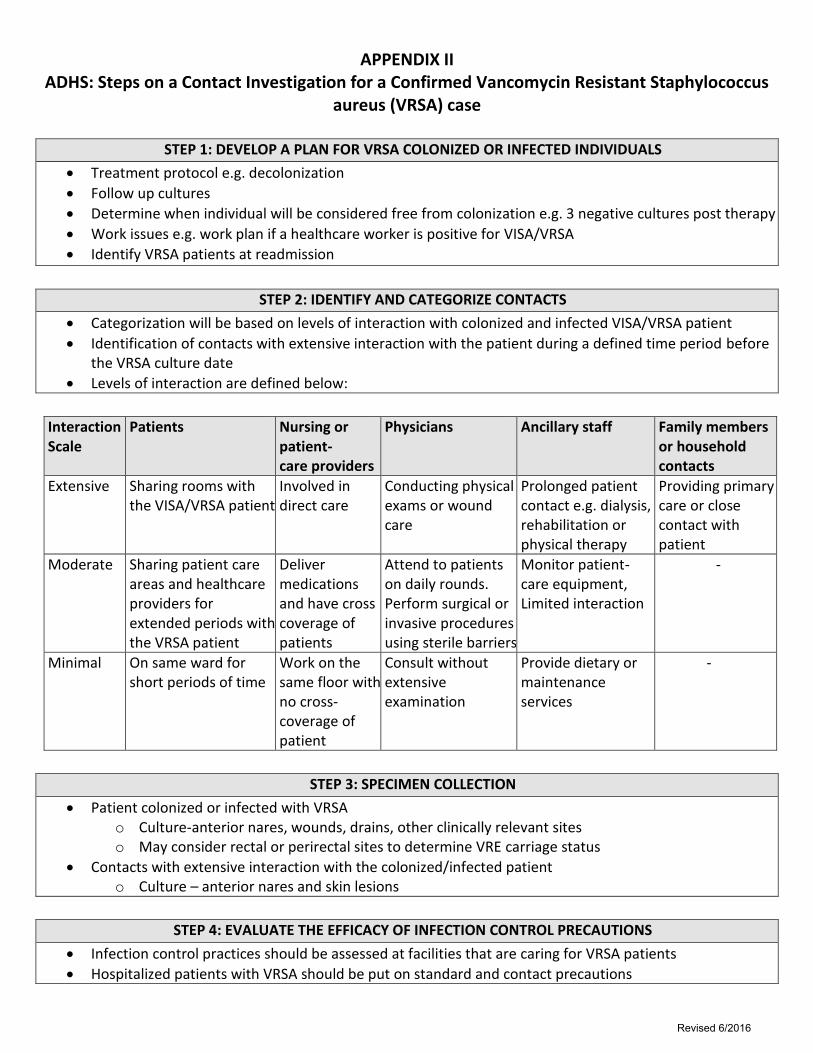
APPENDIX II ADHS: Steps on a Contact Investigation for a Confirmed Vancomycin Resistant Staphylococcus
aureus (VRSA) case
STEP 1: DEVELOP A PLAN FOR VRSA COLONIZED OR INFECTED INDIVIDUALS
Treatment protocol e.g. decolonization
Follow up cultures
Determine when individual will be considered free from colonization e.g. 3 negative cultures post therapy
Work issues e.g. work plan if a healthcare worker is positive for VISA/VRSA
Identify VRSA patients at readmission
STEP 2: IDENTIFY AND CATEGORIZE CONTACTS
Categorization will be based on levels of interaction with colonized and infected VISA/VRSA patient
Identification of contacts with extensive interaction with the patient during a defined time period before the VRSA culture date
Levels of interaction are defined below:
Interaction Scale
Patients Nursing or patient- care providers
Physicians Ancillary staff Family members or household contacts
Extensive Sharing rooms with the VISA/VRSA patient
Involved in direct care
Conducting physical exams or wound care
Prolonged patient contact e.g. dialysis, rehabilitation or physical therapy
Providing primary care or close contact with patient
Moderate Sharing patient care areas and healthcare providers for extended periods with the VRSA patient
Deliver medications and have cross coverage of patients
Attend to patients on daily rounds. Perform surgical or invasive procedures using sterile barriers
Monitor patient-care equipment, Limited interaction
-
Minimal On same ward for short periods of time
Work on the same floor with no cross-coverage of patient
Consult without extensive examination
Provide dietary or maintenance services
-
STEP 3: SPECIMEN COLLECTION
Patient colonized or infected with VRSA o Culture-anterior nares, wounds, drains, other clinically relevant sites o May consider rectal or perirectal sites to determine VRE carriage status
Contacts with extensive interaction with the colonized/infected patient o Culture – anterior nares and skin lesions
STEP 4: EVALUATE THE EFFICACY OF INFECTION CONTROL PRECAUTIONS
Infection control practices should be assessed at facilities that are caring for VRSA patients
Hospitalized patients with VRSA should be put on standard and contact precautions
Revised 6/2016







