
Tumor Imaging in Nuclear Medicine: Current Status and
Future ProspectsFuture Prospects
Bennett S. Greenspan, MD
SNMMWM Albuquerque, NMSNM MWM Albuquerque, NM
January 30, 2010

Tumor Imaging – Part I Current Status
• Current status – agents that are FDA‐approved for routine clinical useapproved for routine clinical use.

Tumor ImagingTumor Imaging
• Indications for tumor imaging:• Indications for tumor imaging:
• Identification, diagnosis
• Staging/re‐staging
• Identification of recurrence residual• Identification of recurrence, residual disease
• Monitoring response to therapy
• Evaluating prognosisEvaluating prognosis

Tumor Imaging ‐ AgentsTumor Imaging Agents
• Ga‐67 citrateGa 67 citrate• Organ imaging, e.g. thyroid, bone• Thallium‐201• Thallium‐201 • Tc‐99m Sestamibi – Breast imagingL b l d l l tib di• Labeled monoclonal antibodies
• Peptide receptor imaging In‐111 pentetreotide• Adrenal tumor imaging – I‐123 MIBG• F‐18 FDG

Ga‐67 citrate ‐ LymphomaGa 67 citrate Lymphoma

Ga‐67 citrate ‐MelanomaGa 67 citrate Melanoma

Ga‐67 citrateGa 67 citrate
• Mechanism of uptake – bound to• Mechanism of uptake – bound to transferrin, uptake in tumor cells by l d d l i ti llysosomes and endoplasmic reticulum
• Now nearly obsolete as a tumor imaging agent – outperformed by FDG PETagent – outperformed by FDG PET

Ga‐67 citrateGa 67 citrate
• Probable only remaining indication for• Probable only remaining indication for Ga‐67 citrate in tumor imaging:– Differentiating hepatocellular carcinoma from regenerating nodules in patients with cirrhosis

Thyroid CarcinomaThyroid Carcinoma
• Indications for imaging with I‐131:• Indications for imaging with I‐131:
1. Detect active residual disease (papillary or follicular thyroid CA)
2. Detect functioning metastases2. Detect functioning metastases
3. Assess results of treatment

Papillary Thyroid CancerPapillary Thyroid Cancer

Papillary Thyroid CancerPapillary Thyroid Cancer

Papillary Thyroid CarcinomaPapillary Thyroid Carcinoma

Metastatic Thyroid CarcinomaMetastatic Thyroid Carcinoma

I‐131 – Thyroid CarcinomaI 131 Thyroid Carcinoma
• I‐131: Oldest radionuclide (RN) in clinical useI 131: Oldest radionuclide (RN) in clinical use
• Images are not very pretty, due to the high gamma energy but the information obtainedgamma energy, but the information obtained is extremely useful.
H i i i d b i i• Having a gamma emission and a beta emission makes this RN uniquely suited to therapy, esp. f h id di Th i lfor thyroid disease. There is no replacement on the horizon.

Bone Scan ‐Prostate Carcinoma –d d bwidespread bone metastases

Bone scanBone scan
• Agent: Tc‐99m MDP (or HDP)Agent: Tc 99m MDP (or HDP)
• Uptake related to blood flow and osteoblastic activityactivity
• Very sensitive for metastases that generate an bl i ( )osteoblastic response (most tumors)
• Useful for staging/re‐staging, assessing response to therapy, detecting recurrence or residual disease
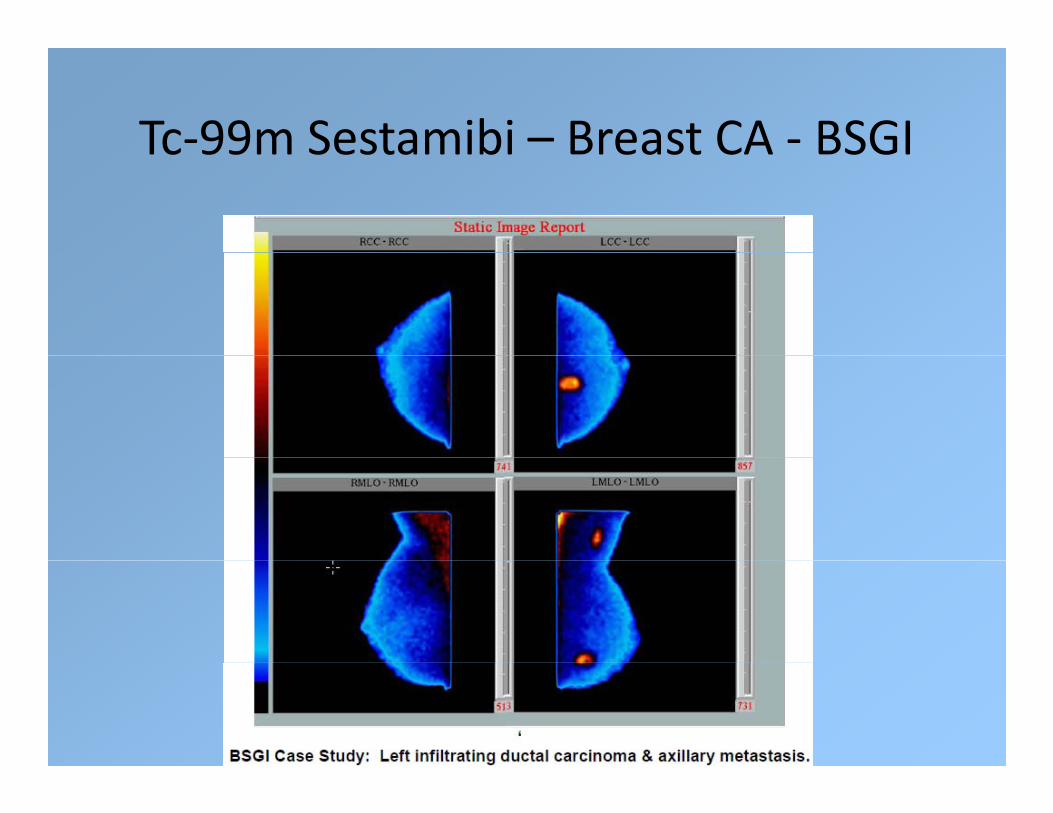
Tc‐99m Sestamibi – Breast CA ‐ BSGITc 99m Sestamibi Breast CA BSGI

Breast Specific Gamma Imaging (BSGI)Breast Specific Gamma Imaging (BSGI)

BSGI ‐ 4 mm tumorBSGI 4 mm tumor

BSGIBSGI
• Fairly new technique‐ utilizes small gamma camera optimized to image the breast
• Will not replace mammography, but may be aWill not replace mammography, but may be a useful adjunct in certain circumstances, particularly if MRI is indicated but cannot beparticularly if MRI is indicated but cannot be done.
• Greater sensitivity and specificity than• Greater sensitivity and specificity than conventional scintimammography.
SNM P d G id li d d l t• SNM Procedure Guideline under development

ProstascintProstascint
• Monoclonal Antibodies – Prostascint –Monoclonal Antibodies Prostascint Capromab Pendetide, labeled with In‐111
• Used in patients with prostate cancer to• Used in patients with prostate cancer, to detect recurrent or residual disease.

SPECT/CT ‐ NormalSPECT/CT Normal

Tumor in Prostate BedTumor in Prostate Bed

Nodal metastases ‐ pelvisNodal metastases pelvis

Para‐aortic nodes – Coronal images /SPECT/CT

ProstascintProstascint
• Only monoclonal antibody in routine clinicalOnly monoclonal antibody in routine clinical use.
• Not a very good agent less sensitive than is• Not a very good agent – less sensitive than is desirable, and images are often difficult to readread.
• Also, test is performed over 4‐7 days.

Peptide Receptor ImagingPeptide Receptor Imaging
• Somatostatin receptor imaging ‐ In‐111Somatostatin receptor imaging In 111 pentetreotide (Octreotide, Octreoscan).
• Neuroendocrine tumors derived from APUD• Neuroendocrine tumors – derived from APUD (Amine Precursor Uptake and Decarboxylation) system cellsDecarboxylation) system cells
• Examples: carcinoid, pituitary adenoma, i i l ll ll ll lpancreatic islet cell tumor, small cell lung
cancer, pheochromocytoma, neuroblastoma

In‐111 Pentetreotide (Octreoscan) ‐k l llMerkel cell tumor

Metastatic carcinoid, with meningiomaMetastatic carcinoid, with meningioma

Adrenal Tumor ImagingAdrenal Tumor Imaging
• Adrenal tumor imaging–Adrenal tumor imaging
• I‐123 MIBG: Pheochromocytoma, Neuroblastoma ParagangliomaNeuroblastoma, Paraganglioma
• MIBG (metaiodobenzylguanidine) is an analog f i h iof norepinephrine
• Taken up by chromaffin cells, and therefore useful in imaging sympathetic adrenergic tissue.

Recurrent Malignant h hPheochromocytoma
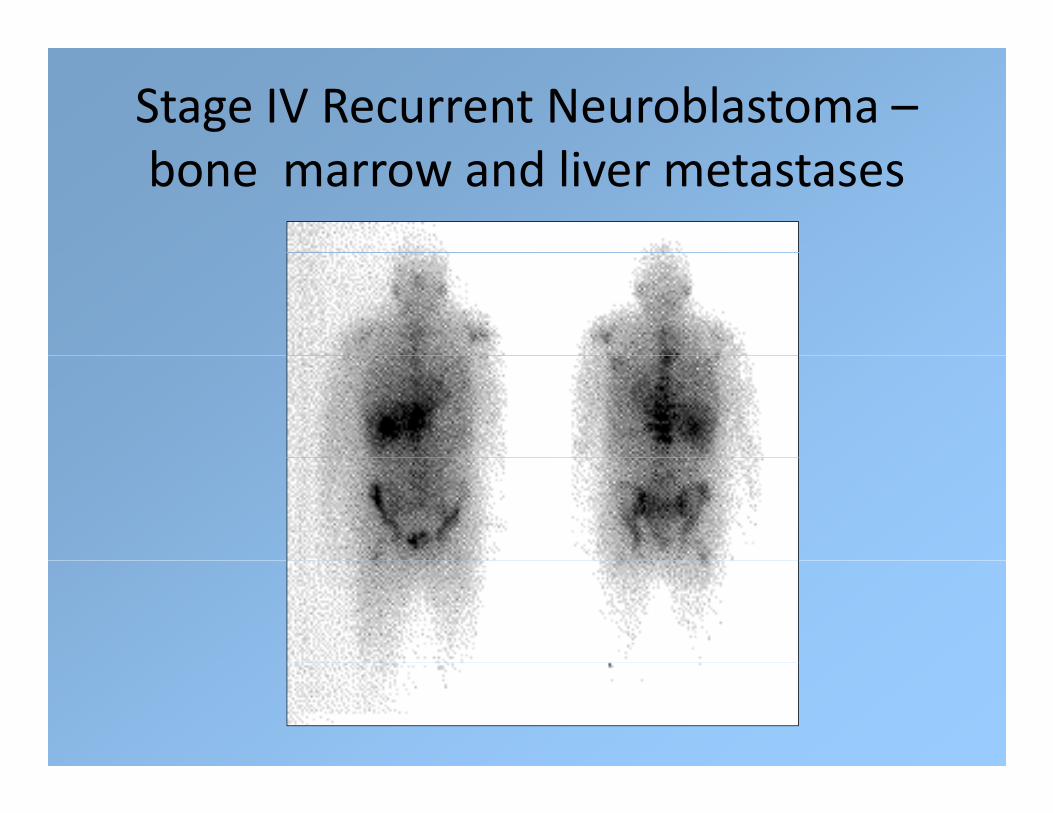
Stage IV Recurrent Neuroblastoma –b d lbone marrow and liver metastases

Tumor – FDG PETTumor FDG PET
• F‐18 FDGF 18 FDG
• Used for many tumors for staging/re‐staging, monitoring response to therapymonitoring response to therapy, detecting recurrent or residual disease
F l H d d k l l h• For example: Head and neck, lung, lymphoma, melanoma, esophageal, colorectal, breast,
i l CAcervical CA

Positron DecayMettler and Guiberteau, Essentials of Nuclear Medicine Imaging, 2006, p. 361

Metabolism of F‐18 FDGMettler and Guiberteau, Essentials of Nuclear Medicine Imaging, 2006, page 372

F‐18 FDG H&N – Base of Tongue CAF 18 FDG H&N Base of Tongue CA
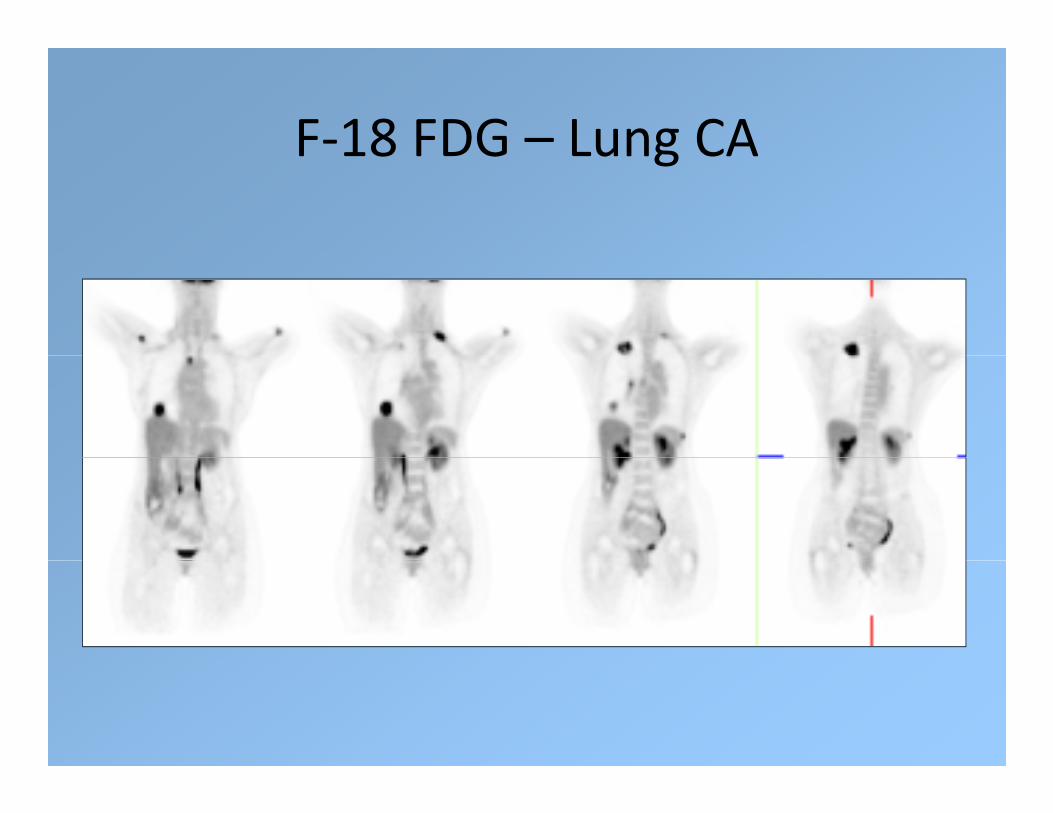
F‐18 FDG – Lung CAF 18 FDG Lung CA

DLBCL – Extensive Bone Marrow lInvolvement
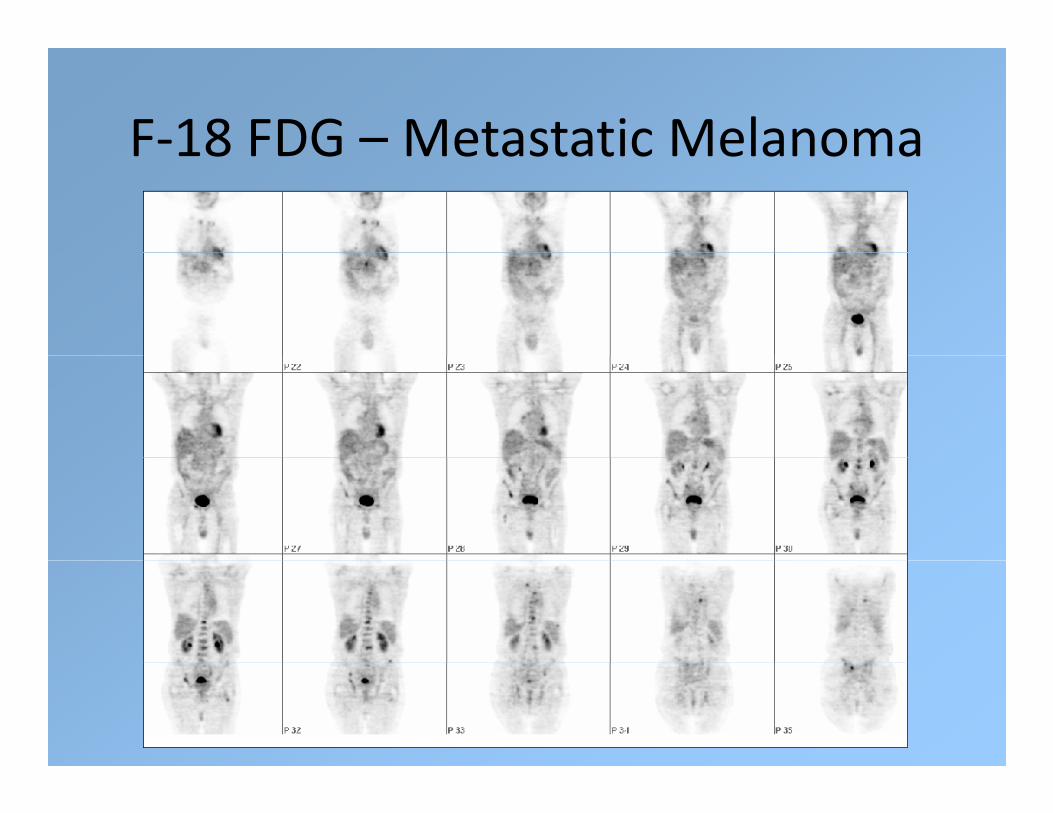
F‐18 FDG – Metastatic MelanomaF 18 FDG Metastatic Melanoma

F‐18 FDG Esophageal CA with Liver Metastases

F‐18 FDG ‐Disseminated cervical cancer metastases

F‐18 – FDGF 18 FDG
• While F‐18 ‐ FDG is a “non‐specific” agent it isWhile F 18 FDG is a non specific agent, it is useful for many different malignancies. It measures glycolysis which is increased inmeasures glycolysis, which is increased in many tumors.
• Photon flux is 100 times greater than for• Photon flux is 100 times greater than for conventional single photon agents, allowing for better spatial resolutionfor better spatial resolution.

Current Molecular Imaging in routine l l l ( )clinical use in Oncology (Part I)
• I‐131 – thyroidI 131 thyroid
• In‐111 octreotide (pentetreotide)
23/ 3 G• I‐123/131 MIBG
• In‐111 monoclonal antibody ‐ Capromab Pendetide (Prostascint)
• Ga‐67 citrate (essentially obsolete as a tumor ( yimaging agent)
• F‐18 FDGF 18 FDG


Tumor Imaging – Part IITumor Imaging Part II
• Future prospects –Future prospects
• Note – Except for F‐18 FDG, the following agents are not FDA approved Many of theseagents are not FDA‐approved. Many of these are in clinical trials.

• DetectionDetection
• Treatment – especially as a precursor for targeted therapytargeted therapy
• Early Intervention
• Drug Discovery and Development

Molecular ImagingMolecular Imaging
• Molecular imaging (MI) –Molecular imaging (MI)
• MI will have an expanding clinical relevance as it will become increasingly important init will become increasingly important in patient care and management in the near future; andfuture; and ‐
• PET is the most sensitive and the most specific h i i l l h itechnique to image molecular pathways in
patients

Why the Interest in Molecular Imaging?
• The ultimate goal is targeted therapy toThe ultimate goal is targeted therapy to provide personalized medicine.
• Targeted imaging: finding the right molecular• Targeted imaging: finding the right molecular probe for the right target to monitor the right disease in the right patientdisease in the right patient.
• Streamlining drug discovery: finding the right d i h i h h i hdrug against the right target to treat the right disease in the right patient

Molecular ImagingMolecular Imaging

Molecular ImagingMolecular Imaging

Molecular ImagingMolecular Imaging
• Therapeutic response criteria –Therapeutic response criteria
• Will be based on metabolic characteristics rather than size alonerather than size alone
• Translational research – bringing experimental i i d h i h i himaging and therapeutic techniques to the clinic after extensive testing in experimental
d l (b h b d id )models (bench to bedside)

Molecular ImagingMolecular Imaging
Radiotracer Imaging of cancerRadiotracer Imaging of cancer
• Categories:• Categories:
– Proliferation/DNA synthesis
– Hypoxia
– Receptors– Receptors
– Angiogenesis
– Metabolism – F‐18 FDG/Amino acid transporttransport

Cancer Imaging Agents
• Radiopharmaceuticals for imaging cellular proliferation
3’ d 3’ [18 ]fl h idi ([18 ] )– 3’‐deoxy‐3’‐[18F]fluorothymidine ([18F]FLT)
– Imaging with 18F‐labeled sigma‐2 receptor ligands
• Imaging tumor hypoxia
– 60/64Cu‐ATSMCu ATSM
– 18F‐MISO
• Imaging upregulation of receptors in tumors
– 68Ga‐labeled somatostatin analogs

Cancer Imaging Agents
• Radiopharmaceuticals for imaging cellular proliferation
3’ d 3’ [18 ]fl h idi ([18 ] )– 3’‐deoxy‐3’‐[18F]fluorothymidine ([18F]FLT)
– Imaging with 18F‐labeled sigma‐2 receptor ligands
• Imaging tumor hypoxia
– 60/64Cu‐ATSMCu ATSM
– 18F‐MISO
• Imaging upregulation of receptors in tumors
– 68Ga‐labeled somatostatin analogs

Why Image Cellular ProliferationWhy Image Cellular Proliferation
• Rationale – Proliferative status of tumors mayRationale Proliferative status of tumors may indicate which patients are at high risk of recurrence as that has a profound effect onrecurrence, as that has a profound effect on outcome from therapy.
• A change in the proliferative status of a tumor• A change in the proliferative status of a tumor during or after therapy may also be an indicator of response and allow furtherindicator of response and allow further tailoring of therapy.

O
18F‐Labeled Thymidine Analogs
HN
O
CH3
N
HN
O
O
CH3
HN
O
Br
N
HN
O
O
I
O
HH
HO
NO
O18FH
HH
HO
NO
O18FH
HO
NO
O18FH
HO
NO
H18FHH
[18F]FLT
HOHHH
[18F]FMAU
HOHHH
[18F]FBAU
HOHHH
[18F]FIAU

F 18 i th di l b l d f f th i idi l id
3′deoxy‐3′‐[18F]fluorothymidine: [18F] FLT
F-18 is the radiolabeled form of the pyrimidine nucleoside, thymidine
FLT is retained within the cell after phosphorylation providing a f ll l th idi ki (TK1) ti itmeasure of cellular thymidine kinase (TK1) activity, an enzyme
which is closely related to cellular proliferation. TK1 is up-regulated in the S phase of the cell cycle
N
NH
OHO
O
O N
NH
OO
O
OPHOO
O
TK-1DNA synthesis
O
OH
O
OH
O
O O
THYMIDINE
N
NH
OHO
O
18F
O N
NH
OO
O
18F
OPHOO
O
TK-1DNA synthesis
18F 18F
FLUOROTHYMIDINE [18F]FLT dTMP

F‐18 FLTF 18 FLT
• F‐18 FLT – F‐18 replaces OH at 3’ position – itF 18 FLT F 18 replaces OH at 3 position it cannot be incorporated into DNA, and is trapped in tumor cells followingtrapped in tumor cells following phosphorylation of the 5’‐hydroxy group by thymidine kinase (TK‐1)thymidine kinase (TK 1).
• Analogous to trapping of F‐18 FDG in cells following phosphorylation by hexokinasefollowing phosphorylation by hexokinase.
• F‐18 FLT is a marker of cell proliferation, but d di l DNA h idoes not directly measure DNA synthesis.

F‐18 FLT ‐ ProliferationF 18 FLT Proliferation • F‐18 Fluorothymidine (F‐18 FLT) Mach, et al, PET Clinics, Jan, 2009

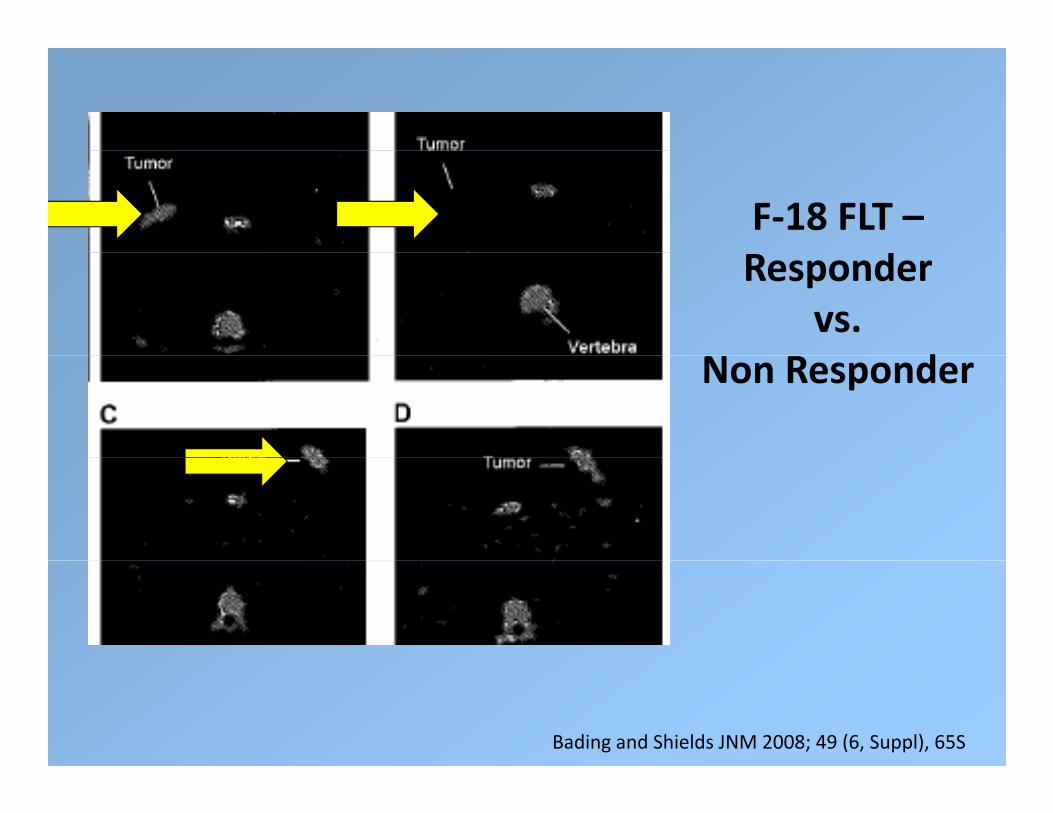
F‐18 FLT –dResponder
vs. dNon Responder
Bading and Shields JNM 2008; 49 (6, Suppl), 65S

F‐18 FLT –dResponder
vs. dNon Responder
Bading and Shields JNM 2008; 49 (6, Suppl), 65S
F‐18 FLT –dResponder
vs. dNon Responder
Bading and Shields JNM 2008; 49 (6, Suppl), 65S

F‐18 FLT –dResponder
vs. dNon Responder
Bading and Shields JNM 2008; 49 (6, Suppl), 65S

ProliferationProliferation

ProliferationProliferation


Proliferation – Sigma‐2 ReceptorsProliferation Sigma 2 Receptors

Sigma‐2 ReceptorsSigma 2 Receptors

Sigma‐2 ReceptorsSigma 2 Receptors

ProliferationProliferation

Proliferation: F‐18 ISOProliferation: F 18 ISO

F‐18 FLT, F‐18 FMAU, F‐18 ISO‐1F 18 FLT, F 18 FMAU, F 18 ISO 1

Proliferation AgentsProliferation Agents

F‐18 ‐ FLT vs. F‐18 ‐ ISOF 18 FLT vs. F 18 ISO
• FLT shows some promise and is in currentFLT shows some promise, and is in current clinical trials sponsored by SNM
• However FLT only shows proliferating cells in• However, FLT only shows proliferating cells in S‐phase, about 2% of proliferating cells.
F ISO h ll f h lif i ll d• F‐ISO shows all of the proliferating cells, and may turn out to be a better agent for d i lif i lldetecting proliferating cells.

Cancer Imaging Agents
• Radiopharmaceuticals for imaging cellular proliferation
3’ d 3’ [18 ]fl h idi ([18 ] )– 3’‐deoxy‐3’‐[18F]fluorothymidine ([18F]FLT)
– Imaging with 18F‐labeled sigma‐2 receptor ligands
• Imaging tumor hypoxia
– 60/64Cu‐ATSMCu ATSM
– 18F‐MISO
• Imaging upregulation of receptors in tumors
– 68Ga‐labeled somatostatin analogs

HypoxiaHypoxia
• Tumor cells that outgrow their blood supplyTumor cells that outgrow their blood supply become hypoxic, and slow their growth rate.
• Chemotherapy and radiotherapy become less• Chemotherapy and radiotherapy become less effective – chemotherapy depends on proliferation rate to be effective andproliferation rate to be effective, and cytotoxicity of radiotherapy depends on level of intracellular oxygenof intracellular oxygen.
Why Image Hypoxia?
• Hypoxia influences response to treatment:
(1)Radiotherapy - hypoxic cells are protected fromlethal effects of conventional ionizing radiationtherapytherapy
(2)Chemotherapy - effect of hypoxia on specialgenes and drug delivery
• Imaging of hypoxia is required in order to predictresponse to traditional therapies
• Imaging of hypoxia in the brain, heart and cancer havebeen explored

HypoxiaHypoxia

HypoxiaHypoxia
• PET imaging agents that can be used to assessPET imaging agents that can be used to assess regional tumor hypoxia:
• F‐18 Misonidazole (FMISO)
• Cu‐64 ATSM

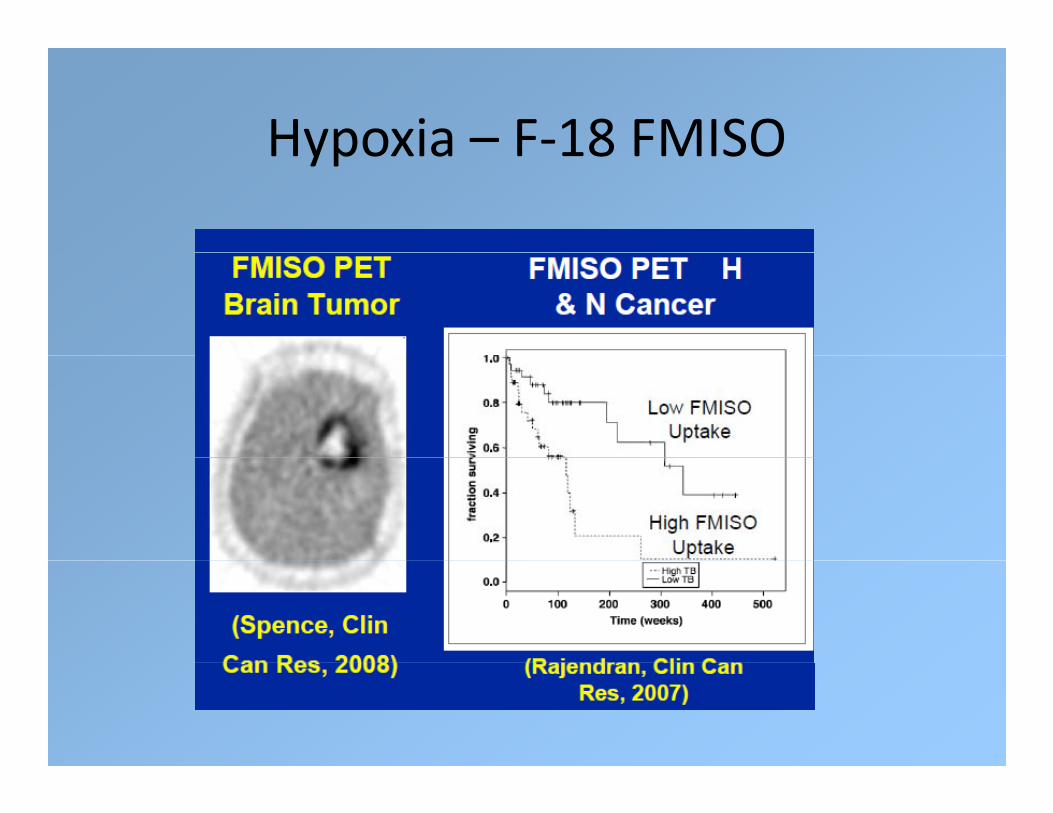
Hypoxia – F‐18 FMISOHypoxia F 18 FMISO

Hypoxia – F‐18 FMISOHypoxia F 18 FMISO
• Most widely used PET agent for regionalMost widely used PET agent for regional hypoxia.
• It is retained in hypoxic cells; it enters by• It is retained in hypoxic cells; it enters by passive diffusion and undergoes reduction, eventually forming covalent bonds witheventually forming covalent bonds with macromolecules, and is trapped in the cell.
I f l b i id if• Images are of low contrast, but it can identify clinically significant regional hypoxia.
Hypoxia – F‐18 FMISOHypoxia F 18 FMISO
• It requires a venous blood sample takenIt requires a venous blood sample taken during imaging, to determine a normalized map of a tissue to blood ratio T/Bmap of a tissue to blood ratio, T/B.
• The hypoxic portion of a tumor can be characterized by a maximum T/B or T/Bcharacterized by a maximum T/B, or T/B greater than a defined threshold.

Hypoxia – F‐18 FMISOHypoxia F 18 FMISO
• Identification of hypoxic tumor may helpIdentification of hypoxic tumor may help facilitate image‐directed radiotherapy.
• It appears to have the potential to predict the• It appears to have the potential to predict the response to treatment (better than F‐18 FDG) and provide prognostic informationand provide prognostic information.
• However, there are some drawbacks to this agent.
Hypoxia – F‐18 FMISOHypoxia F 18 FMISO

HypoxiaCu ATSMCu‐ATSM
CH3H3CTheory:Theory:N N NN
S SHN NH
Cu
yy
NOTTRAPPED
NOTTRAPPEDTRAPPEDTRAPPED
CH3 CH3
CH3H3C
N N N
CH3
N
H3C
TRAPPEDTRAPPED
N N N
CH3
N
H3C
CuN N NN
SH HSHN NH
CH3 CH3
NN
S SHN NH
CH3 CH3
CuNN
S SHN NH
CH3 CH3
Cu
Normal cell (+ONormal cell (+O22))Hypoxic cell (Hypoxic cell (--OO22))

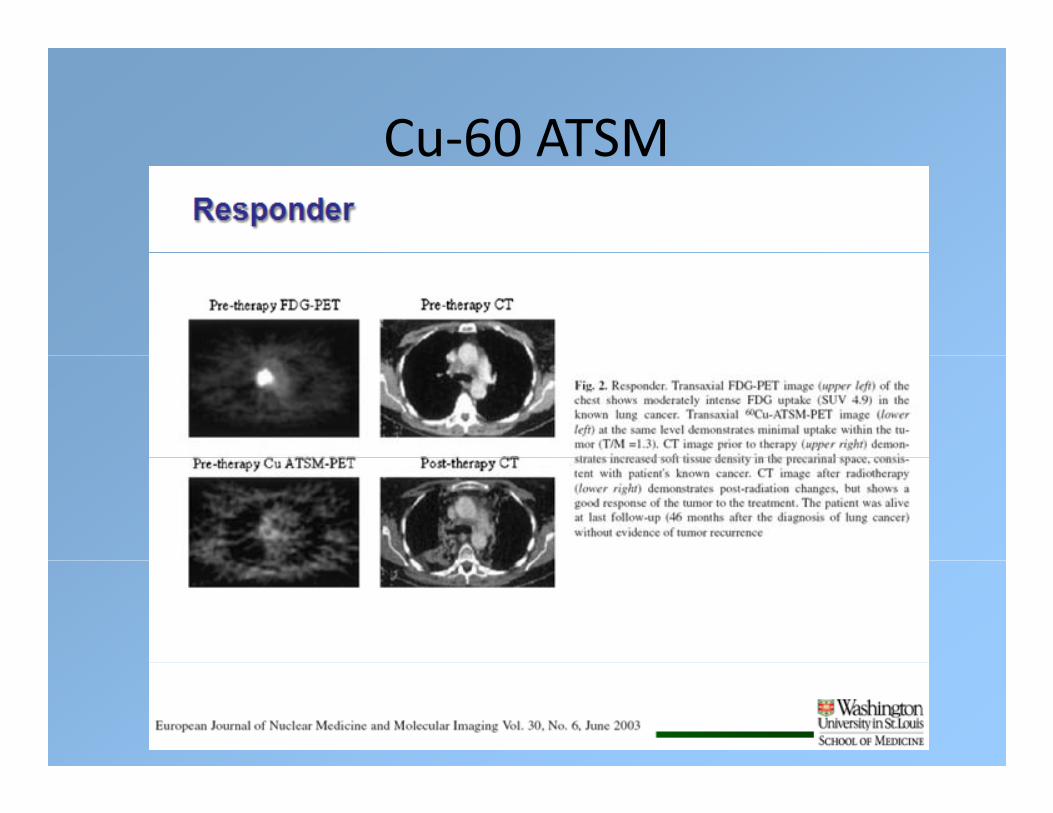
Cu‐ATSMCu ATSM
• In the hypoxic cell Cu (II) ATSM is reduced toIn the hypoxic cell, Cu (II) ATSM is reduced to Cu (I) ATSM.
• Cu (I) is then released from ATSM and is• Cu (I) is then released from ATSM and is trapped in the hypoxic cell.
C (II) i d i i ll• Cu (II) is not trapped in normoxic cells.

Copper RadionuclidesCopper Radionuclides
Isotope Half-life
Decay modes
Maximum + Reaction Natural abundancelife modes
/% energy (MeV)
abundanceof target isotope
60Cu
23 7 m
/93 0
3 92 60Ni(p n)
26 1%Cu
23.7 m /93.0EC/7.0
3.92 Ni(p,n) 26.1%
61Cu 3.32 h +/60.0 1.22 61Ni(p,n) 1.25% /60.0EC/7.0
(p, ) %
64Cu 12.7 h +/17.8 0.66 64Ni(p,n) 1.16% EC/43.8 -/38.4*
*Qaim et al. Radiochimica Acta 2007; 95:67-73

Cu‐60 /Cu‐64Cu 60 /Cu 64
• Most of the early clinical trials were done withMost of the early clinical trials were done with Cu‐60.
• However Cu 60 has too short a half life for• However, Cu‐60 has too short a half‐life for multicenter clinical trials.
Th FDA d fi h C 64• The FDA wanted to confirm that Cu‐64 gave similar results, and could be used in place of C 60 i h 12 7 h h lf lif i b dCu‐60; with a 12.7 hr half life, it can be used for multi‐center clinical trials.

Uptake of 64Cu(ATSM), 64Cu(PTSM) and 18F‐MISO in EMT6 cells after 1 h at varying levels of oxygen
10064Cu(PTSM)
60
80
ptak
e
20
40% u
p
64Cu(ATSM)
18F-MISO0
20
1 10 102 103 104 105 106
Oxygen concentration (ppm)

Cu‐ATSMCu ATSM

Cu‐60‐ATSM NSCLCCu 60 ATSM NSCLC

Cu‐ATSM NSCLCCu ATSM NSCLC

Cu‐60 ATSM vs. F‐18 FDGCu 60 ATSM vs. F 18 FDG
Cu‐60 ATSMCu 60 ATSM

Cu‐60 ATSMCu 60 ATSM

Cu‐60 ATSM Predictor of SurvivalCu 60 ATSM Predictor of Survival

Cu‐60 ATSM vs. F‐18 FDGCu 60 ATSM vs. F 18 FDG

Cu‐64 ATSM vs. Cu‐60 ATSMCu 64 ATSM vs. Cu 60 ATSM

Cu‐64 ATSM vs. Cu‐60 ATSMCu 64 ATSM vs. Cu 60 ATSM


Hypoxia• In cervical CA, tumor hypoxia is predictive of decreased disease‐free survival and poorerdecreased disease free survival and poorer overall survival.
• Cu 64 ATSM provides prognostic information in• Cu‐64 ATSM provides prognostic information in cervical cancer that F‐18 FDG is unable to provideprovide.
• Cu‐64 ATSM is strongly correlated with response t th d ll i lto therapy and overall survival.
• Currently an ACRIN clinical trial is ongoing with Cu‐64 ATSM in patients with cervical cancer.

Cancer Imaging Agents
• Radiopharmaceuticals for imaging cellular proliferation
3’ d 3’ [18 ]fl h idi ([18 ] )– 3’‐deoxy‐3’‐[18F]fluorothymidine ([18F]FLT)
– Imaging with 18F‐labeled sigma‐2 receptor ligands
• Imaging tumor hypoxia
– 60/64Cu‐ATSMCu ATSM
– 18F‐MISO
• Imaging upregulation of receptors in tumors
– 68Ga‐labeled somatostatin analogs

Receptor ImagingReceptor Imaging

Receptor ImagingReceptor Imaging
• Tumor receptors have an important role inTumor receptors have an important role in carcinogenesis and tumor growth.
• Evaluation of tumor receptor expression is• Evaluation of tumor receptor expression is critical in cancer therapy directed at tumor receptorsreceptors.
• The ability to measure expression of tumor i i l f l i i freceptors is essential for selecting patients for
receptor‐targeted therapy.
Receptor ImagingReceptor Imaging
• Tumor receptor imaging can:Tumor receptor imaging can:
• 1. characterize tumor biology,
2 id if h i d• 2. identify therapeutic targets, and
• 3. delineate the pharmacodynamics of targeted cancer therapy.
• Advantages: Noninvasive, measurement of g ,receptor expression of entire disease burden, and potential for serial studies.p

Gallium‐68Gallium 68

Gallium‐68Gallium 68

Ga‐68Ga 68

Receptor ImagingReceptor Imaging

Summary – Proliferation, Hypoxiay , yp• Proliferation:
– FLT has applications in determining proliferative status of tumors havingFLT has applications in determining proliferative status of tumors having implications in predicting aggressiveness and monitoring therapy
– Radiolabeled DNA precursors underestimate the P:Q ratio
receptor imaging agents show promise in animal studies but need to– 2 receptor imaging agents show promise in animal studies but need to be validated in human imaging studies
• Hypoxia– 60Cu‐ATSM has shown promise in several clinical studies for imaging
hypoxia in NSCLC, head and neck, rectal and cervical cancers
– 64Cu‐ATSM provides higher quality images and is currently under IND p g q y g ywith a multi‐center trial to begin soon
– Caution should be advised that this agent does not image hypoxia in all tumor types, i.e. prostate canceryp , p

Summary – ReceptorsSummary Receptors
• Receptor Targeted Agents:• Receptor Targeted Agents:– Somatostatin is one tumor receptor that has been heavily studied both
pre‐clinically as well as clinically 68 111– The implementation of PET agents (68Ga) compared to SPECT (111In) has
greatly improved the tumor targeting and non‐target tissue clearance

Translational Molecular Imaging in Oncology
• Current Near FutureCurrent Near Future
• I‐131 –Thyroid Proliferation
id 8 / SO• In‐111 octreotide ∙ F‐18 FLT/ISO
• I‐123/131 MIBG Hypoxia
• In‐111 capromab ∙ Cu‐64 ATSM/FMISO
• F‐18 FDG ReceptorsF 18 FDG Receptors
Angiogenesis


Tumor Imaging – Future ProspectsTumor Imaging Future Prospects
• I would like to thank the following colleagues:I would like to thank the following colleagues:• Carolyn Anderson
• Jon McConathyy
• Robert Mach
• Mike Graham
• Barry Siegel
• Mike Welch
• Steve Larson







