Value-of-Information Analysis for Patient-Centered Outcomes Research Prioritization
Prepared for:
Patient-Centered Outcomes Research Institute
1701 Pennsylvania Avenue, NW, Suite 300
Washington, DC 20006
www.pcori.org
Prepared by:
Duke Evidence-based Practice Center
Durham, NC
Authors:
Evan Myers, M.D., M.P.H.
Amanda J. McBroom, Ph.D.
Lan Shen, M.D.
Rachael E. Posey, M.S.L.S.
Rebecca Gray, D.Phil.
Gillian D. Sanders, Ph.D.
March 9, 2012
DISCLAIMER
All statements in this report, including its findings and conclusions, are solely those of the authors
and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute
(PCORI), its Board of Governors or Methodology Committee. PCORI has not peer-reviewed or
edited this content, which was developed through a contract to support the Methodology
Committee’s development of a report to outline existing methodologies for conducting patient-
centered outcomes research, propose appropriate methodological standards, and identify
important methodological gaps that need to be addressed. The report is being made available free
of charge for the information of the scientific community and general public as part of PCORI’s
ongoing research programs. Questions or comments about this report may be sent to PCORI at
[email protected] or by mail to 1828 L St., NW, Washington, DC 20036.
1
I. Introduction
The purpose of this document is to discuss the potential use of value-of-information analysis
(VOI) as a tool for research priority setting for the Patient-Centered Outcomes Research
Institute (PCORI). The paper is divided into six sections. First, we provide a brief description of
VOI, using an example based on the standard cost-effectiveness framework. Next, we review
the existing literature on the application of VOI to research prioritization in health care settings,
followed by a discussion of challenges to VOI identified in this literature. In the fourth section,
we discuss the unique challenges to the use of VOI for research prioritization by PCORI, in
particular, the desirability of alternatives to cost-effectiveness as a decision threshold, followed
by some proposed solutions to these challenges. Finally, we provided suggestions for
evaluating these potential solutions within PCORI’s research agenda.
II. Description of VOI
VOI is an approach to research prioritization which uses Bayesian methods to estimate the
potential benefits of gathering further information (through more research) before making a
decision. In “classic” decision analysis, the optimal choice between two or more strategies is the
one with the highest expected value; for each strategy, the expected value is calculated by
multiplying the probability of a given outcome by the value of that outcome. Because this
calculation is almost always an estimate made on the basis of imprecise or incomplete data, the
result is more properly referred to as the expected value given current information. The
underlying uncertainty in the data raises the possibility that a decision made on the basis of the
expected value given current information may be incorrect. Using Bayesian methods, it is
possible to calculate the expected value given perfect information—in other words, the outcome
if the optimal decision were made every time. The difference between these two values is the
expected value of perfect information (EVPI), the upper bound of the opportunity cost of making

2
a wrong decision; any effort to improve the quality of available data that costs less than the
EVPI is worth pursuing.
A. Example Based on the Standard Cost-Effectiveness Framework
We can compare two hypothetical treatments, A and B, for a potentially fatal disease.
Although VOI for health care research has traditionally been performed using a cost-
effectiveness framework, where the optimal decision is based on a willingness-to-pay (WTP)
threshold defined in terms of cost per quality-adjusted life year (QALY) saved,1-5 the approach
requires only that an “optimal” decision be defined—how that decision is defined is less
important (the implications for this for PCORI are discussed in the last two sections). For this
example, we assume that the initial costs of the two treatments are identical, so that the only
costs that need to be considered are those associated with failed treatment or treatment
complications, and our primary outcome is unadjusted life expectancy. We also assume that no
randomized trials have been performed, and that the only available data on treatment
effectiveness and complication rates are from two case series of 50 (Treatment A) and 100
(Treatment B) patients, while data on mortality after a complication is available from an
administrative dataset of 1000 patients. For the purposes of this example, we do not consider
the effects of inadequate study design on uncertainty and focus only on sample size; we also do
not consider the effects of uncertainty in cost estimates. Table 1 shows the available “data,”
including 95 percent confidence intervals, and Figure 1 shows a simple decision tree used to
estimate the expected value given this data.
Table 1. Input Variables and Values for Treatments A and B
Parameter Treatment A
(95% CI)
Treatment B
(95% CI)
Cure rate 94%
(86.0 to 98.6%)
90%
(83.5 to 95.0%)
Life expectancy if cured 20 years
Life expectancy if treatment fails 5 years

3
Parameter Treatment A
(95% CI)
Treatment B
(95% CI)
Costs of managing treatment failure $50,000
Overall complication rate 20%
(10.0 to 27.5%)
5%
(2.1 to 10.1%)
Mortality rate after complication 10%
(8.2 to 12.0%)
Cost of complication $10,000
Costs associated with fatal complication
$50,000
Abbreviation: CI = confidence interval
Figure 1. Schematic of decision tree used in example. pCompA = complication rate for treatment
A, pCompB = complication rate for treatment B, MortalityComp = mortality rate after experiencing
a complication, pCureA = probability of cure with Treatment A, pCureB = probability of cure with

4
Treatment B, “#” = 1-the probability of the branch above the “#”.
Table 2 shows the expected values based on the mean value of the parameters. Treatment
A results in better overall life expectancy because of the higher cure rate, but has higher overall
costs because of a higher complication rate, resulting in an incremental cost-effectiveness ratio
of $692 per year of life saved.
Table 2. Expected Values of Outcomes of Interest Given Treatment A or B
Outcome Treatment A Treatment B
Mean life expectancy 18.72 years 18.40 years
Mean costs $10,940 $10,725
Mortality from complications of treatment 2.0% 0.5%
In a setting where the optimal decision is based on cost-effectiveness, Treatment A would
be preferred based on these results if a decisionmaker were willing to pay at least $692 for each
year of life saved. An alternative to incremental cost-effectiveness ratios for comparing different
options across varying WTP thresholds is net benefits, expressed as either net monetary
benefits (NMB) or net health benefits (NHB). Both measures integrate costs, effectiveness, and
WTP into a single number. For example, NMB is defined as
Willingness-to-pay threshold * Net quality-adjusted life expectancy – Net costs
At any given WTP, the option with the highest NMB is “optimal”; in Table 2, the NMB for
Treatment A at a WTP threshold of $600 (less than the incremental cost-effectiveness ratio of
$692) would be ($600*18.72) – $10,940, or $292, while for Treatment B it would be
($600*18.40) – $10,725, or $315, and Treatment B would be preferred; at a threshold of $750 (a
value higher than the incremental cost-effectiveness ratio), the corresponding values would be
$3,100 for Treatment A and $3,075 for Treatment B, and Treatment A is “optimal.”

5
However, even at a single WTP, the possibility that Treatment B would be preferred cannot
be ruled out given the wide confidence intervals for both effectiveness and complication rates. In
probabilistic sensitivity analysis (PSA), multiple simulations are performed; drawing the value for
each parameter from a distribution based on the available data or expert input at the beginning
of each simulation. The expected value is the mean of all the simulations and should
approximate the expected value estimated from the means of each parameter. The advantages
of PSA include quantification of the uncertainty surrounding the expected value, and, in the
context of decisionmaking, an estimate of the probability of making an incorrect decision based
on the available information.
Table 3 shows the results of 10 simulations from our original example, at a WTP threshold of
$750.
Table 3. Outcomes from 10 Simulations of Treatment A and B Assuming a WTP Threshold of $750
Simulation Number Net Benefits Treatment A
Net Benefits Treatment B
Maximum Net Benefits
Preferred Strategy
Opportunity Cost
1 $4,180 $4,306 $4,306 B $0
2 $2,273 $2,415 $2,415 B $0
3 $7,095 $4,507 $7,095 A $2,588
4 $3,186 $4,017 $4,017 B $0
5 $3,504 $3,433 $3,504 A $72
6 $5,698 $6,740 $6,740 B $0
7 $4,762 $3,718 $4,762 A $1,044
8 $3,960 $1,919 $3,960 A $2,041
9 $5,071 $5,964 $5,964 B $0
10 $1,904 $5,123 $5,123 B $0
Expected value (mean of simulations 1–10) $4,163 $4,214 $4,789 $575
Abbreviation: WTP = willingness-to-pay
Each simulation draws the values for effectiveness, complication rates, and mortality from
the distributions determined by the sample size. The mean value for all the simulations is the
expected value—for Treatment A, $4,163, and, for Treatment B, $4,214. Based on the expected

6
NMB, Treatment B is the preferred option. However, in 4 of the 10 simulations, Treatment A had
the higher NMB. If we knew the results of each simulation, we would choose the option with the
highest net benefit in that simulation. In this case, the expected value would be the mean of the
maximum values for the entire set of simulations, or the expected value given perfect
information. The difference between this value ($4,789) and the expected value given current
information ($4,214) is the expected value of perfect information (EVPI, $575).
Alternatively, this can be considered as the opportunity cost based on making the wrong
decision. If we choose Treatment B based on its higher expected value, there is a 40 percent
chance that we would be wrong; the difference between the net benefits of A and B in each
simulation where A was preferred (numbers 3, 4, 7, and 8 in Table 3) represents the opportunity
cost of choosing B based on its expected value; the expected overall opportunity cost is the
mean of these, or $575 (identical to the value obtained by subtracting the expected value given
current information from the expected value given perfect information).
Further research might result in a narrower range of parameter values for both treatments—
the higher the EVPI, the more worthwhile it would be to invest in further research. Note that the
EVPI is dependent on the WTP threshold—in general, the EVPI will be highest at values of the
threshold where there is the greatest uncertainty about the optimal decision. The decision model
generates estimates of the EVPI for individual “patients”; these can then be converted to a
population-level estimate based on the number of potential patients, the time horizon under
which the intervention will be used, and an appropriate discount rate. If the expected costs of
research to reduce uncertainty are less than the population EVPI, then further research could be
considered. At the simplest level, using the example above, the EVPI value of $575 would be
multiplied by the expected number of patients who would be candidates for Treatment A or
Treatment B over a given future time horizon, incorporating an appropriate discount rate; this
value represents the upper bound of what would be reasonable to spend to reduce uncertainty
7
surrounding Treatments A and B. As a tool for research prioritization, the population EVPI has
two main potential applications: (a) as a “go/no go” threshold for deciding whether further
research is worthwhile; and (b) in theory, as a way to compare the “cost-effectiveness” of
research across different interventions, or even across different clinical problems or therapeutic
areas.
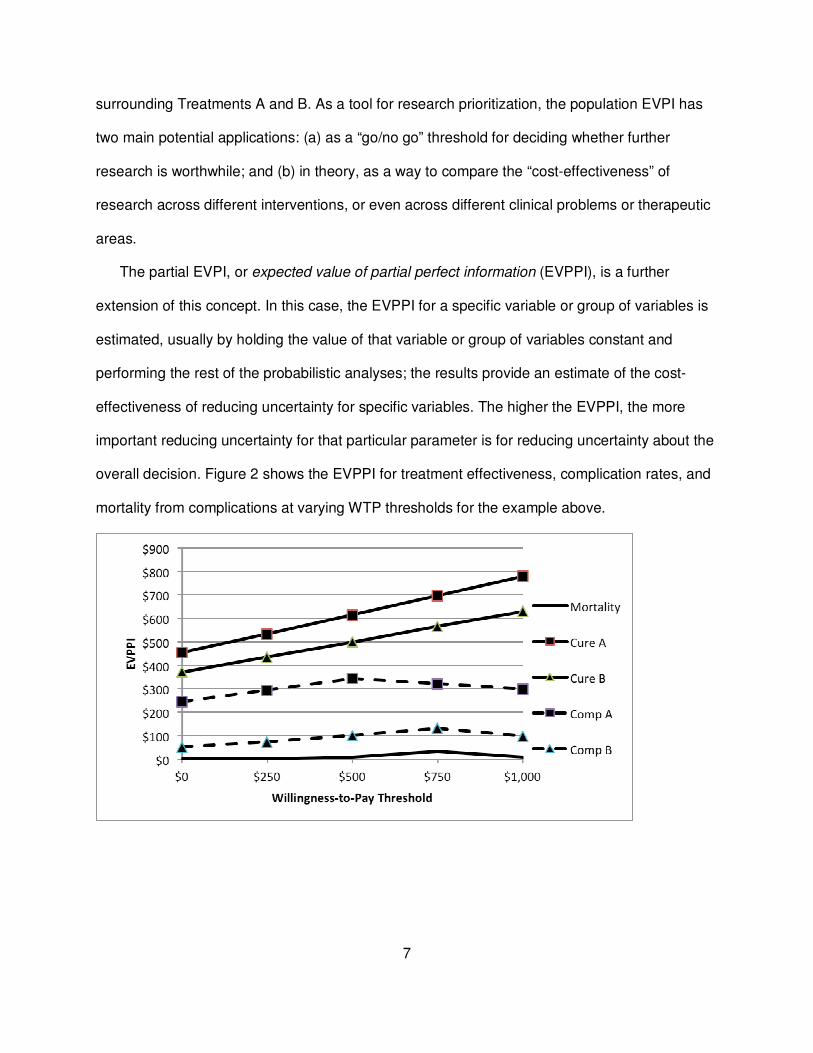
The partial EVPI, or expected value of partial perfect information (EVPPI), is a further
extension of this concept. In this case, the EVPPI for a specific variable or group of variables is
estimated, usually by holding the value of that variable or group of variables constant and
performing the rest of the probabilistic analyses; the results provide an estimate of the cost-
effectiveness of reducing uncertainty for specific variables. The higher the EVPPI, the more
important reducing uncertainty for that particular parameter is for reducing uncertainty about the
overall decision. Figure 2 shows the EVPPI for treatment effectiveness, complication rates, and
mortality from complications at varying WTP thresholds for the example above.

8
Figure 2. EVPPI at varying WTP thresholds for uncertain parameters. Cure A = cure rate of
Treatment A; Cure B = cure rate of Treatment B; Comp A = complication rate of Treatment A;
Comp B = complication rate of treatment B; Mortality = mortality rate after complications.
In this example, the mortality rate for complications has a very low EVPPI, in part because of
the greater precision of the already existing data. Complication rates are next in importance,
with rates associated with Treatment A having a higher EVPPI (because of lower precision).
Effectiveness has the highest EVPPI, with Treatment A again having the highest value.
Therefore, it follows that reducing uncertainty about the relative effectiveness of the two
treatments has the highest priority, followed by complication rates. These values can be used to
inform study designs, including sample size needs.1,6-13
B. Summary
In summary, VOI is a method for estimating the impact of uncertainty on the likelihood of
making an incorrect decision. By estimating the overall EVPI based on the currently available
data, policymakers can estimate the value of any further research prior to making a decision. By
estimating the EVPPI for specific components of the uncertainty, policymakers can estimate the
relative value of research on those components. The next section reviews specific published
applications of VOI within the health care setting.
III. Current State of VOI in Health Care Research Prioritization
A. Literature Search Methods
Search Strategy
To identify published literature relevant to this review, we performed a search of the
PubMed® database using search terms relevant to VOI. We also reviewed all included
references from a prior study performed by our research group in which we evaluated the use of
modeling techniques, including VOI analysis, for research prioritization.14 Details of the search

9
strategy used, a flow diagram depicting the results of the search and screening process, and
lists of included and excluded articles are provided in Appendix A.
Inclusion and Exclusion Criteria
At the title-and-abstract screening level, articles were included if they met the following
criteria:
• Published in English language from January 1, 1990, to the present
• Describe an explicit priority-setting process which employs either VOI or decision
modeling in another format, or provide explicit discussion or examples of VOI analyses
Articles were excluded if they focused on establishing priorities for providing health services
rather than prioritization of research.
We retrieved the full text of all potentially relevant literature included at the title-and-abstract
level and conducted a second review for inclusion and exclusion. For inclusion at the full-text
stage, articles were required to meet the following criteria:
• Available in English
• Full publication (excluding articles only available as abstracts)
• Published January 1, 1990 to present
• Either
1. describes an explicit priority-setting process which employs either VOI or
decision modeling in another format, or
2. provides explicit discussion or examples of VOI analyses
• Focused on research prioritization (excluding prioritization of health services or other
topics)
• Includes a formal framework or process for research prioritization
• Includes specific research prioritization recommendations (excluding articles that provide
only a description of a framework/ process)

10
• Prioritization is VOI- or decision analysis-based
• Context is relevant to PCORI
Study Selection
Two investigators independently reviewed each title and abstract for potential relevance;
articles included by either investigator underwent full-text screening. At the full-text screening
stage, two investigators independently reviewed the full text of each article and indicated a
decision to include or exclude the article for data abstraction. When the paired reviewers arrived
at different decisions about whether an article met criteria for inclusion, or about the reason for
exclusion, we reached a final agreement through review and discussion among investigators.
Full-text articles meeting eligibility criteria were included for data abstraction. All screening
decisions were made and tracked in a Distiller SR database (Evidence Partners Inc., Manotick,
ON, Canada).
Data Abstraction
We developed a data abstraction form in Distiller SR for collecting data from all included
studies. Abstractors worked in pairs: the first abstracted the data, and the second reviewed the
article and the accompanying abstraction form to check for accuracy and completeness.
Disagreements were resolved by consensus or by assistance from a third, arbitrating member of
the study team. Abstracted data elements are listed in Appendix B.
Additional Analysis Based on Web of Science Search
To explore the potential impact and translation of the VOI studies we identified and their
findings we performed a Web of Science search to determine the number of published studies
that cited our included VOI papers. These studies were then evaluated to determine whether
they were methods papers, systematic reviews, or cost-effectiveness analyses, or if they could
potentially represent primary research on a topic informed by the VOI.

11
B. Literature Search Findings
Table 4 illustrates the results of the search. The majority of the identified VOIs included
patient preferences or behaviors (usually as part of a QALY) as one of the outcomes or key
probabilities; of these, approximately half identified these parameters as one of the three most
important sources of uncertainty (i.e., had high EVPPI).
Table 4. Characteristics of Existing VOI Literature
Sponsor Number of VOI Papers (% of all VOI)
Studies with Patient Preferences Included (% of VOI Papers by Sponsor)
Studies That Cite Patient Preferences as Important* (% of VOI Papers by Sponsor Where Patient Preferences Included)
UK NICE 28 (34) 27 (96) 10 (37)
Other non-U.S. government 17 (21) 14 (82) 6 (43)
U.S. government 9 (11) 7 (78) 4 (57)
Other** 28 (34) 19 (68) 8 (42)
TOTAL 82 (100) 67 (82) 28 (42)
*Includes studies that listed uncertainties related to patient preferences/adherence within the top three parameters requiring future research **Includes studies funded through academic, advocacy groups, or industry sources, and those where the sponsor was either unclear or unreported. Abbreviations: NICE = National Institute for Health and Clinical Excellence; VOI = value-of-information analysis
Based on the available evidence, the greatest experience with the use of VOI for
prioritization by research sponsors is in the UK with 28 of the 82 (34%) included papers being
supported by the National Institute for Health and Clinical Excellence (NICE) within the UK’s
Health Technology Assessment (HTA) program; an additional 18 studies were not specifically
funded by NICE but were performed by authors within the UK through other research funding
mechanisms. There does not appear to be any meaningful experience in the United States
other than small pilot studies. Of particular interest to PCORI, patient-centered outcomes such
as quality of life, or patient behaviors such as adherence to recommendations, had high EVPPIs
in approximately half of the papers where these parameters were included as an outcome.

12
Even within the UK, however, the extent to which VOI analyses have specifically informed
coverage decisions or funding for studies judged to be worthwhile on the basis of VOI is
unclear. Of the 556 articles citing the included VOI papers identified in the Web of Science, only
40 were not methods papers, systematic reviews, or cost-effectiveness analyses, and—based
on their title, abstract, and date of publication—could potentially represent primary research on
a topic informed by the VOI. However, none of these papers specifically cited the VOI as a
justification for the study or as a validation of the importance of the results. Technically, VOI is
clearly feasible for patient-centered research and is able to generate potentially useful estimates
of EVPI and EVPPI. However, there are challenges to the broader use of VOI by the research
community which have been consistently identified. The next section describes these general
challenges, focusing on broad issues rather than specific unresolved methodological debates.
IV. General Challenges to the Use of VOI for Research
Prioritization
A. Resources Needed to Develop Appropriate Models.
Conducting a VOI requires extensive resources, including:
• Personnel: Expertise is required in the clinical area being studied, in the evaluation
and synthesis of literature and other data sources, in computer decision modeling,
and in the use of VOI and its associated analyses itself. Centers with the appropriate
mix of expertise are limited; indeed, our review showed that 38% of all the identified
VOI papers were authored by one of only three groups (20 studies from the
University of York, 7 from Erasmus University Medical Center, and 4 from University
of Chicago).
• Time: The parameter inputs for a VOI require, at the very least, a systematic review
of the literature, and often involve primary data analysis and synthesis (for example,

13
of cost data) as well. If such a review has not preceded the decision to utilize VOI,
time must be budgeted for this review. Model building, validation, and calibration also
require substantial amounts of time. Finally, because of the need to use probabilistic
analytic methods, the physical time required to perform VOI can be substantial.
• Computing resources: The time required to perform VOI can be reduced with more
powerful computers, or with distributed computing, but this requires additional
investment in hardware and software programming.
In some cases, a “minimal modeling” approach to VOI can be used which requires
substantially less investment. As described by Meltzer and colleagues,15 minimal modeling
appears to be most useful when an intervention affects quality of life alone (eliminating the need
to model survival or other clinical outcomes); when a study follows cohorts of patients
randomized from the time of treatment to death and records all relevant outcomes; or when
outcomes data are available from a study in which survival or quality of life differ up to a certain
point, then become similar. This approach is unlikely to be applicable for interventions for
chronic disease, where followup to death is uncommon, and, as the authors note, estimating the
EVPPI for specific parameters is impossible without a decision model. Another disadvantage is
the inability to use the same model to evaluate different interventions, populations, or other
scenarios by revising the model parameters.
As the authors point out, even a minimal modeling approach requires an investment of
resources that could otherwise potentially be used to fund direct research to answer research
questions. Whether the substantial investment required to incorporate VOI into research
prioritization by PCORI would ultimately lead to a more efficient use of resources is unclear, but
there may be methods to provide some empiric data, which we discuss in the final section.

14
B. Scope of VOI
There are numerous potential ways that VOI can be used to inform research priorities, but
some of these are likely to be more feasible than others.
• Prioritizing across disease areas: In theory, population EVPIs could be estimated for
broad classifications of diseases and conditions (e.g., cancer versus heart disease
versus pregnancy-related conditions), or within narrower categories (e.g., breast versus
ovarian versus prostate cancer), and these estimates used to allocate resources (for
example, to the appropriate National Institutes of Health [NIH] institutes). However, the
technical challenges and resources required to develop the comprehensive set of
models needed to generate reasonable estimates across diseases and conditions make
this impractical for the foreseeable future. In the shorter term, VOI is likely to be limited
to condition-specific prioritization decisions.
• Prioritizing within a condition: For conditions where several broad categories of
intervention are potentially available, it may be possible to compare the relative value of
further research within each category. For example, attempts at identifying effective
screening strategies for ovarian cancer have consistently failed,16,17 and modeling
studies suggest that this is largely due to the natural history of the disease rather than
inadequate screening technology.18,19 VOI comparing the EVPI for further research into
screening relative to primary prevention strategies or improved treatments for ovarian
cancer could help inform the relative allocation of resources.
• Prioritizing specific comparative effectiveness research: The most common application
of VOI to date has been in identifying whether further research is justified prior to
adapting a particular intervention, and which specific areas contribute most to
uncertainty, and it seems likely that this will remain the most common application for
some time. This suggests that initial applications of VOI may fall within areas where
15
there are already existing and generally well-accepted models (such as cervical, breast,
prostate, colorectal cancer, cardiovascular disease, and HIV); however, these areas may
not necessarily be the ones where the potential benefits of VOI are greatest.
• Prioritizing attributes of patient experience common to multiple conditions: One potential
category where comparison of VOI results across different diseases or conditions might
be useful is in prioritizing research into different aspects of patient experiences with the
healthcare system that affect multiple conditions. In this case, the between-condition
comparisons could focus on relative ranking, rather than specific EVPIs or EVPPIs. For
example, adherence to recommendations is likely to be important to the overall
effectiveness of screening for a variety of conditions. If uncertainty about the impact of
specific attributes of a physician/health system experience on adherence is consistently
highly ranked in terms of EVPPI in VOI analyses of screening for multiple conditions,
further research into those attributes might have greater overall impact than for attributes
that are more unique to a given condition.
C. Stakeholder Engagement
Feedback from decisionmakers and stakeholders from both the UK NICE experience 20 and
the much smaller Agency for Healthcare Research and Quality (AHRQ) pilot of the use of VOI
performed by the Duke Evidence-based Practice Center14 was generally positive, but several
consistent themes were noted (many of these were also noted in a review of the use of
modeling in systematic reviews conducted by the University of Minnesota for AHRQ) :21
• Lack of familiarity with the methodology: The majority of stakeholders are not familiar
with decision modeling, Bayesian techniques, or VOI. This is particularly true in the U.S.
setting. To the extent that analysts are able to provide appropriate background materials,
this can be somewhat ameliorated, but this requires additional time and effort on the part
of the analysis team. Ultimately, if VOI is to be part of the prioritization process, methods

16
for providing basic training in the principles of VOI are required; in the context of PCORI,
special efforts may be needed for patient representatives, particularly if these come from
outside the advocacy/policy community.
• Timing of VOI: One of the Duke pilot projects involved stakeholders who had recently
participated in a consensus-based approach to research prioritization. Although all of the
stakeholders felt the VOI results were helpful, they were evenly divided on whether the
VOI results would have been more helpful as background prior to beginning the
consensus process, or as something to be integrated into the consensus approach as
part of an iterative process.
In the setting of a research sponsor such as PCORI, VOI could be performed prior to
a solicitation for research proposals, with the solicitation specifically requesting
proposals only in those areas identified as having acceptable EVPI/EVPPI. Alternatively,
VOI could be performed after an initial review of proposals as part of the funding
decision, with proposals with higher EVPI/EVPPIs receiving higher priority for funding. In
either case, the sponsor would need to specify specific areas of research interest that
could be incorporated into a model for VOI. Another possibility would be to encourage,
or even require, investigators to include a VOI analysis as part of the rationale for their
proposals.
D. Heterogeneity and Equity
VOI has typically been performed using a population-level perspective. However,
differences between individuals or subgroups in the probability of different outcomes, or in
preferences for different outcomes, can have substantial effects on VOI results.
• Heterogeneity in probability of outcomes: Different subgroups may have different results
based on the probability of different outcomes. For example, in one of the Duke pilot
studies, the individual EVPI for further research in non-hysterectomy treatment for

17
uterine fibroids was somewhat higher for African-American women than for white
women, because of a higher incidence of fibroids at younger ages.14 Because the overall
incidence is so much higher in African-American women, this does not substantially
affect the relative population-level EVPIs; however, for conditions with less striking
disparities, or for conditions affecting a smaller subgroup, it is possible that population
EVPIs would be lower. This issue is especially important if population-level EVPIs are
used to prioritize research across different conditions or diseases—rare conditions would
inevitably rank lower, raising issues of how to balance overall burden of disease, the
potential population benefits of reducing uncertainty for a particular condition, and equity.
• Heterogeneity in patient preferences for outcomes: There may be variation between
subgroups in the distribution of patient preferences for different outcomes. For example,
the relative importance of quality of life and survival may vary between individual cancer
patients,22 and the “average” optimal choice may be suboptimal for a substantial
proportion of patients.23 Again, equity considerations need to be balanced with the
absolute size of the relevant subgroup and the magnitude of preference differences
when using population-level EVPI for research prioritization. On the other hand, the
basic approach behind estimating VOI can be helpful in identifying the value of
considering patient preferences, through estimation of the expected value of
individualized care (EVIC),24 which calculates the value of “research” into elicitation of
individual patient preferences; for example, Basu and Meltzer found a very high value for
eliciting individual patient preferences prior to treatment for prostate cancer in 65 year
old men compared to treatment based on population-level preference data.24
• Heterogeneity in patient preferences for other attributes of care: Variability in
preferences for other attributes of care beyond outcomes is also important, but has not
been systematically incorporated into VOI. If preferences for these attributes affect

18
behavior, these can be incorporated into models as probability parameters—for
example, as mentioned above, the potential effect of different attributes of screening
tests on adherence to colorectal cancer screening had the largest EVPPI of any
parameter in a recent cost-effectiveness/VOI analysis.25 However, other attributes are
not readily captured within QALY framework; many women have very strong preferences
for the labor and delivery process, but converting these preferences into utilities based
on elicitation via standard gamble or time trade-off has questionable face validity.
Alternative approaches, such as discrete choice experiments,26-28 may be a useful
alternative for capturing patient values for a range of relevant attributes.
E. Effect of Resolving Uncertainty on Patient and Provider Choices
A fundamental assumption underlying VOI is that research resolving uncertainty will lead to
improved clinical decisionmaking. However, recent experience in the US suggests that new
evidence is often met with substantial resistance from both patients and providers,29-31
especially for treatments that have already been incorporated into practice. The VOI approach
can be extended to incorporate the relative value of interventions to increase adherence to
evidence-based practice (the expected value of implementation;10,32,33 such an analysis might
suggest that research into methods for improving adherence should have a higher priority than
research into clinical effectiveness; such research may or may not be part of PCORI’s research
portfolio, but knowing that improved implementation is more important than improved certainty
about effectiveness is useful in either case.
These general challenges to the use of VOI are faced by any organization seeking to utilize
the method for research prioritization.2 However, there are some unique challenges to PCORI,
especially related to how to use VOI when decision making based on an explicit cost-
effectiveness threshold is not currently an option.
19
V. Specific Challenges to the Use of VOI by PCORI
Patient-centered outcomes research is defined by PCORI as research that:
• Assesses the benefits and harms of preventive, diagnostic, therapeutic, or health
delivery system interventions to inform decisionmaking, highlighting comparisons and
outcomes that matter to people;
• Is inclusive of an individual’s preferences, autonomy and needs, focusing on outcomes
that people notice and care about such as survival, function, symptoms, and health-
related quality of life;
• Incorporates a wide variety of settings and diversity of participants to address individual
differences and barriers to implementation and dissemination; and
• Investigates (or may investigate) optimizing outcomes while addressing burden to
individuals, resources, and other stakeholder perspectives.34
VOI can certainly address all of these areas, although the last is the one where there has
been the greatest experience. Although the final research agenda and evaluation criteria for
PCORI have not yet been published, preliminary indications are that specific disease areas will
not be targeted; instead, the research portfolio will be divided between five broad themes—
clinical effectiveness, improving health systems, communication and dissemination,
fairness/addressing disparities, and accelerating patient-centered research.35 VOI can be used
to inform research priorities for the first four areas, and, to the extent that greater use of VOI
might lead to the development of a more efficient research process, investment in VOI
resources can potentially contribute to the fifth as well.
Table 5 shows proposed prioritization/review criteria for research for PCORI, and specific
ways in which VOI could potentially be used to help evaluate each domain.

20
Table 5. Potential Use of VOI in Proposed PCORI Evaluation Criteria
PCORI Evaluation Criteria Potential Use of VOI
Impact on health of individuals and populations
Population EVPI allows comparison across conditions. Population EVPPI allows comparison of specific components of uncertainty within a condition/intervention
Probability of improvability via research EVPPI can estimate relative impact of different parameters; feasibility of research requires additional judgments
Inclusiveness of different sub-populations
Effect of differences in sub-populations can be explicitly modeled.
Current gaps in knowledge/variations in care
VOI explicitly addresses the relative importance of different gaps in knowledge, and can be extended to incorporate variation in care.
Impact on health system performance Depending on definition, “health system performance” can be incorporated into VOI
Current health disparities Effect of reducing existing disparities can be explicitly modeled
Potential to influence decision-making at the point of care
VOI explicitly considers impact of reducing uncertainty in specific parameters affecting decisions; usefulness depends on extent to which this uncertainty actually drives decision-making
Responsiveness to expressed needs N/A
Fits PCORI definition N/A
Novel use of technology N/A
Efficient use of research resources VOI explicitly compares relative value of different research areas, allowing resources to be directed to areas of greatest impact
Abbreviations: EVPI = expected value of perfect information; EVPPI = expected value of partial perfect information; N/A = not applicable; PCORI = Patient-Centered Outcome Research Institute; VOI = value of information
VOI has the potential to be a useful tool for PCORI in developing a research agenda.
However, in addition to the general issues related to VOI identified in Section III above, the
current ambiguity about how cost-effectiveness research and the use of quality-adjusted life
expectancy as an outcome fit within PCORI’s research portfolio36-38 suggests that alternative
approaches may need to be considered, or used alongside the “classic” approach. Although this
is not an insurmountable challenge, and may have some advantages compared to “classic” VOI,
the lack of a monetized decision threshold makes it almost impossible to directly translate VOI
findings into a research budget—decisionmakers will need to incorporate other criteria besides
the quantitative rankings from alternative VOI approaches in making funding decisions.
Although this would be true with monetized VOI results as well, the lack of a specific relationship
between the value of the research and the research budget makes the process somewhat more

21
difficult (of course, since VOI results are not currently used, this would not represent a change
from the status quo).
Ultimately, the underlying purpose of VOI for health care is to help decide whether further
research will increase the likelihood of a given stakeholder making an optimal decision, given
his or her preferences for the inevitable trade-offs between clinical benefits and harms, and
economic costs. Incremental costs per QALY or NMB are simply methods for summarizing
these trade-offs. In principle, alternative summary measures can be used. Options for the use of
VOI outside of a cost-effectiveness framework include:
• Using cost-benefit analysis: There are a variety of alternative approaches to valuing
preferences for non-market goods such as health care, including stated preference
methods such as contingent valuation and discrete choice experiments (where
questionnaires are used to elicit preferences for different states or attributes), and
revealed preference (where preferences are inferred from observed data such as the
time and costs associated with travel).39 Such approaches are commonly used in the
economic evaluation of environmental and safety regulation, and could potentially be
applied to the health care setting.40 Individual- or subgroup-level variations in the
distribution of preferences can be incorporated into models. Another advantage of this
approach is that using data from certain stated preference methods such as discrete
choice would greatly facilitate incorporating preferences for different nonclinical
attributes of a choice (e.g., surgical versus nonsurgical management when “hard”
outcomes are similar) into the model, especially compared to QALYs.26,27 The basic
approach to estimating EVPI and EVPPI would be similar.41 Finally, because the
principles and language of cost-benefit analysis are familiar to policymakers from their
use in other settings that affect health, a cost-benefit framework may facilitate
communication of the results of VOI in some settings.

22
• Using “harm-benefit ratios” or multiple other criteria: If costs are not to be considered at
all, a VOI approach could still be used. For example, the incidence of specific harms
could be considered as “costs” in the numerator, with clinical benefits in the
denominator; specific weights could be used for different harms and benefits. The effect
of uncertainty of different parameters on the “optimal” outcome could still be quantified
and used to help with decisions, as long as decision makers are willing to specify an
acceptable threshold. Figure 3 illustrates this using the hypothetical example from
Section I. The first panel (A) is a cost-effectiveness acceptability curve, where the Y-axis
represents the proportion of simulations where a given option had the highest NMB, and
the Y-axis represents a WTP threshold. In the second panel (B), the analysis was
conducted using total complication incidence as the numerator and life expectancy as
the denominator, while the third panel (C) uses fatal complication incidence as the
denominator.
A.

23
B.
C.
Figure 3. Acceptability curves for (a) cost per life-year saved, (b) total complications per life year
saved, and (c) fatal complications/life-year saved from the example given in Section I. Graphs
show the percentage of simulations where Treatment A (squares) or B (triangles) was optimal at a
given threshold for WTP for an extra year of life-saved in terms of costs, complications, or fatal
complications.
There have been a variety of methods proposed as alternatives to cost-effectiveness for
quantifying the joint distribution of benefits and harms,42-47 some of which include probabilistic
analyses, but we did not identify any examples where the results of these methods were used to

24
help with research prioritization. Challenges to this approach include the need for
decisionmakers to explicitly identify thresholds for the trade-offs, as well as the difficulty in
translating these results into a research budget; however, costs—whether from a societal,
payer, or patient perspective—could readily be incorporated. This approach might be
particularly helpful in quantifying uncertainty and identifying research priorities in the setting of
evidence-based guidelines or recommendations where costs are not explicitly considered, such
as those by the U.S. Preventive Services Task Force (USPSTF). Models are increasingly used
to help inform the recommendations; using VOI to quantify uncertainty might be especially
helpful when the optimal trade-offs between benefits and harms is not clear, or when a
surrogate for harm (such as unnecessary invasive diagnostic procedures)48,49 is used. Multi-
criteria decision analysis (MCDA), another method borrowed from environmental
policymaking,50,51 may have the most promise; there has been some pilot work with using
MCDA in a health care setting, but primarily in the context of coverage decisions42,47 or
individual decisionmaking;52 it should be possible to expand this approach to address research
prioritization.
These options are not mutually exclusive, and, indeed, a single VOI analysis could
potentially incorporate all of them—each approach is an attempt to improve decisionmaking by
clarifying the trade-offs involved in making a decision now compared to putting off the decision
and collecting more data. The inputs and outputs are similar across the various approaches,
with the main difference being the way that the individual components of the decision—harms,
benefits, and costs—are aggregated to facilitate decisionmaking. It is likely that, in many if not
most cases, the results will be quite similar no matter which approach is taken. In that case, the
best approach is probably the one that is easiest to communicate to decisionmakers,
researchers, and patients.

25
VI. Recommendations
We believe that VOI has significant potential as a tool for research prioritization by PCORI,
despite both the general challenges to its application and the challenges specific to its use by
PCORI described in this paper. Addressing these challenges is certainly feasible, but will
require investment of resources. We suggest the following initial steps by PCORI:
A. Formal Discussions/Conference with Other Policymakers
The ultimate success of VOI as a tool will require a critical mass of both methodologists able
to perform VOI, and policy makers comfortable enough with the approach to be able to use the
results of VOI. Whether and when this critical mass develops will be driven by the extent to
which VOI is adopted by research sponsors. PCORI should engage with other research
sponsors with experience with VOI (particularly NICE). We are aware of ongoing pilot work to
incorporate VOI into prioritization by one of the cooperative trials groups sponsored by the
National Cancer Institute (NCI),53 and of active interest on the part of the National Heart, Lung,
and Blood Institute (NHLBI).54,55 Development of a common research agenda and
implementation plan by major sponsors would both increase overall efficiency and help
accelerate development of the necessary infrastructure to fully utilize VOI.
B. “Comparative Effectiveness”/Proof of Principle of VOI
In order to justify the investment in developing this infrastructure, it would be helpful to have
better evidence that the use of VOI will ultimately lead to more efficient use of research
resources. As noted above, there is no evidence that VOI has actually been used to make
decisions about research funding. One way to make a more compelling case for greater use of
VOI would be to directly compare the results of prioritization based on VOI to current practice.
Our search identified one such “forensic” analysis, which compared the estimated VOI of a
completed trial based on information available at the time of study design to the actual cost of
26
the trial and concluded that the investment was worthwhile;56 the NHLBI Working Group on VOI
has suggested similar analyses.54 However, VOI is designed to help with decisions
prospectively—retrospective analysis of a single study may provide some insight into whether
the decision to fund that study was appropriate from a VOI perspective, but it does not provide
any useful information about whether funding that study was appropriate compared to the other
alternatives available at the time.
A more informative analysis would be to use VOI to evaluate the choices made in resource
allocation. Possible designs include:
• Within a single study, compare funded sample size to optimal sample size based on
expected value of sample information.
• Using a completed request for applications/proposals for a condition where there is an
existing model which can be adapted for VOI (and with appropriate protections for
confidentiality and the peer review process), compare rankings of the proposals based
on VOI to both the final peer review scoring for “significance” and to the ultimate funding
decision by the sponsor.
• Alternatively, the above-described comparison could be performed prospectively, in
parallel with an ongoing review.
C. Developing a Specific Strategy for VOI
The first two steps will help PCORI decide whether the investment required to optimally
incorporate VOI into its research prioritization is worthwhile. Once this decision is made, a more
detailed strategy for developing VOI capacity can be formulated. This would include decisions
about appropriate decision criteria, the timing of VOI relative to evaluation of research
proposals, and the nature of the infrastructure to support VOI for PCORI.

27
D. Parallel Development/Evaluation of VOI and Value of
Implementation
Finally, as discussed above, scientific uncertainty alone is not the sole (or, in many cases,
the major) contributor to variability in practice, inefficiency, or excess costs. Investment in
research that does not result in practice change is ultimately not the best use of resources, no
matter how high the EVPI. Any use of VOI by PCORI needs to include a “value of
implementation” component so that, when appropriate, research resources are directed towards
understanding and overcoming barriers to the use of evidence by patients and providers prior to
obtaining the evidence itself.

28
References
1. Chilcott J, Brennan A, Booth A, et al. The role of modelling in prioritising and planning
clinical trials. Health Technol Assess 2003;7(23):iii, 1-125. PMID: 14499052.
2. Claxton K, Cohen JT, Neumann PJ. When is evidence sufficient? Health Aff (Millwood)
2005;24(1):93-101. PMID: 15647219.
3. Eckermann S, Willan AR. Expected value of information and decision making in HTA.
Health Econ 2007;16(2):195-209. PMID: 16981193.
4. Fleurence RL. Setting priorities for research: a practical application of 'payback' and
expected value of information. Health Econ 2007;16(12):1345-57. PMID: 17328053.
5. Groot Koerkamp B, Weinstein MC, Stijnen T, et al. Uncertainty and patient heterogeneity
in medical decision models. Med Decis Making 2010;30(2):194-205. PMID: 20190188.
6. Claxton K, Thompson KM. A dynamic programming approach to the efficient design of
clinical trials. J Health Econ 2001;20(5):797-822. PMID: 11558649.
7. Eckermann S, Karnon J, Willan AR. The value of value of information: best informing
research design and prioritization using current methods. Pharmacoeconomics
2010;28(9):699-709. PMID: 20629473.
8. Eckermann S, Willan AR. Globally optimal trial design for local decision making. Health
Econ 2009;18(2):203-16. PMID: 18435429.
9. Willan AR. Optimal sample size determinations from an industry perspective based on
the expected value of information. Clin Trials 2008;5(6):587-94. PMID: 19029207.
10. Willan AR, Eckermann S. Optimal clinical trial design using value of information methods
with imperfect implementation. Health Econ 2010;19(5):549-61. PMID: 19399753.
11. Willan AR, Pinto EM. The value of information and optimal clinical trial design. Stat Med
2005;24(12):1791-806. PMID: 15806619.
29
12. Ades AE, Lu G, Claxton K. Expected value of sample information calculations in medical
decision modeling. Med Decis Making 2004;24(2):207-27. PMID: 15090106.
13. McKenna C, Claxton K. Addressing adoption and research design decisions
simultaneously: the role of value of sample information analysis. Med Decis Making
2011;31(6):853-65. PMID: 21393558.
14. Myers E, Sanders GD, Ravi D, et al. Evaluating the Potential Use of Modeling and
Value-of-Information Analysis for Future Research Prioritization Within the Evidence-
based Practice Center Program. (Prepared by the Duke Evidence-based Practice Center
under Contract No. 290-2007-10066-I.) AHRQ Publication No. 11-EHC030-EF.
Rockville, MD: Agency for Healthcare Research and Quality; June 2011. Available at:
www.effectivehealthcare.ahrq.gov/reports/final.cfm. Accessed January 9, 2012. PMID:
21977527.
15. Meltzer DO, Hoomans T, Chung JW, et al. Minimal modeling approaches to value of
information analysis for health research. Med Decis Making 2011;31(6):E1-E22. PMID:
21712493.
16. Fung MF, Bryson P, Johnston M, et al. Screening postmenopausal women for ovarian
cancer: a systematic review. J Obstet Gynaecol Can 2004;26(8):717-28. PMID:
15307976.
17. Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer mortality: the
Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized
Controlled Trial. JAMA 2011;305(22):2295-303. PMID: 21642681.
18. Havrilesky LJ, Sanders GD, Kulasingam S, et al. Development of an ovarian cancer
screening decision model that incorporates disease heterogeneity: implications for
potential mortality reduction. Cancer 2011;117(3):545-53. PMID: 21254049.

30
19. Havrilesky LJ, Sanders GD, Kulasingam S, et al. Reducing ovarian cancer mortality
through screening: Is it possible, and can we afford it? Gynecol Oncol 2008;111(2):179-
87. PMID: 18722004.
20. Claxton KP, Sculpher MJ. Using value of information analysis to prioritise health
research: some lessons from recent UK experience. Pharmacoeconomics
2006;24(11):1055-68. PMID: 17067191.
21. Kunz K, Sainfort F, Butler M, et al. Decision and simulation modeling in systematic
reviews [draft]. Prepared by the Minnesota Evidence-based Practice Center under
Contract HHSA 290 2007 10064-I. Rockville, MD: Agency for Healthcare Research and
Quality; 2010.
22. Thrumurthy SG, Morris JJ, Mughal MM, et al. Discrete-choice preference comparison
between patients and doctors for the surgical management of oesophagogastric cancer.
Br J Surg 2011;98(8):1124-31; discussion 1132. PMID: 21674471.
23. Sommers BD, Beard CJ, D'Amico AV, et al. Decision analysis using individual patient
preferences to determine optimal treatment for localized prostate cancer. Cancer
2007;110(10):2210-7. PMID: 17893907.
24. Basu A, Meltzer D. Value of information on preference heterogeneity and individualized
care. Med Decis Making 2007;27(2):112-27. PMID: 17409362.
25. Hassan C, Hunink MG, Laghi A, et al. Value-of-Information Analysis to Guide Future
Research in Colorectal Cancer Screening. Radiology 2009;253(3):745-52. PMID:
19789242.
26. Scotland GS, McNamee P, Cheyne H, et al. Women's preferences for aspects of labor
management: results from a discrete choice experiment. Birth 2011;38(1):36-46. PMID:
21332773.
31
27. Petrou S, McIntosh E. Women's preferences for attributes of first-trimester miscarriage
management: a stated preference discrete-choice experiment. Value Health
2009;12(4):551-9. PMID: 18798807.
28. Ryan M, Gerard K, Amaya-Amaya M. (editors). Using discrete choice experiments to
value health and health care. Dordrecht, the Netherlands: Springer; 2010.
29. Wulff KC, Miller FG, Pearson SD. Can coverage be rescinded when negative trial results
threaten a popular procedure? The ongoing saga of vertebroplasty. Health Aff (Millwood)
2011;30(12):2269-76. PMID: 22147854.
30. Mortimer D, Li JJ, Watts J, et al. Breaking up is hard to do: the economic impact of
provisional funding contingent upon evidence development. Health Economics, Policy, &
Law 2011;6(4):509-27. PMID: 21819632.
31. Couzin-Frankel J, Ogale Y. FDA. Once on 'fast track,' avastin now derailed. Science
2011;333(6039):143-4. PMID: 21737712.
32. Fenwick E, Claxton K, Sculpher M. The value of implementation and the value of
information: combined and uneven development. Med Decis Making 2008;28(1):21-32.
PMID: 18263559.
33. Hoomans T, Fenwick EA, Palmer S, et al. Value of Information and Value of
Implementation: Application of an Analytic Framework to Inform Resource Allocation
Decisions in Metastatic Hormone-Refractory Prostate Cancer. Value in Health
2009;12(2):315-24. PMID: 18657098.
34. Patient-Centered Outcomes Research Institute. Patient-Centered Outcomes Research.
Available at: www.pcori.org/patient-centered-outcomes-research. Accessed January 9,
2012.

32
35. Selby JV. Update from Patient-Centered Outcomes Research Institute (PCORI).
Presented at Evidence-based Practice Center Director’s Meeting, Rockville, MD,
November 17, 2011.
36. Dentzer S. The researcher-in-chief at the patient-centered outcomes research institute.
Health Aff (Millwood) 2011;30(12):2252-8. PMID: 22147852.
37. Garber AM. How the patient-centered outcomes research institute can best influence
real-world health care decision making. Health Aff (Millwood) 2011;30(12):2243-51.
PMID: 22147851.
38. Garber AM, Sox HC. The role of costs in comparative effectiveness research. Health Aff
(Millwood) 2010;29(10):1805-11. PMID: 20921479.
39. Whitehead J, Haab T, Huang JC, eds. Preference Data for Environmental Valuation:
Combining Revealed and Stated Approaches. New York: Routledge; 2011.
40. Johnson FR, Adamowicz WL. Valuation and cost-benefit analysis in health and
environmental economics. In: McIntosh E, Clarke PM, Frew EJ, et al., eds. Applied
Methods of Cost-benefit Analysis in Health Care. NY: Oxford University Press; 2010: 79-
96.
41. McIntosh E. Using discrete choice experiments within a cost-benefit analysis framework:
some considerations. Pharmacoeconomics 2006;24(9):855-68. PMID: 16942121.
42. Goetghebeur MM, Wagner M, Khoury H, et al. Bridging Health Technology Assessment
(HTA) and Efficient Health Care Decision Making with Multicriteria Decision Analysis
(MCDA): Applying the EVIDEM Framework to Medicines Appraisal. Med Decis Making
2011. PMID: 21987539.
43. Tervonen T, van Valkenhoef G, Buskens E, et al. A stochastic multicriteria model for
evidence-based decision making in drug benefit-risk analysis. Stat Med
2011;30(12):1419-28. PMID: 21268053.

33
44. Guo JJ, Pandey S, Doyle J, et al. A review of quantitative risk-benefit methodologies for
assessing drug safety and efficacy-report of the ISPOR risk-benefit management
working group. Value Health 2010;13(5):657-66. PMID: 20412543.
45. Felli JC, Noel RA, Cavazzoni PA. A multiattribute model for evaluating the benefit-risk
profiles of treatment alternatives. Med Decis Making 2009;29(1):104-15. PMID:
18812582.
46. Towse A. Net clinical benefit: the art and science of jointly estimating benefits and risks
of medical treatment. Value Health 2010;13 Suppl 1:S30-2. PMID: 20618793.
47. Tony M, Wagner M, Khoury H, et al. Bridging health technology assessment (HTA) with
multicriteria decision analyses (MCDA): field testing of the EVIDEM framework for
coverage decisions by a public payer in Canada. BMC Health Serv Res 2011;11:329.
PMID: 22129247.
48. Zauber AG, Lansdorp-Vogelaar I, Knudsen AB, et al. Evaluating Test Strategies for
Colorectal Cancer Screening—Age to Begin, Age to Stop, and Timing of Screening
Intervals: A Decision Analysis of Colorectal Cancer Screening for the U.S. Preventive
Services Task Force from the Cancer Intervention and Surveillance Modeling Network
(CISNET). Evidence Synthesis No. 65, Part 2. AHRQ Publication No. 08-05124-EF-2.
Rockville, MD: Agency for Healthcare Research and Quality; March 2009. Available at:
www.ncbi.nlm.nih.gov/books/NBK34013. Accessed January 9, 2012. PMID: 20722163.
49. Kulasingam SL, Havrilesky L, Ghebre R, et al. Kulasingam SL, Havrilesky L, Ghebre R,
Myers ER. Screening for Cervical Cancer: A Decision Analysis for the U.S. Preventive
Services Task Force. AHRQ Publication No. 11-05157-EF-1. Rockville, MD: Agency for
Healthcare Research and Quality; May 2011. Available at:
www.uspreventiveservicestaskforce.org/uspstf11/cervcancer/cervcancerdecan.pdf.
Accessed January 9, 2012.

34
50. Linkov I, Welle P, Loney D, et al. Use of multicriteria decision analysis to support weight
of evidence evaluation. Risk Anal 2011;31(8):1211-25. PMID: 21371061.
51. Kiker GA, Bridges TS, Varghese A, et al. Application of multicriteria decision analysis in
environmental decision making. Integr Environ Assess Manag 2005;1(2):95-108. PMID:
16639891.
52. Cunich M, Salkeld G, Dowie J, et al. Integrating evidence and individual preferences
using a web-based multi-criteria decision analytic tool: an application to prostate cancer
screening. Patient 2011;4(3):153-62. PMID: 21766911.
53. Schmidt C. Researchers consider value-of-information theory for selecting trials. J Natl
Cancer Inst 2010;102(3):144-6. PMID: 20107161.
54. NHLBI Working Group on Value of Information Modeling. Executive Summary of
Working Group Teleconferences Held on December 7th and 17th, 2010. Available at:
http://www.nhlbi.nih.gov/meetings/workshops/info-modeling.htm. Accessed January 9,
2012.
55. National Heart Lung and Blood Institute (NHLBI). Request for Information (RFI) on Value
of Information (VOI) Research. January 6, 2012. Available at:
http://grants.nih.gov/grants/guide/notice-files/NOT-HL-12-002.html. Accessed January 9,
2012.
56. Ramsey SD, Blough DK, Sullivan SD. A forensic evaluation of the National Emphysema
Treatment Trial using the expected value of information approach. Med Care
2008;46(5):542-8. PMID: 18438203.
35
Abbreviations
AHRQ Agency for Healthcare Research and Quality
EVIC expected value of individualized care
EVPI expected value of perfect information
EVPPI expected value of partial perfect information
HTA Health Technology Assessment
MCDA multi-criteria decision analysis
NCI National Cancer Institute
NHB net health benefit
NHLBI National Heart, Lung, and Blood Institute
NICE National Institute for Health and Clinical Excellence
NIH National Institutes of Health
NMB net monetary benefit
PCORI Patient-Centered Outcomes Research Institute
PSA probabilistic sensitivity analysis
QALY quality-adjusted life year
USPSTF U.S. Preventive Services Task Force
VOI value-of-information analysis
WTP willingness-to-pay

36
Appendix A. Literature Search and Screening Results
PubMed® Search Strategy
Search date: November 3, 2011 Exact search string:
(("value of information"[ALL] OR "Value of Additional Information"[ALL] OR "Value of
Information Analysis"[ALL] OR "Expected Value of Perfect Information"[ALL] OR
"EVPI"[ALL] OR "EVPPI"[ALL] OR "Expected Value of Partial Perfect Information"[ALL] OR
"Bayesian Approach to Uncertainty"[ALL] OR "Value of Research"[ALL])) AND (("Decision
Making"[MH] OR "Decision Theory"[MH]) OR ("Research"[MH] OR "Health Services
Research"[MH]) OR research[TIAB])
Set # Terms # of Results
#1 Search (("value of information"[ALL] OR "Value of Additional Information"[ALL] OR "Value of Information Analysis"[ALL] OR "Expected Value of Perfect Information"[ALL] OR "EVPI"[ALL] OR "EVPPI"[ALL] OR "Expected Value of Partial Perfect Information"[ALL] OR "Bayesian Approach to Uncertainty"[ALL] OR "Value of Research"[ALL]))
337
#2 Search (("Decision Making"[MH] OR "Decision Theory"[MH]) OR ("Research"[MH] OR "Health Services Research"[MH]) OR research[TIAB])
1078887
#3 Search #1 AND #2 177
Literature Screening Results
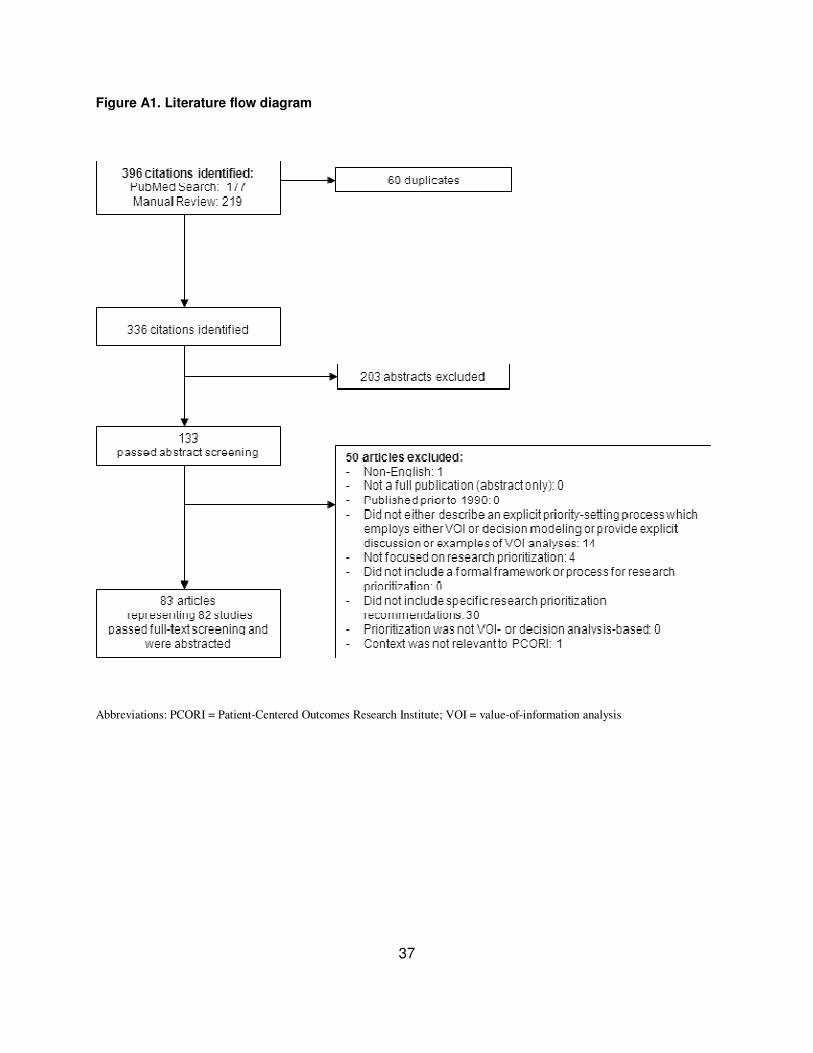
Figure A1 summarizes the results of our literature search and screening.
37
Figure A1. Literature flow diagram
Abbreviations: PCORI = Patient-Centered Outcomes Research Institute; VOI = value-of-information analysis

38
List of Included Studies
Ades AE, Lu G, Claxton K. Expected value of
sample information calculations in medical
decision modeling. Med Decis Making
2004;24(2):207-27. PMID: 15090106.
Attema AE, Lugner AK, Feenstra TL. Investment in antiviral drugs: a real options
approach. Health Econ 2010;19(10):1240-54.
PMID: 19816857.
Bansback N, Ara R, Ward S, et al. Statin therapy
in rheumatoid arthritis: a cost-effectiveness and
value-of-information analysis.
Pharmacoeconomics 2009;27(1):25-37. PMID:
19178122.
Basu A, Meltzer D. Value of information on
preference heterogeneity and individualized care.
Med Decis Making 2007;27(2):112-27. PMID: 17409362.
Bojke L, Claxton K, Sculpher MJ, et al.
Identifying research priorities: the value of
information associated with repeat screening for
age-related macular degeneration. Med Decis
Making 2008;28(1):33-43. PMID: 18263560.
Bojke L, Hornby E, Sculpher M. A comparison
of the cost effectiveness of pharmacotherapy or
surgery (laparoscopic fundoplication) in the
treatment of GORD. Pharmacoeconomics
2007;25(10):829-41. PMID: 17887805.
Brush J, Boyd K, Chappell F, et al. The value of FDG positron emission
tomography/computerised tomography
(PET/CT) in pre-operative staging of colorectal
cancer: a systematic review and economic
evaluation. Health Technol Assess
2011;15(35):1-192. PMID: 21958472.
Castelnuovo E, Thompson-Coon J, Pitt M, et al.
The cost-effectiveness of testing for hepatitis C
in former injecting drug users. Health Technol
Assess 2006;10(32):iii-iv, ix-xii, 1-93. PMID:
16948891.
Cher DJ, Maclure M. Use of randomized
controlled trials in organizational decision
making: a cost-minimization approach. Am J
Manag Care 2000;6(8):894-904. PMID:
11186501.
Chilcott J, Brennan A, Booth A, et al. The role of
modelling in prioritising and planning clinical
trials. Health Technol Assess 2003;7(23):iii, 1-
125. PMID: 14499052.
Claxton K, Ginnelly L, Sculpher M, et al. A pilot
study on the use of decision theory and value of
information analysis as part of the NHS Health Technology Assessment programme. Health
Technol Assess 2004;8(31):1-103, iii. PMID:
15248937.
Claxton K, Neumann PJ, Araki S, et al. Bayesian
value-of-information analysis. An application to
a policy model of Alzheimer's disease. Int J
Technol Assess Health Care 2001;17(1):38-55.
PMID: 11329844.
Claxton KP, Sculpher MJ. Using value of
information analysis to prioritise health research:
some lessons from recent UK experience. Pharmacoeconomics 2006;24(11):1055-68.
PMID: 17067191.
Colbourn T, Asseburg C, Bojke L, et al. Prenatal
screening and treatment strategies to prevent
group B streptococcal and other bacterial
infections in early infancy: cost-effectiveness
and expected value of information analyses.
Health Technol Assess 2007;11(29):1-226, iii.
PMID: 17651659.
Colbourn TE, Asseburg C, Bojke L, et al.
Preventive strategies for group B streptococcal
and other bacterial infections in early infancy: cost effectiveness and value of information
analyses. BMJ 2007;335(7621):655. PMID:
17848402.
Collins R, Fenwick E, Trowman R, et al. A
systematic review and economic model of the
clinical effectiveness and cost-effectiveness of
docetaxel in combination with prednisone or
prednisolone for the treatment of hormone-
refractory metastatic prostate cancer. Health
Technol Assess 2007;11(2):iii-iv, xv-xviii, 1-
179. PMID: 17181985.
Dong H, Coyle D, Buxton M. Value of
information analysis for a new technology:
computer-assisted total knee replacement. Int J
Technol Assess Health Care 2007;23(3):337-42.
PMID: 17579936.
Eckermann S, Willan AR. Globally optimal trial
design for local decision making. Health Econ
2009;18(2):203-16. PMID: 18435429.

39
Felli JC, Hazen GB. Sensitivity analysis and the
expected value of perfect information. Med
Decis Making 1998;18(1):95-109. PMID:
9456214.
Fenwick E, Marshall DA, Blackhouse G, et al.
Assessing the impact of censoring of costs and effects on health-care decision-making: an
example using the Atrial Fibrillation Follow-up
Investigation of Rhythm Management
(AFFIRM) study. Value Health 2008;11(3):365-
75. PMID: 17854433.
Fenwick E, Palmer S, Claxton K, et al. An
iterative Bayesian approach to health technology
assessment: application to a policy of
preoperative optimization for patients
undergoing major elective surgery. Med Decis
Making 2006;26(5):480-96. PMID: 16997926.
Fleurence RL. Setting priorities for research: a practical application of 'payback' and expected
value of information. Health Econ
2007;16(12):1345-57. PMID: 17328053.
Fox M, Mealing S, Anderson R, et al. The
clinical effectiveness and cost-effectiveness of
cardiac resynchronisation (biventricular pacing)
for heart failure: systematic review and
economic model. Health Technol Assess
2007;11(47):iii-iv, ix-248. PMID: 17999842.
Galani C, Al M, Schneider H, et al. Uncertainty
in decision-making: value of additional information in the cost-effectiveness of lifestyle
intervention in overweight and obese people.
Value Health 2008;11(3):424-34. PMID:
18179675.
Garside R, Pitt M, Somerville M, et al.
Surveillance of Barrett's oesophagus: exploring
the uncertainty through systematic review, expert
workshop and economic modelling. Health
Technol Assess 2006;10(8):1-142, iii-iv. PMID:
16545207.
Ginnelly L, Claxton K, Sculpher MJ, et al. Using
value of information analysis to inform publicly funded research priorities. Appl Health Econ
Health Policy 2005;4(1):37-46. PMID:
16076237.
Girling AJ, Freeman G, Gordon JP, et al.
Modeling payback from research into the
efficacy of left-ventricular assist devices as
destination therapy. Int J Technol Assess Health
Care 2007;23(2):269-77. PMID: 17493314.
Griebsch I, Knowles RL, Brown J, et al.
Comparing the clinical and economic effects of
clinical examination, pulse oximetry, and
echocardiography in newborn screening for
congenital heart defects: a probabilistic cost-
effectiveness model and value of information
analysis. Int J Technol Assess Health Care 2007;23(2):192-204. PMID: 17493305.
Groot Koerkamp B, Nikken JJ, Oei EH, et al.
Value of information analysis used to determine
the necessity of additional research: MR imaging
in acute knee trauma as an example. Radiology
2008;246(2):420-5. PMID: 18227539.
Groot Koerkamp B, Weinstein MC, Stijnen T, et
al. Uncertainty and patient heterogeneity in
medical decision models. Med Decis Making
2010;30(2):194-205. PMID: 20190188.
Grutters JP, Joore MA, van der Horst F, et al.
Decision-Analytic Modeling to Assist Decision Making in Organizational Innovation: The Case
of Shared Care in Hearing Aid Provision. Health
Serv Res 2008. PMID: 18522663.
Grutters JP, Pijls-Johannesma M, Ruysscher DD,
et al. The cost-effectiveness of particle therapy in
non-small cell lung cancer: Exploring decision
uncertainty and areas for future research. Cancer
Treat Rev 2010;36(6):468-76. PMID: 20303217.
Hall PS, Hulme C, McCabe C, et al. Updated
cost-effectiveness analysis of trastuzumab for
early breast cancer: a UK perspective considering duration of benefit, long-term
toxicity and pattern of recurrence.
Pharmacoeconomics 2011;29(5):415-32. PMID:
21504241.
Harris J, Felix L, Miners A, et al. Adaptive e-
learning to improve dietary behaviour: a
systematic review and cost-effectiveness
analysis. Health Technol Assess 2011;15(37):1-
160. PMID: 22030014.
Hassan C, Benamouzig R, Spada C, et al. Cost
effectiveness and projected national impact of
colorectal cancer screening in France. Endoscopy 2011;43(9):780-93. PMID:
21623557.
Hassan C, Hunink MG, Laghi A, et al. Value-of-
Information Analysis to Guide Future Research
in Colorectal Cancer Screening. Radiology
2009;253(3):745-52. PMID: 19789242.
Hassan C, Pickhardt PJ, Di Giulio E, et al.
Value-of-information analysis to guide future
research in the management of the colorectal

40
malignant polyp. Dis Colon Rectum
2010;53(2):135-42. PMID: 20087087.
Henriksson M, Lundgren F, Carlsson P.
Informing the efficient use of health care and
health care research resources - the case of
screening for abdominal aortic aneurysm in Sweden. Health Econ 2006;15(12):1311-22.
PMID: 16786498.
Hewitt C, Gilbody S, Brealey S, et al. Methods
to identify postnatal depression in primary care:
an integrated evidence synthesis and value of
information analysis. Health Technol Assess
2009;13(36):1-145, 147-230. PMID: 19624978.
Hoomans T, Fenwick EA, Palmer S, et al. Value
of Information and Value of Implementation:
Application of an Analytic Framework to Inform
Resource Allocation Decisions in Metastatic
Hormone-Refractory Prostate Cancer. Value in Health 2009;12(2):315-24. PMID: 18657098.
Hornberger J. A cost-benefit analysis of a
cardiovascular disease prevention trial, using
folate supplementation as an example. Am J
Public Health 1998;88(1):61-7. PMID: 9584035.
Hornberger J, Eghtesady P. The cost-benefit of a
randomized trial to a health care organization.
Control Clin Trials 1998;19(2):198-211. PMID:
9551284.
Hunink MG. Decision making in the face of
uncertainty and resource constraints: examples from trauma imaging. Radiology
2005;235(2):375-83. PMID: 15858081.
Iglesias CP, Claxton K. Comprehensive
decision-analytic model and Bayesian value-of-
information analysis: pentoxifylline in the
treatment of chronic venous leg ulcers.
Pharmacoeconomics 2006;24(5):465-78. PMID:
16706572.
Karnon J. Planning the efficient allocation of
research funds: an adapted application of a non-
parametric Bayesian value of information
analysis. Health Policy 2002;61(3):329-47. PMID: 12098524.
Kee F, Erridge S, Bradbury I, et al. The value of
positron emission tomography in patients with
non-small cell lung cancer. Eur J Radiol
2010;73(1):50-8. PMID: 19084367.
Koerkamp BG, Spronk S, Stijnen T, et al. Value
of information analyses of economic randomized
controlled trials: the treatment of intermittent
claudication. Value Health 2010;13(2):242-50.
PMID: 19818058.
Leelahavarong P, Teerawattananon Y,
Werayingyong P, et al. Is a HIV vaccine a viable
option and at what price? An economic
evaluation of adding HIV vaccination into
existing prevention programs in Thailand. BMC Public Health 2011;11:534. PMID: 21729309.
Linkov I, Bates ME, Canis LJ, et al. A decision-
directed approach for prioritizing research into
the impact of nanomaterials on the environment
and human health. Nat Nanotechnol 2011.
PMID: 21963715.
Martikainen JA, Kivioja A, Hallinen T, et al.
Economic evaluation of temozolomide in the
treatment of recurrent glioblastoma multiforme.
Pharmacoeconomics 2005;23(8):803-15. PMID:
16097842.
McKenna C, Burch J, Suekarran S, et al. A systematic review and economic evaluation of
the clinical effectiveness and cost-effectiveness
of aldosterone antagonists for postmyocardial
infarction heart failure. Health Technol Assess
2010;14(24):1-162. PMID: 20492762.
McKenna C, McDaid C, Suekarran S, et al.
Enhanced external counterpulsation for the
treatment of stable angina and heart failure: a
systematic review and economic analysis. Health
Technol Assess 2009;13(24):iii-iv, ix-xi, 1-90.
PMID: 19409154.
Meltzer D, Basu A, Conti R. The economics of
comparative effectiveness studies: societal and
private perspectives and their implications for
prioritizing public investments in comparative
effectiveness research. Pharmacoeconomics
2010;28(10):843-53. PMID: 20831292.
Meltzer DO, Basu A, Meltzer HY. Comparative
effectiveness research for antipsychotic
medications: how much is enough? Health Aff
(Millwood) 2009;28(5):w794-808. PMID:
19622539.
Meltzer DO, Hoomans T, Chung JW, et al. Minimal Modeling Approaches to Value of
Information Analysis for Health Research.
Methods Future Research Needs Report No. 6
(Prepared by the University of Chicago Medical
Center and the Blue Cross and Blue Shield
Association Technology Evaluation Center
Evidence-Based Practice Center under Contract
No. 29007-10058.) AHRQ Publication No. 11-
EHC062-EF. Rockville, MD: Agency for
Healthcare Research and Quality; June 2011.

41
Available at:
www.effectivehealthcare.ahrq.gov/reports/final.c
fm. Accessed January 10, 2012. PMID:
21977528.
Meltzer DO, Hoomans T, Chung JW, et al.
Minimal modeling approaches to value of information analysis for health research. Med
Decis Making 2011;31(6):E1-E22. PMID:
21712493.
Mooney C, Mushlin AI, Phelps CE. Targeting
assessments of magnetic resonance imaging in
suspected multiple sclerosis. Med Decis Making
1990;10(2):77-94. PMID: 2112217.
Myers E, Sanders GD, Ravi D, et al. Evaluating
the Potential Use of Modeling and Value-of-
Information Analysis for Future Research
Prioritization Within the Evidence-based
Practice Center Program. (Prepared by the Duke Evidence-based Practice Center under Contract
No. 290-2007-10066-I.) AHRQ Publication No.
11-EHC030-EF. Rockville, MD: Agency for
Healthcare Research and Quality; June 2011.
Available at:
www.effectivehealthcare.ahrq.gov/reports/final.c
fm. Accessed January 9, 2012. PMID: 21977527.
Oostenbrink JB, Al MJ, Oppe M, et al. Expected
value of perfect information: an empirical
example of reducing decision uncertainty by
conducting additional research. Value in Health 2008;11(7):1070-80. PMID: 19602213.
Peck SC, Kavet R. Research strategies for
magnetic fields and cancer. Risk Anal
2005;25(1):179-88. PMID: 15787767.
Philips Z, Claxton KP, Palmer S, et al. Priority
setting for research in health care: an application
of value of information analysis to glycoprotein
IIb/Illa antagonists in non-ST elevation acute
coronary syndrome. Int J Technol Assess Health
Care 2006;22(3):379-87. PMID: 16984067.
Purmonen TT, Pankalainen E, Turunen JH, et al.
Short-course adjuvant trastuzumab therapy in early stage breast cancer in Finland: cost-
effectiveness and value of information analysis
based on the 5-year follow-up results of the
FinHer Trial. Acta Oncol 2011;50(3):344-52.
PMID: 21299447.
Ramsey SD, Blough DK, Sullivan SD. A
forensic evaluation of the National Emphysema
Treatment Trial using the expected value of
information approach. Med Care
2008;46(5):542-8. PMID: 18438203.
Rao C, Haycock A, Zacharakis E, et al.
Economic analysis of esophageal stenting for
management of malignant dysphagia. Dis
Esophagus 2009;22(4):337-47. PMID:
19207559.
Robinson M, Palmer S, Sculpher M, et al. Cost-effectiveness of alternative strategies for the
initial medical management of non-ST elevation
acute coronary syndrome: systematic review and
decision-analytical modelling. Health Technol
Assess 2005;9(27):iii-iv, ix-xi, 1-158. PMID:
16022802.
Rodgers M, McKenna C, Palmer S, et al.
Curative catheter ablation in atrial fibrillation
and typical atrial flutter: systematic review and
economic evaluation. Health Technol Assess
2008;12(34):iii-iv, xi-xiii, 1-198. PMID:
19036232.
Rogowski W, Burch J, Palmer S, et al. The effect
of different treatment durations of clopidogrel in
patients with non-ST-segment elevation acute
coronary syndromes: a systematic review and
value of information analysis. Health Technol
Assess 2009;13(31):iii-iv, ix-xi, 1-77. PMID:
19573471.
Rojnik K, Naversnik K. Gaussian process
metamodeling in Bayesian value of information
analysis: a case of the complex health economic
model for breast cancer screening. Value Health 2008;11(2):240-50. PMID: 18380636.
Singh S, Nosyk B, Sun H, et al. Value of
information of a clinical prediction rule:
informing the efficient use of healthcare and
health research resources. Int J Technol Assess
Health Care 2008;24(1):112-9. PMID:
18218176.
Smith KJ, Ness RB, Wiesenfeld HC, et al. Cost-
effectiveness of alternative outpatient pelvic
inflammatory disease treatment strategies. Sex
Transm Dis 2007;34(12):960-6. PMID:
18077847.
Smits M, Dippel DW, Nederkoorn PJ, et al.
Minor head injury: CT-based strategies for
management--a cost-effectiveness analysis.
Radiology 2010;254(2):532-40. PMID:
20093524.
Soeteman DI, Busschbach JJ, Verheul R, et al.
Cost-effective psychotherapy for personality
disorders in the Netherlands: the value of further
research and active implementation. Value
Health 2011;14(2):229-39. PMID: 21296601.

42
Soini EJ, Garcia San Andres B, Joensuu T.
Trabectedin in the treatment of metastatic soft
tissue sarcoma: cost-effectiveness, cost-utility
and value of information. Ann Oncol 2010.
PMID: 20627875.
Speight PM, Palmer S, Moles DR, et al. The cost-effectiveness of screening for oral cancer in
primary care. Health Technol Assess
2006;10(14):1-144, iii-iv. PMID: 16707071.
Stevenson MD, Scope A, Sutcliffe PA. The
Cost-Effectiveness of Group Cognitive
Behavioral Therapy Compared with Routine
Primary Care for Women with Postnatal
Depression in the UK. Value Health
2010;13(5):580-4. PMID: 20384978.
Stevenson MD, Scope A, Sutcliffe PA, et al.
Group cognitive behavioural therapy for
postnatal depression: a systematic review of clinical effectiveness, cost-effectiveness and
value of information analyses. Health Technol
Assess 2010;14(44):1-107, iii-iv. PMID:
20863477.
Tappenden P, Chilcott JB, Eggington S, et al.
Methods for expected value of information
analysis in complex health economic models:
developments on the health economics of
interferon-beta and glatiramer acetate for
multiple sclerosis. Health Technol Assess
2004;8(27):iii, 1-78. PMID: 15215017.
Torgerson D, Donaldson C, Reid D. Using
economics to prioritize research: a case study of
randomized trials for the prevention of hip
fractures due to osteoporosis. J Health Serv Res
Policy 1996;1(3):141-6. PMID: 10180860.
Townsend J, Buxton M, Harper G. Prioritisation of health technology assessment. The PATHS
model: methods and case studies. Health
Technol Assess 2003;7(20):iii, 1-82. PMID:
13678549.
Wailoo AJ, Sutton AJ, Cooper NJ, et al. Cost-
effectiveness and value of information analyses
of neuraminidase inhibitors for the treatment of
influenza. Value Health 2008;11(2):160-71.
PMID: 18380629.
Willan AR. Clinical decision making and the
expected value of information. Clin Trials
2007;4(3):279-85. PMID: 17715257.
Willan AR, Eckermann S. Optimal clinical trial
design using value of information methods with
imperfect implementation. Health Econ
2010;19(5):549-61. PMID: 19399753.
Wilson E, Gurusamy K, Gluud C, et al. Cost-
utility and value-of-information analysis of early
versus delayed laparoscopic cholecystectomy for
acute cholecystitis. Br J Surg 2010;97(2):210-9.
PMID: 20035545.

43
List of Excluded Studies
All studies listed below were reviewed in their full-text version and excluded. Following each
reference, in italics, is the reason for exclusion. Reasons for exclusion signify only the
usefulness of the articles for this study and are not intended as criticisms of the articles.
Back PE, Rosen L and Norberg T. Value of
information analysis in remedial investigations.
Ambio 2007:36(6);486-93. Full-text Exclude -
Context is not relevant to PCORI.
Baio G and Russo P. A decision-theoretic framework
for the application of cost-effectiveness analysis in
regulatory processes. Pharmacoeconomics
2009:27(8);645-55. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Barton GR, Briggs AH and Fenwick EA. Optimal
cost-effectiveness decisions: the role of the cost-
effectiveness acceptability curve (CEAC), the cost-
effectiveness acceptability frontier (CEAF), and the
expected value of perfection information (EVPI).
Value Health 2008:11(5);886-97. Full-text Exclude -
No specific research prioritization recommendations.
Barton P. What happens to value of information
measures as the number of decision options
increases? Health Econ 2011:20(7);853-63. Full-text
Exclude - No specific research prioritization
recommendations.
Bell DS. Decision-analytic valuation of clinical
information systems: application to an alerting
system for coronary angiography. Proc AMIA Annu Fall Symp 1997:173-7. Full-text Exclude - Not
focused on research prioritization.
Benini A and Conley C. Rapid humanitarian
assessments and rationality: a value-of-information
study from Iraq, 2003-04. Disasters 2007:31(1);29-
48. Full-text Exclude - Not focused on research
prioritization.
Black C, Clar C, Henderson R, et al. The clinical
effectiveness of glucosamine and chondroitin
supplements in slowing or arresting progression of
osteoarthritis of the knee: a systematic review and
economic evaluation. Health Technol Assess
2009:13(52);1-148. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Brennan A, Kharroubi S, O'hagan A, et al.
Calculating partial expected value of perfect
information via Monte Carlo sampling algorithms.
Med Decis Making 2007:27(4);448-70. Full-text
Exclude - No specific research prioritization
recommendations.
Chua B, Ung O, Taylor R, et al. Is information from
axillary dissection relevant to patients with clinically
node-negative breast cancer? Breast J 2003:9(6);478-
84. Full-text Exclude - Does not either (1) describe
an explicit priority-setting process which employs
either VOI or decision modeling or (2) provide
explicit discussion or examples of VOI analyses.
Claxton K. Bayesian approaches to the value of information: implications for the regulation of new
pharmaceuticals. Health Econ 1999:8(3);269-74.
Full-text Exclude - Does not either (1) describe an
explicit priority-setting process which employs either
VOI or decision modeling or (2) provide explicit
discussion or examples of VOI analyses.
Claxton K, Cohen JT and Neumann PJ. When is
evidence sufficient? Health Aff (Millwood) 2005:24(1);93-101. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Claxton K and Thompson KM. A dynamic
programming approach to the efficient design of clinical trials. J Health Econ 2001:20(5);797-822.
Full-text Exclude - Does not either (1) describe an
explicit priority-setting process which employs either
VOI or decision modeling or (2) provide explicit
discussion or examples of VOI analyses.

44
Coyle D and Oakley J. Estimating the expected value
of partial perfect information: a review of methods.
Eur J Health Econ 2008:9(3);251-9. Full-text Exclude
- No specific research prioritization
recommendations.
Disantostefano RL, Biddle AK and Lavelle JP. The
long-term cost effectiveness of treatments for benign
prostatic hyperplasia. Pharmacoeconomics
2006:24(2);171-91. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Eckermann S, Karnon J and Willan AR. The value of
value of information: best informing research design
and prioritization using current methods.
Pharmacoeconomics 2010:28(9);699-709. Full-text
Exclude - No specific research prioritization
recommendations.
Eckermann S and Willan AR. Expected value of
information and decision making in HTA. Health
Econ 2007:16(2);195-209. Full-text Exclude - No
specific research prioritization recommendations.
Fenwick E, Claxton K and Sculpher M. The value of
implementation and the value of information: combined and uneven development. Med Decis
Making 2008:28(1);21-32. Full-text Exclude - No
specific research prioritization recommendations.
Fleurence RL and Torgerson DJ. Setting priorities for
research. Health Policy 2004:69(1);1-10. Full-text
Exclude - No specific research prioritization
recommendations.
Fontaine O, Kosek M, Bhatnagar S, et al. Setting
research priorities to reduce global mortality from
childhood diarrhoea by 2015. PLoS Med
2009:6(3);e41. Full-text Exclude - Does not either (1)
describe an explicit priority-setting process which
employs either VOI or decision modeling or (2)
provide explicit discussion or examples of VOI
analyses.
Gazmuri RJ, Nolan JP, Nadkarni VM, et al. Scientific
knowledge gaps and clinical research priorities for
cardiopulmonary resuscitation and emergency
cardiovascular care identified during the 2005
International Consensus Conference on ECC and
CPR Science with Treatment Recommendations. A
consensus statement from the International Liaison
Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care
Committee; the Stroke Council; and the
Cardiovascular Nursing Council. Resuscitation
2007:75(3);400-11. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Goeree R, Levin L, Chandra K, et al. Health
technology assessment and primary data collection
for reducing uncertainty in decision making. J Am
Coll Radiol 2009:6(5);332-42. Full-text Exclude - No
specific research prioritization recommendations.
Griffin S, Claxton K and Sculpher M. Decision
analysis for resource allocation in health care. J
Health Serv Res Policy 2008:13 Suppl 3(23-30. Full-
text Exclude - No specific research prioritization
recommendations.
Griffin S, Welton NJ and Claxton K. Exploring the research decision space: the expected value of
information for sequential research designs. Med
Decis Making 2010:30(2);155-62. Full-text Exclude -
No specific research prioritization recommendations.
Groot Koerkamp B, Hunink MG, Stijnen T, et al.
Limitations of acceptability curves for presenting
uncertainty in cost-effectiveness analysis. Med Decis Making 2007:27(2);101-11. Full-text Exclude - No
specific research prioritization recommendations.
Groot Koerkamp B, Myriam Hunink MG, Stijnen T,
et al. Identifying key parameters in cost-effectiveness
analysis using value of information: a comparison of
methods. Health Econ 2006:15(4);383-92. Full-text
Exclude - No specific research prioritization
recommendations.
Hoyle M. Historical lifetimes of drugs in England:
application to value of information and cost-
effectiveness analyses. Value Health 2010:13(8);885-
92. Full-text Exclude - No specific research
prioritization recommendations.
Hunink MG. Outcomes research and cost-
effectiveness analysis in radiology. Eur Radiol
1996:6(5);615-20. Full-text Exclude - Does not either
(1) describe an explicit priority-setting process which
employs either VOI or decision modeling or (2)
provide explicit discussion or examples of VOI
analyses.
Janssen MP and Koffijberg H. Enhancing value of
information analyses. Value Health 2009:12(6);935-
41. Full-text Exclude - No specific research

45
prioritization recommendations.
Lomas J, Fulop N, Gagnon D, et al. On being a good listener: setting priorities for applied health services
research. Milbank Q 2003:81(3);363-88. Full-text
Exclude - Does not either (1) describe an explicit
priority-setting process which employs either VOI or
decision modeling or (2) provide explicit discussion
or examples of VOI analyses.
Mar J, Gutierrez-Moreno S and Chilcott J.
[Probabilistic cost-effectiveness analysis of the treatment of sleep apnea]. Gac Sanit 2006:20(1);47-
53. Full-text Exclude - Not available in English.
Meltzer D. Addressing uncertainty in medical cost-
effectiveness analysis implications of expected utility
maximization for methods to perform sensitivity
analysis and the use of cost-effectiveness analysis to
set priorities for medical research. J Health Econ
2001:20(1);109-29. Full-text Exclude - No specific
research prioritization recommendations.
Miller P. Role of pharmacoeconomic analysis in
R&D decision making: when, where, how?
Pharmacoeconomics 2005:23(1);1-12. Full-text
Exclude - No specific research prioritization
recommendations.
Nahin RL. Identifying and pursuing research
priorities at the National Center for Complementary
and Alternative Medicine. FASEB J
2005:19(10);1209-15. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Oakley JE, Brennan A, Tappenden P, et al.
Simulation sample sizes for Monte Carlo partial
EVPI calculations. J Health Econ 2010:29(3);468-77.
Full-text Exclude - No specific research prioritization
recommendations.
Paltiel AD and Kaplan EH. The epidemiological and
economic consequences of AIDS clinical trials. J
Acquir Immune Defic Syndr 1993:6(2);179-90. Full-
text Exclude - No specific research prioritization
recommendations.
Petticrew M, Chalabi Z and Jones DR. To RCT or
not to RCT: deciding when 'more evidence is needed' for public health policy and practice. J Epidemiol
Community Health 2011:Full-text Exclude - No
specific research prioritization recommendations.
Philips Z, Claxton K and Palmer S. The half-life of
truth: what are appropriate time horizons for research
decisions? Med Decis Making 2008:28(3);287-99.
Full-text Exclude - No specific research prioritization
recommendations.
Price MJ, Welton NJ, Briggs AH, et al. Model
averaging in the presence of structural uncertainty
about treatment effects: influence on treatment
decision and expected value of information. Value
Health 2011:14(2);205-18. Full-text Exclude - No
specific research prioritization recommendations.
Ricci PF, Cox LA, Jr. and Macdonald TR.
Precautionary principles: a jurisdiction-free
framework for decision-making under risk. Hum Exp
Toxicol 2004:23(12);579-600. Full-text Exclude - No
specific research prioritization recommendations.
Schmidt C. Researchers consider value-of-
information theory for selecting trials. J Natl Cancer Inst 2010:102(3);144-6. Full-text Exclude - No
specific research prioritization recommendations.
Sculpher M and Claxton K. Establishing the cost-
effectiveness of new pharmaceuticals under
conditions of uncertainty--when is there sufficient
evidence? Value Health 2005:8(4);433-46. Full-text
Exclude - No specific research prioritization
recommendations.
Shabtai I, Leshno M, Blondheim O, et al. The value
of information for decision-making in the healthcare
environment. Stud Health Technol Inform
2007:127(91-7. Full-text Exclude - Does not either
(1) describe an explicit priority-setting process which
employs either VOI or decision modeling or (2)
provide explicit discussion or examples of VOI
analyses.
Swint JM and Nelson WB. The application of
economic analysis to evaluation of alcoholism
rehabilitation programs. Inquiry 1977:14(1);63-72.
Full-text Exclude - No specific research prioritization
recommendations.
Walton SM, Schumock GT, Lee KV, et al.
Prioritizing future research on off-label prescribing:
results of a quantitative evaluation. Pharmacotherapy
2008:28(12);1443-52. Full-text Exclude - Does not
either (1) describe an explicit priority-setting process
which employs either VOI or decision modeling or
(2) provide explicit discussion or examples of VOI
analyses.
Welton NJ, Madan J and Ades AE. Are head-to-head

46
trials of biologics needed? The role of value of
information methods in arthritis research.
Rheumatology (Oxford) 2011:50 Suppl 4(iv19-25.
Full-text Exclude - No specific research prioritization
recommendations.
Willan A and Kowgier M. Determining optimal
sample sizes for multi-stage randomized clinical
trials using value of information methods. Clin Trials
2008:5(4);289-300. Full-text Exclude - Not focused
on research prioritization.
Willan AR. Optimal sample size determinations from
an industry perspective based on the expected value
of information. Clin Trials 2008:5(6);587-94. Full-
text Exclude - Not focused on research prioritization.
Willan AR and Kowgier ME. Cost-effectiveness
analysis of a multinational RCT with a binary
measure of effectiveness and an interacting covariate.
Health Econ 2008:17(7);777-91. Full-text Exclude -
No specific research prioritization recommendations.
Willan AR and Pinto EM. The value of information
and optimal clinical trial design. Stat Med
2005:24(12);1791-806. Full-text Exclude - No
specific research prioritization recommendations.
Woodward RS, Boxerman SB, Schnitzler MA, et al. Optimum investments in project evaluations: when
are cost-effectiveness analyses cost-effective? J Med
Syst 1996:20(6);385-93. Full-text Exclude - No
specific research prioritization recommendations
.

47
Appendix B. Data Abstraction Elements I. Study Characteristics
• Last name of first author
• Year of publication
• Study objective
• Indicate region(s) where study was performed (check all that apply):
o U.S.
o Canada
o UK
o Europe
o South America
o Central America
o Asia
o Africa
o Australia/ New Zealand
o Unclear/ Not reported
o Other (specify)
• List country(ies) where study was performed
• Analysis type (check all that apply):
o VOI
o Other modeling
• Funding organization (check all that apply):
o NIH
o AHRQ
o Other US government (specify)
o Non-US government (specify)
o WHO
o Professional society (specify)
o Advocacy group or NGO (e.g. AHA, ACS)
o Industry
o Academic
o NICE
o Unclear/ Not reported
• Primary audience for research priorities (check all that apply):
o Study sponsor/ funder (e.g. HTA by NICE)
o Named research funder other than study sponsor
o Unspecified research funders
o Other (specify)
II. Patient Preferences
• Measure of patient preferences (check all that apply):
o Utilities/QALY's
o Willingness to pay
o Other (specify)

48
o None/ not reported
• Source for patient preferences (check all that apply):
o Systematic review specifically for this article
o Cited systematic reviews
o Non-systematic review specifically for this article
o Cited non-systematic review
o Study conducted as part of this project
o Other (specify)
o None/ not reported
• Method for eliciting patient preferences (check all that apply):
o Linear rating scale
o Time-tradeoff
o Standard gamble
o Contingent valuation (willingness-to-pay)
o Discrete choice/conjoint analysis
o Other (specify)
o None/ not reported
• Prioritization method for modeling-based approaches (check all that apply):
o VOI analysis
o Cost effectiveness
o Probabilistic decision analytic model
o Other (specify)
o Not specified
III. Importance of Uncertainty About Patient Preferences on Results
• Ranking of at least one patient-centered outcome (including preferences/utilities,
adherence) in terms of key uncertainties
o Top 3
o Reported, but not in top 3
o Not important
o Not reported
• List the reported outcomes/ key uncertainties







