
Philippe Van der Linden MD, PhD
Transfusion & Mortality

In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Nordic Pharma SA Fresenius-Kabi GmbH
Janssen-Cilag SA
Conflict of Interest Disclosure
Blood Transfusion in Cardiac Surgery Patients: Effects on Mortality, Morbidity & Cost
From Murphy GJ et al. Circulation 116: 2544-52, 2007.
ü Retrospective cohort study (04/1996 – 12/2003; N=8,598)
ü Primary outcomes • Infection: respiratory, wound infection or septicemia • Ischemia: myocardial infarction, permanent or transient stroke, renal complication (creat > 200 mmol/L or requirement for dialysis)
ü Costs: ICU and hospital stay, blood products
ü Associations estimated by regression modeling with adjustment for potential confounding

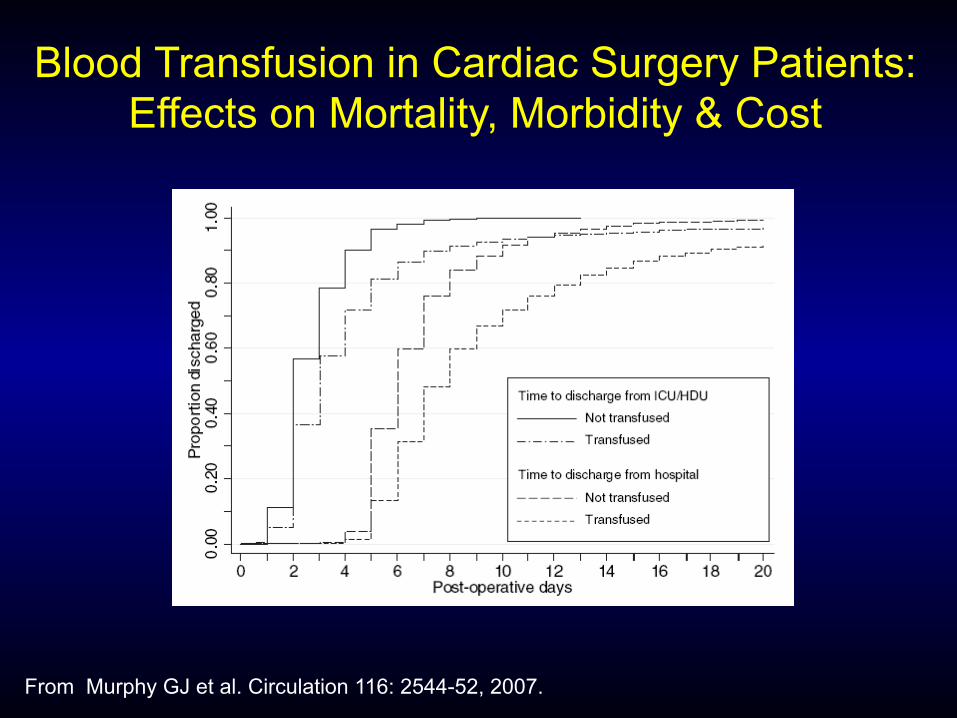
Blood Transfusion in Cardiac Surgery Patients: Effects on Mortality, Morbidity & Cost
From Murphy GJ et al. Circulation 116: 2544-52, 2007.
Overall transfusion rate: 57%
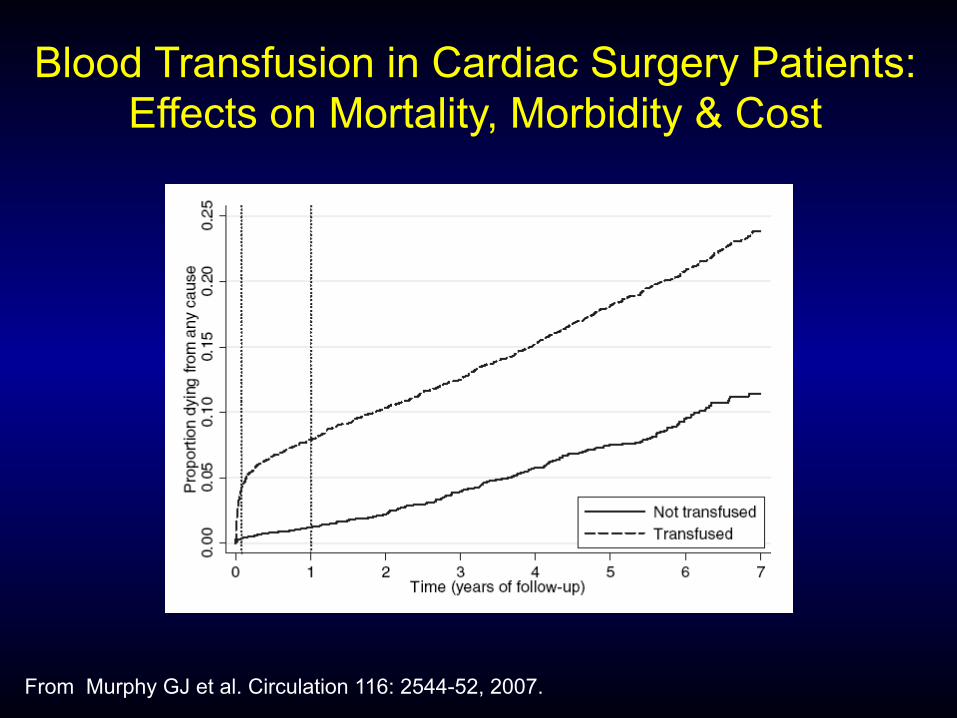
Blood Transfusion in Cardiac Surgery Patients: Effects on Mortality, Morbidity & Cost
From Murphy GJ et al. Circulation 116: 2544-52, 2007.
Blood Transfusion in Cardiac Surgery Patients: Effects on Mortality, Morbidity & Cost
From Murphy GJ et al. Circulation 116: 2544-52, 2007.

Blood Transfusion & Postoperative Morbi-Mortality After Cardiac Surgery
From Loor G et al. J Thorac Cardiovasc Surg 144:538-46, 2012.
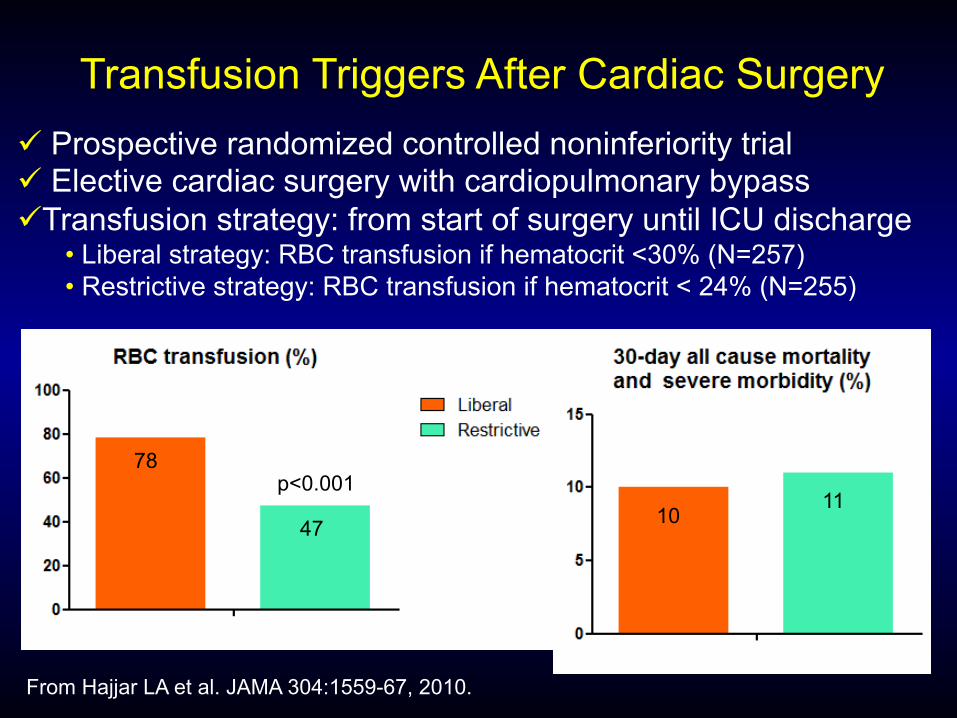
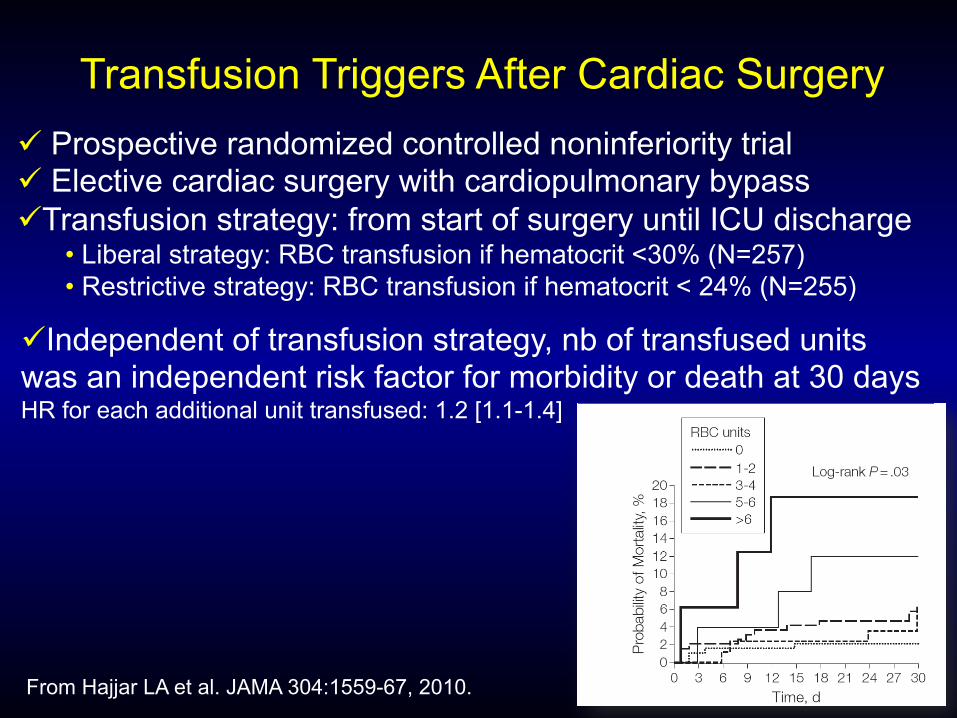
Transfusion Triggers After Cardiac Surgery
From Hajjar LA et al. JAMA 304:1559-67, 2010.
ü Prospective randomized controlled noninferiority trial ü Elective cardiac surgery with cardiopulmonary bypass
ü Transfusion strategy: from start of surgery until ICU discharge • Liberal strategy: RBC transfusion if hematocrit <30% (N=257) • Restrictive strategy: RBC transfusion if hematocrit < 24% (N=255)
ü Primary endpoint: : 30-day all-cause of mortality & severe morbidity (cardiogenic shock, ARDS or acute renal failure)
ü Noninferiority margin was predefined at -8%
Transfusion Triggers After Cardiac Surgery ü Prospective randomized controlled noninferiority trial ü Elective cardiac surgery with cardiopulmonary bypass ü Transfusion strategy: from start of surgery until ICU discharge
• Liberal strategy: RBC transfusion if hematocrit <30% (N=257) • Restrictive strategy: RBC transfusion if hematocrit < 24% (N=255)
From Hajjar LA et al. JAMA 304:1559-67, 2010.
10 11
78
47
p<0.001
Transfusion Triggers After Cardiac Surgery ü Prospective randomized controlled noninferiority trial ü Elective cardiac surgery with cardiopulmonary bypass ü Transfusion strategy: from start of surgery until ICU discharge
• Liberal strategy: RBC transfusion if hematocrit <30% (N=257) • Restrictive strategy: RBC transfusion if hematocrit < 24% (N=255)
From Hajjar LA et al. JAMA 304:1559-67, 2010.
ü Independent of transfusion strategy, nb of transfused units was an independent risk factor for morbidity or death at 30 days HR for each additional unit transfused: 1.2 [1.1-1.4]

Transfusion Thresholds & Other Strategies for Guiding Allogeneic
RBC Transfusion
ü Results: restrictive transfusion strategies • ê risk of receiving RBC transfusion (RR: 0.57; 95% CI: 0.49 to 0.65)
• ê volume of transfused RBCs (-1.30; 95% CI: -1.85 tp -0.75)
• No impact on 30-day mortality (RR:0.97; 95% CI: 0.81 to1.16)
• No impact on cardiac events, myocardial infarction, stroke,
rebleeding, sepsis / bacteremia, pneumonia / wound infection,
thromboembolism, renal failure, and mental confusion
• Functional recovery: not assessed
From Carson JL et al. Cochrane Database of Systematic Review, 2016 Oct 12, CD002042.
31 trials – 12,587 patients
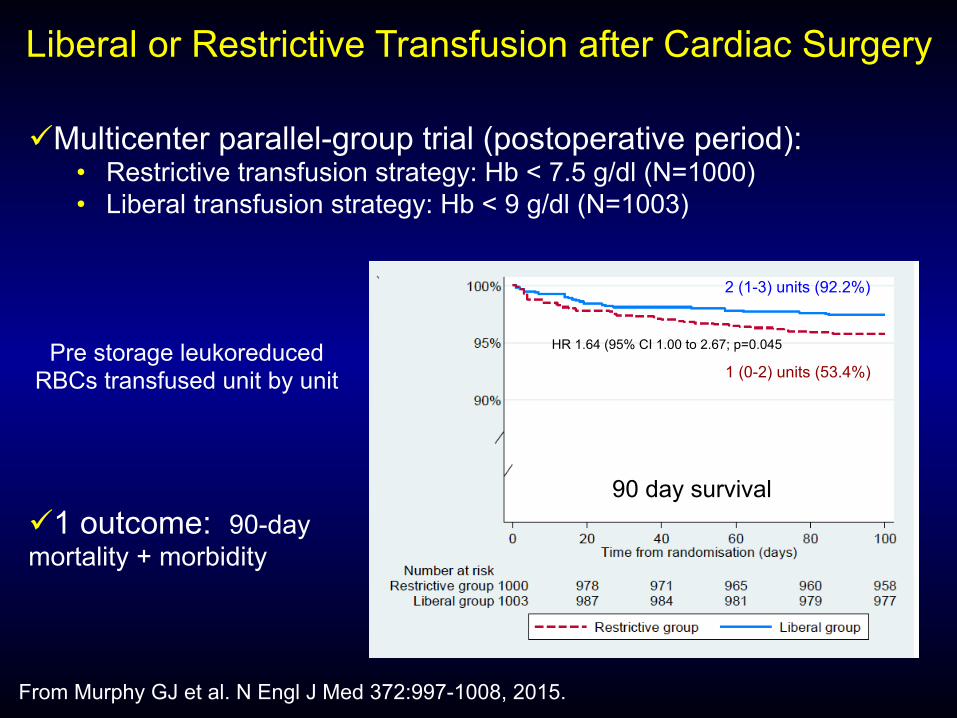
Liberal or Restrictive Transfusion after Cardiac Surgery
From Murphy GJ et al. N Engl J Med 372:997-1008, 2015.
ü Multicenter parallel-group trial (postoperative period): • Restrictive transfusion strategy: Hb < 7.5 g/dl (N=1000) • Liberal transfusion strategy: Hb < 9 g/dl (N=1003)
ü 1 outcome: 90-day mortality + morbidity
Pre storage leukoreduced RBCs transfused unit by unit
2 (1-3) units (92.2%)
1 (0-2) units (53.4%)
1 outcome 2 (1-3) units (92.2%)
1 (0-2) units (53.4%)
90 day survival
HR 1.64 (95% CI 1.00 to 2.67; p=0.045

From Hovaguimian F & Myles PS. Anesthesiology 125:46-61, 2016.
ü Context-specific systematic review and meta-analysis of RCTs: effects of restrictive transfusion strategies
ü Cardiac/vascular procedures (8 studies; N=3,322 patients) 1. Risk of events reflecting inadequate D02: 1.09 [0.91 to 1.22] 2. Risk of mortality: 1.39 [0.95 to 2.04] 3. Composite events (1+2):

Transfusion Medicine Goodnough LT et al, NEJM 340:438-444,1999.
« It is unlikely that any level of hemoglobin can be used as a universal threshold for transfusion ».
Transfusion Thresholds Barr PJ, Bailie KEM NEJM 365; 26: 2532-3, 2011.
« The decision to transfuse should be guided by an assessment of individual patient on the basis of a combination of symptoms, signs, lab measures and not by a single hemoglobin level ».
Association Between Blood Transfusion & Morbi-Mortality After Major Surgery
Is transfusion the causal event leading to worse outcome or rather a marker for a sicker patient population that is more
likely to undergo transfusion for many reasons?

Incidence & Importance of Anemia in Patients Undergoing Cardiac Surgery in UK
From Klein AA et al. Anaesthesia 71:627-35, 2016.
ü National service audit (2010-2012):12/35 UK cardiac surgery centers provided data
ü 20% of the patients (4754/23,800) did not have preop Hb ü Incidence of anemia (WHO definition): 31% (23 to 45%) ü Regional variation remained an independent effect
ü Independent association of anemia with transfusion, mortality, and hospital stay
A 10g/L ê in Hb was associated with a 43% é in the risk of transfusion and a 16% é in the risk of death (both p<0.001)
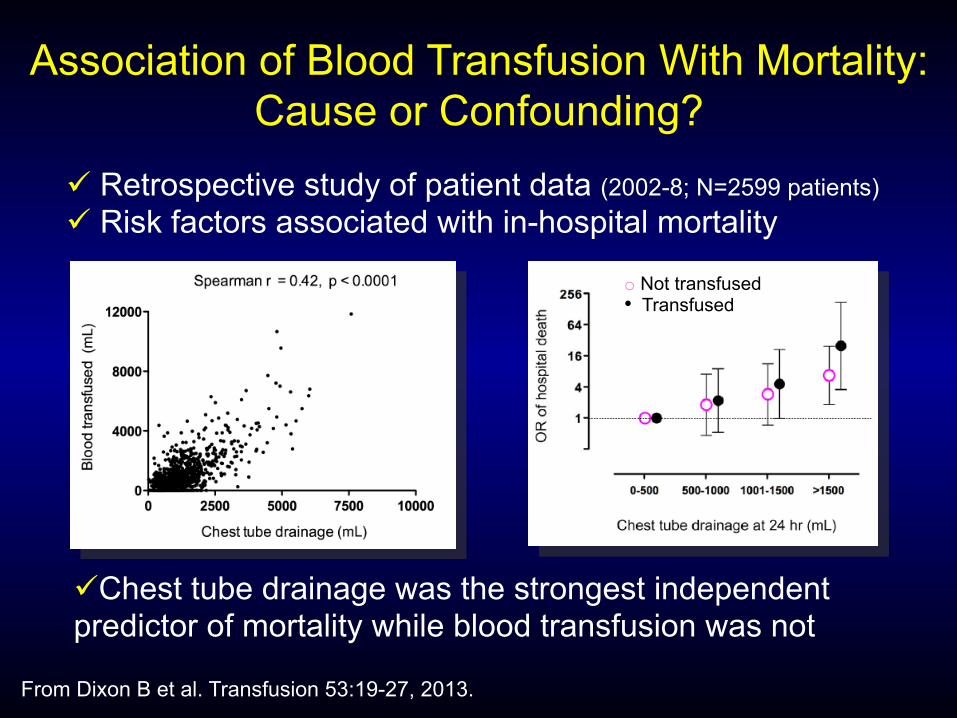
Association of Blood Transfusion With Mortality: Cause or Confounding?
From Dixon B et al. Transfusion 53:19-27, 2013.
ü Retrospective study of patient data (2002-8; N=2599 patients) ü Risk factors associated with in-hospital mortality
ü Chest tube drainage was the strongest independent predictor of mortality while blood transfusion was not
o Not transfused • Transfused
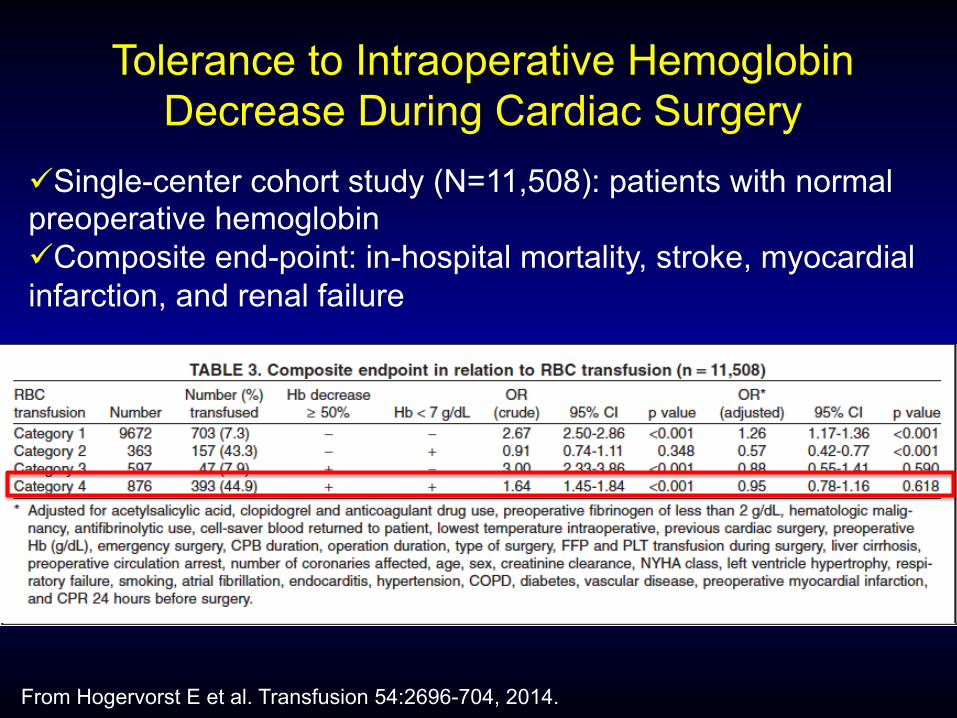
Tolerance to Intraoperative Hemoglobin Decrease During Cardiac Surgery
From Hogervorst E et al. Transfusion 54:2696-704, 2014.
ü Single-center cohort study (N=11,508): patients with normal preoperative hemoglobin ü Composite end-point: in-hospital mortality, stroke, myocardial infarction, and renal failure

Indications For RBC Transfusion In Pediatric Cardiac Surgery: Effects on Outcome
ü Indications for RBC transfusion: • To maintain a predefined hematocrit on bypass
• To treat perioperative blood loss and/or inadequate oxygen delivery
ü Hypothesis: indication for RBC transfusion may impact the
effects of transfusion on postoperative morbi-mortality in
pediatric cardiac surgery
From Willems A et al. Eur J Cardiothorac Surg 45:1050-7, 2014.

ü Retrospective cohort study (2006-2009; N=855)
ü Transfused children (N=568) • Maintenance on-bypass hct of 24% ( CPB driven: N=358) • Hemorrhage or O2 delivery increase (therapeutic: N= 210)
ü Primary outcome: composite measure including either hospital
death and/or the presence of at least 2 of the following events: • Pulmonary failure (mechanical ventilation duration > 75th percentile) • Prolonged inotropic support (inotropes > 5 µg/kg.min for more than 48h) • Renal failure (reduction of postop creat clearance ≥ 75% from baseline)
From Willems A et al. Eur J Cardiothorac Surg 45:1050-7, 2014.
Indications For RBC Transfusion In Pediatric Cardiac Surgery: Effects on Outcome
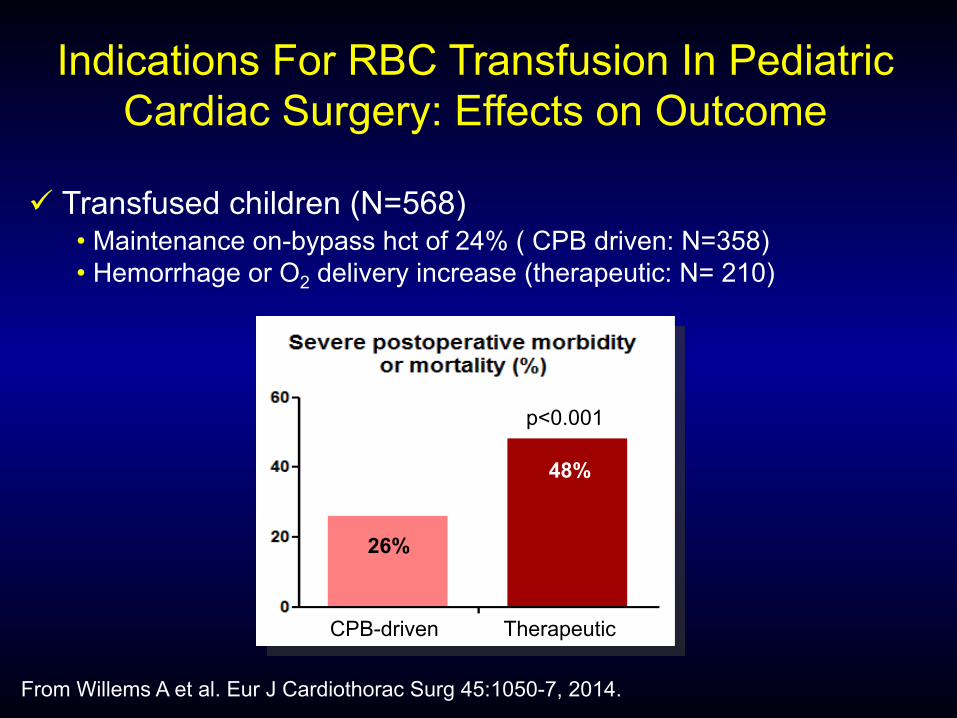
ü Transfused children (N=568) • Maintenance on-bypass hct of 24% ( CPB driven: N=358) • Hemorrhage or O2 delivery increase (therapeutic: N= 210)
CPB-driven Therapeutic
p<0.001
48%
26%
From Willems A et al. Eur J Cardiothorac Surg 45:1050-7, 2014.
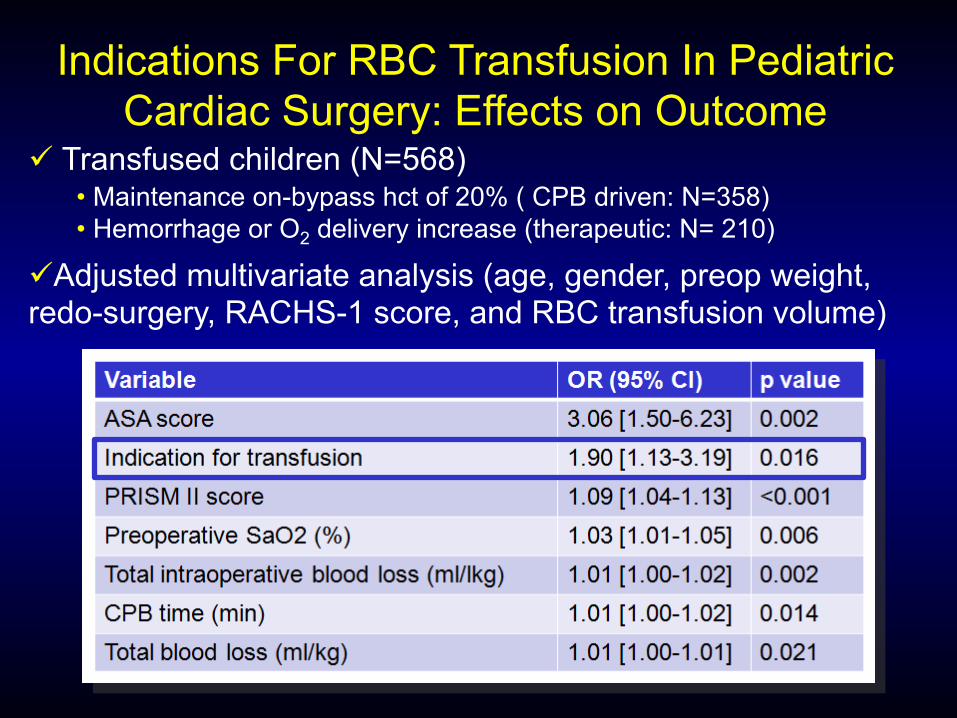
Indications For RBC Transfusion In Pediatric Cardiac Surgery: Effects on Outcome

ü Transfused children (N=568) • Maintenance on-bypass hct of 20% ( CPB driven: N=358) • Hemorrhage or O2 delivery increase (therapeutic: N= 210)
0 50 100 1500
50
100
150
0 5 10 15 20 25 30
86
88
90
92
94
96
98
100
Time (days)
Survival probability (%)
Number at risk
CPB driven transfusion group:
356 348 220 104 66 39 29Therapeutic transfusion group:
208 199 164 106 83 64 48
CPB driven transfusion group
Logrank p < 0.05
Therapeutic transfusion group
From Willems A et al. Eur J Cardiothorac Surg 45:1050-7, 2014.
Indications For RBC Transfusion In Pediatric Cardiac Surgery: Effects on Outcome
ü Transfused children (N=568) • Maintenance on-bypass hct of 20% ( CPB driven: N=358) • Hemorrhage or O2 delivery increase (therapeutic: N= 210)
ü Adjusted multivariate analysis (age, gender, preop weight, redo-surgery, RACHS-1 score, and RBC transfusion volume)
Indications For RBC Transfusion In Pediatric Cardiac Surgery: Effects on Outcome

ü Retrospective cohort study (2006-2012; N=1215)
ü Studied population (N=854) • No transfusion (N=439) • Transfused to maintain an on-bypass hct of 24% (N= 415)
ü Primary outcome: composite measure including either hospital
death and/or the presence of at least 2 of the following events: • Pulmonary failure (mechanical ventilation duration > 75th percentile) • Prolonged inotropic support (inotropes > 5 µg/kg.min for more than 48h) • Renal failure (reduction of postop creat clearance ≥ 75% from baseline)
From Willems A et al. Anesth Analg 123:420-9, 2016.
Does On-bypass RBC Transfusion Affect Outcome In Pediatric Cardiac Surgery

ü Retrospective cohort study (2006-2012; N=1215)
ü Studied population (N=854) • No transfusion (N=439) • Transfused to maintain an on-bypass hct of 24% (N= 415)
Does On-bypass RBC Transfusion Affect Outcome In Pediatric Cardiac Surgery
0
10
20
30
40
50
Composite primary outcome (%)
Not transfusedCPB transfused
P=0.538
From Willems A et al. Anesth Analg 123:420-9, 2016.

ü The real impact of RBC transfusion on postoperative
morbi-mortality remains to be determined.
ü Efforts should be done to modify clinical conditions
asociated with blood transfusion • Preoperative anemia
• Perioperative blood losses
Transfusion & Mortality Conclusions







