Download - The Vermont Primary Care Workforce
The Vermont Primary Care Workforce2012 SNAPSHOT
wOrkfOrce SHOwS imPrOvemeNT buT SHOrTAge iN AdulT PrimArY cAre PerSiSTS

About vermont AHec
The Vermont Area Health Education Centers (AHEC) Program, in collaboration with many partners, improves access to quality health care through its focus on workforce development. AHEC work includes: support for pipeline programs in health careers awareness and exploration for Vermont youth; support for and engagement of health professions students at the University of Vermont and residents at Fletcher Allen Health Care; and support to help recruit and retain a high-quality healthcare workforce in Vermont.
In addition to health workforce development, AHEC brings educational and quality improvement programming to Vermont’s primary care practitioners and supports community health education.
AHEC believes that success in healthcare innovation, transformation, and reform depends on an adequate supply and distribution of well-trained healthcare professionals so that all Vermonters, including those who live in rural areas and underserved populations, have access to high-quality care.
AHec History & Partners
The Vermont Area Health Education Centers Program was established in 1996 by the Office of Primary Care at the University of Vermont College of Medicine. AHEC is funded through multiple grants and contracts including: Federal HRSA Title VII, State of Vermont, Vermont Department of Health, University of Vermont College of Medicine, Fletcher Allen Health Care, Vermont’s 13 community hospitals, private foundations, and individual contributors.
The statewide infrastructure of AHEC consists of a program office at the University of Vermont College of Medicine and three regional centers which are each a 501(c)(3), non-profit organization. AHEC is a dynamic, academic-community partnership linking the University of Vermont College of Medicine and communities in every county of the state.
Acknowledgments
We thank all those involved in primary care in Vermont who helped produce this report, including: the Vermont primary care practices who provided practice- and practitioner-level information; Helen Riehle, Judy Wechsler, and Tammy Johnson of Champlain Valley AHEC; Marty Hammond, Susan White, and Doreen Moran of Southern Vermont AHEC; Nicole LaPointe and Mary E. Fleck of Northeastern Vermont AHEC; the UVM AHEC staff; and Laurie Hurowitz, PhD, Health Workforce Researcher.
TAble Of cONTeNTS
Primary Care Workforce Summary 2012 .................................... 1
Background, Benchmarks, Challenges, Ongoing Work ............. 2
Primary Care Practitioners – Statewide Findings 2012
Primary Care Practice Sites ................................................... 4
From Individual Practitioners to FTEs .................................. 4
Primary Care Practitioners (in FTEs)
By Specialty .................................................................... 5
Limiting New Patients by Specialty .............................. 6
By Region ....................................................................... 7
Limiting New Patients by Region ................................. 9
2012 Survey Findings by AHEC Region
Northeastern Vermont ....................................................... 10
Champlain Valley ................................................................ 11
Southern Vermont .............................................................. 12
Endnotes ..................................................................................... 13
contact AHec
university of vermont college of medicine Office of Primary care AHec Program
Burlington, VT 802-656-2179www.vtahec.org
Northeastern vermont Area Health education center
St. Johnsbury, VT 802-748-2506www.nevahec.org
champlain valley Area Health education center
St. Albans, VT802-527-1474www.cvahec.org
Southern vermont Area Health education center
Springfield, VT 802-885-2126www.svahec.org
www.vtahec.org 1
•
Windham
WindsorRutland
Bennington
Washington
Orange
Caledonia
LamoilleOrleans
Essex
•
Franklin
Chittenden
Addison
•
Grand Isle
•
WorkforceShowsImprovementbutShortageinAdultPrimaryCarePersists
PrimArY cAre wOrkfOrce SummArY 2012
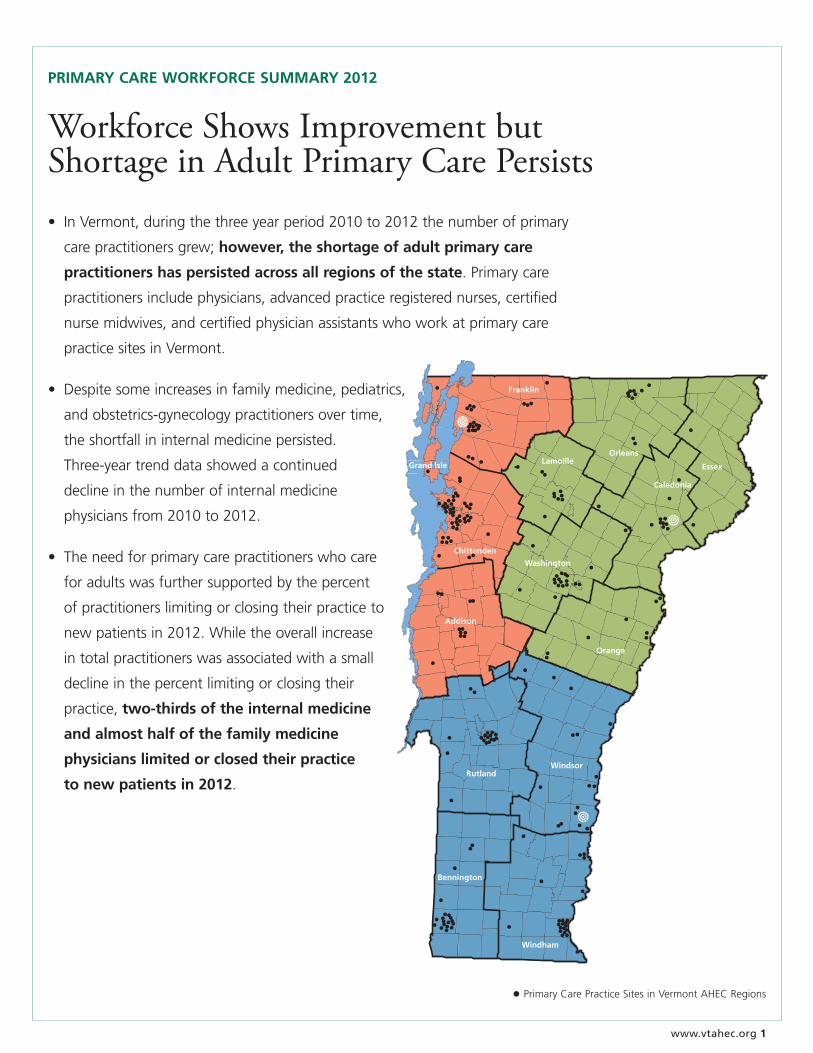
• InVermont,duringthethreeyearperiod2010to2012thenumberofprimary
carepractitionersgrew;however, the shortage of adult primary care
practitioners has persisted across all regions of the state.Primarycare
practitionersincludephysicians,advancedpracticeregisterednurses,certified
nursemidwives,andcertifiedphysicianassistantswhoworkatprimarycare
practicesitesinVermont.
• Despitesomeincreasesinfamilymedicine,pediatrics,
andobstetrics-gynecologypractitionersovertime,
theshortfallininternalmedicinepersisted.
Three-yeartrenddatashowedacontinued
declineinthenumberofinternalmedicine
physiciansfrom2010to2012.
• Theneedforprimarycarepractitionerswhocare
foradultswasfurthersupportedbythepercent
ofpractitionerslimitingorclosingtheirpracticeto
newpatientsin2012.Whiletheoverallincrease
intotalpractitionerswasassociatedwithasmall
declineinthepercentlimitingorclosingtheir
practice,two-thirds of the internal medicine
and almost half of the family medicine
physicians limited or closed their practice
to new patients in 2012.
• PrimaryCarePracticeSitesinVermontAHECRegions

2 www.vtahec.org
background: Annual AHec Survey
Inthisreportweexaminetheclinicalhoursofprimarycarepractitioners(PCPs)includingphysicians(MD/DOs),advancedpractiticeregisterednurses(APRNs),certifiednursemidwives(CNMs),andcertifiedphysicianassistants(PA-Cs)inprimarycarepractices.AnalysesarepresentedbyprimarycarespecialtytoidentifytheneedsofdifferentpopulationsofVermonters:
• familymedicinepractitionersservechildrenthroughadults;
• generalinternalmedicinepractitionersserveadolescentsandadults;
• generalpediatricpractitionersservechildrenandadolescents;and
• generalobstetrics-gynecologypractitionersserveadolescentsandadultwomen.
RegionalanalysesexaminetheprimarycareworkforceindifferentpartsofVermont,includingcountyandmulti-countyregions:NortheasternVermont,ChamplainValley,andSouthernVermont.
Thisreportisasnapshotofthenet changesintotalPCPsfromyeartoyearbetween2010and2012.Itspurposeistoidentifyareaswheretheprimarycareworkforceisadequateandwherethereareshortfalls.ThesupplyofpractitionersisexaminedbyprimarycarespecialtybothstatewideandwithinregionsofVermont.
benchmarks: How many Practitioners do we Need?
Forthis2012report,wearemaintainingthesamemethodasusedinpreviousyearsforanalyzingtheprimarycareworkforce,employingnationalbenchmarkstodeterminehowmanypractitionersareneeded.Astheprimarycareservicesevolveandasnewbenchmarksaredeveloped,1,2,3wewillupdateouranalyses(seeEndnotes,page13,forinformationonthecurrentmethod).Someofthefactorswhichputpressureonolderbench-marksincludetheimplementationofhealthcarereformsbothinVermontandnationally,whichwilllikelyincreasethenumberofpeoplewhowillbeseekingprimarycare.Demographicanalysesalsoshowanagingpopulationwhichisgenerallyassociatedwithincreasedneedformedicalcare.
Inthiseraofhealthcarereform,theorganizationofthehealthcaredeliverysystemisalsochanging.4Inthecurrentreport,weincludephysicians,advancedpracticeregisterednurses,physicianassistants,andcertifiednursemidwives.AsmoreVermontpracticesemployateamapproachtodelivercare,andasmoreprimarycarepracticesbecomemedicalhomes,additionaldisciplines(professions)mayneedtobeaddedtotheanalyses.ChangesinthedeliveryofcaremayalsochangetheroleofcurrentPCPs;thisshouldalsobereflectedinfutureworkforcebenchmarks.
Vermonthasseenaveryrapidadoptionofelectronicmedicalrecords(EMR)overthepastthreeyears.Whilethismayleadtoadvancesinsafetyandefficiencydowntheroad,theprocessofchoosing,installing,andlearningtouseanEMRtakesaconsiderablecommitmentoftimeandenergyonthepartofeverymemberofapractice.ItisnotyetclearifEMRadoptionwillleadtolongtermchangesinthecapacityofPCPsorprimarycarepractice.5
1. KuenningT.NegotiatedRulemakingCommittee:DesignationofMedicallyUnderservedPopulationsandHealthProfessionalShortageAreas.PresentedattheBi-StatePrimaryCare Meeting,Montpelier,VT,12/15/2011.2. www.healthworkforce.unc.edu/documents/PF_FAQ_Aug2012.pdf,11/26/2012.3. www.annfammed.org/content/10/6/503.full.pdf+html,12/5/2012.4. Bielaszka-DuVernayC.Vermont’sBlueprintforMedicalHomes,CommunityHealthTeams,andBetterHealthatLowerCost.HealthAffairs,2011;30(3):383-386.5. HillestadR,BigelowJ,BowerA,GirosiF,MeiliR,ScovilleR,TaylorR.Canelectronicmedicalrecordsystemstransformhealthcare?Potentialhealthbenefits,savings,andcosts. HealthAffairs,2005Sep-Oct;24(5):1103-17.
www.vtahec.org �
challenges: maintaining/increasing the Primary care workforce
Therearestillspecialchallengestomaintainingand,whereneeded,increasingtheprimarycareworkforceinVermont:
• financialandotherpressuresonhealthcaretrainees,includingmedicalstudentsandresidents,nursepractitioners,andphysicianassistants,tosub-specializeratherthanchooseprimarycare;
• reimbursementofandworkloadpressuresonprimarycarepractitioners;
• theagingofVermontprimarycarepractitioners,especiallyinternalmedicinephysicians;6
• theimpactoftheelderlypopulationbecominganincreasinglylargerproportionofthepopulation,asthisgroupisassociatedwithincreasedneedformedicalcare;and
• competitionfromotherstatesthatarealsoworkingtoincreasetheirprimarycareworkforce.
Ongoing work: Strengthening the Primary care workforce
ThereissignificantactivityunderwayinVermonttosupportdevelopmentofthenextgenerationofhealthcareworkers.ExamplesincludeAHEC’shealthcarecareerexplorationprogramsinmiddleandhighschool,andthesupportandengagementofhealthcareprofessionsstudentsattheUniversityofVermontandresidentsatFletcherAllenHealthCare.TheseprogramsencouragetraineestoconsiderfuturepracticeinhealthcareersinVermont.
TheVermontBlueprintforHealthisworkingtochangethewaywedeliverhealthcare,particularlyintheadvancedprimarycarepracticeinitiativewhichisprovidinganopportunitytoexplorenovelandmoreefficientwaystoimprovehealth.
Thereareconsiderablecommunityandstatewideactivitiesandprogramstohelprecruitandretaintheprimarycareworkforce,includingthestate-funded,AHEC-administeredVermontEducationalLoanRepaymentProgramforPrimaryCarePractitioners.Thesefundshelptoreduceapractitioner’seducationaldebtinexchangeforacommitmenttopracticeinVermont.Todate,overone-quarterofVermont’sprimarycarephysicianshavebenefittedfromthisprogram.
6. VermontDepartmentofHealth.2010PhysicianSurveyStatisticalReport,Burlington,VT,Aug2011.NOTE:Reportonthe2012surveyofindividualphysiciansisexpectedin2013.
� www.vtahec.org
PrimArY cAre PrAcTiTiONerS – STATewide fiNdiNgS 2012
Primary care Practice Sites
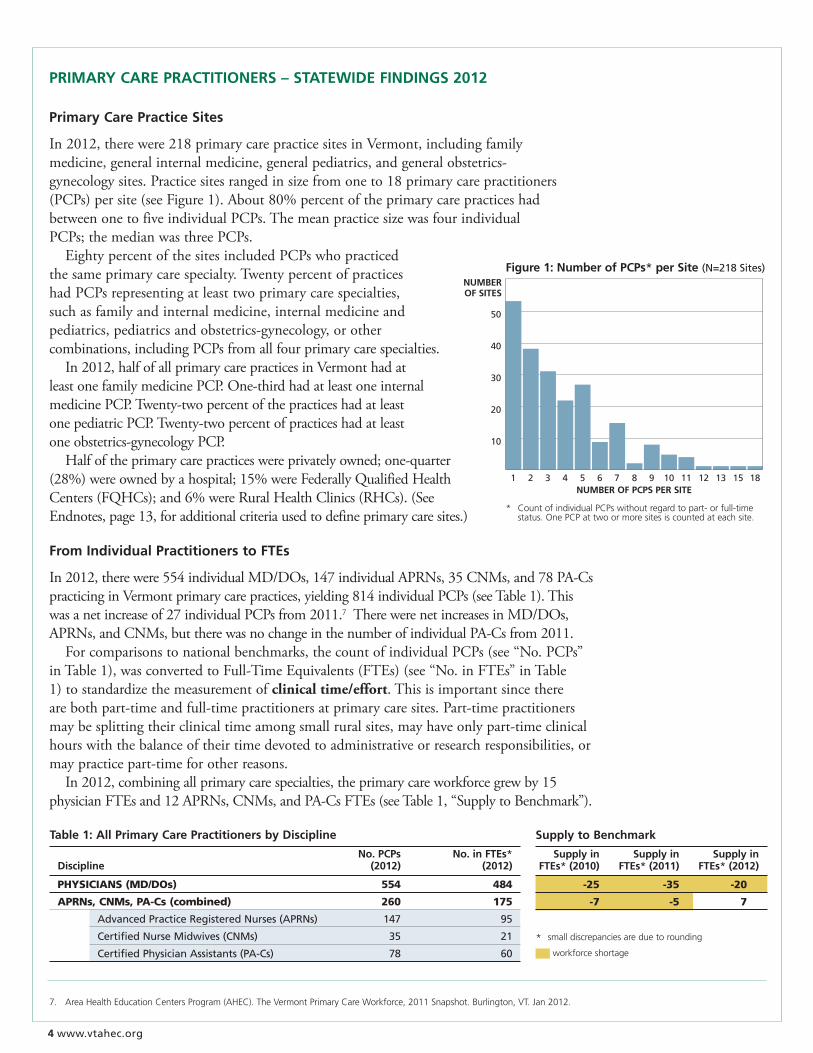
In2012,therewere218primarycarepracticesitesinVermont,includingfamilymedicine,generalinternalmedicine,generalpediatrics,andgeneralobstetrics-gynecologysites.Practicesitesrangedinsizefromoneto18primarycarepractitioners(PCPs)persite(seeFigure1).About80%percentoftheprimarycarepracticeshadbetweenonetofiveindividualPCPs.ThemeanpracticesizewasfourindividualPCPs;themedianwasthreePCPs. EightypercentofthesitesincludedPCPswhopracticedthesameprimarycarespecialty.TwentypercentofpracticeshadPCPsrepresentingatleasttwoprimarycarespecialties,suchasfamilyandinternalmedicine,internalmedicineandpediatrics,pediatricsandobstetrics-gynecology,orothercombinations,includingPCPsfromallfourprimarycarespecialties. In2012,halfofallprimarycarepracticesinVermonthadatleastonefamilymedicinePCP.One-thirdhadatleastoneinternalmedicinePCP.Twenty-twopercentofthepracticeshadatleastonepediatricPCP.Twenty-twopercentofpracticeshadatleastoneobstetrics-gynecologyPCP. Halfoftheprimarycarepracticeswereprivatelyowned;one-quarter(28%)wereownedbyahospital;15%wereFederallyQualifiedHealthCenters(FQHCs);and6%wereRuralHealthClinics(RHCs).(SeeEndnotes,page13,foradditionalcriteriausedtodefineprimarycaresites.)
from individual Practitioners to fTes
In2012,therewere554individualMD/DOs,147individualAPRNs,35CNMs,and78PA-CspracticinginVermontprimarycarepractices,yielding814individualPCPs(seeTable1).Thiswasanetincreaseof27individualPCPsfrom2011.7TherewerenetincreasesinMD/DOs,APRNs,andCNMs,buttherewasnochangeinthenumberofindividualPA-Csfrom2011. Forcomparisonstonationalbenchmarks,thecountofindividualPCPs(see“No.PCPs”inTable1),wasconvertedtoFull-TimeEquivalents(FTEs)(see“No.inFTEs”inTable1)tostandardizethemeasurementofclinical time/effort.Thisisimportantsincetherearebothpart-timeandfull-timepractitionersatprimarycaresites.Part-timepractitionersmaybesplittingtheirclinicaltimeamongsmallruralsites,mayhaveonlypart-timeclinicalhourswiththebalanceoftheirtimedevotedtoadministrativeorresearchresponsibilities,ormaypracticepart-timeforotherreasons. In2012,combiningallprimarycarespecialties,theprimarycareworkforcegrewby15physicianFTEsand12APRNs,CNMs,andPA-CsFTEs(seeTable1,“SupplytoBenchmark”).
7. AreaHealthEducationCentersProgram(AHEC).TheVermontPrimaryCareWorkforce,2011Snapshot.Burlington,VT.Jan2012.
Table 1: All Primary care Practitioners by discipline
No. PcPs No. in fTes* discipline (2012) (2012)
Physicians(MD/DOs) 554 484
aPRns,cnMs,Pa-cs(combined) 260 175
Advanced Practice Registered Nurses (APRNs) 147 95
Certified Nurse Midwives (CNMs) 35 21
Certified Physician Assistants (PA-Cs) 78 60
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
-25 -35 -20
-7 -5 7
* smalldiscrepanciesareduetorounding
workforceshortage
50
40
30
20
10
1 2 3 4 5 6 7 8 9 10 11 12 13 15 18
figure 1: Number of PcPs* per Site (N=218 Sites)
* CountofindividualPCPswithoutregardtopart-orfull-time status.OnePCPattwoormoresitesiscountedateachsite.
Number Of PcPS Per SiTe
Number Of SiTeS
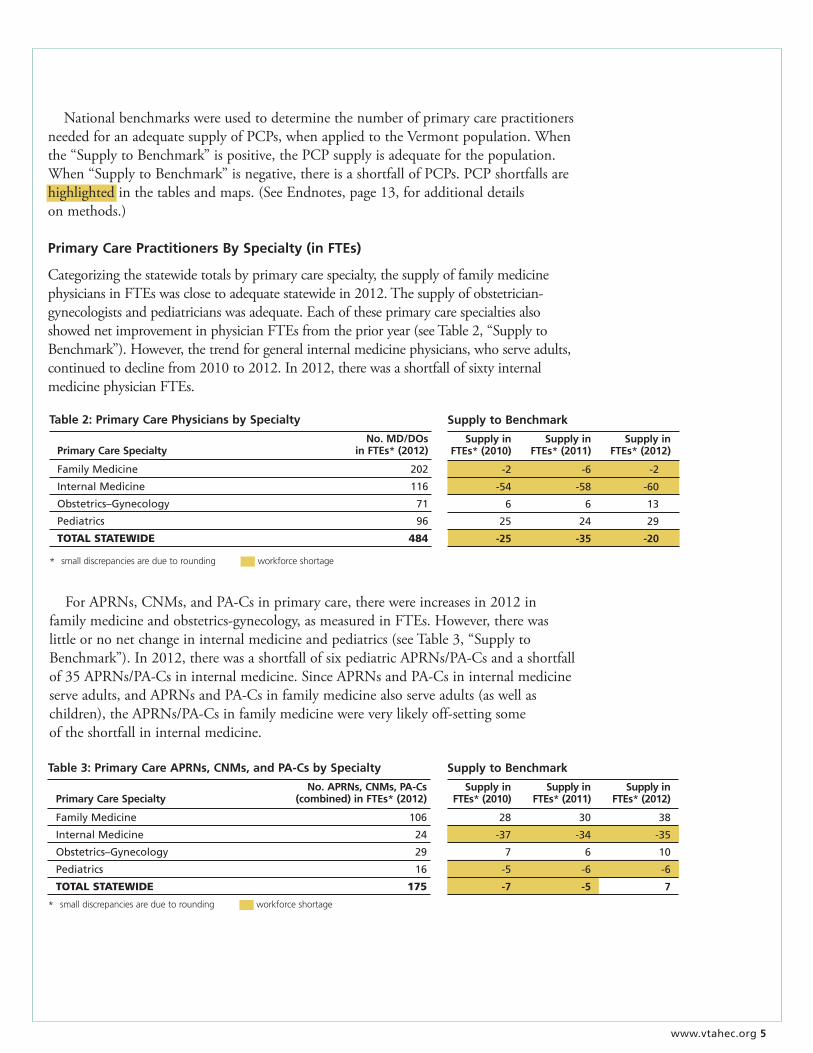
Table �: Primary care APrNs, cNms, and PA-cs by Specialty
No. APrNs, cNms, PA-cs Primary care Specialty (combined) in fTes* (2012)
Family Medicine 106
Internal Medicine 24
Obstetrics–Gynecology 29
Pediatrics 16
TOTalsTaTewiDe 175
* smalldiscrepanciesareduetorounding workforceshortage
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
28 30 38
-37 -34 -35
7 6 10
-5 -6 -6
-7 -5 7
Table 2: Primary care Physicians by Specialty
No. md/dOs Primary care Specialty in fTes* (2012)
Family Medicine 202
Internal Medicine 116
Obstetrics–Gynecology 71
Pediatrics 96
TOTalsTaTewiDe 484
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
-2 -6 -2
-54 -58 -60
6 6 13
25 24 29
-25 -�5 -20
* smalldiscrepanciesareduetorounding workforceshortage
ForAPRNs,CNMs,andPA-Csinprimarycare,therewereincreasesin2012infamilymedicineandobstetrics-gynecology,asmeasuredinFTEs.However,therewaslittleornonetchangeininternalmedicineandpediatrics(seeTable3,“SupplytoBenchmark”).In2012,therewasashortfallofsixpediatricAPRNs/PA-Csandashortfallof35APRNs/PA-Csininternalmedicine.SinceAPRNsandPA-Csininternalmedicineserveadults,andAPRNsandPA-Csinfamilymedicinealsoserveadults(aswellaschildren),theAPRNs/PA-Csinfamilymedicinewereverylikelyoff-settingsomeoftheshortfallininternalmedicine.
NationalbenchmarkswereusedtodeterminethenumberofprimarycarepractitionersneededforanadequatesupplyofPCPs,whenappliedtotheVermontpopulation.Whenthe“SupplytoBenchmark”ispositive,thePCPsupplyisadequateforthepopulation.When“SupplytoBenchmark”isnegative,thereisashortfallofPCPs.PCPshortfallsarehighlightedinthetablesandmaps.(SeeEndnotes,page13,foradditionaldetailsonmethods.)
Primary care Practitioners by Specialty (in fTes)
Categorizingthestatewidetotalsbyprimarycarespecialty,thesupplyoffamilymedicinephysiciansinFTEswasclosetoadequatestatewidein2012.Thesupplyofobstetrician-gynecologistsandpediatricianswasadequate.EachoftheseprimarycarespecialtiesalsoshowednetimprovementinphysicianFTEsfromtheprioryear(seeTable2,“SupplytoBenchmark”).However,thetrendforgeneralinternalmedicinephysicians,whoserveadults,continuedtodeclinefrom2010to2012.In2012,therewasashortfallofsixtyinternalmedicinephysicianFTEs.
www.vtahec.org 5
� www.vtahec.org
Combiningphysicians(seeTable2)withAPRNsandPA-Cs(seeTable3)ininternalandfamilymedicine,theoverall increase in all PCPs in 2012 did not improve the area of greatest need in Vermont: primary care services for adults.FurtherevidenceoftheneedforPCPsinadultprimarycareispresentedintheregionalsectionsofthisreportinTables10,11and12(seepages10-12).
limiting New Patients by Specialty
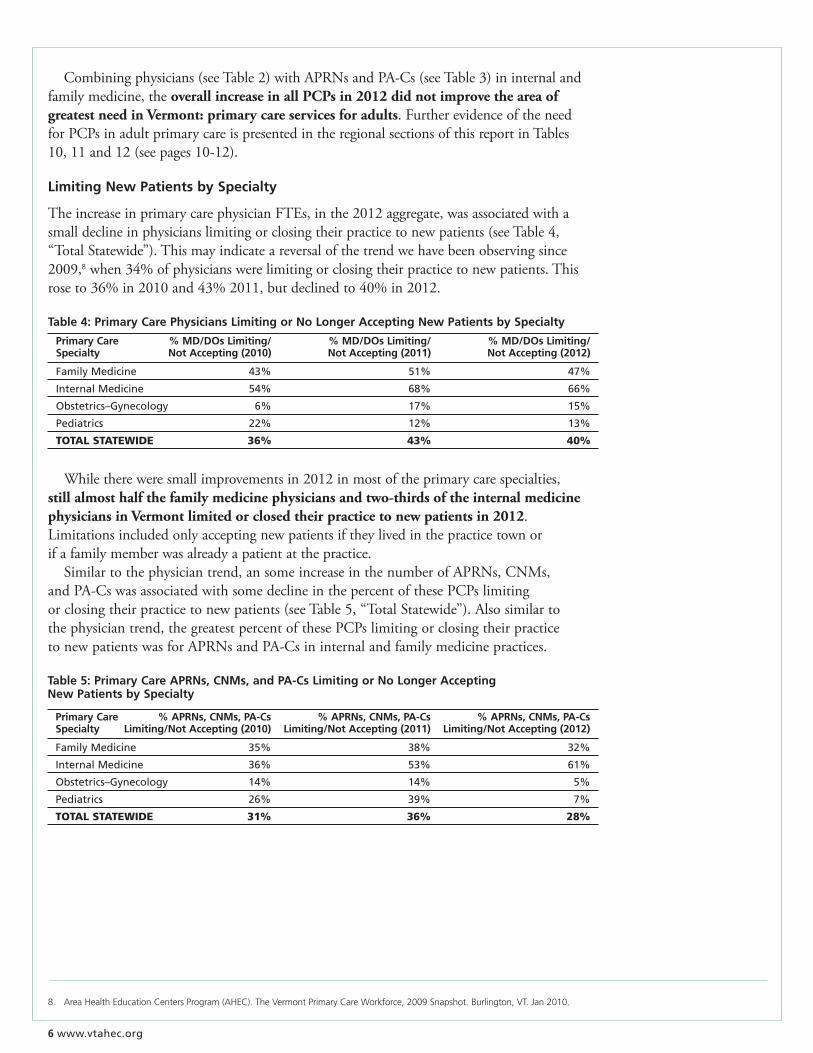
TheincreaseinprimarycarephysicianFTEs,inthe2012aggregate,wasassociatedwithasmalldeclineinphysicianslimitingorclosingtheirpracticetonewpatients(seeTable4,“TotalStatewide”).Thismayindicateareversalofthetrendwehavebeenobservingsince2009,8when34%ofphysicianswerelimitingorclosingtheirpracticetonewpatients.Thisroseto36%in2010and43%2011,butdeclinedto40%in2012.
Table 5: Primary care APrNs, cNms, and PA-cs limiting or No longer Accepting New Patients by Specialty
Primary care % APrNs, cNms, PA-cs % APrNs, cNms, PA-cs % APrNs, cNms, PA-cs Specialty limiting/Not Accepting (2010) limiting/Not Accepting (2011) limiting/Not Accepting (2012)
Family Medicine 35% 38% 32%
Internal Medicine 36% 53% 61%
Obstetrics–Gynecology 14% 14% 5%
Pediatrics 26% 39% 7%
TOTalsTaTewiDe 31% 36% 28%
Table �: Primary care Physicians limiting or No longer Accepting New Patients by Specialty
Primary care % md/dOs limiting/ % md/dOs limiting/ % md/dOs limiting/ Specialty Not Accepting (2010) Not Accepting (2011) Not Accepting (2012)
Family Medicine 43% 51% 47%
Internal Medicine 54% 68% 66%
Obstetrics–Gynecology 6% 17% 15%
Pediatrics 22% 12% 13%
TOTalsTaTewiDe 36% 43% 40%
Whilethereweresmallimprovementsin2012inmostoftheprimarycarespecialties,still almost half the family medicine physicians and two-thirds of the internal medicine physicians in Vermont limited or closed their practice to new patients in 2012.Limitationsincludedonlyacceptingnewpatientsiftheylivedinthepracticetownorifafamilymemberwasalreadyapatientatthepractice. Similartothephysiciantrend,ansomeincreaseinthenumberofAPRNs,CNMs,andPA-CswasassociatedwithsomedeclineinthepercentofthesePCPslimitingorclosingtheirpracticetonewpatients(seeTable5,“TotalStatewide”).Alsosimilartothephysiciantrend,thegreatestpercentofthesePCPslimitingorclosingtheirpracticetonewpatientswasforAPRNsandPA-Csininternalandfamilymedicinepractices.
8. AreaHealthEducationCentersProgram(AHEC).TheVermontPrimaryCareWorkforce,2009Snapshot.Burlington,VT.Jan2010.

www.vtahec.org 7
Table �: Primary care Physicians by county
Population No. Practice No. md/dOs county (est. 2011) Sites (2012) in fTes* (2012)
nORTheasTeRnveRMOnT
Caledonia 31,166 11 24
Essex 6,291 2 2
Lamoille 24,701 10 19
Orange 29,006 8 20
Orleans 27,173 10 22
Washington 59,626 19 51
chaMPlainvalley
Addison 36,742 11 25
Chittenden 157,491 50 141
Franklin 48,113 21 30
Grand Isle 6,931 2 1
sOuTheRnveRMOnT
Bennington 36,970 19 30
Rutland 61,289 18 41
Windham 44,266 21 38
Windsor 56,666 16 39
TOTalsTaTewiDe 626,431 218 484
* smalldiscrepanciesareduetorounding workforceshortage.
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
-15 -9 -5
1 -1 -1
-3 -3 -3
-2 -1 -1
-5 -3 -3
-5 -4 0
-1 3 3
5 -7 -3
3 -1 -4
18 6 15
-10 -8 -9
-5 -4 -5
-14 -19 -12
0 -3 1
-12 -10 -8
5 5 3
-7 -11 -7
-25 -35 -20
Primary care Practitioners by region (in fTes)
Examiningtheprimarycarephysicianshortfallsbyregionsofthestate,eachoftheAHECregionsreflectedthestatewidetrendandshowedsomeimprovementinthetotalnumberofprimarycarephysicianFTEsin2012,thoughashortfallpersistedineachregion(seeTable6,“SupplytoBenchmark”forNortheasternVT,ChamplainValley,andSouthernVT).Despite the overall increases since 2011, the need for primary care services for adults within each region continued in 2012,asshowninfurtherregionalbreakdownsbyspecialtyinTables10,11and12(seepages10-12).
� www.vtahec.org
Table 7: Primary care APrNs, cNms, and PA-cs by region by county
No. APrNs, cNms, PA-cs county (combined) in fTes* (2012)
nORTheasTeRnveRMOnT
Caledonia 10
Essex 2
Lamoille 7
Orange 9
Orleans 9
Washington 20
chaMPlainvalley
Addison 9
Chittenden 41
Franklin 13
Grand Isle 2
sOuTheRnveRMOnT
Bennington 9
Rutland 15
Windham 12
Windsor 15
TOTalsTaTewiDe 175
* smalldiscrepanciesareduetorounding workforceshortage
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
7 8 11
1 1 2
0 0 1
0 0 1
0 1 1
4 3 2
2 3 4
-13 -12 -2
-3 -4 -1
-7 -10 -2
-3 1 0
0 -1 0
-2 -1 -2
-3 0 -1
0 1 -2
3 0 0
-2 -2 0
-7 -5 7
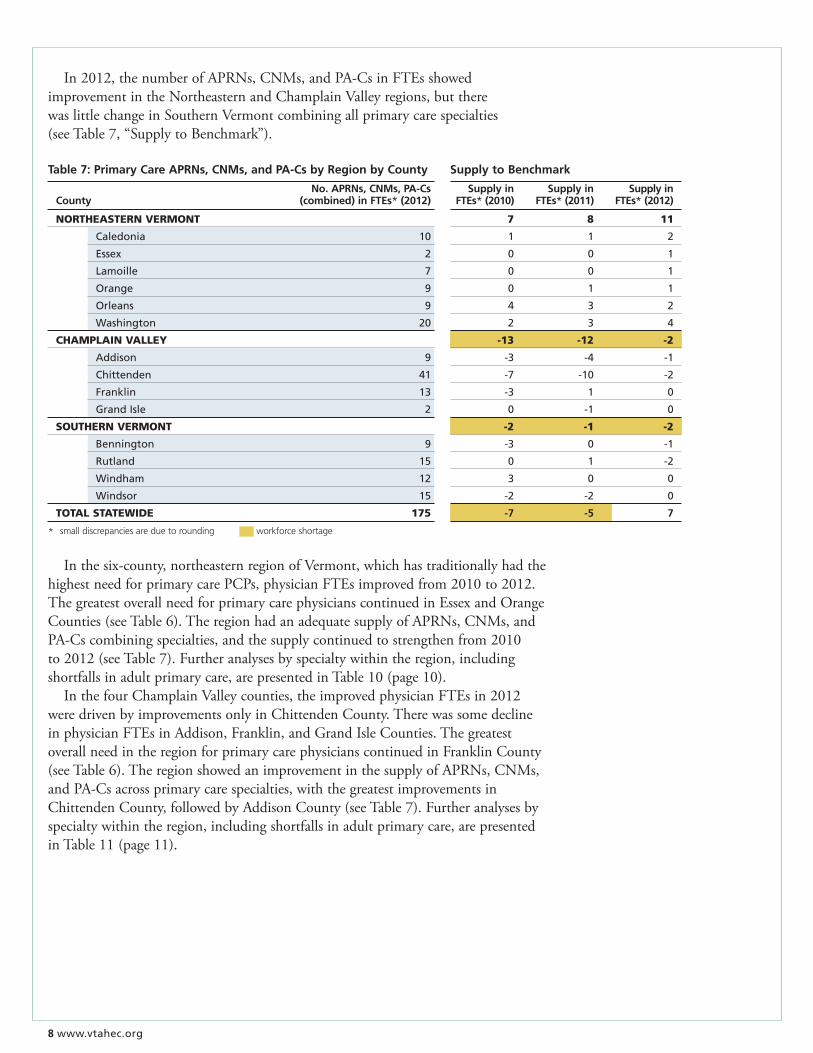
Inthesix-county,northeasternregionofVermont,whichhastraditionallyhadthehighestneedforprimarycarePCPs,physicianFTEsimprovedfrom2010to2012.ThegreatestoverallneedforprimarycarephysicianscontinuedinEssexandOrangeCounties(seeTable6).TheregionhadanadequatesupplyofAPRNs,CNMs,andPA-Cscombiningspecialties,andthesupplycontinuedtostrengthenfrom2010to2012(seeTable7).Furtheranalysesbyspecialtywithintheregion,includingshortfallsinadultprimarycare,arepresentedinTable10(page10). InthefourChamplainValleycounties,theimprovedphysicianFTEsin2012weredrivenbyimprovementsonlyinChittendenCounty.TherewassomedeclineinphysicianFTEsinAddison,Franklin,andGrandIsleCounties.ThegreatestoverallneedintheregionforprimarycarephysicianscontinuedinFranklinCounty(seeTable6).TheregionshowedanimprovementinthesupplyofAPRNs,CNMs,andPA-Csacrossprimarycarespecialties,withthegreatestimprovementsinChittendenCounty,followedbyAddisonCounty(seeTable7).Furtheranalysesbyspecialtywithintheregion,includingshortfallsinadultprimarycare,arepresentedinTable11(page11).
In2012,thenumberofAPRNs,CNMs,andPA-CsinFTEsshowedimprovementintheNortheasternandChamplainValleyregions,buttherewaslittlechangeinSouthernVermontcombiningallprimarycarespecialties(seeTable7,“SupplytoBenchmark”).

www.vtahec.org �
Table �: Primary care Physicians limiting or No longer Accepting New Patients by county
% md/dOs limiting/ % md/dOs limiting/ % md/dOs limiting/ county Not Accepting (2010) Not Accepting (2011) Not Accepting (2012)
Northeastern Vermont 55% 51% 43%
Champlain Valley 31% 40% 42%
Southern Vermont 29% 40% 35%
TOTalsTaTewiDe 36% 43% 40%
ThefoursoutherncountiesofBennington,Rutland,Windham,andWindsorcombinedtobetheregionwiththegreatestneedforprimarycarephysiciansinVermontin2012.ThiswasdrivenbyhighneedsinRutlandandWindsorCounties,whencombiningallprimarycarespecialties.Despitetheseneeds,mostcountiesintheregionshowedsomeimprovementinthenumberofphysicianFTEsfrom2011to2012(seeTable6).ThesupplyofAPRNs,CNMs,andPA-Csintheregionwasclosetoadequatein2012,withRutlandCountyexperiencingthegreatestneed(seeTable7).Furtheranalysesbyspecialtywithintheregion,includingshortfallsinadultprimarycare,arepresentedinTable12onpage12.
limiting New Patients by region
From2011to2012,theoverallimprovementinthetotalnumberofprimarycareMD/DOs,APRNs,CNMs,andPA-CswasgenerallyassociatedwithadeclineinthepercentofPCPslimitingornotacceptingnewpatients(seeTables8&9).Therewasalsolessvariabilitybetweentheregionsin2012,comparedto2010.
Table �: Primary care APrNs, cNms, and PA-cs limiting or No longer Accepting
New Patients by county
% APrNs, cNms, PA-cs % APrNs, cNms, PA-cs % APrNs, cNms, PA-cs county limiting/Not Accepting (2010) limiting/Not Accepting (2011) limiting/Not Accepting (2012)
Northeastern Vermont 44% 38% 26%
Champlain Valley 24% 38% 32%
Southern Vermont 22% 33% 25%
TOTalsTaTewiDe 31% 36% 28%
10 www.vtahec.org
2 0 1 2 S u r v e Y f i N d i N g S b Y A H e c r e g i O N
• PrimaryCarePracticeSite
NortheasternVermontcaledonia, essex, lamoille, Orange, Orleans, and washington counties
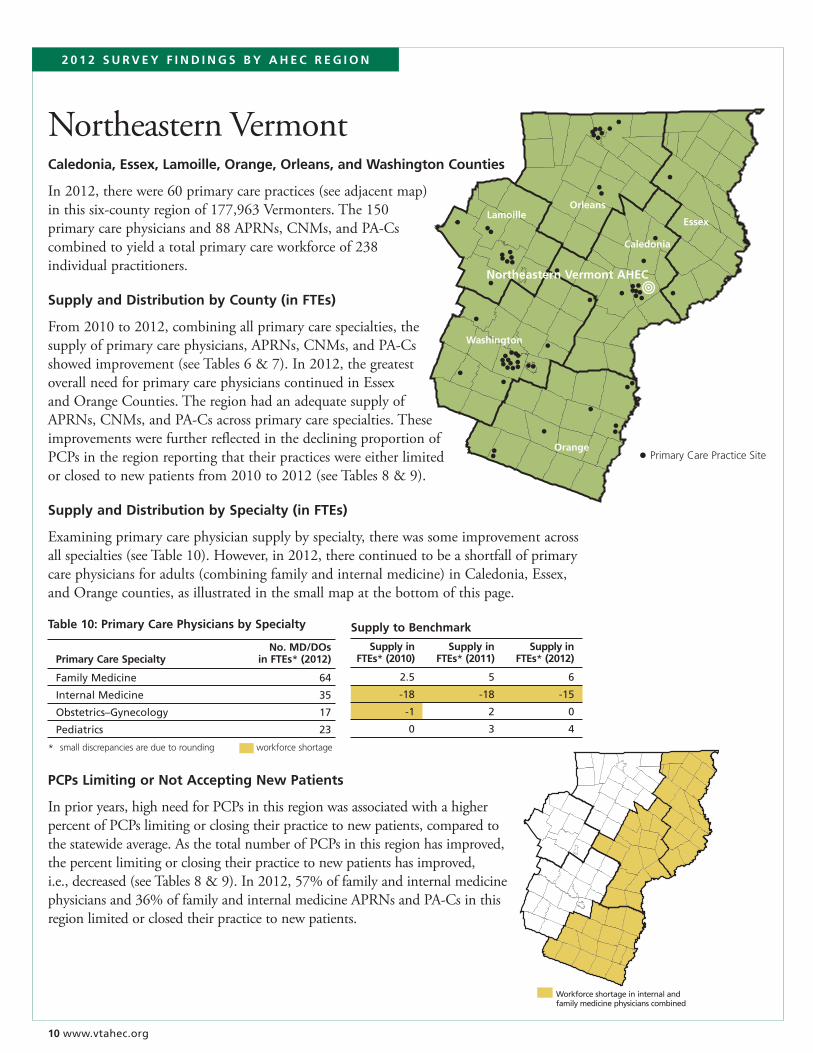
In2012,therewere60primarycarepractices(seeadjacentmap)inthissix-countyregionof177,963Vermonters.The150primarycarephysiciansand88APRNs,CNMs,andPA-Cscombinedtoyieldatotalprimarycareworkforceof238individualpractitioners.
Supply and distribution by county (in fTes)
From2010to2012,combiningallprimarycarespecialties,thesupplyofprimarycarephysicians,APRNs,CNMs,andPA-Csshowedimprovement(seeTables6&7).In2012,thegreatestoverallneedforprimarycarephysicianscontinuedinEssexandOrangeCounties.TheregionhadanadequatesupplyofAPRNs,CNMs,andPA-Csacrossprimarycarespecialties.TheseimprovementswerefurtherreflectedinthedecliningproportionofPCPsintheregionreportingthattheirpracticeswereeitherlimitedorclosedtonewpatientsfrom2010to2012(seeTables8&9).
Supply and distribution by Specialty (in fTes)
Examiningprimarycarephysiciansupplybyspecialty,therewassomeimprovementacrossallspecialties(seeTable10).However,in2012,therecontinuedtobeashortfallofprimarycarephysiciansforadults(combiningfamilyandinternalmedicine)inCaledonia,Essex,andOrangecounties,asillustratedinthesmallmapatthebottomofthispage.
Washington
Orange
Caledonia
LamoilleOrleans
Essex
•Northeastern vermont AHec
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
2.5 5 6
-18 -18 -15
-1 2 0
0 3 4
Table 10: Primary care Physicians by Specialty
No. md/dOs Primary care Specialty in fTes* (2012)
Family Medicine 64
Internal Medicine 35
Obstetrics–Gynecology 17
Pediatrics 23
* smalldiscrepanciesareduetorounding workforceshortage
PcPs limiting or Not Accepting New Patients
Inprioryears,highneedforPCPsinthisregionwasassociatedwithahigherpercentofPCPslimitingorclosingtheirpracticetonewpatients,comparedtothestatewideaverage.AsthetotalnumberofPCPsinthisregionhasimproved,thepercentlimitingorclosingtheirpracticetonewpatientshasimproved,i.e.,decreased(seeTables8&9).In2012,57%offamilyandinternalmedicinephysiciansand36%offamilyandinternalmedicineAPRNsandPA-Csinthisregionlimitedorclosedtheirpracticetonewpatients.
Workforce shortage in internal and family medicine physicians combined

www.vtahec.org 11
2 0 1 2 S u r v e Y f i N d i N g S b Y A H e c r e g i O N
• PrimaryCarePracticeSite
ChamplainValleyAddison, chittenden, franklin, and grand isle counties
In2012,therewere84primarycarepractices(seeadjacentmap)inthisfour-countyregionof249,277Vermonters.The236primarycarephysiciansand93APRNs,CNMs,andPA-Cscombinedtoyieldatotalprimarycareworkforceof329individualpractitioners.
Supply and distribution by county (in fTes)
Theregionshowedimprovementinthetotalnumberofphysiciansacrossprimarycarespecialties(seeTable6),butthiswasdrivenbyincreasesinChittendenCountyandsomedeclineinAddison,Franklin,andGrandIsleCounties.ThegreatestneedscontinuedinFranklinCounty.Theregionhasshownanincreaseintheproportionofprimarycarephysiciansreportingthattheirpracticeswerelimitedorclosedtonewpatientssince2010(seeTable8).
TherewereimprovementsinthesupplyofAPRNs,CNMs,andPA-Csacrossprimarycarespecialties,withthegreatestimprovementsinChittenden,followedbyAddisonCounty(seeTable7).ThiswasassociatedwithadeclineintheproportionofthesePCPsreportingtheirpracticeslimitedorclosedtonewpatientssince2011(seeTable9).
Supply and distribution by Specialty (in fTes)
Examiningprimarycarephysiciansbyspecialty,obstetrics-gynecologyphysiciansshowedthemostimprovement(seeTable11).Thesupplyofpediatriciansremainedadequate.Butthesupplyofphysiciansforadults,includingfamilyandinternalmedicine,continuedtoshowaveryhighneed.Asillustratedonthesmallmapatthebottomofthispage,everycountyintheregionhadashortfallofphysicianstoserveadultsinprimarycarein2012.
Franklin
Chittenden
Addison
•
Grand Isle
•champlain valley AHec
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
-12 -16 -15
-14 -17 -19
10 8 13
21 17 18
Table 11: Primary care Physicians by Specialty
No. md/dOs Primary care Specialty in fTes* (2012)
Family Medicine 66
Internal Medicine 51
Obstetrics–Gynecology 36
Pediatrics 44
* smalldiscrepanciesareduetorounding workforceshortage
PcPs limiting or Not Accepting New Patients
In2012,59%offamilyandinternalmedicinephysiciansand41%offamilyandinternalmedicineAPRNsandPA-Cslimitedorclosedtheirpracticetonewpatientsinthisregion.
Workforce shortage in internal and family medicine physicians combined
12 www.vtahec.org
• PrimaryCarePracticeSite
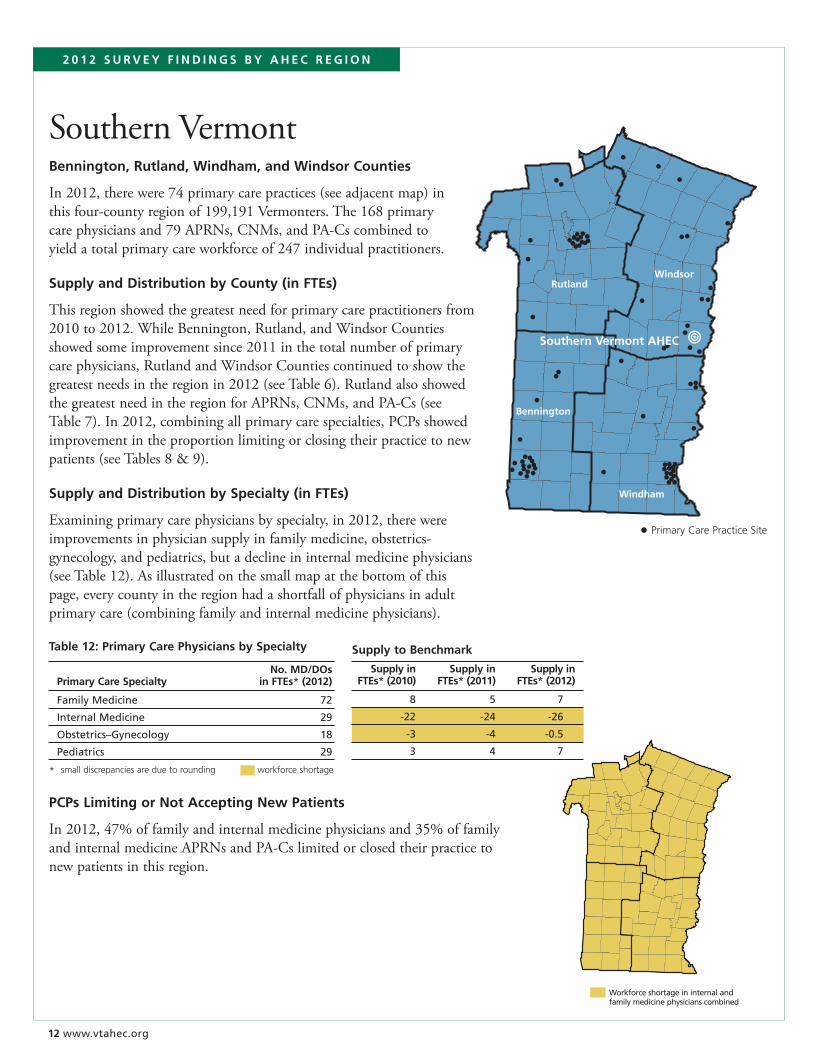
SouthernVermontbennington, rutland, windham, and windsor counties
In2012,therewere74primarycarepractices(seeadjacentmap)inthisfour-countyregionof199,191Vermonters.The168primarycarephysiciansand79APRNs,CNMs,andPA-Cscombinedtoyieldatotalprimarycareworkforceof247individualpractitioners.
Supply and distribution by county (in fTes)
Thisregionshowedthegreatestneedforprimarycarepractitionersfrom2010to2012.WhileBennington,Rutland,andWindsorCountiesshowedsomeimprovementsince2011inthetotalnumberofprimarycarephysicians,RutlandandWindsorCountiescontinuedtoshowthegreatestneedsintheregionin2012(seeTable6).RutlandalsoshowedthegreatestneedintheregionforAPRNs,CNMs,andPA-Cs(seeTable7).In2012,combiningallprimarycarespecialties,PCPsshowedimprovementintheproportionlimitingorclosingtheirpracticetonewpatients(seeTables8&9).
Supply and distribution by Specialty (in fTes)
Examiningprimarycarephysiciansbyspecialty,in2012,therewereimprovementsinphysiciansupplyinfamilymedicine,obstetrics-gynecology,andpediatrics,butadeclineininternalmedicinephysicians(seeTable12).Asillustratedonthesmallmapatthebottomofthispage,everycountyintheregionhadashortfallofphysiciansinadultprimarycare(combiningfamilyandinternalmedicinephysicians).
•
Windham
WindsorRutland
Bennington
• Primary Care Practice Site
Southern vermont AHec
2 0 1 2 S u r v e Y f i N d i N g S b Y A H e c r e g i O N
Workforce shortage in internal and family medicine physicians combined
Supply to benchmark
Supply in Supply in Supply in fTes* (2010) fTes* (2011) fTes* (2012)
8 5 7
-22 -24 -26
-3 -4 -0.5
3 4 7
Table 12: Primary care Physicians by Specialty
No. md/dOs Primary care Specialty in fTes* (2012)
Family Medicine 72
Internal Medicine 29
Obstetrics–Gynecology 18
Pediatrics 29
* smalldiscrepanciesareduetorounding workforceshortage
PcPs limiting or Not Accepting New Patients
In2012,47%offamilyandinternalmedicinephysiciansand35%offamilyandinternalmedicineAPRNsandPA-Cslimitedorclosedtheirpracticetonewpatientsinthisregion.
www.vtahec.org 1�
Primary care Practice:Anofficeorclinicwhichofferedgeneralprimarycaretoadultsand/orchildren,anongoingrelationshipbetweenaprimarycarepractitioner(PCP)andthepatient,comprehensivecare,continuityofcare,andcoordinationofcareinfamilymedicine,generalinternalmedicine,generalobstetrics-gynecology,andgeneralpediatrics.Sitemayhaveincludedthepatient’shomeforan“allhomecare”primarycarepractitioner.
Sitesnotincludedwere:walk-in/immediate/acutecareclinics,school-basedclinics,freeclinics,PlannedParenthoodclinics,collegehealthcenters,DepartmentofCorrectionshealthfacilities,sitesforat-riskyouth,sitesforhomelesspeople,nursinghomes,residentialassisted-livingfacilities,andVeteransAdministrationclinics.
Primary care Practitioners:PCPsincludedphysicians(MDsandDOs),advancedpracticeregisterednurses(APRNs),certifiednursemidwives(CNMs),andcertifiedphysicianassistants(PA-Cs)atprimarycarepracticesites.
Practice-based Survey:Primarycareofficeadministratorsfromall218primarycarepracticesinVermontweresurveyedbyAHECinthespring/earlysummerof2012,toupdatetheprioryear’slistofPCPsandtoreporttheircurrent,typical,weeklyofficehoursatthepracticesite.PerdiemorothertemporaryPCPswerenotincluded,ifthepracticewassearchingforapermanentpractitioner.
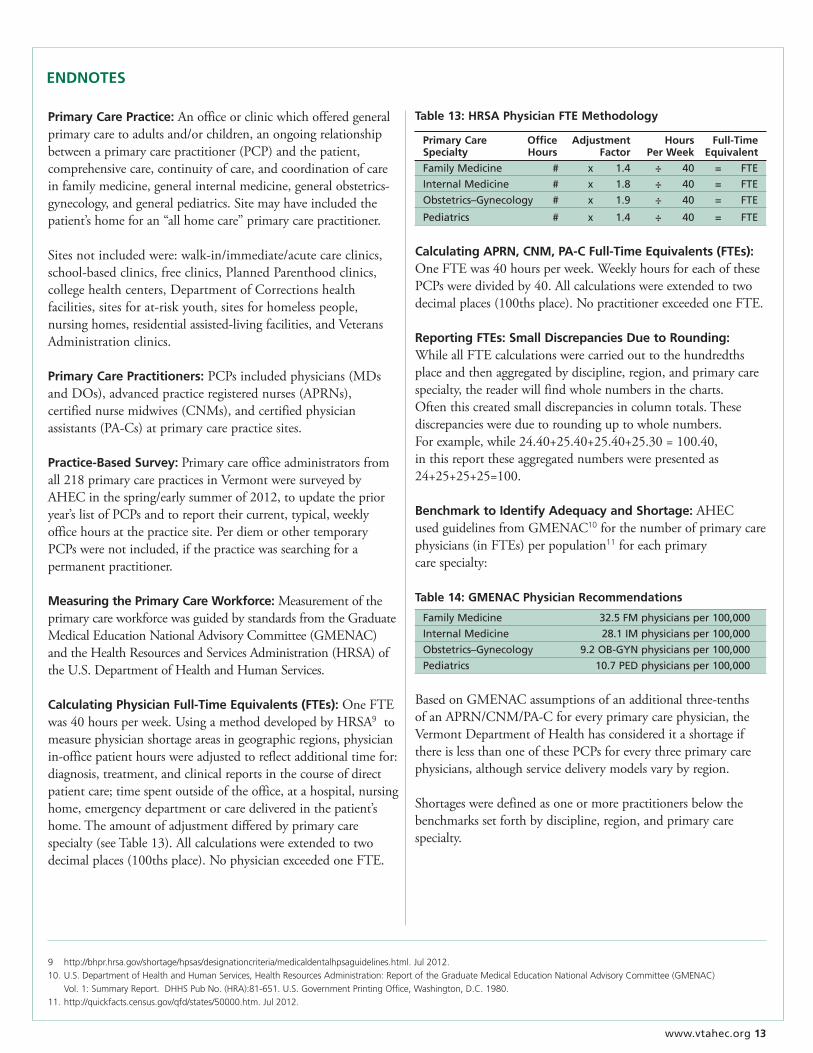
measuring the Primary care workforce: MeasurementoftheprimarycareworkforcewasguidedbystandardsfromtheGraduateMedicalEducationNationalAdvisoryCommittee(GMENAC)andtheHealthResourcesandServicesAdministration(HRSA)oftheU.S.DepartmentofHealthandHumanServices.
calculating Physician full-Time equivalents (fTes): OneFTEwas40hoursperweek.UsingamethoddevelopedbyHRSA9tomeasurephysicianshortageareasingeographicregions,physicianin-officepatienthourswereadjustedtoreflectadditionaltimefor:diagnosis,treatment,andclinicalreportsinthecourseofdirectpatientcare;timespentoutsideoftheoffice,atahospital,nursinghome,emergencydepartmentorcaredeliveredinthepatient’shome.Theamountofadjustmentdifferedbyprimarycarespecialty(seeTable13).Allcalculationswereextendedtotwodecimalplaces(100thsplace).NophysicianexceededoneFTE.
Table 1�: HrSA Physician fTe methodology
Primary care Office Adjustment Hours full-Time Specialty Hours factor Per week equivalent
Family Medicine # x 1.4 ÷ 40 = FTE
Internal Medicine # x 1.8 ÷ 40 = FTE
Obstetrics–Gynecology # x 1.9 ÷ 40 = FTE
Pediatrics # x 1.4 ÷ 40 = FTE
calculating APrN, cNm, PA-c full-Time equivalents (fTes):OneFTEwas40hoursperweek.WeeklyhoursforeachofthesePCPsweredividedby40.Allcalculationswereextendedtotwodecimalplaces(100thsplace).NopractitionerexceededoneFTE.
reporting fTes: Small discrepancies due to rounding: WhileallFTEcalculationswerecarriedouttothehundredthsplaceandthenaggregatedbydiscipline,region,andprimarycarespecialty,thereaderwillfindwholenumbersinthecharts.Oftenthiscreatedsmalldiscrepanciesincolumntotals.Thesediscrepancieswereduetoroundinguptowholenumbers.Forexample,while24.40+25.40+25.40+25.30=100.40,inthisreporttheseaggregatednumberswerepresentedas24+25+25+25=100.
benchmark to identify Adequacy and Shortage:AHECusedguidelinesfromGMENAC10forthenumberofprimarycarephysicians(inFTEs)perpopulation11foreachprimarycarespecialty:
Table 1�: gmeNAc Physician recommendations
Family Medicine 32.5 FM physicians per 100,000
Internal Medicine 28.1 IM physicians per 100,000
Obstetrics–Gynecology 9.2 OB-GYN physicians per 100,000
Pediatrics 10.7 PED physicians per 100,000
BasedonGMENACassumptionsofanadditionalthree-tenthsofanAPRN/CNM/PA-Cforeveryprimarycarephysician,theVermontDepartmentofHealthhasconsidereditashortageifthereislessthanoneofthesePCPsforeverythreeprimarycarephysicians,althoughservicedeliverymodelsvarybyregion.
Shortagesweredefinedasoneormorepractitionersbelowthebenchmarkssetforthbydiscipline,region,andprimarycarespecialty.
eNdNOTeS
9 http://bhpr.hrsa.gov/shortage/hpsas/designationcriteria/medicaldentalhpsaguidelines.html.Jul2012.10.U.S.DepartmentofHealthandHumanServices,HealthResourcesAdministration:ReportoftheGraduateMedicalEducationNationalAdvisoryCommittee(GMENAC) Vol.1:SummaryReport.DHHSPubNo.(HRA):81-651.U.S.GovernmentPrintingOffice,Washington,D.C.1980.11.http://quickfacts.census.gov/qfd/states/50000.htm.Jul2012.

Connecting students to careers, professionals to communities, and communities to better health.
For more information contact your regional AHEC or
Elizabeth Cote, Director
(802) 656-0030
www.vtahec.orgJanuary2013
Primary care Survey
PRACTICENAME DATEOFCOMPLETION
PHySICALTOWNOFPRACTICE
CONTACTPERSON CONTACTEMAIL CONTACTTELEPHONE
PracticeSiteOwnership: FQHC RHC Hospital-owned Privatepractice
PleaseincludeallMDs,DOs,APRNs,CNMs,andPA-Cswhoseepatientsatyourpracticesite.Indicateofficehours,notincludingcall,roundsoradministrativetime.
Practitioner degree/ Specialty in-Office Patient Accepting New Patients? Name certificate Hours Per week Yes No limited to:







