
5/21/2014
1
Catherine Juillard, MD MPH
May 29, 2014
Trauma: Year in Review
Overview
• Hemorrhage control
• Traumatic Neurologic Injury
• Shifting of practice patterns for specific injuries
– Rib Fractures
– Major Vascular Injuries
Hemorrhage Control
• Major advances
– 1:1 RBC:FFP resuscitation
• PROMMTT
• PROPPR
– Prothrombin Complex
• Minor advances
– CRASH‐2 trial

5/21/2014
2
Coagulopathy of Trauma
• 20%‐30% of severely injured patients are coagulopathic upon arrival to ED.
• Causes– Consumption of factors (active hemorrhage)
– Dilution of factors (resuscitation)
– Prescription medications• Plavix, Coumadin, Aspirin, and new anticoagulants increasingly common in trauma patients
• Cornerstone of “Lethal Triad”– Acidosis, hypothermia, coagulopathy
Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003 Jun;54(6):1127‐30.Bellal J, Amini A, Friese RS, et al. Factor IX complex for the correction of coagulopathy. J Trauma. 2011 Dec;72(4):828‐834.
“Bloody Vicious Cycle”
BleedingBleeding
Acidosis Hypothermia
Acidosis Hypothermia
CoagulopathyCoagulopathy
“Damage Control”
• Permissive hypotension
• Minimization of crystalloid
• Liberal use of blood products
• Drugs to combat coagulopathy
Damage Control ResuscitationProthrombin Complex

5/21/2014
3
1:1 Resuscitation
• “Damage Controlled Resuscitation”
– >100 publications in last 24 months
• Avoid crystalloid in favor of balanced RBC:FFP in severely injured
• Significant mortality benefit
• All studies retrospective in civilian literature until 2013
Civilian Literature (2008)
2746 pts needing operative intervention135 pts needing >10 units PRBC4yr retrospective study
Closer to 1:1 = BETTER
>=8 units PRBCN = 415Prospective cohort studyJ Trauma. 2008 Nov;65(5):986‐93.J Trauma. 2008;65:272‐278.
Could these become a simple score?

5/21/2014
4
But…in need of prospective data…
• Prospective, observational, cohort study• 10 Level 1 trauma centers• July 2009‐October 2010• Primary objective:
– Investigate in‐hospital mortality in all patients surviving at least 30 minutes after ED admission
• Minute to minute tracking until resuscitation complete
• Followed until hospital discharge
Prospective Observational Multicenter Major Trauma Transfusion study
• Inclusion criteria:• Major trauma activation
• At least 16 years old
• Arrival from scene
• Received at least 1 unit of RBCs in first 6 hours of care
• 1245 patients• 905 Received 3 or more units of blood products
• 297 Massive transfusions (10+ RBC in 24 hours)
Prospective Observational Multicenter Major Trauma Transfusion study

5/21/2014
5
Methods: Trigger Selection
CITT Study
• Adapted from military
• SBP <90 mm Hg
• Hemoglobin <11 g/dL
• Temperature <35.5 C
• INR >1.5
• BD >=6
ABC Study
• Civilian Score
• SBP<90 mmHg
• HR >=120 bpm
• FAST exam positive
• Penetrating trauma
• Entire cohort (1245 patients)
• 1st ED Value utilized for each trigger
• As numbers of triggers positive increased, highly predictive of increasing risk for need for MT
5/21/2014
6
plasma 2:1 1:1 1:2 pRBCs
Ev
an
s B
lue
(u
g/g
tis
su
e)
0
2
4
6
8
10
12
14
plasma 2:1 1:1 1:2 pRBCs
Ev
an
s B
lue
(u
g/g
tis
su
e)
0
5
10
15
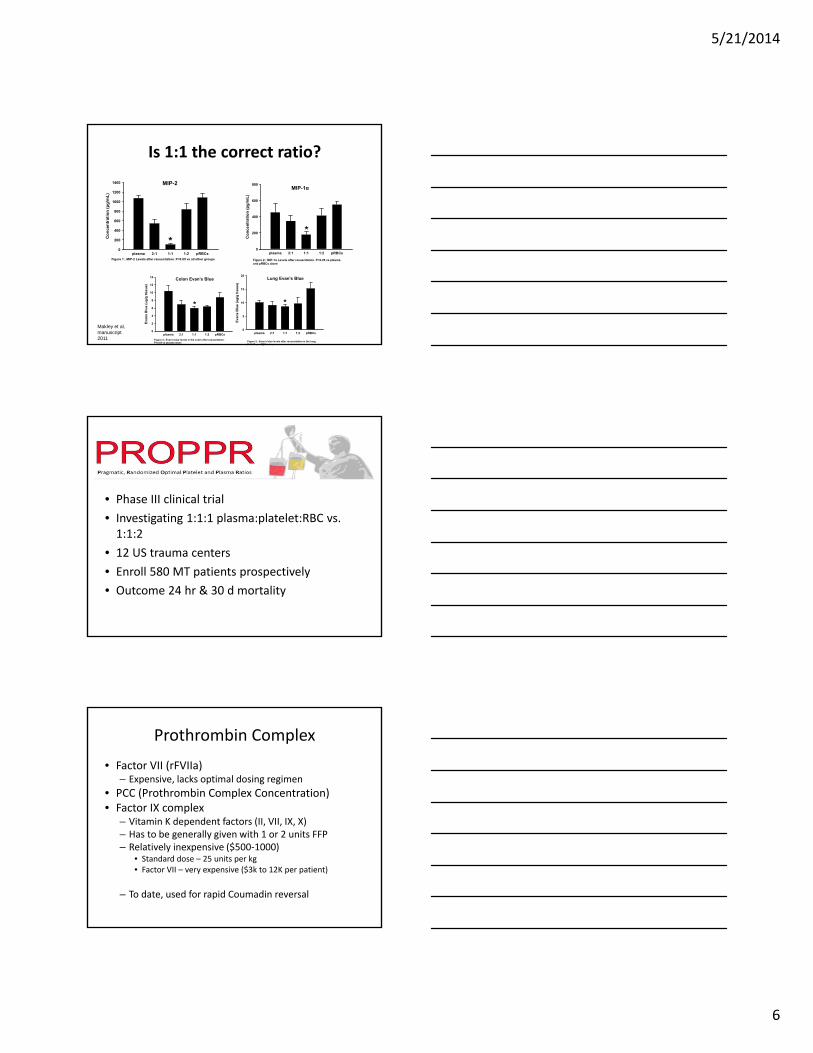
20Colon Evan’s Blue Lung Evan’s Blue
Figure 4:. Evan’s blue levels in the colon after resuscitation. P<0.05 vs plasma alone
* *
Figure 5:. Evan’s blue levels after resuscitation in the lung. P<0.05 vs pRBCs alone
Is 1:1 the correct ratio?
plasma 2:1 1:1 1:2 pRBCs
Co
nce
ntr
atio
n (
pg
/mL
)
0
200
400
600
800
1000
1200
1400 MIP-2
Figure 1:. MIP-2 Levels after resuscitation. P<0.05 vs all other groups
*plasma 2:1 1:1 1:2 pRBCs
Co
nce
ntr
ati
on
(p
g/m
L)
0
200
400
600
800MIP-1α
Figure 2:. MIP-1α Levels after resuscitation. P<0.05 vs plasma and pRBCs alone
*
Makley et al, manuscript 2011
• Phase III clinical trial
• Investigating 1:1:1 plasma:platelet:RBC vs. 1:1:2
• 12 US trauma centers
• Enroll 580 MT patients prospectively
• Outcome 24 hr & 30 d mortality
Prothrombin Complex
• Factor VII (rFVIIa)– Expensive, lacks optimal dosing regimen
• PCC (Prothrombin Complex Concentration)• Factor IX complex
– Vitamin K dependent factors (II, VII, IX, X)– Has to be generally given with 1 or 2 units FFP – Relatively inexpensive ($500‐1000)
• Standard dose – 25 units per kg• Factor VII – very expensive ($3k to 12K per patient)
– To date, used for rapid Coumadin reversal

5/21/2014
7
“PCC therapy leads to a significant correction of INR in ALL trauma patients, regardless of coumadin use…”
Reduction in RBC & FFP needs
CRASH‐2
• “Aim to assess effect of Transexamic acid on death in trauma patients with significant hemorrhage.”
• RCT double blind placebo controlled
• 20,211 pts in 274 hospitals in 40 countries
• Adult patients with or at risk of major hemorrhage– 1 gm over 10 minute loading dose
– 1 gm infusion over 8 hours

5/21/2014
8
Lancet 377(9771): 1096‐101; 2011
Traumatic Neurologic Injury
• ProTECT trial – role of progesterone
• Brain tissue oxygenation as a target for early therapy
• Vasopressor therapy/targets
• Spinal Cord Injury
• Amantadine role in recovery once rehab stage is reached.
ProTECT (Phase III)
• Progesterone for Traumatic Brain Injury: Experimental Clinical Treatment (ProTECT)
• 2008 – Two completed Phase II RCTs that showed benefit
• Progesterone – acts as a neurosteroid
– Protecting damaged cells
• Multi‐center, NIH, randomized, placebo controlled, Phase III trial underway

5/21/2014
9
ProTECT (Phase III)
• Progesterone felt to have several neuroprotective effects:
– Decreases cerebral edema
– Rebuilding of Blood‐brain barrier
– Downregulating inflammatory cascade
– Limiting cellular necrosis/apoptosis
VERY PRELIMINARY –“Vasopressin safe and effective for maintenance of CPP after TBI”
• Multi‐center, prospective cohort study
• 360 patients, 14 centers, 2005‐2009
• 43% of C‐spine had attempt at extubation
– 89% were successful
• High C‐spine 35% attempt
– 88% successful
• 72% no MV @ d/c

5/21/2014
10
Amantadine Hydrochloride
• Aimed at those with severe TBI in a minimally conscious state or vegetative state
• Vegetative state:• 50% regain consciousness at 1 year
• Minimally conscious state • 50% severely disabled at 1 year
• Mechanism of action unknown• Acts as an indirect dopamine agonist
• 184 patients, 11 sites, 3 countries
• Vegetative or minimally conscious state for 4‐16 wks after TBI
• 4 week course of drug or placebo
• No difference in adverse effects
Injury Specific
• Rib fracture stabilization
• Vascular trauma
– Shunts
– Balloon occlusion control of major injury
– Stent injuries

5/21/2014
11
Rib Fractures
Kaewlai R et al. Radiographics 2008;28:1555-1570
©2008 by Radiological Society of North America
Rib Fixation
• >20 studies
• Indications debated
– ?Pain
– ?Flail chest
– ?non‐union at what time point
• Markov analysis
• Showed ORIF is cost‐effective

5/21/2014
12
Vascular Injuries
• Shunts• Extremity injury
• Balloon Occlusion• Venous Injuries
• Covered Stents• Subclavian Artery
• Aorta
• Vena Cava
Shunts
Tourniquets, vascular shunts, and endovascular technologies: Esoteric or essential? A report from the 2011 AAST Military Liaison Panel.
J Trauma Acute Care Surg. 2012 Jul;73(1):282‐285.
Gaining Control IVC
Traditional
• Manual tamponade• Sponge stick
• Hard to maintain while repairing
• Flatten IVC• Complicated repair
• Urinary/Fogarty balloons• Still have to disrupt
hematoma
• Ligation• High amputation rate
• Very morbid
Cattell Maneuver

5/21/2014
13
Gaining Control IVC
Traditional
• Manual tamponade• Sponge stick
• Hard to maintain while repairing
• Flatten IVC• Complicated repair
• Urinary/Fogarty balloons• Still have to disrupt
hematoma
• Ligation• High amputation rate
• Very morbid
Cattell Maneuver
GB Duodenum andpancreas
Aorta
Cava
Gaining Control IVC
Angiogram Balloon Occlusion
• Percutaneously delivered
• Can be done before opening
• Theoretically reduces blood loss
• Avoids entering hematoma without proximal control
• Reduces operative time
• Allows potential stent options
• Resuscitative endovascular balloon occlusion of the aorta (REBOA)
• Emergence of training courses (ESTARS, BEST)
• Hybrid ORs
• AORTA Study (AAST)

5/21/2014
14
Case 1
• 20 yo male single GSW to L scapula, no exit wound
• Decreased L Radial pulse
• Abnormal BP in L arm
• Initially HD stable
• CXR – no hemothorax
Case 1
• 20 yo male single GSW to L scapula, no exit wound
• Decreased L Radial pulse
• Abnormal BP in L arm
• Initially HD stable
• CXR – no hemothorax
Case 1
• 20 yo male single GSW to L scapula, no exit wound
• Decreased L Radial pulse
• Abnormal BP in L arm
• Initially HD stable
• CXR – no hemothorax

5/21/2014
15
Case 1
• 20 yo male single GSW to L scapula, no exit wound
• Decreased L Radial pulse
• Abnormal BP in L arm
• Initially HD stable
• CXR – no hemothorax
Case 1
• 20 yo male single GSW to L scapula, no exit wound
• Decreased L Radial pulse
• Abnormal BP in L arm
• Initially HD stable
• CXR – no hemothorax
Case 1
• 20 yo male single GSW to L scapula, no exit wound
• Decreased L Radial pulse
• Abnormal BP in L arm
• Initially HD stable
• CXR – no hemothorax

5/21/2014
16
L subclavian artery injury
Proximal control – anterior thoracotomythrough 3rd ICS
Distal control – often need supraclavicularincision
Trap door
• Alternative for access for L subclavian/Common carotid
• Poor exposure
• Significant morbidity incision
Considerations
• Pain
• Clavicular stability
• Not surgically that easy
• Takes time to expose

5/21/2014
17
Subclavian Artery Repair
Dr. Paul Tahalele, Indonesia
Case 2
• 20 yo male multiple large caliber GSW to back, chest, LE
• Presented in extremis with hemoptysis
• Emergently intubated & resuscitated
• Injuries included: • L subclavian artery injury• L IJ transection• Esophageal Injury x 2• Mandible fracture• LE compartment syndrome• UE fractures
Subclavian Stent Considerations
• Hemodynamically stable
• Focal injury
• Endovascular‐surgical hybrid suite
• Have to be able to traverse injury with guidewire
• Ready availability of trauma/vascular surgeon

5/21/2014
18
Subclavian Endovascular Repair
• >20 papers in last 12 months
• “Endovascular management of peripheral artery trauma in patients presenting in hemorrhagic shock.” (J Cardiovasc Surg Aug 2012)– 18 patients
– All were technical successes
• Experience is limited
Summary
• A number of important advances in last 12 months
• Exciting time
• More to come…
References
• Bellal J, Amini A, Friese RS, et al. Factor IX complex for the correction of coagulopathy. J Trauma. 2011 Dec;72(4):828‐834.
• Bhatnagar A, Mayberry J, Nirula R. Rib fracture fixation for flail chest: what is the benefit? J Am Coll Surg. 2012 Aug;215(2):201‐5.
• Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003 Jun;54(6):1127‐30. • Callcut RA, Cotton BA, Muskat P, et al. Defining when to initiate massive transfusion: A validation study of
individual massive transfusion triggers in PROMMTT patients. J Trauma Acute Care Surg. 2013 Jan;74(1):59‐65.• CRASH‐2 Trial Collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion
in trauma patients with significant haemorrhage (CRASH‐2): a randomised, placebo‐controlled trial. Lancet. 2010 Jul 3;376(9734):23‐32.
• CRASH‐2 Trial Collaborators. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH‐2 randomised controlled trial .Lancet. 2011 Mar26;377(9771):1096‐1101.
• Duchense JC, Hunt JP, Whal G, et al. Review of current blood transfusion strategies in a mature level I trauma center: were we wrong for the last 60 years? J Trauma. 2008;65:272‐278.
• Giacino JT, White J, Bagiella E, et al. Placebo Controlled Trial of Amantadine for Severe Traumatic Brain Injury. N Engl J Med. 2012 Mar 1;366(9):819‐26.
• Holcomb JB, Fox EE, Scalea TM, et al. Current opinion on catheter‐based hemorrhage control in trauma patients. J Trauma Acute Care Surg. 2014 Mar;76(3):888‐93
• Kornblith LZ, Kutcher ME, Callcut RA, et al. Mechanical ventilation weaning and extubation after spinal cord injury. J Trauma Acute Care Surg. 2013 Dec;75(6):1060‐9.
• Sperry JL, Ochoa JB, Gunn SR, et al. An FFP:PRBC transfusion ratio >= 1:1.5 is associated with a lower risk of mortality after massive transfusion. J Trauma.2008 Nov;65(5):986‐93.
• Wright DW, Kellerman AL, Hertzberg VS, et al. ProTECT: a randomized clinical trial of progesterone for acute traumatic brain injury. Ann Emerg Med. 2007 Apr;49(4):391‐402







