i
The use of elastic therapeutic tape for treatment of lateral elbow tendinosis
Raewyn Lin Wegener
B Occ Thy
Grad Cert (Wound Care)
M Hlth Sci (Occupational Therapy)
A thesis submitted in fulfilment of the requirement of the:
Doctor of Philosophy
(Thesis by Publications)
Supervisors:
Dr Lisa O’Brien
A/Prof Ted Brown
Department of Occupational Therapy
Faculty of Medicine, Nursing and Health Sciences
Monash University
Victoria, Australia
2016

2
Notice 1 © Raewyn Lin Wegener (2016)
Under the Copyright Act 1968, this thesis must be used only under the normal conditions
of scholarly fair dealing. In particular, no results or conclusions should be extracted from
it, nor should it be copied or closely paraphrased in whole or in part without the written
consent of the author. Proper written acknowledgement should be made for any
assistance obtained from this thesis.
Notice 2
© Raewyn Lin Wegener (2016)
I certify that I have made all reasonable efforts to secure copyright permissions for third-
party content included in this thesis and have not knowingly added copyright content to
my work without the owner’s permission.

3
General Declaration
In accordance with Monash University Doctorate Regulation 17 / Doctor of Philosophy
and Master of Philosophy regulations, the following declarations are made:
I hereby declare that this thesis contains no material which has been accepted for the
award of any other degree or diploma at any university or equivalent institution and
that, to the best of my knowledge and belief, this thesis contains no material previously
published or written by another person, except where due reference is made in the text
of the thesis. All pictures throughout this thesis were taken of myself and one of my
colleagues (with consent) who assisted in the study. Permission has been obtained for
all figures that have been included from other sources or published text.
This thesis includes five original papers and one opinion piece published (or in press) in
peer-reviewed journals. The ideas, development and writing up of all papers in the thesis
were the principal responsibility of myself, working under the supervision of Dr Lisa
O’Brien and Associate Professor Ted Brown.
Signature:
Name: Raewyn Lin Wegener
Date: 17/10/2016

4
Thesis Chapter
Publication Title Publication Status
Nature and % of candidate’s contribution
Co-authors
3 A scoping review of the use of elastic therapeutic tape for neck and upper extremity conditions.
Published 80% - Concept development, literature review, data collection, writing, submission and amendments to manuscript.
A/Prof Ted Brown Dr Lisa O’Brien 20% - Revision of drafts and amendments to manuscript.
4 Knowledge of and willingness to recommend kinesiotape for upper limb overuse injuries: A comparison of therapists', GPs' and surgeons' perspectives.
Published 80% - Concept development, literature review, data collection, writing, submission and amendments to manuscript.
A/Prof Ted Brown Dr Lisa O’Brien 20% - Revision of drafts and amendments to manuscript.
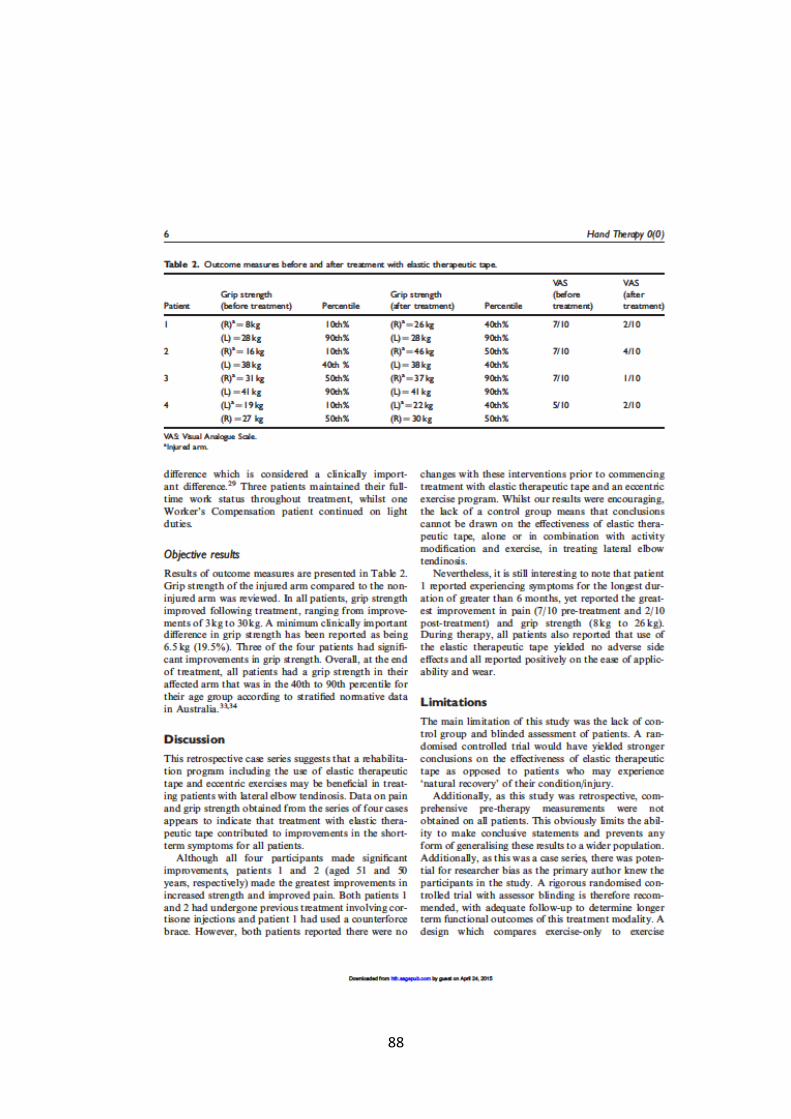
5 The use of elastic therapeutic tape and eccentric exercises for lateral elbow tendinosis: a case series.
Published 80% - Concept development, literature review, data collection, writing, submission and amendments to manuscript.
A/Prof Ted Brown Dr Lisa O’Brien 20% - Revision of drafts and amendments to manuscript.

5
Thesis Chapter
Publication Title Publication Status
Nature and % of candidate’s contribution
Co-authors
6 A randomized controlled trial of comparative effectiveness of elastic therapeutic tape, sham tape or eccentric exercises alone for lateral elbow tendinosis.
Published 80% - Concept development, literature review, data collection, writing, submission and amendments to manuscript.
A/Prof Ted Brown Dr Lisa O’Brien 20% - Revision of drafts and amendments to manuscript.
7 A qualitative review
of patients’
experiences using
Kinesio tape for
lateral epicondylitis.
Submitted to journal – (undergoing second revision)
80% - Concept development, literature review, data collection, writing, submission and amendments to manuscript.
A/Prof Ted Brown Dr Lisa O’Brien 20% - Revision of drafts and amendments to manuscript.
Signed: Date: 17/10/2016

6
Table of Contents
GENERAL DECLARATION ........................................................................................... 3
LIST OF FIGURES ..................................................................................................... 10
LIST OF TABLES ....................................................................................................... 11
APPENDICES ........................................................................................................... 12
ACKNOWLEDGEMENTS ........................................................................................... 13
THESIS SUMMARY .................................................................................................. 14
ABBREVIATIONS ..................................................................................................... 16
THESIS PUBLICATIONS ............................................................................................ 17
CHAPTER 1 – GENERAL INTRODUCTION .................................................................. 18
1.1 INTRODUCTION AND OVERVIEW OF THESIS STRUCTURE ................................................ 18
1.2 LITERATURE REVIEW ................................................................................................... 22
1.2.1 Clinical presentation and diagnostic tests ..................................................... 25
1.2.2 Treatment for lateral elbow tendinosis .......................................................... 27
1.2.3 Using elastic therapeutic tape for tendinosis ................................................. 29
1.3 CONCEPTUAL FRAMEWORKS ......................................................................................... 31
1.3.1 Biomechanical Model of Health (BMH) .......................................................... 32
1.3.2 The Occupational Adaptation Model (OAM) ................................................. 34
1.3.3 The International Classification of Functioning, Disability, and Health (ICF) . 37
1.4 CHAPTER SUMMARY ................................................................................................... 39
CHAPTER 2 – METHODOLOGY ................................................................................. 40
2.1 INTRODUCTION .......................................................................................................... 40
2.2 RESEARCH QUESTIONS ................................................................................................. 40
2.3 MATERIALS AND METHODS .......................................................................................... 42
2.3.1 Research Question 1: What is the current evidence relating the use of elastic
therapeutic tape in treating neck and upper extremity conditions? ...................... 42

7
2.3.2 Research Question 2: What are the current perspectives amongst Hand
Therapists, General Practitioners and Hand Surgeons on the use of elastic
therapeutic tape and how often is it used or recommended? ................................ 43
2.3.3 Research Question 3: What is the preliminary evidence into the benefit of
elastic therapeutic tape and eccentric exercises for the treatment of lateral elbow
tendinosis? ............................................................................................................... 45
2.3.4 Research Question 4: Is the application of elastic therapeutic tape according
to the ‘Clinical Therapeutic Applications of the Kinesio Taping Method’ manual
(with the tape applied on tension), in conjunction with an eccentric exercise
program and activity modification advice, more effective than: (i) sham taping
(application with no stretch); or (ii) eccentric exercises alone; for people with
lateral elbow tendinosis? ........................................................................................ 47
2.3.5 Research Question 5: What are the experiences of people using elastic
therapeutic tape for lateral elbow tendinosis? ....................................................... 50
2.6 CHAPTER SUMMARY ................................................................................................... 52
CHAPTER 3 - A SCOPING REVIEW OF THE USE OF ELASTIC THERAPEUTIC TAPE FOR
NECK AND UPPER EXTREMITY CONDITIONS ............................................................ 53
3.1 INTRODUCTION .......................................................................................................... 53
3.2 CHAPTER CONTENTS ................................................................................................... 53
3.3 IMPACT OF THE STUDY ................................................................................................. 65
3.4 CHAPTER SUMMARY ................................................................................................... 66
CHAPTER 4 - A COMPARISON OF HAND THERAPISTS’, GENERAL PRACTITIONERS’ AND
SURGEONS’ PERSPECTIVES ON THE USE OF ELASTIC THERAPEUTIC TAPE ................. 69
4.1 INTRODUCTION .......................................................................................................... 69
4.2 CHAPTER CONTENTS ................................................................................................... 70
4.3 IMPACT OF THE STUDY ................................................................................................. 78
4.4 CHAPTER SUMMARY ................................................................................................... 78
CHAPTER 5 - THE USE OF ELASTIC THERAPEUTIC TAPE AND ECCENTRIC EXERCISES FOR
LATERAL ELBOW TENDINOSIS: A CASE SERIES. ........................................................ 81
5.1 INTRODUCTION .......................................................................................................... 81
5.2 CHAPTER CONTENTS ................................................................................................... 82
5.3 IMPACT OF THE STUDY ................................................................................................. 91

8
5.4 CHAPTER SUMMARY ................................................................................................... 92
CHAPTER 6 – A RANDOMISED CONTROLLED TRIAL OF COMPARATIVE EFFECTIVENESS
OF ELASTIC THERAPEUTIC TAPE, SHAM TAPE OR ECCENTRIC EXERCISES ALONE FOR
LATERAL ELBOW TENDINOSIS ................................................................................. 94
6.1 INTRODUCTION .......................................................................................................... 94
6.2 CHAPTER CONTENTS ................................................................................................... 96
6.3 IMPACT OF THE STUDY ............................................................................................... 106
6.4 CHAPTER SUMMARY ................................................................................................. 107
CHAPTER 7 - A QUALITATIVE REVIEW OF PATIENTS’ EXPERIENCES USING KINESIO
TAPE FOR LATERAL EPICONDYLITIS ....................................................................... 109
7.1 INTRODUCTION ........................................................................................................ 109
7.2 CHAPTER CONTENTS ................................................................................................. 109
7.3 IMPACT OF THE STUDY ............................................................................................... 132
7.4 CHAPTER SUMMARY ................................................................................................. 134
CHAPTER 8 – DISCUSSION AND CONCLUSION ........................................................ 137
8.1 CHAPTER OVERVIEW ................................................................................................. 137
8.2 REVISITING THE RESEARCH QUESTIONS ......................................................................... 137
8.3 DISCUSSION OF STUDY FINDINGS ................................................................................. 143
8.4 IMPLICATIONS FOR CLINICAL PRACTICE.......................................................................... 147
8.5 LIMITATIONS OF THIS THESIS ....................................................................................... 152
8.6 RECOMMENDATIONS FOR FUTURE RESEARCH ................................................................. 154
8.7 CHAPTER SUMMARY ................................................................................................. 155
REFERENCES ......................................................................................................... 156
APPENDIX ............................................................................................................ 162
APPENDIX A: PUBLISHED OPINION PIECE ............................................................................. 163
APPENDIX B: ETHICS APPROVAL AND FINAL REPORT .............................................................. 166
APPENDIX C: CONFERENCE PARTICIPATION ......................................................................... 169
Current Abstract Submissions ............................................................................... 169
Conference Presentations ..................................................................................... 169
Other Presentations .............................................................................................. 170
APPENDIX D: APPLICATION OF TAPE (STUDY 4) ................................................................... 171

9
APPENDIX E: ECCENTRIC EXERCISE PROGRAM (STUDY 4) ....................................................... 173
APPENDIX F: OUTCOME MEASURES (STUDY 4) .................................................................... 175
APPENDIX G: QUALITATIVE QUESTIONS (STUDY 5) ............................................................... 184

10
List of Figures
Figure 1 Biomechanical Model of Health (BMH) Page 33
Figure 2 Occupational Adaptation Model Page 36
Figure 3 International Classification of Functioning Page 38

11
List of Tables
Table 1 Thesis Publications Page 17
Table 2 Summary of Research Questions and Study Findings Page 139
12
Appendices
Appendix A Published Opinion Piece Page 163
Appendix B Ethics Approval and Final Report Page 166
Appendix C Conference Participation Page 167
Appendix D Application of Tape (Study 4) Page 171
Appendix E Exercise Program (Study 4) Page 173
Appendix F Outcome Measures (Study 4) Page 175
Appendix G Qualitative Questions (Study 5) Page 184

13
Acknowledgements
First and foremost, I would like to express my genuine gratitude to Dr Lisa
O’Brien and Associate Professor Ted Brown for their help, advice, supervision and
support during my PhD. I feel that I was blessed to have such exceptional supervisors! I
am sincerely grateful for their continual encouragement and guidance which has
enabled me to reach such significant milestones in my research. They have both played
an invaluable role in improving my knowledge, as well as creating opportunities for
future learning and development. For this experience, I will forever be thankful to them.
I would also like to thank my husband, Andrew, for his unwavering support over
the many years of Postgraduate study. You have stood by me with continual
encouragement and motivation, especially when I doubted myself. Thank you to my
wonderful family and parents, Des and Alice, who have shared this journey with me. I
have valued your support and kindness during this time. I am also very grateful to my
Uncle David for his help and technical assistance during my studies.
Importantly, I would also like to acknowledge all of my patients for their help in
furthering my knowledge in the area of Hand Therapy. Without them, this learning and
research would not have been possible and, for that, I am sincerely appreciative.

14
Thesis Summary
The development of this thesis arose from my clinical experience as a hand
therapist in a private practice setting. As is shown in the literature, lateral elbow
tendinosis is a common, yet complex, upper limb condition that is associated with long
term morbidity. Due to its degenerative aetiology, research has supported a shift away
from surgery and the use of passive interventions, such as immobilisation with splinting,
ultrasound, massage and the use of thermal modalities. Despite this evidence, it was my
observation that these treatment modalities were still commonly used amongst
therapists, including myself, who were attempting to manage the complexities of this
patient population. In particular, elastic therapeutic tape was used extensively for
tendinosis within the practice I worked, despite a lack of supporting evidence into its
use. When further examining this condition, I was led to question my own clinical
practice to ensure I was implementing interventions that were in line with the literature.
As a health professional, I felt strongly about working within an evidence-based practice
model.
These concepts listed above have been explored within this thesis, based on the
frameworks of the Biomechanical Model (which is prevalent in Hand Therapy), the
Occupational Adaptation Model (OAM) and the International Classification of

15
Functioning, Disability and Health (ICF). A variety of methodologies have been utilised
to address the above clinical questions, including a scoping review, cross-sectional
study, case series, qualitative methodology and a randomised controlled trial. This forms
the basis of the five publications that comprise Chapters 3 to 7. All studies supported
existing research that passive interventions, including elastic therapeutic tape, have
little impact on this condition. Overall, findings also revealed that:
1. Elastic therapeutic tape for lateral elbow tendinosis is no more effective than
sham taping or eccentric exercises at six-months post randomisation. Evidence
supports activity modification and exercises as successful interventions for this
condition.
2. Lateral elbow tendinosis is complex and treatment should be carefully
considered based on a clear diagnosis, duration of symptoms, awareness of
patient experiences and use of evidence-based interventions.
3. Further examination into elastic therapeutic tape for upper limb conditions is
warranted, especially in relation to comparisons between acute and chronic
conditions.

16
Abbreviations
PRTEE Patient-Rated Tennis Elbow Evaluation
OSAv2.2 Occupational Self-Assessment (version 2.2)
SF-36 Short Form-36
BMH Biomechanical Model of Health
OAM Occupational Adaptation Model
ICF International Classification of Functioning, Disability and Health

17
Thesis Publications
Title Journal Impact
Factor
Page
Article 1: Taylor, R.L., O’Brien, L. & Brown, T. (2014). A scoping review of the use of elastic therapeutic tape for neck or upper extremity conditions. Journal of Hand Therapy, 27(3), 235-246.
2.0 54
Article 2: Taylor, R.L., Brown, T. & O’Brien, L. (2015). Knowledge of and willingness to recommend kinesiotape for upper limb overuse injuries: A comparison of therapists’, general practitioners’ and surgeons’ perspectives. International Journal of Therapy and Rehabilitation, 22(5), 238-245.
N/A 71
Opinion piece: Taylor, R.L., Brown, T. & O’Brien, L. (2015). Using and prescribing kinesiotape as a treatment modality for musculoskeletal disorders. International Journal of Therapy and Rehabilitation, 22(9), 408-409.
N/A 163
Article 3: Wegener, R.L., Brown, T. & O’Brien, L. (2015). The use of elastic therapeutic tape and eccentric exercises for lateral elbow tendinosis: a case series. Hand Therapy, 20(2), 56-63.
N/A 83
Article 4: Wegener, R.L., Brown, T. & O’Brien, L. (2016). A randomized controlled trial of comparative effectiveness of elastic therapeutic tape, sham tape or eccentric exercises alone for lateral elbow tendinosis. Hand Therapy, 1758998316656660.
N/A 997
Article 5: Wegener, R.L., Brown, T. & O’Brien, L. (2016). A qualitative review of patients’ experiences using Kinesio tape for lateral epicondylitis. Submitted to the British Journal of Occupational Therapy (under second revision).
0.935 111

18
Chapter 1 – General Introduction
1.1 Introduction and Overview of Thesis Structure
The aim of this chapter is to:
Provide an outline of the structure of the thesis.
Describe the scope of the problem related to lateral elbow tendinosis in the hand
therapy and rehabilitation context, including current evidence-based practice.
Examine the existing evidence relating to the use of elastic therapeutic tape for
neck and upper limb conditions.
Review health frameworks and conceptual models in relation to how these form
the foundation of the thesis.
This PhD thesis has been completed as a ‘Thesis by Publications’ and, for this
reason, it is comprised as a series of five research papers. Four of these papers are
currently published, whilst one remaining paper is under its second review by the British
Journal of Occupational Therapy. Each publication is linked with the Biomechanical
Model of Health (BMH) (Brown, 1981), the Occupational Adaptation Model (OAM)
(Schkade & Schultz, 1992; Schultz & Schkade, 1992) and the International Classification
of Functioning, Disability and Health (ICF) (WHO, 2007).

19
Chapter 1 details an overview of the background for the research, defines the nature
of the problem and the need to examine current and future clinical practice for
therapists treating this condition. This chapter also covers the literature, scope of
practice and describes the conceptual models and frameworks that underpin this
thesis.
Chapter 2 details the methodologies of each study, as well as the research questions
and aims that underpin the thesis.
Chapter 3 contains the first of the publications, which is a scoping review of evidence
relating to the use of elastic therapeutic tape for neck and upper extremity
conditions. Findings showed that elastic therapeutic tape may play a role in reducing
short-term neck and upper extremity pain, however, future high quality studies that
contribute to this body of knowledge are needed.
Chapter 4 identified the perspectives amongst Australian surgeons, general
practitioners (GPs) and therapists (Physiotherapists and Occupational Therapists) on
the use of elastic therapeutic tape. Findings indicated that therapists were more
likely to rate the use of elastic therapeutic tape as successful and recommend its
clinical use, indicating that they placed greater emphasis on their own clinical
experience than on available research evidence. It is inferred that GPs and surgeons
have a higher level of scepticism for interventions without supporting evidence.
20
More evidence from randomised controlled trials are required to inform
practitioners about the use of elastic therapeutic tape as an intervention.
Chapter 5 explored a case series of four patients who had used elastic therapeutic
tape, in conjunction with an eccentric exercise program, in managing lateral elbow
tendinosis. Findings showed that there may be some clinical benefit in the use of
elastic therapeutic tape, in conjunction with eccentric exercises and activity
modification techniques, for the treatment of lateral elbow tendinosis. However,
more rigorous and comprehensive studies are recommended to further investigate
this intervention.
Chapter 6 describes a randomised controlled trial of 40 participants on the
effectiveness of elastic therapeutic tape for lateral elbow tendinosis, in conjunction
with eccentric exercises and activity modification techniques. This trial compared
three different interventions: (1) elastic therapeutic tape, (2) sham tape, and (3) no
tape. All groups received the same eccentric exercises and activity modification
education. Findings indicated that, at three- and six-months post randomisation,
improvements were made in all three groups as assessed with pain-free grip
strength, the Patient-Rated Tennis Elbow Evaluation (PRTEE), Short Form 36 (SF-36)
and the Occupational Self-Assessment (OSA). However, there were no statistically
significant differences between the three participant groups. We also found no

21
significant side effects or symptom exacerbation with using elastic therapeutic tape
as an intervention strategy. Further studies are needed to assess the use of elastic
therapeutic tape for a range of upper extremity conditions, especially in relation to
its use for acute versus chronic conditions.
Chapter 7 involves a qualitative study that explored the experiences of 11 patients
from the intervention group of the randomised controlled trial. Thematic analysis
was used and findings showed that, regardless of treatment, the consequences of
lateral elbow tendinosis resulted in an adjustment to work and daily activities for a
significant period. Long term changes implemented by the person themselves were
identified as the main contributing factor to improvements in their function, as
opposed to specific treatment modalities. The three key themes were:
1. Frustration at the length of time needed for functional recovery and the impact
on life roles.
2. The importance of long-term self-management.
3. Elastic therapeutic tape was easy to self-apply but was an adjunct in recovery
compared to self-management strategies.
Chapter 8 presents the discussion and conclusion to the thesis. This combines all
research projects, in conjunction with current evidence, and the impact on clinical
practice for hand therapists. It summarises the original contribution this thesis and

22
research has made to the area of hand therapy. Furthermore, limitations of the
studies and suggestions are made for future research.
Appendices are included and contain documents that are relevant to this research
project, such as ethics approvals, assessment proformas and conference
presentations.
1.2 Literature Review
Lateral elbow pain, or ‘tennis elbow/lateral epicondylitis’ as it is commonly
referred to in the literature, is a condition that is known to be difficult for Hand
therapists to treat (Fedorczyk, 2006a). This is due to its long term recovery, considerable
morbidity and financial costs, including those associated with time off work and
prolonged treatment (Burton, Kendall, Pearce, Birrell, & Bainbridge, 2009). It is one of
the most common work-related disorders of the elbow with over 70% of cases being
occupation related, especially amongst individuals who perform forceful and repetitive
activities, such as tradespeople, athletes, and mine workers (Fedorczyk, 2006a). Overall
prevalence in the general population is thought to range from 1% to 5% (Shiri, Viikari-
Juntura, Varonen, & Heliövaara, 2006). Both males and females are equally affected with
the most common age of onset being 40-60 years. Approximately 40% of people will
experience lateral elbow pain at some point in their life and over 50% of these report

23
not being fully recovered at 12-months post onset (Bisset & Vicenzino, 2015; Fedorczyk,
2006b; Gruchow & Pelletier, 1979). Direct costs per case are approximately US$8099,
resulting in a significant economic burdens to the individual, health care system and
society (Bisset & Vicenzino, 2015; Silverstein, Viikari‐Juntura, & Kalat, 2002).
To date, ‘lateral epicondylitis’ and ‘tennis elbow’ are common terms used by
physicians and therapists when describing the clinical diagnosis related to pain
experienced at or around the lateral epicondyle (Fedorczyk, 2006b). However, new
research reveals that these terms are misleading. The suffix ‘itis’ implies an
inflammatory pathology, but extensive histological immunehistochemical and electron
microscopy studies have shown that the condition is degenerative rather than
inflammatory (Stasinopoulos & Johnson, 2006). It has been suggested that the more
appropriate terms for this condition are either (i) lateral elbow tendinosis, or (ii) lateral
elbow tendinopathy (Ashe, McCauley, & Khan, 2004; Stasinopoulos & Johnson, 2006). It
is important to apply the correct diagnostic terminology since the previous labels for this
condition have led to misunderstanding and inappropriate treatment. For the purpose
of this PhD research, the term ‘lateral elbow tendinosis’ is used hereafter.
Understanding the pathophysiology of lateral elbow tendinosis may enable
better targeting of treatment and rehabilitation efforts (Khan, Cook, Bonar, Harcourt, &
Åstrom, 1999; Khan, Cook, Kannus, Maffulli, & Bonar, 2002). Extensive histological,

24
immunehistochemical, and electron microscopy studies have shown that the condition
is degenerative rather than inflammatory. The muscles of the lateral aspect of the elbow
include the brachioradialis, extensor carpi radialis longus (ECRL), extensor carpi radialis
brevis (ECRB), extensor carpi ulnaris (ECU), and supinators (Hausman & Lang, 2014;
Ljung, Lieber, & Friden, 1999; Reichel & Morales, 2013). All of these structures blend
together at the elbow and attach to the humerus as a merged extensor origin. These
structures become distinct only in the forearm (Hausman & Lang, 2014). Anatomical
studies of the lateral aspect of the elbow demonstrate that there is often considerable
contact between the extensor carpi radicalise brevis (ECRB) and the lateral edge of the
capitellum, especially with repeated contraction of the wrist extensor muscles, leading
to ‘wear and tear’ of the tendon. Bowing and stretching of the tendon occur with the
elbow in extension regardless of wrist position. Subsequently, degeneration at the origin
of the ECRB muscle results from an increased presence of fibroblasts, vascular
hyperplasia, proteoglycans, and glycosaminoglycans together with disorganised and
immature collagen which all occur in the absence of inflammatory cells (Cook & Purdam,
2009b).
It is still not clear why tendinosis is painful, given the absence of inflammatory
cells, nor is it known why collagen fails to mature. The true cause of pain may be
mechanical discontinuity of collagen fibers or biochemical irritation that results from
25
damaged tendon tissue that activates nociceptors (Chourasia et al., 2012; Cook &
Purdam, 2009a). There may also be other potential mechanisms of tendon pain
including the involvement of other tissues such as nerves, vessels and bones that are
intimately related to tendon (Khan, Cook, Maffulli, & Kannus, 2000b).
1.2.1 Clinical presentation and diagnostic tests
As with most conditions managed by hand therapists, it is important that clinical
symptoms and assessments of lateral elbow tendinosis are correlated with relevant
imaging findings and advice from the referring Specialist/Surgeon where applicable. A
skilled therapist should elicit appropriate information via a person’s history that will
direct a specific physical examination of key structures that need to be assessed.
Magnetic Resonance Imaging (MRI) is still the gold standard in diagnosing lateral
elbow tendinosis (Geoffroy, Yaffe, & Rohan, 1994; Miller, Shapiro, Schultz, & Kalish,
2002; Vicenzino, Brooksbank, Minto, Offord, & Paungmali, 2003). However, in general,
lateral elbow tendinosis can be a relatively straightforward condition to identify in the
clinic, with the key physical examination features being (i) reproduction of pain in
response to direct palpation over the lateral epicondyle (or up to 5mm anterior or distal)
and (ii) pain provocation in response to tests of forearm extensor muscle function
(Fedorczyk, 2006b; Valdes & LaStayo, 2013). In most cases, there is often a deficit in

26
strength in these muscles, especially with a reduced ability to tolerate load with the
elbow extended. Common reported symptoms are aching in the evening and stiffness
in the morning. Gripping, resisted wrist extension, radial deviation, finger extension, and
forearm supination can produce pain depending on the irritability of the tissues
(Wilhelm, 2009).
Specifically, there are also a number of provocative tests that are typically used
to diagnose lateral elbow tendinosis (Fedorczyk, 2006b; MacDermid & Michlovitz, 2006).
These include:
1. Chair Test – lifting the back of a chair with three digits (thumb, index and middle
fingers), whilst extending the elbow, provokes pain at the lateral epicondyle.
2. Cozens Test - The elbow is extended and then a fist is made with wrist extension
against resistance. This is followed by pronation and passive radial deviation to
examine pain at the lateral epicondyle.
3. Mill’s Test – passively moving the elbow in pronation with wrist flexion then
elbow extension provokes pain at the lateral epicondyle.
4. Maudsley Test – resisted middle finger extension with the forearm in pronation
provokes pain at the lateral epicondyle.
Apart from MRI, the Mill’s Test has the highest diagnostic accuracy with specificity
of 100% in some studies. It must be noted that the sensitivity of these tests are not

27
discussed in detail as they have not been recently or thoroughly examined to determine
their diagnostic accuracy or clinical usefulness (Valdes & LaStayo, 2013). It is important
to consider that differential diagnoses for lateral elbow tendinosis can include cervical
radiculopathy, neurovascular entrapment, and radial tunnel syndrome (Vicenzino &
Wright, 1996). It is beyond the scope of this PhD to discuss all the tests or pathologies
of the elbow.
1.2.2 Treatment for lateral elbow tendinosis
To date, there has been consensus that the recommended management of
tendinosis is through conservative treatment (Vicenzino, 2003). While many treatments
for lateral elbow tendinosis have been researched, including friction massage,
ultrasound, acupuncture, orthotics, splinting, shock wave therapy, oral non-steroidal
anti-inflammatory medications and surgery, many have small short-term effects and few
have shown consistent effectiveness over other treatments (Bisset & Vicenzino, 2015;
Buchbinder, Green, Bell, et al., 2002; Buchbinder, Green, White, et al., 2002; Green et
al., 2002; Green et al., 2001; Labelle et al., 1992; Smidt et al., 2002; Struijs et al., 2001).
From the available evidence, there is emerging support for exercise as an
important aspect of the management of lateral elbow tendinosis. Systematic reviews
have concluded that eccentric exercises have had some positive effect on clinical
28
outcomes such as pain, function, patient satisfaction and return to work amongst this
population (Cullinane, Boocock, & Trevelyan, 2014; Raman, MacDermid, & Grewal,
2012). It has been suggested that eccentric loading may assist with tendon rehabilitation
by improving collagen alignment and stimulating collagen cross-linkage formation, both
of which can improve tensile strength. Although most studies did not adequately
address exercise dosages or include exercise descriptions that could be reproduced,
Raman, MacDermid, and Grewal (2012) suggested that a protocol of eccentric exercises
performed for three sets of 10-15 repetitions daily for approximately 6-12 weeks has
the best current supporting evidence.
Despite the reported benefits of eccentric exercises, a barrier in conservative
management is often the considerable pain reported by people with elbow tendinosis
which directly impacts on their ability to effectively undertake a therapeutic exercise
program (Malliaras, Maffulli, & Garau, 2008). The pain also directly impacts patients’
abilities to engage in many daily functional activities that require elbow movement, such
as keyboarding, driving a car, lifting objects off a shelf, doing up buttons, and
handwriting. The hand therapists’ management of lateral elbow tendinosis revolves
primarily around modulating tendon pain, as pain is the primary presenting and limiting
factor experienced by this patient group (Carlo, 2009; Clarke, Ahmad, Curtis, & Connell,
2013). Additional goals of rehabilitative treatment are to maintain movement and

29
strength, and to develop endurance over time to increase function and maintain
participation in work and meaningful activities (Cook & Purdam, 2013).
One suggested modality for managing pain during elbow motion and exercise is
the application of elastic therapeutic tape (Kase, Tatsuyuki, & Tomoko, 1996). The next
section describes how elastic tape is thought to work, and how it may be applied in the
management of tendinosis.
1.2.3 Using elastic therapeutic tape for tendinosis
It is proposed that elastic therapeutic tape may play a role in biomechanically
unloading the affected tendon, thereby reducing symptoms and allowing patients to
undertake appropriate strengthening exercises (Bassett, 2010). Developed in the 1970’s
by Dr Kenzo Kase, a chiropractor, elastic therapeutic tape is a relatively new modality
used for treating a variety of injuries (Kase, Tatsuyuki, & Tomoko, 1996). Since that time,
different names and brands have emerged and it has gained increased recognition
especially after it was donated to 58 countries for use during the 2008 Olympic Games
and was used by many high-profile athletes. Traditional taping methods for elbow
tendinopathy have been examined in clinical studies (Amro et al., 2010; Vicenzino,
Brooksbank, Minto, Offord, & Paungmali, 2003) with results demonstrating some short-
term improvements in pain-free grip strength; however, no studies have explored the

30
use of elastic therapeutic tape for this condition with long term follow-up (Taylor,
O'Brien, & Brown, 2014).
Although unsupported by evidence, the proposed mechanisms of elastic
therapeutic tape include alleviating pain, correcting muscle function, restoring
functional movement patterns, improving circulation, and relieving abnormal muscle
tension (Bassett, 2010; Kase, Tatsuyuki, & Tomoko, 1996; Moore, 2012). In particular, it
is reported that the application of elastic therapeutic tape over stretched muscle will
create convolutions in the person’s skin which subsequently reduce the pressure in the
mechanoreceptors that are located below the dermis, thereby decreasing nociceptive
stimuli (Parreira et al., 2014). Through these mechanisms, it is hypothesised that elastic
therapeutic tape can assist in reducing symptoms and thus allow patients to undertake
appropriate rehabilitative exercises (Bassett, 2010).
Recommended tape application methods are outlined in ‘Clinical Therapeutic
Applications of the Kinesio Taping Method’ (Kase, 2003). Elastic therapeutic tape is
designed to allow for a longitudinal stretch of up to 140% of its resting length; however,
the majority of tape applications are applied between 25-50% and occasionally up to
100%. The tape has no horizontal stretch and it is designed to approximate the elastic
qualities of the human skin. There are currently no available guidelines on how to
achieve consistency with the tape’s stretch and application; therefore, therapists must

31
rely on their own clinical judgement during tape application (Kase, 2003; Kase,
Tatsuyuki, & Tomoko, 1996). In particular, this factor is an important consideration when
teaching patients or family members to re-apply the tape and may affect compliance
with treatment.
Despite its popularity and widespread clinical use, there is relatively little
evidence to support the effectiveness of elastic therapeutic tape, let alone for specific
neck and upper extremity conditions. To date, evidence regarding the effectiveness of
elastic therapeutic tape has relied predominantly on case reports, small pilot studies and
research on healthy participant groups (Bassett, 2010).
1.3 Conceptual frameworks
Evidence-based practice in the absence of a good foundation in theoretical
models is problematic because it is difficult to evaluate research findings without
understanding theory (Peachey-Hill & Law, 2000). For the research presented in this
thesis, an understanding of theoretical conceptual models and frameworks underpinned
the assessments and interventions to both measure and facilitate change in patients’
occupational performance. This knowledge provides the explanatory power on how
interventions guide change in our patients’ function (Ikiugu, Smallfield, & Condit, 2009).
32
Two models and one framework have been selected to provide a theoretical
foundation for this PhD program: (1) the Biomechanical Model of Health (BMH) (Brown,
1981), (2) The Occupational Adaptation Model (OAM) (Schkade & Schultz, 1992; Schultz
& Schkade, 1992), and (3) the International Classification of Functioning, Disability and
Health (ICF) (WHO, 2007). These models and frameworks were chosen to guide the
biopsychosocial approach to this study. Whilst hand therapy has traditionally used a
biomechanical approach towards treatment, it was important to include the OAM and
ICF to address broader psychosocial components.
1.3.1 Biomechanical Model of Health (BMH)
The BMH (Seidel, 1998) has commonly been used in the treatment of patients
with musculoskeletal conditions, such as lateral elbow tendinosis, within a rehabilitation
setting. It has intuitive appeal and is supported by a wealth of biological findings
(Mishler, 1981). The BMH has foundations in assessing the symptoms of an injury or
condition to determine what is not functioning optimally. Once the pathology is
identified, treatment aims to eliminate, repair or correct the existing pathology through
medical methods. This model incorporates exercise and activity to reduce deficits in
occupational performance components and emphasises that the reduction of physical
deficits will promote independence in daily activities (Cole & Tufano, 2008; Jackson &
33
Schkade, 2001b). The therapist considers the patient’s goals; however, treatment
focuses on overcoming deficits, improving range of motion, increasing mobility and
prescribing strengthening exercises (Cole & Tufano, 2008). The BMH is consistent with
the theories that underpin the use of elastic therapeutic tape and eccentric exercises in
managing lateral elbow tendinosis.
A limitation of using this model in isolation is that it may not provide the person
with much opportunity to plan and participate in the process of therapy. The role of the
person can become passive; therefore, the BMH does not incorporate all the strengths
of occupational therapy service delivery (Cole & Tufano, 2008). For this reason, an
additional occupational model and a health framework were also used as the foundation
of this thesis.
Figure 1: Biomechanical Model of Health (Brown, 1981; Kielhofner, 2009)
Joint Range of Motion
Physical Endurance
Muscle Strength
34
1.3.2 The Occupational Adaptation Model (OAM)
The OAM developed by Schkade and Schultz (1992) differs from other models
due to its focus on one’s internal adaptation (ability to adjust oneself to different
conditions and environments) as opposed to occupational performance. In doing so, this
model has great applicability to the specialty area of Hand Therapy. Therapists often
assume that, as clients recover function (i.e. improved goniometer measures of Range
of Motion, increased grip strength and return to work), they will become more adaptive.
However, function and adaptation are not the same – increased function does not
necessarily mean more adaptation, especially in the case of long-term conditions.
Therapists may incorrectly assume that as the patient acquires more functional skills,
adaptation is occurring; however, the person’s internal adaptation may actually remain
unchanged (Schultz & Schkade, 1992).
Occupational adaptation is described as a normative process that leads to
competence in occupational functioning. This model proposes that occupation involves
the means through which adaptation occurs and an end for which functional adaptation
is desirable (Schkade & Schultz, 1992; Schultz & Schkade, 1992). Illness or trauma may
disrupt this internal process and result in maladaptive responses to daily occupational
challenges. In this model, the therapist’s role is to facilitate restoration of a functional
internal adaptation process (Jackson & Schkade, 2001a).

35
In relation to this thesis, the OAM complements the BMH as it does not exclude
biomechanical and rehabilitation principles for therapeutic interventions (Jackson &
Schkade, 2001a). However, the primary focus of treatment is placed on the patient’s
meaningful occupational role, involvement in the therapy process, and the adaptation
outcome. From the literature, lateral elbow tendinosis is recognised for having a
significant period of time during which people will experience occupational dysfunction.
As discussed previously, this condition frequently takes years to improve, during which
time people are required to develop adaptations to enable resumption of meaningful
occupations.
An adaptive response results in the person achieving greater relative mastery in
their occupational activities which is measured by three properties – efficiency (the use
of time, energy and resources), effectiveness (the degree to which one achieves a
desired result) and satisfaction (the extent to which the outcome was personally
satisfying and well-regarded) (Schkade & Schultz, 1992). Schultz and Schkade (1992)
further state that the person’s response to both intrinsic (personal) and extrinsic
(environmental) factors will dictate their final outcome. A successful response will result
in ‘occupational performance with mastery and satisfaction’ or a successful return to
meaningful occupations.

36
The diagram of the OAM (presented below) contains three elements – (i) the
person, (ii) the occupational environment and (iii) the interaction of the two as they
come together in occupation (Schkade & Schultz, 1992; Schultz & Schkade, 1992). The
occupational adaptation model can be conceptualised as having two major processes:
(1) the first is the process of moving from the press for mastery to an occupational
response, and (2) the second part is the process by which individuals make adaptive
responses through relative mastery to an occupational response.
Figure 2: Occupational Adaptation Model (Schultz & Schkade, 1992)
In the hand therapy setting, the OAM has great applicability as a large majority
of patients sustain lengthy disruptions to their everyday function, requiring them to
come forth with an adaptive response to deal with their injury. The process from the

37
onset of lateral elbow tendinosis to return to activities of daily living (ADLs) is considered
to be one of ongoing adaptation. Therapists have often focused on treating the person’s
condition, neglecting to address the illness experience (Schultz & Schkade, 1992).
This is an important concept in relation to this PhD as it focuses on physical
dysfunction, but also the notion of understanding an individual’s perspective and
experience of adaptation.
1.3.3 The International Classification of Functioning, Disability, and Health
(ICF)
Another conceptual framework that underpins this thesis is the International
Classification of Functioning, Disability, and Health (ICF) (WHO, 2007). This is structured
around the following broad components: (i) body function and structure, (ii) activities,
(iii) participation, (iv) environmental factors and (v) personal factors.
Within the ICF, functioning and disability are viewed as complex interactions
between the health condition of the individual, the environmental context, as well as
personal factors (WHO, 2007). It identifies these dimensions as being interactive and
dynamic, as opposed to linear and static. The ICF is able to assist health practitioners in
assessing the degree of disability, even though it is not a measurement instrument
(Cieza et al., 2002b). All aspects of a person’s life (development, participation and
environment) are incorporated into the ICF instead of focusing solely on a ‘diagnosis’.

38
The ICF is an important framework for this research and it complements the BMH
which forms the basis for the use of elastic therapeutic tape. The ICF acknowledges the
importance of understanding disease and dysfunction in health care (similar to the
BMH); however, it further recognises the person as a whole, including their lived
context. Identifying the limitations of function through the ICF can provide important
information to plan and implement interventions. It can be applied across cultures, age
groups and genders, making it highly suitable for various populations. It also supports
the OAM in this thesis by incorporating a holistic approach to the assessment and
management of lateral elbow tendinosis.
Figure 3: International Classification of Functioning, Disability, and Health (ICF) (WHO, 2007)
39
1.4 Chapter Summary
Whilst there appears to be some anecdotal evidence that merits using elastic
therapeutic tape as an addition to existing treatment modalities, broader, systematic
examination of this treatment is needed in order to clarify its effectiveness for neck and
upper extremity conditions. The Biomechanical and Occupational Adaptation Models,
as well as the ICF, may assist us to understand how the treatment may or may not be
effective. The next chapter outlines the origins of each research question and study that
are subsequently answered in each publication (Chapters 3 to 7). The aims and
methodologies for each study will also be outlined.
40
Chapter 2 – Methodology
2.1 Introduction
This thesis proposes a research program to investigate the effectiveness of
elastic therapeutic tape in managing lateral elbow tendinosis. It is anticipated that the
results of this research study will inform the development of a clinical pathway for hand
therapists for the management of lateral elbow tendinosis with the use of elastic
therapeutic tape.
This chapter will outline the five research questions that underpin the
foundations of this thesis which are subsequently addressed in the publications that
form Chapters 3 to 7. The separate methodologies used within each publication will also
be outlined and justified, including a scoping review, cross-sectional study, case series,
randomised controlled trial and a qualitative study.
2.2 Research questions
Specific research questions of the thesis are:
1. What is the current evidence relating the use of elastic therapeutic tape in
treating neck and upper extremity conditions?

41
2. What are the current perspectives amongst hand therapists, general
practitioners and hand surgeons on the use of elastic therapeutic tape and how
often is it used or recommended?
3. What is the preliminary evidence into the benefit of elastic therapeutic tape and
eccentric exercises for the treatment of lateral elbow tendinosis?
4. Is the application of elastic therapeutic tape according to the ‘Clinical
Therapeutic Applications of the Kinesio Taping Method’ manual (Kase, 2003)
(with the tape applied on tension), in conjunction with an eccentric exercise
program and activity modification advice, more effective than (i) a sham
application ( i.e. the tape applied with no stretch), or (ii) eccentric exercises
alone, in people with lateral elbow tendinosis? Are the benefits of three months
of treatment using elastic therapeutic tape sustained six-months post
intervention?
5. What are the experiences of people using elastic therapeutic tape for lateral
elbow tendinosis?

42
2.3 Materials and Methods
2.3.1 Research Question 1: What is the current evidence relating the use of
elastic therapeutic tape in treating neck and upper extremity conditions?
Aim: To synthesise the available evidence relating to the use of elastic
therapeutic tape in treating neck and upper extremity conditions.
Methodology: Scoping review.
Level of Evidence: N/A
A scoping review was used to address this research question as it includes a
broader range of studies and articles, including both empirical and non-empirical
sources of information, especially when there is a lack of randomised controlled
trials available.
Search strategy:
Relevant English, peer-reviewed documents were identified from a search of
OVID Medline, CINAHL and ProQUEST. Grey literature in ProQUEST Dissertations
and Theses were also included. The search was conducted between July and
September 2013. As this scoping review aimed to include all studies, no
limitations were placed in terms of and publication type.

43
Data Collection:
Where possible, data was extracted regarding the recommended application and
wear-time of elastic therapeutic tape in the treatment of neck and/or upper
extremity disorders. Participant outcomes examined were pain, range of motion,
strength and patient preference.
Data Analysis:
Study quality was assessed based on the McMaster Guidelines for Critical Review
of Quantitative Studies which examines research approach, methodology,
sample size, intervention, outcome measures and results. Studies were also
classified using the Oxford Level of Evidence.
2.3.2 Research Question 2: What are the current perspectives amongst Hand
Therapists, General Practitioners and Hand Surgeons on the use of elastic
therapeutic tape and how often is it used or recommended?
Aim: To gain insight into current perspectives on the use of elastic therapeutic
tape amongst health professionals (occupational therapists and
physiotherapists), general practitioners and hand surgeons.
Methodology: Cross-sectional study.
Level of Evidence: 4

44
This cross-sectional study used a self-report survey to gather data from
respondents. Information included number of years in clinical practice, number
of patients treated each week presenting with conditions such as ‘tennis elbow’,
self-rating of knowledge regarding the use and purpose of kinesiotape, perceived
level of success with tape when used, and reasons for recommending/not
recommending the tape.
Participants:
Inclusion criteria included being a qualified physiotherapist or occupational
therapist registered with the Australian Hand Therapy Association (AHTA) or a
qualified medical practitioner with experience in the treatment of upper limb
injuries.
Data Collection:
A convenience sampling approach was used to recruit participants. All 472
members of the Australian Hand Therapy Association (AHTA), 67 general
practitioners and surgeons in South-East Queensland and 24 hand therapists and
surgeons in Victoria were given the questionnaire via email, postage or in person.
Data Analysis:
Data was analysed using SPSS statistical software, version 20. Comparisons
between therapists, GPs and surgeons on continuous outcomes were made

45
using one-way ANOVA tests. Post-hoc comparisons were made using the Tukey
HSD test. Linear regression was used to examine which variables affected the
level of recommendation of the tape. Chi-square tests examined barriers to the
use of kinesiotape and were grouped into discrete categories based on
responses to five listed categories. Participants were provided with the
opportunities to use free text in this section; however, none of the participants
did so. Power calculations were not completed for this study as cluster sampling
was used (e.g. all members of the Australian Hand Therapy Association were
provided with the survey, as well as all upper limb Surgeons from South East
Queensland).
2.3.3 Research Question 3: What is the preliminary evidence into the benefit
of elastic therapeutic tape and eccentric exercises for the treatment of lateral
elbow tendinosis?
Aim: To examine outcomes of a retrospective case series of patients who used
elastic therapeutic tape and eccentric exercises for the treatment of lateral
elbow tendinosis.
Methodology: Case series.
Level of Evidence: 4.
Participants:

46
All four patients were treated by the same hand therapist and received
application of the tape for varying durations from one to three months. The tape
was applied in the same way for each patient in conjunction with an evidence-
based standard daily exercise program including heat, stretches, progressive
eccentric exercises and the use of compression as needed.
Data Collection:
Descriptive and retrospective review involving four patients who underwent
rehabilitation with the use of elastic therapeutic tape, in conjunction with
eccentric exercises and activity modification techniques, for treatment of lateral
elbow tendinosis. Outcome measures included a 10 cm Visual Analogue Scale
(VAS) to evaluate subjective pain levels and the Jamar dynamometer to measure
objective grip strength measurements.
Data Analysis:
Descriptive statistics and analyses of the outcome measures were recorded and
compared.

47
2.3.4 Research Question 4: Is the application of elastic therapeutic tape
according to the ‘Clinical Therapeutic Applications of the Kinesio Taping
Method’ manual (with the tape applied on tension), in conjunction with an
eccentric exercise program and activity modification advice, more effective
than: (i) sham taping (application with no stretch); or (ii) eccentric exercises
alone; for people with lateral elbow tendinosis?
Additionally, are the benefits of three months of treatment using elastic
therapeutic tape sustained six-months post intervention?
Aim: To assess the effectiveness of elastic therapeutic tape (in conjunction with
an eccentric exercise program and activity modification advice) in treating lateral
elbow tendinosis in adults when compared to sham taping or no taping (i.e.
reduced pain, increased strength and improved functional outcomes).
Methodology: Randomised Controlled Trial (RCT).
Level of Evidence: 1B.
This was a randomised controlled trial of 40 participants with lateral elbow
tendinosis who received (i) elastic therapeutic tape, (ii) sham tape, and (iii) no
tape, over a 12-week period (four weekly and 4 fortnightly sessions) with a 6
month follow up. All participants received eccentric exercises and advice on
activity modification techniques.
48
Participants:
Participants with lateral elbow tendinosis, aged between 18 and 80 years, were
recruited through three private hand therapy practices. Selection criteria was
based on medical investigations confirming lateral elbow tendinosis (e.g. MRI),
or provocative tests completed by the treating therapist. Participants were
excluded if they had co-morbidities, any contraindications to the use of taping,
inability to understand written material in English and inability to give informed
consent.
Data Collection:
40 participants were randomly allocated to receive three different approaches
for the management of lateral elbow tendinosis. Participants in all three groups
received the same evidence-based exercise program and advice on activity
modification techniques, including ergonomic modifications and how to avoid
aggravating tasks. Exercises and the application of tape (for the three participant
groups) were reviewed at each session to further enhance adherence to therapy.
Primary outcomes were pain and level of disability as measured by the Patient
Rated Tennis Elbow Evaluation (PRTEE) and pain-free grip strength assessments
using the Jamar dynamometer. Secondary outcome measures were overall
health status as measured by the Short Form 36 (SF-36), the Occupational Self-
49
Assessment (OSA v 2.2). All of these are standardised outcomes measures. In
particular, the PRTEE was specifically chosen for this study due to its high validity,
reliability, reproducibility and sensitivity to change amongst a ‘tennis elbow’
population. Other outcome measures, such as the Disability of the Arm, Shoulder
and Hand (DASH) and the Upper Extremity Functional Index (UEFI), have been
used in clinical practice to measure elbow conditions; however, these measures
are general in nature and have been found to not accurately assess the specific
symptoms and functions of an individual joint. Therefore, the PRTEE was the
most appropriate choice as a primary outcome measure.
Data Analysis:
Data analysis was conducted by the un-blinded primary researcher and
independently checked by a statistician who was blinded to group allocation. All
data was coded for analysis. Differences in primary and secondary outcomes
between groups were compared using intention-to-treat analysis. Baseline
participant characteristics in the three groups were compared using one-way
ANOVA for continuous variables (age) and chi-square tests for categorical
variables (gender, work status). Outcomes were compared over the follow-up
period with one-way ANOVA for all variables; however, linear mixed model
analysis was also used for primary outcome variables (PRTEE and grip strength)

50
due to missing data amongst these measures. The Statistical Package for Social
Sciences (SPSS version 20) was used for all analyses (SPSS, 2011).
2.3.5 Research Question 5: What are the experiences of people using elastic
therapeutic tape for lateral elbow tendinosis?
Aim: To investigate people’s experience with using elastic therapeutic tape,
adherence with treatment, and the perceived impact of using the tape on their
recovery, function and return to pre-injury roles.
Methodology: Qualitative Study.
Thematic analysis was the methodological framework used to categorise data
into patterns and develop themes in order to find meaning.
Level of Evidence: N/A.
Participants:
Qualitative interviews were undertaken with 11 participants from the
intervention group of the randomised controlled trial at six-months post
randomisation.
Data Collection:
The qualitative interviews were semi-structured and conducted face-to-face to
encourage participants to freely express their own views and experiences,

51
specifically in relation to using the tape. Guiding questions were drafted by the
primary researcher and piloted amongst three other therapists to review the
appropriateness of questions. Following minor grammatical changes, the
interviews were implemented in person and prompts were used when required.
All interviews were recorded using a digital voice recorder and transcribed for
analysis by the first author. The following specific areas of interest were
explored:
1. Perceptions of impact on overall function over the six months after the
commencement of the taping intervention.
2. Patient experiences during everyday activities.
3. Experiences of using elastic therapeutic tape as a treatment modality.
Data Analysis:
Transcripts of the interviews were analysed using a three-step process. First level
coding described and categorised responses; second level coding identified
patterns or groups in the first level codes; third level coding involved interpreting
these to find meanings behind the perceptions expressed by the participants.
Contextual information from field notes was also used (e.g. body language to
clarify the meaning of some texts) and a reflective diary was kept after each
interview. Transcripts and codes were then checked with two of the interviewees

52
to ensure that the interpretation of the findings accurately represented
participants’ perceptions regarding their experience.
2.6 Chapter Summary
This chapter has outlined the five research questions that form the foundation of this
thesis, in addition to the selection of various methodologies to address these questions.
The following chapters will address the specific details of each individual study, starting
with the next chapter which is a scoping review of the evidence into the use of elastic
therapeutic tape for neck and upper extremity conditions.

53
Chapter 3 - A scoping review of the use of elastic
therapeutic tape for neck and upper extremity conditions
3.1 Introduction
Chapter Three contains both an extract from the manuscript of Study 1, as well
as the full article, which is published in ‘Journal of Hand Therapy’. This is the first of five
publication chapters and presents a scoping review on the current evidence for the use,
implementation and effectiveness of elastic therapeutic tape for neck and upper
extremity conditions in clinical practice.
3.2 Chapter Contents
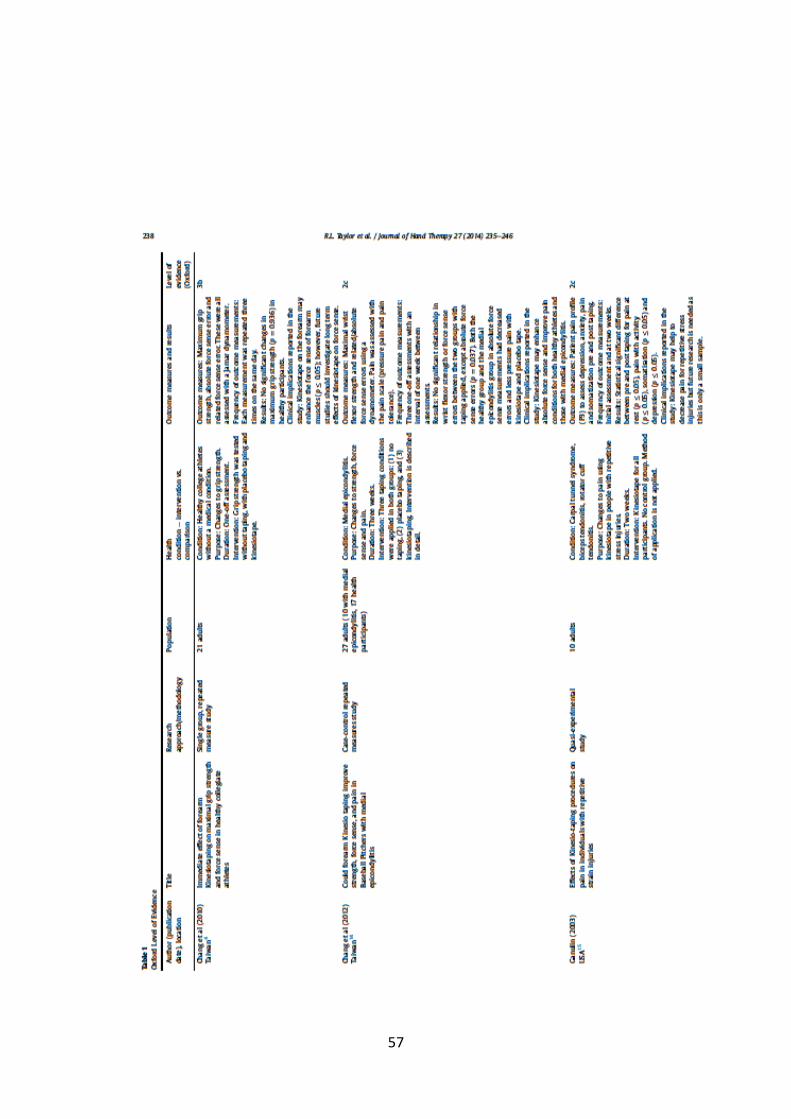
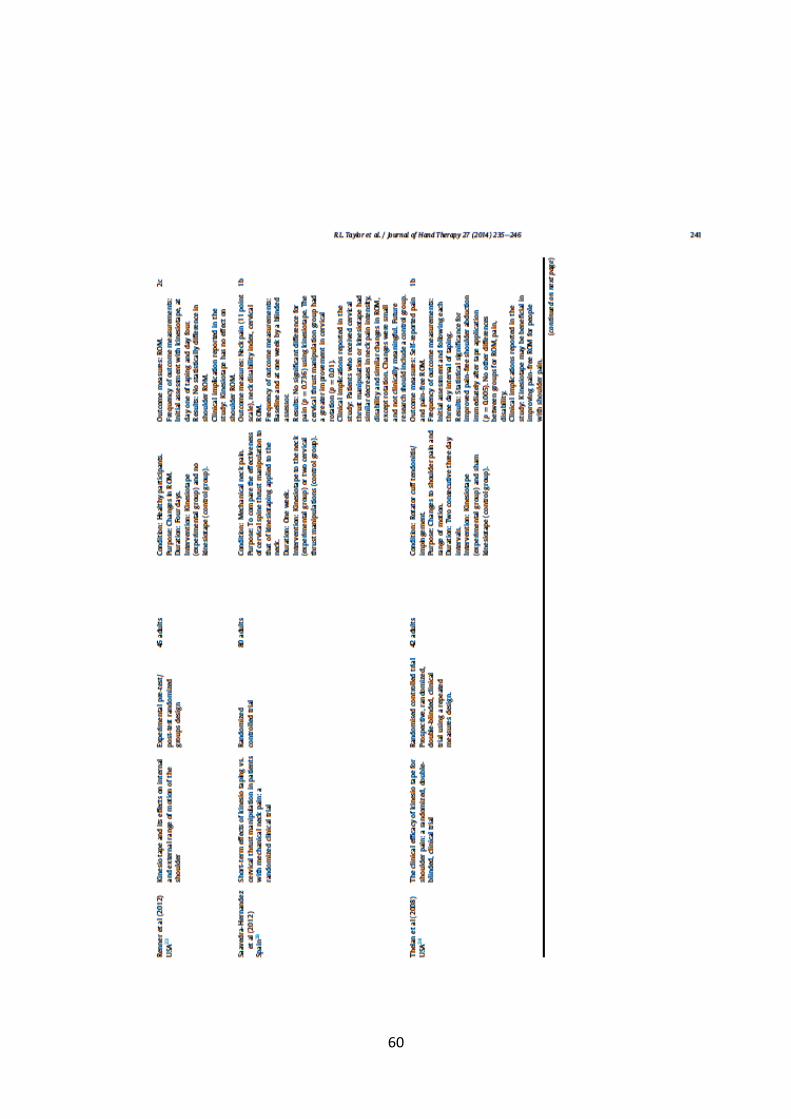
Taylor, R.L., O’Brien, L. & Brown, T. (2014). A scoping review of the use of elastic
therapeutic tape for neck or upper extremity conditions. Journal of Hand Therapy, 27,
235-246.
Date submitted: 3rd December 2013
Date of resubmission: 20th February 2014
Date of acceptance: 10th March 2014
Date of publication in hard copy: July 2014

54

55

56
57

58

59
60

61

62

63

64
65
3.3 Impact of the study
Journal Metrics:
Source Normalized Impact per Paper (SNIP) - 0.762
Impact per Publication (IPP) – 1.331
SCImago Journal Rank (SJR) – 0.547
Despite its popularity and widespread clinical use, this study revealed that there
is relatively little evidence to support the effectiveness of elastic therapeutic tape for
specific neck and upper extremity conditions. These findings provide useful information
for therapists using this intervention, especially in relation to the use of evidence-based
practices. At present, therapists who incorporate elastic taping in their clinical practice
are required to construct a treatment plan using the manufacturer’s information, their
own experience, and previous clinical observations. This exposes them to the risks
associated with prescribing a treatment modality that has uncertain clinical benefits,
cost-effectiveness, and/or safety. It is important for therapists to be aware of these
considerations.

66
3.4 Chapter Summary
The study presented in this chapter specifically examined 14 documents relating
to the use of elastic therapeutic tape for neck and upper extremity disorders from
searches in OVID Medline, CINAHL, ProQUEST and ProQUEST Dissertations. The key
findings of this study were:
To date, evidence regarding the effectiveness of elastic therapeutic tape has
relied predominantly on case reports, small pilot studies and research on healthy
participant groups.
There appears to be some anecdotal evidence that merits using elastic
therapeutic tape as an addition to existing treatment modalities, but broader,
systematic examination of this treatment is needed in order to clarify its
effectiveness for neck and upper extremity conditions.
It must be acknowledged that, due to the small sample size of the seven RCT’s
included in this scoping review, the lack of significant findings may represent a
Type II error. These studies may have concluded that there was no difference
between treatment groups when, in fact, there may have been a difference but
the study was not adequately powered.
No side effects or adverse events were documented in any of the studies.

67
Overall, this is a topic with limited high quality published research. Ideally, future
studies would be multi-centred, include an adequate sample size/population,
follow-up participants for at least 6 months or longer, and consider the cost-
effectiveness of elastic therapeutic tape compared to other existing
interventions for neck and upper extremity disorders.

68

69
Chapter 4 - A comparison of hand therapists’, general
practitioners’ and surgeons’ perspectives on the use of
elastic therapeutic tape
4.1 Introduction
This chapter specifically explores the experiences and opinions of
physiotherapists, occupational therapists, general practitioners and hand surgeons on
the use of elastic therapeutic tape for upper extremity disorders in clinical practice.
This cross-sectional study used a self-report survey to gather data from
respondents. Information included number of years in clinical practice, number of
patients treated each week presenting with conditions such as ‘tennis elbow’, self-rating
of knowledge regarding the use and purpose of elastic therapeutic tape, level of success
with tape when used, and reasons for recommending/not recommending the tape. The
full article is included in this chapter and is published in ‘International Journal of Therapy
and Rehabilitation’.

70
4.2 Chapter Contents
Taylor, R.L., Brown, T. & O’Brien, L. (2015). Knowledge of and willingness to recommend
kinesiotape for upper limb overuse injuries: A comparison of therapists’, general
practitioners’ and surgeons’ perspectives. International Journal of Therapy and
Rehabilitation, 22(5), 238-245.
Date submitted: 13th January 2014
Date of resubmission: 6th February 2015
Date of acceptance: 17th February 2015
Date of publication in hard copy: May 2015

71

72

73

74

75

76

77

78
4.3 Impact of the Study
Journal Metrics:
Source Normalized Impact per Paper (SNIP) – 0.27
Impact per Publication (IPP) – 0.337
SCImago Journal Rank (SJR) – 0.173
Results of this study supported the findings from the scoping review in Study 1. It is clear
from this survey that the use of elastic therapeutic tape is common amongst therapists
in clinical practice, even though it is not supported by evidence gained from high quality
randomised controlled trials.
4.4 Chapter Summary
This study has shown that hand therapists, GPs and Surgeons have differing
perceptions on the use of elastic therapeutic tape. Although overall perceptions of the
tape’s purpose, usefulness and effectiveness amongst the three groups were only low
to moderate, therapists are more likely to report higher understanding levels and
subsequent higher levels of recommendation and success with its use compared to GPs
and surgeons. GPs and surgeons were less likely to recommend the use of elastic

79
therapeutic tape due to limited understanding of its potential use and/or doubts
regarding its effectiveness in clinical practice.
This survey is consistent with existing literature that states there is a need for
more evidence into the use of elastic therapeutic tape and long-term follow-up into its
reported benefits.

80
81
Chapter 5 - The use of elastic therapeutic tape and
eccentric exercises for lateral elbow tendinosis: a case
series.
5.1 Introduction
Chapter 3 aimed to identify the current evidence on the use of elastic therapeutic
tape and revealed that there was limited high quality evidence available. This was built
on in Chapter 4 in which results showed that therapists were more likely to use and
recommend elastic therapeutic tape (compared to GP’s and Surgeons) despite limited
evidence into its use.
This chapter comprises of Study 3 which arose based on the author’s clinical
experience with using elastic therapeutic tape for lateral elbow tendinosis. The objective
of this study was to retrospectively examine four patients who underwent rehabilitation
with the use of elastic therapeutic tape, in conjunction with eccentric exercises and
activity modification techniques, for treatment of lateral elbow tendinosis. The full
article is included in this chapter and is published in ‘Hand Therapy’.

82
5.2 Chapter Contents
Wegener, R.L., Brown, T. & O’Brien, L. (2015). The use of elastic therapeutic tape and
eccentric exercises for lateral elbow tendinosis: a case series. Hand Therapy, 20(2), 56-
63.
Date submitted: 1st January 2015
Date of resubmission: 8th March 2015
Date of acceptance: 13th March 2015
Date of publication in hard copy: April 2015

83

84

85

86

87
88

89

90

91
5.3 Impact of the Study
Journal Metrics:
Source Normalized Impact per Paper (SNIP) - 0.162
Impact per Publication (IPP) - 0.133
SCImago Journal Rank (SJR) - 0.114
This retrospective case series suggests preliminary benefit for the use of elastic
therapeutic tape and eccentric exercises in treating patients with lateral elbow
tendinosis. However, conclusions by health professionals cannot be drawn from this
study on the effectiveness of elastic therapeutic tape alone, or in combination with
activity modification and exercise without more rigorous examination.
For this reason, it is important to proceed to a randomized controlled trial as
these results cannot confidently conclude results were gained from the tape, as
opposed to patients who may experience ‘natural recovery’ of this condition.
Additionally, as elastic therapeutic tape is reported to have benefit through the
tape’s elastic properties, including a control group involving sham tape will provide
important findings. Although this group will receive an un-blinded ‘placebo
intervention’, these participants will not know they are receiving a treatment that is
not the targeted clinical intervention being examined for its clinical effectiveness.
The role of a possible placebo effect from the tape warrants further investigation.

92
5.4 Chapter Summary
This study provided the potential for preliminary support of elastic therapeutic
tape for lateral elbow tendinosis, in combination with eccentric exercise and activity
modification techniques. Participants in this study reported decreased pain levels, no
adverse effects, tolerated the wearing regime well and reported ease of application. A
rigorous randomised controlled trial with assessor blinding is required, with adequate
follow-up to determine longer term functional outcomes of this treatment modality.
93

94
Chapter 6 – A randomised controlled trial of comparative
effectiveness of elastic therapeutic tape, sham tape or
eccentric exercises alone for lateral elbow tendinosis
6.1 Introduction
The previous chapters have discussed the use of elastic therapeutic tape and
shown that, whilst there is a lack of evidence for its use, there is possibly some
preliminary support for its use for upper limb conditions. This chapter includes Study 4,
a randomised controlled trial, which arose based on the recommendation of Study 3
whereby more high quality evidence into elastic therapeutic tape was required. In
particular, it was also important for the role of the tape’s application (to create skin
convolutions when applied to stretched muscle) to be examined as it has been
hypothesised that this property can reduce pressure in the mechanoreceptors below
the dermis, thereby decreasing nociceptive stimuli. As mentioned throughout this
thesis, there remains conjecture in the literature regarding how and why tape may work,
but concluding that a “perceive benefit” cannot be discounted. This is an important
research question within this study because the theory that skin convolutions are the
mechanism for the tape’s effectiveness (especially in relation to upper limb conditions)
has never been tested in a high-quality randomised controlled trial.

95
Study 4 consisted of a randomised controlled trial of 40 participants with lateral
elbow tendinosis who received (i) elastic therapeutic tape, (ii) sham tape, and (iii) no
tape, over a 12-week period (four weekly and 4 fortnightly sessions) with a 6 month
follow up. All participants received eccentric exercises and advice on activity
modification techniques.
Intervention group: Participants received the application of tape based on the
recommended application techniques by Dr Kenzo Kase in ‘Clinical Therapeutic
Applications of the Kinesio Taping Method’ (refer to Appendix D). Participants were
educated on all precautions (such as how to monitor for reactions to the tape) and were
shown how to remove the tape safely.
Comparison group (Sham taping): Participants in this group were taped the same way
as the intervention group; however, the tape was applied with no tension. Participants
were not aware they were receiving sham treatment as they were instructed on how to
apply the tape without tension and were not told of the alternative method (tape
applied with stretch).
Control group: Participants in this group received no taping.
Participants in all three groups received the same structured exercise program
which was established from existing literature on the benefits of eccentric exercises for

96
lateral elbow tendinosis (refer to Appendix E). Advice on activity modification
techniques were also provided, including ergonomic modifications and how to avoid
aggravating tasks. Exercises and the application of tape (for the intervention and control
groups) were reviewed at each session to further enhance adherence to therapy. The
full article is included in this chapter and is published in ‘Hand Therapy’.
6.2 Chapter Contents
Wegener, R.L., Brown, T. & O’Brien, L. (2016). A randomized controlled trial of
comparative effectiveness of elastic therapeutic tape, sham tape or eccentric exercises
alone for lateral elbow tendinosis. Hand Therapy, 1758998316656660.
Date submitted: 27th March 2016
Date of resubmission: 2nd June 2016
Date of acceptance: 3rd June 2015
Date of publication online: 11th July 2016

97

98

99

100

101
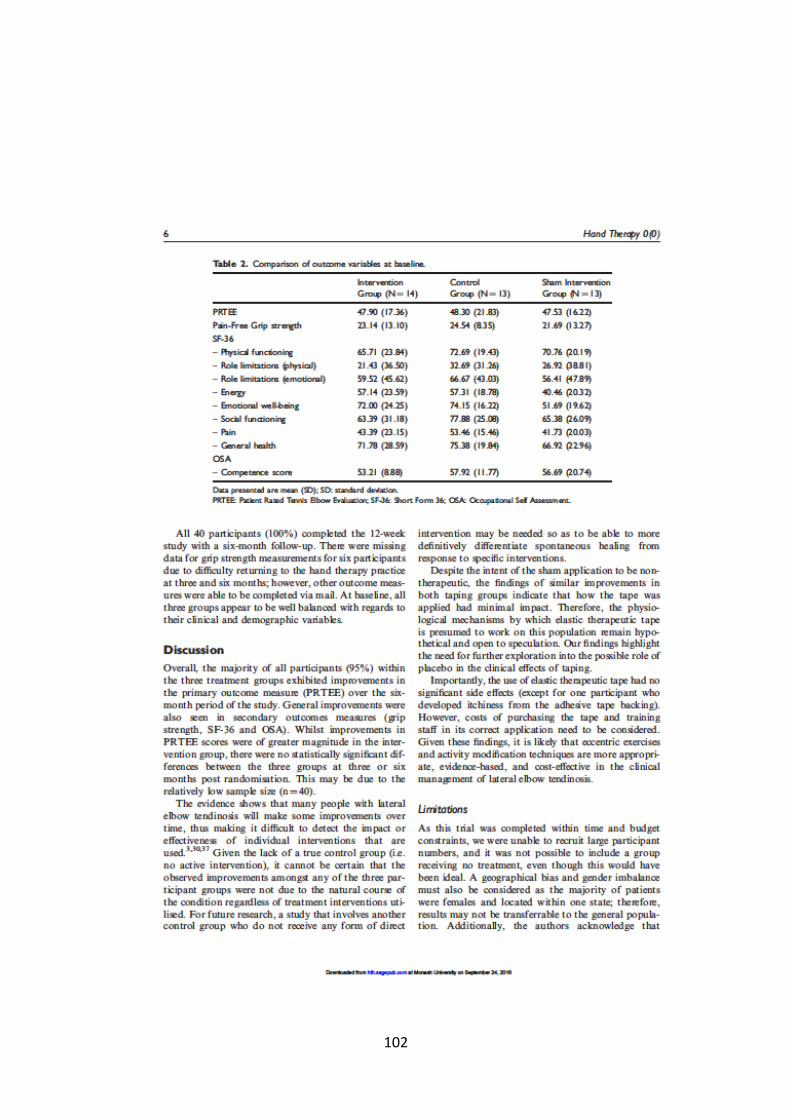
102

103

104

105

106
6.3 Impact of the Study
Journal Metrics:
Source Normalized Impact per Paper (SNIP) - 0.162
Impact per Publication (IPP) - 0.133
SCImago Journal Rank (SJR) - 0.114
The objective of this study was to provide more rigorous information for Hand
therapists when using elastic therapeutic tape for lateral elbow tendinosis. Lateral
elbow tendinosis is well known to cause difficult challenges due to its long-term recovery
and morbidity. Elastic therapeutic tape is commonly used as a treatment modality for
this condition, despite limited evidence.
At three and six-months post randomisation, improvements were made in all
three groups as assessed with the Patient-Rated Tennis Elbow Evaluation (PRTEE), the
Short Form 36 (SF-36) pain-free grip strength, and the Occupational Self-Assessment
(OSA). However, there were no statistically significant differences between groups in
any of these measures.
Whilst all groups improved on key outcomes, it is possible that exercise alone
and/or natural recovery were responsible for improvements. For future research, a
study that involves another control group who do not receive any form of direct

107
intervention may be needed so as to be able to more definitively differentiate
spontaneous healing from response to specific interventions. Despite the intent of the
sham application to be non-therapeutic, the findings of similar improvements in both
taping groups indicates that how the tape was applied had minimal impact. Therefore,
the physiological mechanisms by which elastic therapeutic tape is presumed to work on
this population remains hypothetical and open to speculation. It is positive to note that
the use of elastic therapeutic tape was well tolerated by participants and not associated
with any significant side effects or symptom exacerbation.
6.4 Chapter Summary
This study provided more clarity on the use of elastic therapeutic tape for lateral
elbow tendinosis and, whilst Study 3 showed preliminary support for its use, findings
from this RCT demonstrated that differences were not statistically significant from those
achieved by sham taping or exercises alone.
Given these findings, therapists should continue to be guided by evidence-based
practice when working with this patient population. Based on the literature, eccentric
exercises and activity modification techniques continue to be more appropriate,
evidence-based, and cost-effective in the clinical management of lateral elbow
tendinosis.

108
109
Chapter 7 - A qualitative review of patients’ experiences
using Kinesio tape for lateral epicondylitis
7.1 Introduction
This chapter comprises the final study of this PhD thesis. While many other
interventions for lateral elbow tendinosis are widely used and have been researched,
limited research has been conducted on specific patient experiences with this often
long-term condition which often leads to reduced function in daily life. This qualitative
study aimed to describe the lived experiences of 11 participants from the intervention
group of the RCT in Study 4 (three participants were lost to follow up). This included
their perspectives on the use of a passive intervention, elastic therapeutic tape, for the
treatment of lateral elbow tendinosis compared to self-management strategies alone
over a six-month period. The full article of Study 5 is included in this chapter in its revised
submitted version to the ‘British Journal of Occupational Therapy’.
7.2 Chapter Contents
Wegener, R.L., Brown, T. & O’Brien, L. (2016). A qualitative review of patients’
experiences using Kinesio tape for lateral epicondylitis. Submitted to British Journal of
Occupational Therapy and currently under second review.

110
Date submitted: 12th July 2016
Date of re-submission with revisions: 17th September 2016
Date of acceptance: To be confirmed.

111

112

113

114

115

116
117

118

119

120

121

122

123

124

125

126

127

128

129

130

131

132
7.3 Impact of the Study
Journal Metrics:
Source Normalized Impact per Paper (SNIP) - 0.6
Impact per Publication (IPP) - 0.667
SCImago Journal Rank (SJR) - 0.461
The findings of this study further support existing literature, as well as the results of
Study 4, which identified activity modification and exercises as important components
in the recovery of lateral elbow tendinosis. There is limited research into patients’
experiences with lateral elbow tendinosis and, for this reason, this study adds valuable
information for therapists. It was found that patients’ recovery from lateral epicondylitis
took longer than they expected and that it was a frustrating time involving multiple
impacts and adjustments to their usual work and daily activities. Changes in life roles
during this period led to concerns about future recovery and long-term function.
The limitations of this study that must be acknowledged are: (i) all participant groups
were not interviewed thus restricting the ability to gather broader data regarding
participant experiences of living with and managing the condition; and (ii) the interviews
could have been piloted amongst a patient population (instead of therapists alone) in
order to identify areas of greater conceptual complexity. By reflecting on the research

133
relationship (reflexivity) after this qualitative study, it must be acknowledged that there
was potential for pre-conceptions as the primary researcher knew all of the participants
prior to the interviews. For instance, my perceptions regarding how adherent patients
were with prescribed treatment may have influenced what was emphasised,
explored and, therefore, reported in the findings. My preconceptions may have also
influenced how questions were asked (e.g. such as tone of voice, sympathetic body
language and facial expressions) and subsequently what responses were given. These
two factors may have impacted on the findings of this study. If these interviews were to
be conducted again, it would be beneficial to have another therapist observe the
interviews as they are taking place, thereby providing another perspective on the
interview findings. Discussion with this colleague after the interview may have
revealed angles that I may have overlooked or dismissed without taking the time to
consider them thoroughly. It would also have encouraged critical reflection on the
interview and may have changed how subsequent interviews were
conducted. Additionally, keeping a detailed diary of my own emotions, thoughts and
impressions before and after interviews would also have been useful practice. It is
possible that other issues in my own home and work life were impacting how
interviews were conducted, and may have introduced unconscious bias.
134
Overall, it was identified that these long-term changes implemented by the person
themselves were the most important for improvements in function. By considering the
person’s perception of lateral elbow tendinosis, including their function and
occupational adaptations, therapists improve their understanding of the complexities of
this condition and consider avoiding the trial of multiple passive interventions that may
actually have little additional benefit compared to existing evidence-based
interventions.
7.4 Chapter Summary
The objective of this qualitative study was to gather interview data to identify
people’s experiences with lateral elbow tendinosis, as well as their perception on using
elastic therapeutic tape as an intervention for this complex and often chronic condition.
Emergent themes included:
1. Frustration at the length of time needed for functional recovery and the impact
on life roles.
2. The importance of long-term self-management for lateral epicondylitis.
3. Kinesio tape was an adjunct in recovery compared to self-management
strategies.

135
In particular, these themes fit within the Occupational Adaptation Model which
proposes that increased function does not automatically equate to occupational
adaptation. As is shown in this study, people with this condition will often make
physical/functional improvements over time; however, this does not necessarily result
in occupational adaptation and this should be considered by therapists.
This study concluded that, although this condition has been widely researched, many
focus on quantitative results as opposed to qualitative findings. Specific findings found
that ongoing adjustments to work and daily activities, as well as adherence to prescribed
exercises, were the largest contributor to improvements in function.
The next chapter collaborates all the findings from the previous five chapters and
discusses these in depth, based on existing research and within the context of the
conceptual frameworks and models that underpin this thesis.

136

137
Chapter 8 – Discussion and Conclusion
8.1 Chapter Overview
The purpose of this chapter is to present the overall findings from research
projects that addressed the original thesis research questions. The use of elastic
therapeutic tape as an intervention approach for lateral elbow tendinosis is discussed,
including the current body of evidence, limitations of the thesis, recommendations for
future research, and future implications for practice.
8.2 Revisiting the Research Questions
The five studies presented in this ‘Thesis by Publication’ are the first to
comprehensively investigate the effectiveness as well as clinician and patient
perceptions of elastic therapeutic tape as a treatment for lateral elbow tendinosis. A
summary of the research questions and related study findings are outlined below in
Table 2.
As discussed throughout this thesis, lateral elbow tendinosis is known to result
in considerable morbidity, long-term recovery and high financial costs (Gruchow &
Pelletier, 1979). With a prevalence in the general population of 1-5%, it is a common

138
condition treated in Hand Therapy settings and often presents challenges for achieving
successful rehabilitation (Fedorczyk, 2006b, 2012).
To date, many interventions with varying levels of effectiveness for lateral elbow
tendinosis have been researched. More recently, elastic therapeutic tape has been
increasingly used in clinical practice despite limited evidence being reported regarding
its effectiveness (Bassett, 2010; Bisset & Vicenzino, 2015; Parreira, Costa, Hespanhol
Junior, Lopes, & Costa, 2014). Currently, there is still no gold standard for tape
application and its recommended use varies between different manufacturing brands
(Parreira, Costa, Hespanhol Junior, Lopes, & Costa, 2014). Therapists are required to use
this modality based on the information and recommendations provided by
manufacturers, combined with their own clinical reasoning and previous experience.
This carries risks associated with prescribing an intervention without proven clinical
benefit, safety or cost effectiveness. For this reason, the development of this research
project and its findings aim to inform the practice of hand therapists when using this
treatment modality for lateral elbow tendinosis.

139
Table 2: Summary of research questions and study findings
Research Questions Content Findings
1. Scoping Review What is the current evidence relating the use of elastic therapeutic tape in treating neck and upper extremity conditions? Taylor, R.L., O’Brien, L. & Brown, T. (2014). A scoping review of the use of elastic therapeutic tape for neck or upper extremity conditions. Journal of Hand Therapy, 27(3), 235-246.
A scoping review was completed to review the current evidence of elastic therapeutic tape for the treatment of neck and upper extremity conditions.
Whilst elastic therapeutic tape is reported to be widely used in clinical practice, there is limited evidence into its use for neck or upper extremity disorders and future studies are warranted. Elastic therapeutic tape may play a role in reducing short-term neck and upper extremity pain and it may be a more convenient and comfortable alternative to existing conservative treatments.
2. Cross-sectional Study
What are the current perspectives amongst
hand therapists, general practitioners and hand
surgeons on the use of elastic therapeutic tape
and how often is it used or recommended?
This cross-sectional study used a self-report
survey to gather data from 157 respondents
on the use of elastic therapeutic tape in
clinical practice (Occupational Therapists and
Physiotherapists who practice as hand
therapists, general practitioners and hand
surgeons).
Therapists, general practitioners and surgeons have differing
perceptions on elastic therapeutic tape. Therapists were
more likely to recommend its use based on clinical
experience, whereas GP’s and surgeons were more sceptical
regarding its use and effectiveness due to limited evidence.

140
Taylor, R.L., Brown, T. & O’Brien, L. (2015).
Knowledge of and willingness to recommend
kinesiotape for upper limb overuse injuries: A
comparison of therapists’, general
practitioners’ and surgeons’ perspectives.
International Journal of Therapy and
Rehabilitation, 22(5), 238-245.
3. Case Series What is the preliminary evidence into the benefit of elastic therapeutic tape and eccentric exercises for the treatment of lateral elbow tendinosis? Wegener, R.L., Brown, T. & O’Brien, L. (2015). The use of elastic therapeutic tape and eccentric exercises for lateral elbow tendinosis: a case series. Hand Therapy, 20(2), 56-63.
This study was developed based on the author’s clinical observations and involved a retrospective case series of four patients with lateral elbow tendinosis who were treated with elastic therapeutic tape.
This case series demonstrated some preliminary support for the use of elastic therapeutic tape and eccentric exercises in the management of lateral elbow tendinosis. This study identified the need for a randomised control trial and qualitative study in order to rigorously examine this concept.

141
4. Randomised Controlled Trial Is the application of elastic therapeutic tape according to the ‘Clinical Therapeutic Applications of the Kinesio Taping Method’ manual (with the tape applied on tension), in conjunction with an eccentric exercise program and activity modification advice, more effective than (i) sham taping, or (ii) eccentric exercises alone in patients with lateral elbow tendinosis? Are the benefits of three months of treatment using elastic therapeutic tape sustained six-months post intervention? Wegener, R.L., Brown, T. & O’Brien, L. (2016). A randomized controlled trial of comparative effectiveness of elastic therapeutic tape, sham tape or eccentric exercises alone for lateral elbow tendinosis. Hand Therapy 1758998316656660, first published on July 11, 2016 doi:10.1177/1758998316656660.
This was a randomised controlled trial of 40 participants with lateral elbow tendinosis who received (i) elastic therapeutic tape, (ii) sham tape, and (iii) no tape, over a 12-week period with a 6 month follow up. All participants received eccentric exercises and advice on activity modification techniques.
Whilst 95% of participants improved over six months, there were no statistically significant differences between the intervention, sham, and control groups in measures of pain and function. It is important to note that there were also no significant adverse effects with this treatment modality.
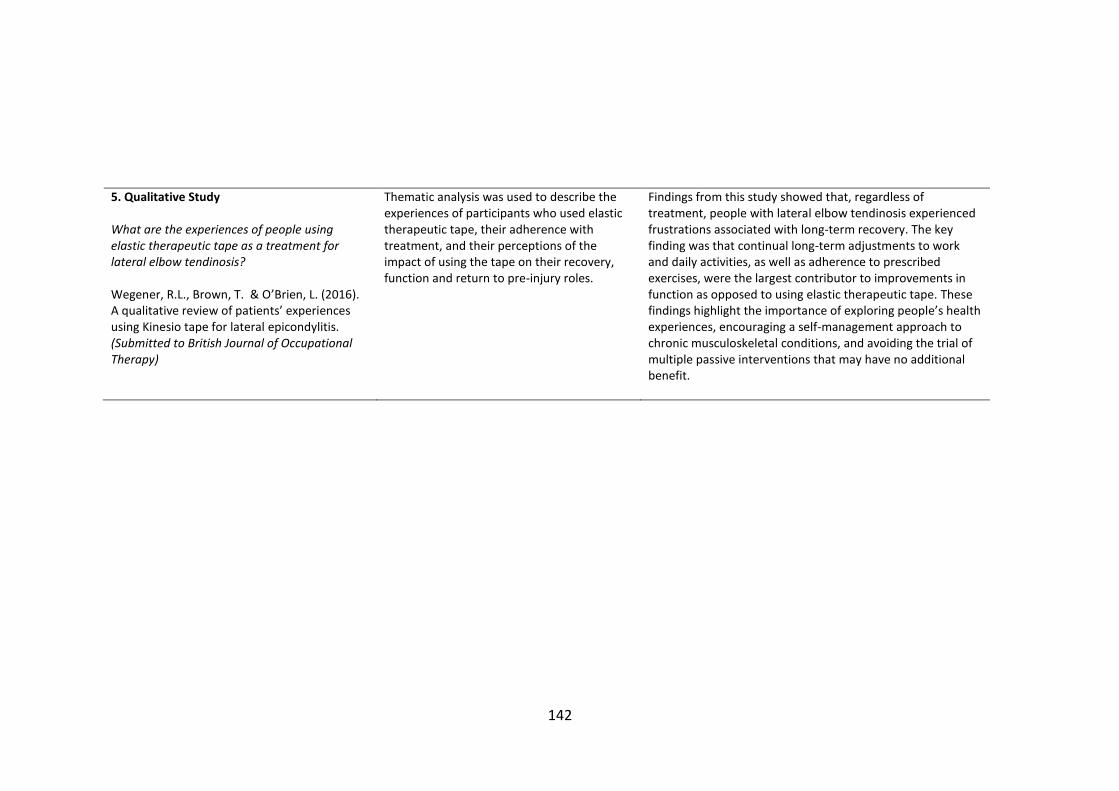
142
5. Qualitative Study What are the experiences of people using elastic therapeutic tape as a treatment for lateral elbow tendinosis? Wegener, R.L., Brown, T. & O’Brien, L. (2016). A qualitative review of patients’ experiences using Kinesio tape for lateral epicondylitis. (Submitted to British Journal of Occupational Therapy)
Thematic analysis was used to describe the experiences of participants who used elastic therapeutic tape, their adherence with treatment, and their perceptions of the impact of using the tape on their recovery, function and return to pre-injury roles.
Findings from this study showed that, regardless of treatment, people with lateral elbow tendinosis experienced frustrations associated with long-term recovery. The key finding was that continual long-term adjustments to work and daily activities, as well as adherence to prescribed exercises, were the largest contributor to improvements in function as opposed to using elastic therapeutic tape. These findings highlight the importance of exploring people’s health experiences, encouraging a self-management approach to chronic musculoskeletal conditions, and avoiding the trial of multiple passive interventions that may have no additional benefit.

143
8.3 Discussion of Study Findings
The findings of this thesis contribute to the body of evidence about the clinical use
and effectiveness of elastic therapeutic tape. New trials on the use of elastic therapeutic
tape for a variety of conditions are frequently being published (Parreira, Costa,
Hespanhol Junior, Lopes, & Costa, 2014). However, the quality of these studies
continues to vary. In particular, there are still minimal high quality studies about the use
of elastic therapeutic tape for upper limb conditions (Taylor, O'Brien, & Brown, 2014).
To date, there are six published systematic reviews that evaluate the effectiveness
of elastic therapeutic tape for different conditions. Williams et al. (2012) assessed
Kinesio Taping in the prevention and treatment of sports injuries. Bassett et al. (2010)
and Mostafavifar et al. (2012) considered Kinesio Taping in people with musculoskeletal
conditions. Morris et al. and Kalron and Bar-Sela (2013) examined musculoskeletal
conditions but extended their review to include other clinical areas, such as neurological
and lymphatic conditions. Most recently, a systematic review was completed by Parreira
et al. (2014) that assessed musculoskeletal conditions, but included more recent trials
(12 RCT’s in total).
The conclusions from these published systematic reviews are very similar. Overall,
the use of elastic therapeutic tape for musculoskeletal conditions has shown no
significant benefit, or the effects have been too small to be considered clinically

144
significant. All systematic reviews included trials comparing taping with a large range of
other modalities (including no treatment, sham taping, exercises, physiotherapy,
electrotherapy) and included outcome measures of pain, disability and quality of life.
Studies that have reported significant benefits from elastic therapeutic tape are mainly
trials conducted on healthy population groups or of low quality (and therefore high risk
of bias), and those with study designs of low methodological quality, such as case reports
(Taylor, O'Brien, & Brown, 2014).
The results from the five studies within this thesis are consistent with the current
evidence obtained from the existing systematic reviews described above. The scoping
review confirmed the lack of evidence into elastic therapeutic tape for neck and upper
limb conditions. The cross-sectional study found differing levels of knowledge of the
tape’s use amongst Surgeons, General Practitioners and Therapists; however, Therapists
were more likely to use a treatment modality without proven clinical effectiveness. The
case series demonstrated some preliminary support for elastic therapeutic tape for
lateral elbow tendinosis; however, this study had limitations and provided only weak
anecdotal level evidence, consistent with other small non-controlled studies that have
been published on elastic therapeutic tape (Mostafavifar, Wertz, & Borchers, 2012;
Parreira, Costa, Hespanhol Junior, Lopes, & Costa, 2014).

145
The subsequent randomised controlled trial of 40 participants with lateral elbow
tendinosis who received either (i) elastic therapeutic tape, (ii) sham taping, or (iii) no
taping, provided stronger findings. Whilst 95% of participants improved over six months,
there were no statistically significant differences between the three sample groups in
measures of pain and function. However, it is important to note that there were no
significant adverse effects to participants with this treatment modality either. This
particular finding supports studies in other populations that found most patients were
satisfied with the comfort and convenience of this treatment and experienced no ill
effects, despite minimal evidence of other benefits (Ristow et al., 2013; Tsai, Hung, Yang,
Huang, & Tsauo, 2009).
The fifth and final study of this thesis involved a qualitative analysis of the
experiences of 11 participants from the intervention group of the RCT (three participants
lost to follow up). Although lateral elbow tendinosis has been widely studied with a focus
on managing physical symptoms (Bassett, 2010), limited research has been conducted
on specific patient experiences with this often long-term condition. Importantly, the
findings from this study indicated that, regardless of the treatment provided, having
lateral elbow tendinosis resulted in frustrations associated with long-term recovery.
Continual long-term adjustments to work and daily activities, as well as adherence
to prescribed exercises, were reported as the largest contributor to improvements in
146
function as opposed to using elastic therapeutic tape. This is an important finding and
possibly the most relevant for therapists in clinical practice when working with this
patient population. From the available evidence, it would seem apparent that both
exercise and ergonomic adjustments are the key aspects of successful management of
lateral elbow tendinosis and a vital component of long-term self-management (Buckle
& Devereux, 2002).
This is consistent with the evidence for other conditions associated with chronic
musculoskeletal pain leading to reduced function in daily life (Lillefjell, Krokstad, &
Espnes, 2007). Individual and psychosocial factors (such as self-efficacy, adaptation,
perceived emotional and physical functioning, pain intensity and pain cognition) are
considered to be among the most important variables that influence the total health
picture (Henderson, Kidd, Pearson, & White, 2005). As therapists, it is important to
recognise that the impacts on a person’s everyday life are dependant not only on the
underlying pathophysiology, but to a larger extent on that person’s perception of the
condition in their present life situation (Henderson, Kidd, Pearson, & White, 2005;
Lillefjell, Krokstad, & Espnes, 2006).

147
8.4 Implications for Clinical Practice
A reasoned argument has been presented throughout this thesis regarding the
need for a number of adjustments in the clinical practice of health professionals who
use elastic therapeutic tape and work with people experiencing lateral elbow tendinosis.
This research enquiry has culminated in three key findings.
For lateral elbow tendinosis, there is currently limited support for long-term
effectiveness of elastic therapeutic tape as a treatment modality.
The results of the Randomised Controlled Trial (RCT) showed limited support for
using elastic therapeutic tape for lateral elbow tendinosis. This is an interesting
finding and potentially adds to existing literature showing minimal evidence for
passive interventions amongst this population. While there were no significant side
effects with the use of the tape, the costs of purchasing the tape and training staff
in its correct application need to be considered. Given these findings, it is likely that
eccentric exercises and activity modification techniques are more appropriate,
evidence-based, and cost-effective interventions in the clinical management of
lateral elbow tendinosis.
These results are further supported by recent studies that continue to
recommend that conservative management for lateral elbow tendinosis remains the

148
best practice and passive interventions should be considered carefully (Bisset &
Vicenzino, 2015).
Furthermore, this study highlights the complexity of managing this condition and
the role of other factors in the aetiology of pain for lateral elbow tendinosis, such as
changes in central pain processing (Heales, Lim, Hodges, & Vicenzino, 2014; Khan,
Cook, Kannus, Maffulli, & Bonar, 2002; Khan, Cook, Maffulli, & Kannus, 2000a).
Although this delves into issues beyond the scope of this PhD, it is important to
consider these other dimensions when managing this condition.
Overall, based on the study findings of this thesis, in combination with the
current body of evidence in the literature, it can be inferred that the ongoing
widespread clinical use of elastic therapeutic tape is due to its high-profile popularity
and associated marketing (such as its use during the Olympics), as opposed to
clinicians relying on high quality scientific evidence with clinically relevant outcomes.
This was supported by findings in Study 2 which demonstrated that therapists were
likely to continue using a treatment modality, such as elastic therapeutic tape, based
on clinical experiences despite a lack of supporting evidence. Therefore, a future
recommendation is that health professionals should carefully evaluate evidence
regarding the tape’s effectiveness when using this intervention. This disparity

149
between emerging evidence and therapists changing their clinical practice is an
important area in need of further examination.
Due to the complexity and chronic nature of lateral elbow tendinosis, it is important
to recognise clients’ health experiences and the need for long-term occupational
adjustments.
Qualitative findings from this thesis demonstrated that the nature of lateral
elbow tendinosis’ slow recovery results in considerable patient frustration. This is an
area that has not been comprehensively examined amongst this patient population
given that research to date has focused on managing physical symptoms within a
biomechanical model (e.g. using interventions, such as elastic therapeutic tape)
(Marcum, 2004). Whilst these factors are still important, it is vital for all health
professionals to work towards optimising health, well-being and participation, as
opposed to only focusing on physical dysfunction. For this reason, the use of the
International Classification of Functioning, Disability and Health (ICF) framework in
this study complements the Biomechanical Model and acknowledges the multiple
components required for successful rehabilitation (WHO, 2001).
Functioning is central to the patient experience in musculoskeletal conditions.
The WHO identifies four health outcomes within this framework, including

150
impairments (body structure and function), activity limitations, restrictions in social
participation and environmental factors (Steiner et al., 2002; WHO, 2001). Being able
to assess the effectiveness of an intervention within each of these domains provides
a means to more accurately assess its benefit and impact. For example, in the case
of lateral elbow tendinosis, an MRI may show improvements in tendon recovery
(impairment); however, the patient may not have regained full function at work
(activity limitation) and remain unable to engage with family and friends (social
participation and environment). Measurements of “outcome” for this patient would
be falsely positive if only the impairment was considered. Due to the often long-term
nature of lateral elbow tendinosis, this is a common situation for this patient
population.
The use of the Short-Form 36 (SF-36) and the Occupational Self-Assessment
(OSA) were chosen as outcome measures within this thesis as they were able to
closely evaluate aspects of these domains within the ICF. Whilst there has been
literature on linking health-status measures to the ICF (including the SF-36) (Brockow
et al., 2004), this is an area that will continue to be developed in the future (Cieza et
al., 2002a; Velstra, Ballert, & Cieza, 2011).
Through the perspective of the Occupational Adaptation Model, Schkade and
Schultz (1992) outlined that increased function does not automatically equate to
151
occupational adaptation. This is a common mistake when working with patients with
conditions such as lateral elbow tendinosis. As previously mentioned, people with
this condition will often make functional improvements over time (e.g. less pain,
improved movement/strength and increased use in everyday activities) however,
this does not necessarily result in adaptation (Lillefjell, Krokstad, & Espnes, 2006,
2007). Therapists should consider these factors early in treatment and recognise
their role in facilitating the internal adaptation process to maintain or re-engage in
meaningful occupations. By incorporating evidence-based practice, there are actions
that can be undertaken in the clinical setting, such as provision of earlier and more
specific education on long-term occupational adjustments and the implementation
of strategies/treatment plans that are occupation-focused (Cullinane, Boocock, &
Trevelyan, 2014; Rothmore et al., 2016).
Changes in terminology from ‘lateral epicondylitis’ to ‘lateral elbow tendinosis’ or
‘lateral elbow tendinopathy’ should be implemented in clinical practice to better
guide treatment.
Extensive current research reveals that commonly used terms such as ‘lateral
epicondylitis’ and ‘tennis elbow’ are misleading as they imply an inflammatory
pathology as opposed to degeneration of the common extensor origin (Bunata,

152
Brown, & Capelo, 2007; Nirschl & Pettrone, 1979). It is important for health
professionals to apply the correct diagnostic terminology to avoid misunderstanding
and inappropriate treatment. More appropriate terms for this condition are either
(i) lateral elbow tendinosis, or (ii) lateral elbow tendinopathy, and there should be a
shift towards using these terms in clinical practice (Ali & Lehman, 2009).
8.5 Limitations of this thesis
There are several limitations that have been identified throughout this thesis and
have been documented in more detail in the five individual studies within Chapters 3 to
7.
Overall, a summary of the main limitations includes –
Due to the limited number of randomised controlled trials into the use of
elastic therapeutic tape for neck and upper extremity disorders, a
systematic review was unable to be completed for this thesis. In order to
synthesise all available evidence into this modality, a scoping review was
completed instead.
The cross-sectional study included a small sample size that was unevenly
distributed by profession and location. Therefore, the findings may not

153
accurately represent the views of all health professionals across
Australia.
In the case series study, the lack of control group, un-blinding of patients
and therapist, as well as a lack of pre-therapy measurements, may have
led to bias in the results observed.
The cost-effectiveness of elastic therapeutic tape compared to other
existing interventions for lateral elbow tendinosis was not
comprehensively examined.
Large participant numbers were unable to be recruited in the RCT and it
was ethically not possible to include a group receiving no treatment.
There was no formal funding provided for this study thus limiting the
recruitment strategies used. We did, however, reach our a-priori
recruitment targets for 80% power to detect a clinically meaningful
difference between groups.
A geographical bias and gender imbalance must also be considered
limitations for this trial, as the majority of patients were females located
within one state; therefore, results may not be generalisable to the
broader population.

154
As it was difficult to have blinding of the assessor and therapists, this may
have increased the possibility of bias.
Another limitation of the RCT may be that the outcome measures used
(PRTEE, SF-36, OSA and grip strength) may not have been sensitive
enough to detect clinical change at three and six month follow up.
More rigorous supervision of each participant’s home exercise program
may have also been beneficial. Non-adherence to the specified treatment
regimen, incorrect exercise techniques or inconsistencies with
application of the tape may have not been reported and would most
likely have impacted on results.
8.6 Recommendations for future research
There is potential for future research into the role of elastic therapeutic tape for
a variety of other musculoskeletal conditions. Further rigorous trials into the use of
elastic therapeutic tape as an intervention strategy are needed, especially in relation to
its role for acute upper limb conditions. It is possible that the proposed mechanisms of
elastic therapeutic tape (such as reducing pressure on mechanoreceptors below the
dermis, improving circulation, decreasing oedema and correcting muscle function) may
be more aligned to the treatment of acute conditions, as opposed to chronic conditions

155
(such as lateral elbow tendinosis) that are not inflammatory in nature. This would
provide research opportunities that build on the findings of the five studies reported in
this thesis.
8.7 Chapter Summary
Elastic therapeutic tape is widely used for upper limb and neck conditions in
clinical practice despite poor evidence of its effectiveness. In particular, this thesis found
that there was limited support for its use for lateral elbow tendinosis; however, it may
be an acceptable adjunct treatment to eccentric exercise and activity modification and
is associated with minimal side effects. It must be noted that the author acknowledges
limitations with this RCT (as mentioned above) and that conclusions are based on
findings in combination with previous underpowered or low-quality published studies.
Overall, this chapter has summarised the results and limitations of the
publications that form this thesis. Implications for clinical practice and future research
have been discussed, with the findings of the five research studies indicating that certain
changes in health practice amongst this patient population are warranted and should be
considered.

156
References
Ali, M., & Lehman, T. A. (2009). Lateral Elbow Tendinopathy: A Better Term Than Lateral Epicondylitis or Tennis Elbow. The Journal of hand surgery, 34(8), 1575.
Amro, A., Diener, I., Bdair, W. O., Isra’M, H., Shalabi, A. I., & Dua’I, I. (2010). The effects of Mulligan mobilisation with movement and taping techniques on pain, grip strength, and function in patients with lateral epicondylitis. Hong Kong Physiotherapy Journal, 28(1), 19-23.
Ashe, M. C., McCauley, T., & Khan, K. M. (2004). Tendinopathies in the upper extremity: A paradigm shift. Journal of Hand Therapy, 17(3), 329-334.
Bassett, K., Lingman, S., Ellis, R. (2010). The use and treatment efficacy of kinaesthetic taping for musculoskeletal conditions: a systematic review. NZ Journal of Physiotherapy, 38(2), 56.
Bisset, L. M., & Vicenzino, B. (2015). Physiotherapy management of lateral epicondylalgia. Journal of physiotherapy, 61(4), 174-181.
Brockow, T., Cieza, A., Kuhlow, H., Sigl, T., Franke, T., Harder, M., et al. (2004). Identifying the concepts contained in outcome measures of clinical trials on musculoskeletal disorders and chronic widespread pain using the International Classification of Functioning, Disability and Health as a reference. Journal of Rehabilitation Medicine, 36(0), 30-36.
Brown, T. M. (1981). The mechanical philosophy and the "animal oeconomy". New York: Arno Press.
Buchbinder, R., Green, S., Bell, S., Barnsley, L., Smidt, N., Assendelft, W., et al. (2002). Surgery for lateral elbow pain. Cochrane Database Syst Rev, 1.
Buchbinder, R., Green, S., White, M., Barnsley, L., Smidt, N., & Assendelft, W. (2002). Shock wave therapy for lateral elbow pain. The Cochrane Library.
Buckle, P. W., & Devereux, J. (2002). The nature of work-related neck and upper limb musculoskeletal disorders. Applied Ergonomics, 33(3), 207-217.
Bunata, R. E., Brown, D. S., & Capelo, R. (2007). Anatomic factors related to the cause of tennis elbow. The Journal of Bone & Joint Surgery, 89(9), 1955-1963.
Burton, A. K., Kendall, N. A., Pearce, B. G., Birrell, L. N., & Bainbridge, L. C. (2009). Management of work-relevant upper limb disorders: a review. Occupational medicine, 59(1), 44-52.
Carlo, M. (2009). 0223: Tendinopathies of the Wrist and Hand. Ultrasound in medicine & biology, 35(8, Supplement 1).
Chourasia, A. O., Buhr, K. A., Rabago, D. P., Kijowski, R., Irwin, C. B., & Sesto, M. E. (2012). Effect of Lateral Epicondylosis on Grip Force Development. Journal of Hand Therapy, 25(1), 27-37.
Cieza, A., Brockow, T., Ewert, T., Amman, E., Kollerits, B., Chatterji, S., et al. (2002a). Linking health-status measurements to the international classification of functioning, disability and health. Journal of Rehabilitation Medicine, 34(5), 205-210.

157
Cieza, A., Brockow, T., Ewert, T., Amman, E., Kollerits, B., Chatterji, S., et al. (2002b). Linking health-status measurements to the international classification of functioning, disability and health. Journal of Rehabilitation Medicine, 34(5), 205-210.
Clarke, A. W., Ahmad, M., Curtis, M., & Connell, D. A. (2013). Lateral elbow tendinopathy: correlation of ultrasound findings with pain and functional disability. American Journal of Sports Medicine, 38(6), 1209-1214.
Cole, M. B., & Tufano, R. (2008). Applied theories in occupational therapy: A practical approach: Slack Thorofare, NJ.
Cook, J., & Purdam, C. (2009a). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British journal of sports medicine, 43(6), 409-416.
Cook, J., & Purdam, C. (2013). The challenge of managing tendinopathy in competing athletes. British journal of sports medicine, bjsports-2012-092078.
Cook, J. L., & Purdam, C. R. (2009b). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6), 409-416. doi:10.1136/bjsm.2008.051193
Cullinane, F. L., Boocock, M. G., & Trevelyan, F. C. (2014). Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clinical rehabilitation, 28(1), 3-19.
Fedorczyk, J. M. (2006a). Tennis elbow: blending basic science with clinical practice. J Hand Ther, 19(2), 146-153. doi:10.1197/j.jht.2006.02.016
Fedorczyk, J. M. (2006b). Tennis Elbow: Blending Basic Science with Clinical Practice. Journal of Hand Therapy, 19(2), 146-153.
Fedorczyk, J. M. (2012). Tendinopathies of the Elbow, Wrist, and Hand: Histopathology and Clinical Considerations. Journal of Hand Therapy, 25(2), 191-201.
Geoffroy, P., Yaffe, M. J., & Rohan, I. (1994). Diagnosing and treating lateral epicondylitis. Canadian Family Physician, 40, 73.
Green, S., Buchbinder, R., Barnsley, L., Hall, S., White, M., Smidt, N., et al. (2002). Acupuncture for lateral elbow pain. Cochrane Database Syst Rev, 1.
Green, S., Buchbinder, R., Barnsley, L., Hall, S., White, M., Smidt, N., et al. (2001). Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst Rev, 4.
Gruchow, H. W., & Pelletier, D. (1979). An epidemiologic study of tennis elbow. Incidence, recurrence, and effectiveness of prevention strategies. The American journal of sports medicine, 7(4), 234-238.
Hausman, M. R., & Lang, P. (2014). Examination of the Elbow: Current Concepts. The Journal of hand surgery, 39(12), 2534-2541.
Heales, L., Lim, E., Hodges, P., & Vicenzino, B. (2014). Sensory and motor deficits exist on the non-injured side of patients with unilateral tendon pain and disability—implications for central nervous system involvement: a systematic review with meta-analysis. British journal of sports medicine, 48(19), 1400-1406.

158
Henderson, M., Kidd, B. L., Pearson, R. M., & White, P. D. (2005). Chronic upper limb pain: an exploration of the biopsychosocial model. Journal of Rheumatology, 32(1), 118-122.
Ikiugu, M. N., Smallfield, S., & Condit, C. (2009). A framework for combining theoretical conceptual practice models in occupational therapy practice. Canadian Journal of Occupational Therapy - Revue Canadienne d Ergotherapie, 76(3), 162-170.
Jackson, J. P., & Schkade, J. K. (2001a). Occupational Adaptation Model Versus Biomechanical-Rehabilitation Model in the Treatment of Patients With Hip Fractures. American Journal of Occupational Therapy September/October, 55(5), 531-537.
Jackson, J. P., & Schkade, J. K. (2001b). Occupational Adaptation Model Versus Biomechanical–Rehabilitation Model in the Treatment of Patients With Hip Fractures. American Journal of Occupational Therapy, 55(5), 531-537. doi:10.5014/ajot.55.5.531
Kase, K. (2003). Clinical therapeutic applications of the Kinesio taping method. USA: Kinesio Taping Association.
Kase, K., Tatsuyuki, H., & Tomoko, O. (1996). Development of Kinesio tape (Vol. 6). USA: Kinesio Taping Association.
Khan, K., Cook, J., Bonar, F., Harcourt, P., & Åstrom, M. (1999). Histopathology of common tendinopathies. Sports medicine, 27(6), 393-408.
Khan, K., Cook, J., Kannus, P., Maffulli, N., & Bonar, S. (2002). Time to abandon the “tendinitis” myth: Painful, overuse tendon conditions have a non-inflammatory pathology. BMJ: British Medical Journal, 324(7338), 626.
Khan, K., Cook, J., Maffulli, N., & Kannus, P. (2000a). Where is the pain coming from in tendinopathy? It may be biochemical, not only structural, in origin. British journal of sports medicine, 34(2), 81-83.
Khan, K. M., Cook, J. L., Maffulli, N., & Kannus, P. (2000b). Where is the pain coming from in tendinopathy? It may be biochemical, not only structural, in origin. British Journal of Sports Medicine, 34(2), 81-83. doi:10.1136/bjsm.34.2.81
Kielhofner, G. (2009). Conceptual foundations of occupational therapy practice: FA Davis. Labelle, H., Guibert, R., Joncas, J., Newman, N., Fallaha, M., & Rivard, C. (1992). Lack of scientific
evidence for the treatment of lateral epicondylitis of the elbow. J Bone Joint Surg Br, 74(5), 646-651.
Lillefjell, M., Krokstad, S., & Espnes, G. A. (2006). Factors predicting work ability following multidisciplinary rehabilitation for chronic musculoskeletal pain. Journal of Occupational Rehabilitation, 16. doi:10.1007/s10926-005-9011-2
Lillefjell, M., Krokstad, S., & Espnes, G. A. (2007). Prediction of function in daily life following multidisciplinary rehabilitation for individuals with chronic musculoskeletal pain; a prospective study. BMC Musculoskeletal Disorders, 8(1), 1-10. doi:10.1186/1471-2474-8-65
Ljung, B. O., Lieber, R. L., & Friden, J. (1999). Wrist extensor muscle pathology in lateral epicondylitis. J Hand Surg Br, 24(2), 177-183. doi:10.1054/jhsb.1998.0178
159
MacDermid, J. C., & Michlovitz, S. L. (2006). Examination of the Elbow: Linking Diagnosis, Prognosis, and Outcomes as a Framework for Maximizing Therapy Interventions. Journal of Hand Therapy, 19(2), 82-97.
Malliaras, P., Maffulli, N., & Garau, G. (2008). Eccentric training programmes in the management of lateral elbow tendinopathy. Disability & Rehabilitation, 30(20-22), 1590-1596.
Marcum, J. A. (2004). Biomechanical and phenomenological models of the body, the meaning of illness and quality of care. Med Health Care Philos, 7(3), 311-320.
Miller, T. T., Shapiro, M. A., Schultz, E., & Kalish, P. E. (2002). Comparison of sonography and MRI for diagnosing epicondylitis. Journal of clinical ultrasound, 30(4), 193-202.
Mishler, E. G. (1981). Viewpoint: Critical perspectives on the biomedical model. Social contexts of health, illness, and patient care, 1-23.
Moore, R. (2012). What is the current evidence for the use of kinesio tape? A literature review. SportEX Dynam, 34(1), 24-30.
Mostafavifar, M., Wertz, J., & Borchers, J. (2012). A systematic review of the effectiveness of kinesio taping for musculoskeletal injury. The Physician and sportsmedicine, 40(4), 33-40.
Nirschl, R., & Pettrone, F. (1979). Tennis elbow. The surgical treatment of lateral epicondylitis. The Journal of Bone & Joint Surgery, 61(6), 832-839.
Parreira, P. d. C. S., Costa, L. d. C. M., Hespanhol Junior, L. C., Lopes, A. D., & Costa, L. O. P. (2014). Current evidence does not support the use of Kinesio Taping in clinical practice: a systematic review. Journal of physiotherapy, 60(1), 31-39.
Parreira, P. d. C. S., Costa, L. d. C. M., Takahashi, R., Junior, L. C. H., da Luz Junior, M. A., da Silva, T. M., et al. (2014). Kinesio Taping to generate skin convolutions is not better than sham taping for people with chronic non-specific low back pain: a randomised trial. Journal of physiotherapy, 60(2), 90-96.
Peachey-Hill, C., & Law, M. (2000). Impact of environmental sensitivity on occupational performance. Canadian Journal of Occupational Therapy - Revue Canadienne d Ergotherapie, 67(5), 304-313.
Raman, J., MacDermid, J. C., & Grewal, R. (2012). Effectiveness of Different Methods of Resistance Exercises in Lateral Epicondylosis—A Systematic Review. Journal of Hand Therapy, 25(1), 5-26.
Reichel, L. M., & Morales, O. A. (2013). Gross Anatomy of the Elbow Capsule: A Cadaveric Study. The Journal of hand surgery, 38(1), 110-116.
Ristow, O., Hohlweg-Majert, B., Kehl, V., Koerdt, S., Hahnefeld, L., & Pautke, C. (2013). Does elastic therapeutic tape reduce postoperative swelling, pain, and trismus after open reduction and internal fixation of mandibular fractures? Journal of Oral and Maxillofacial Surgery, 71(8), 1387-1396.
Rothmore, P., Aylward, P., Oakman, J., Tappin, D., Gray, J., & Karnon, J. (2016). The stage of change approach for implementing ergonomics advice – Translating research into practice. Applied Ergonomics, 59, Part A, 225-233.

160
Schkade, J. K., & Schultz, S. (1992). Occupational adaptation: Toward a holistic approach for contemporary practice, part 1. American Journal of Occupational Therapy, 46(9), 829-837.
Schultz, S., & Schkade, J. K. (1992). Occupational adaptation: Toward a holistic approach for contemporary practice, part 2. American Journal of Occupational Therapy, 46(10), 917-925.
Seidel, A. C. (1998). Theories derived from rehabilitation perspectives. . Philadelphia: Lippincott. Shiri, R., Viikari-Juntura, E., Varonen, H., & Heliövaara, M. (2006). Prevalence and determinants
of lateral and medial epicondylitis: a population study. American journal of epidemiology, 164(11), 1065-1074.
Silverstein, B., Viikari‐Juntura, E., & Kalat, J. (2002). Use of a prevention index to identify industries at high risk for work‐related musculoskeletal disorders of the neck, back, and upper extremity in Washington state, 1990–1998. American journal of industrial medicine, 41(3), 149-169.
Smidt, N., Assendelft, W. J., van der Windt, D. A., Hay, E. M., Buchbinder, R., & Bouter, L. M. (2002). Corticosteroid injections for lateral epicondylitis: a systematic review. Pain, 96(1), 23-40.
SPSS, I. (2011). IBM SPSS statistics base 20. Chicago, IL: SPSS Inc. Stasinopoulos, D., & Johnson, M. I. (2006). ‘Lateral elbow tendinopathy’is the most appropriate
diagnostic term for the condition commonly referred-to as lateral epicondylitis. Medical hypotheses, 67(6), 1400-1402.
Steiner, W. A., Ryser, L., Huber, E., Uebelhart, D., Aeschlimann, A., & Stucki, G. (2002). Use of the ICF model as a clinical problem-solving tool in physical therapy and rehabilitation medicine. Physical Therapy, 82(11), 1098-1107.
Struijs, P., Smidt, N., Arola, H., Van Dijk, C., Buchbinder, R., & Assendelft, W. (2001). Orthotic devices for tennis elbow: a systematic review. Br J Gen Pract, 51(472), 924-929.
Taylor, R. L., O'Brien, L., & Brown, T. (2014). A scoping review of the use of elastic therapeutic tape for neck or upper extremity conditions. Journal of Hand Therapy, 27(3), 235-246.
Tsai, H.-J., Hung, H.-C., Yang, J.-L., Huang, C.-S., & Tsauo, J.-Y. (2009). Could Kinesio tape replace the bandage in decongestive lymphatic therapy for breast-cancer-related lymphedema? A pilot study. Supportive Care in Cancer, 17(11), 1353-1360.
Valdes, K., & LaStayo, P. (2013). The value of provocative tests for the wrist and elbow: a literature review. Journal of Hand Therapy, 26(1), 32-43.
Velstra, I.-M., Ballert, C. S., & Cieza, A. (2011). A systematic literature review of outcome measures for upper extremity function using the international classification of functioning, disability, and health as reference. PM&R, 3(9), 846-860.
Vicenzino, B. (2003). Lateral epicondylalgia: a musculoskeletal physiotherapy perspective. Manual therapy, 8(2), 66-79.
Vicenzino, B., Brooksbank, J., Minto, J., Offord, S., & Paungmali, A. (2003). Initial effects of elbow taping on pain-free grip strength and pressure pain threshold. journal of orthopaedic & sports physical therapy, 33(7), 400-407.

161
Vicenzino, B., & Wright, A. (1996). Lateral epicondylalgia I: epidemiology, pathophysiology, aetiology and natural history. Physical Therapy Reviews, 1(1), 23-34.
WHO. (2001). International classification of functioning, disability and health: ICF: World Health Organization.
Wilhelm, A. (2009). Lateral Epicondylitis Review and Current Concepts. The Journal of hand surgery, 34(7), 1358-1359.

162
Appendix

163
Appendix A: Published opinion piece
R.L., Brown, T. & O’Brien, L. (2015). Using and prescribing kinesiotape as a treatment
modality for musculoskeletal disorders. International Journal of Therapy and
Rehabilitation, 22(9), 408-409.

164

165

166
Appendix B: Ethics approval and Final Report

167

168

169
Appendix C: Conference Participation
Current Abstract Submissions
Wegener, R.L., Brown, T. & O’Brien, L. (2017). The use of Kinesio tape for tennis elbow:
results of quantitative and qualitative studies”. Submitted for oral and poster
presentations at the Occupational Therapy Australia Association Conference, July 2017;
Perth, Australia.
Conference Presentations
Wegener, R.L., Brown, T. & O’Brien, L. (2016). Comparative effectiveness of Kinesio tape,
sham taping or eccentric exercises for tennis elbow. Oral and poster presentations at
the ACT Australian Physiotherapy Association Research Symposium, September 2016;
Canberra, Australia.
Wegener, R.L. (2016). Comparative effectiveness of Kinesio tape, sham taping or
eccentric exercises for tennis elbow. Poster presentation at CHARM (Canberra Hospital
Annual Research Meeting), August 2016; Canberra, Australia.

170
Wegener, R.L., Brown, T. & O’Brien, L. (2016). Comparative effectiveness of Kinesio tape,
sham taping or eccentric exercises for tennis elbow. Oral presentation at the Australian
Hand Therapy Association Conference, August 2016; Sydney, Australia.
Wegener, R.L., Brown, T. & O’Brien, L. (2014). Kinesiotape for lateral elbow tendinosis.
Oral presentation at the Australian Hand Therapy Association Conference, August 2014;
Gold Coast, Australia. Awarded Best Poster Award.
Other Presentations
Wegener, R.L. (2016). Kinesiotape for the upper limb. Oral presentation at the ACT Hand
Therapy Special Interest Group, November 2015; Canberra, Australia.
Wegener, R.L. (2016). The use of elastic therapeutic tape for lateral elbow tendinosis.
Oral presentation at the Victorian Hand Therapy Special Interest Group, June 2015;
Melbourne, Australia.
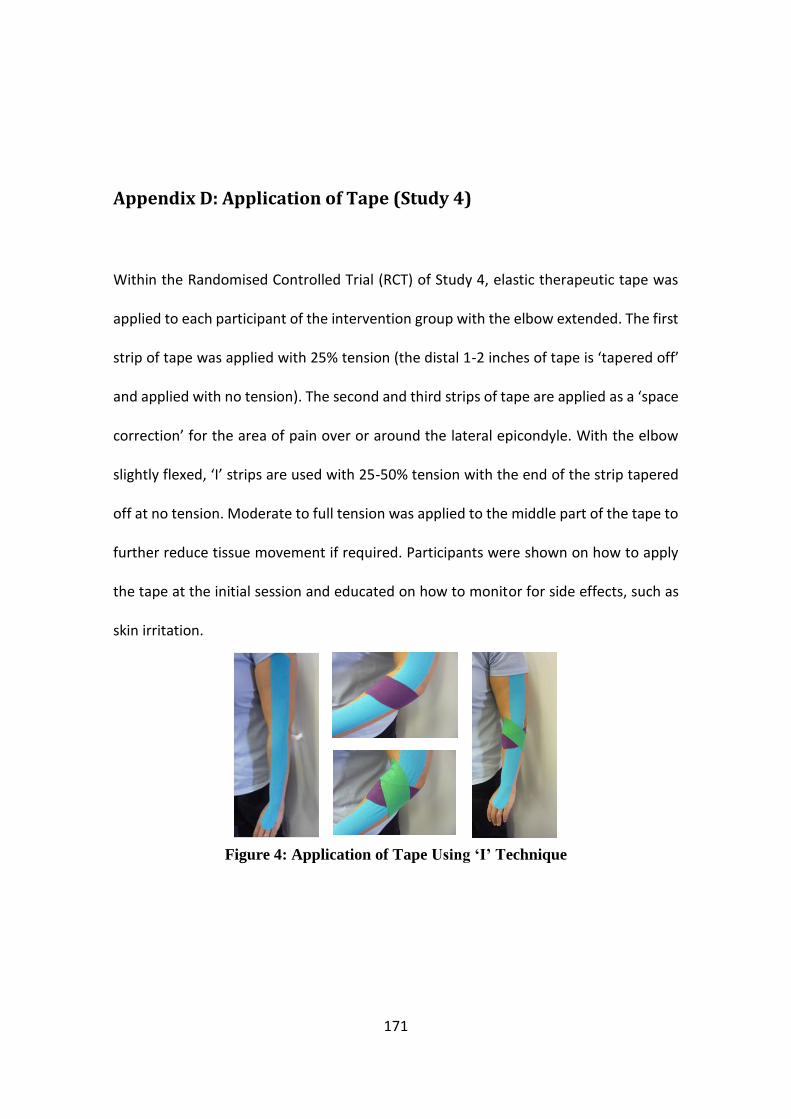
171
Appendix D: Application of Tape (Study 4)
Within the Randomised Controlled Trial (RCT) of Study 4, elastic therapeutic tape was
applied to each participant of the intervention group with the elbow extended. The first
strip of tape was applied with 25% tension (the distal 1-2 inches of tape is ‘tapered off’
and applied with no tension). The second and third strips of tape are applied as a ‘space
correction’ for the area of pain over or around the lateral epicondyle. With the elbow
slightly flexed, ‘I’ strips are used with 25-50% tension with the end of the strip tapered
off at no tension. Moderate to full tension was applied to the middle part of the tape to
further reduce tissue movement if required. Participants were shown on how to apply
the tape at the initial session and educated on how to monitor for side effects, such as
skin irritation.
Figure 4: Application of Tape Using ‘I’ Technique

172
Participants in the ‘sham application’ group were taped the same way as the
intervention group; however, the tape was applied with no tension. As per the
intervention group, participants were shown how to apply the tape, monitor for side
effects, and wearing regime was identical.
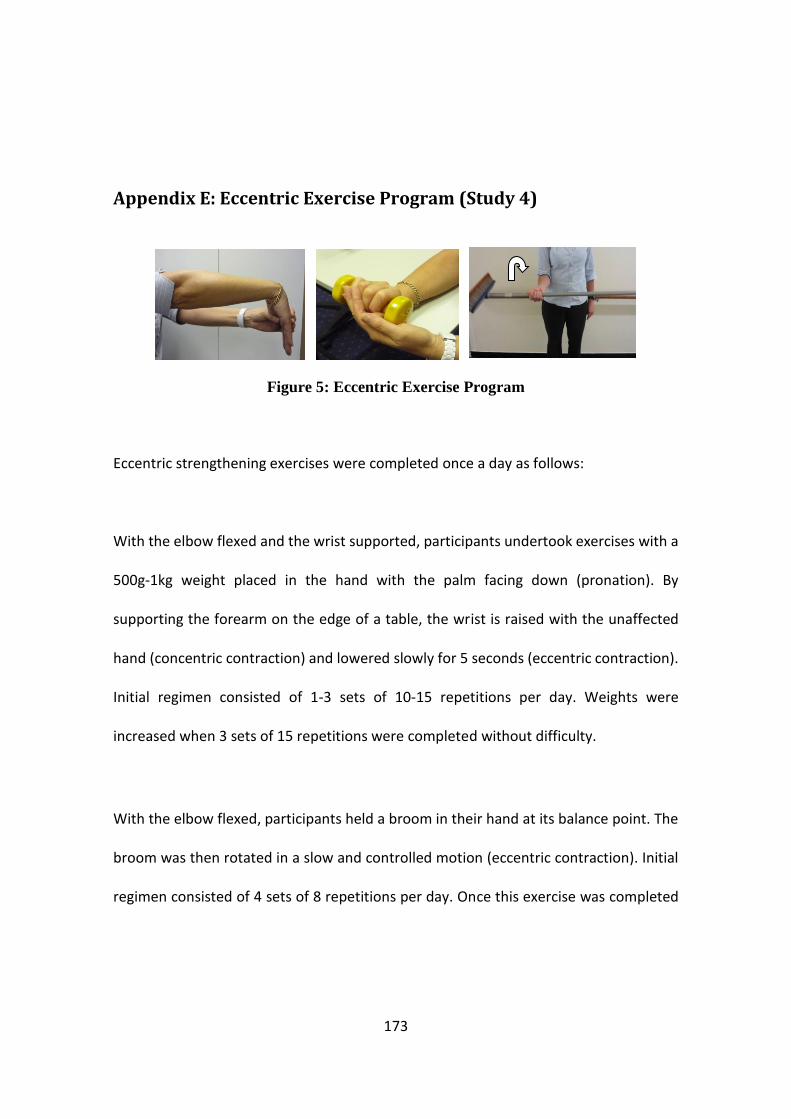
173
Appendix E: Eccentric Exercise Program (Study 4)
Figure 5: Eccentric Exercise Program
Eccentric strengthening exercises were completed once a day as follows:
With the elbow flexed and the wrist supported, participants undertook exercises with a
500g-1kg weight placed in the hand with the palm facing down (pronation). By
supporting the forearm on the edge of a table, the wrist is raised with the unaffected
hand (concentric contraction) and lowered slowly for 5 seconds (eccentric contraction).
Initial regimen consisted of 1-3 sets of 10-15 repetitions per day. Weights were
increased when 3 sets of 15 repetitions were completed without difficulty.
With the elbow flexed, participants held a broom in their hand at its balance point. The
broom was then rotated in a slow and controlled motion (eccentric contraction). Initial
regimen consisted of 4 sets of 8 repetitions per day. Once this exercise was completed

174
with minimal pain, the participant could move their hand 1cm along the handle (away
from the broom head) progressively each day.

175
Appendix F: Outcome Measures (Study 4)

176

177

178
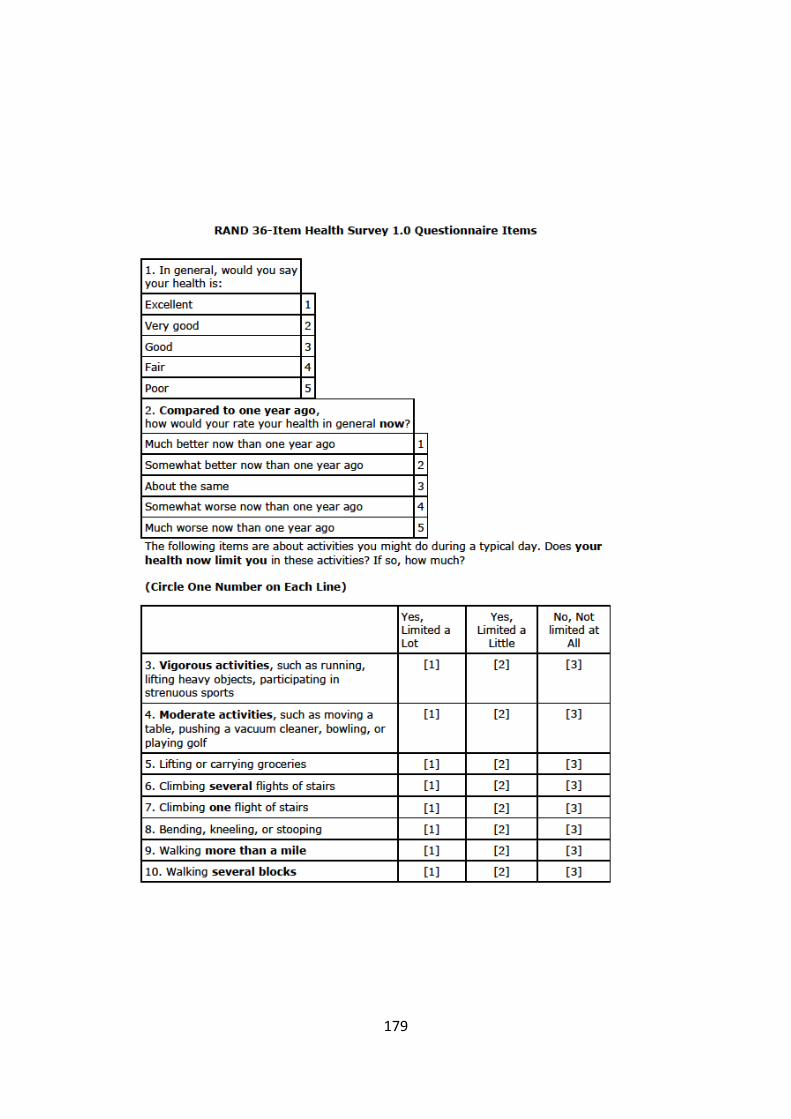
179
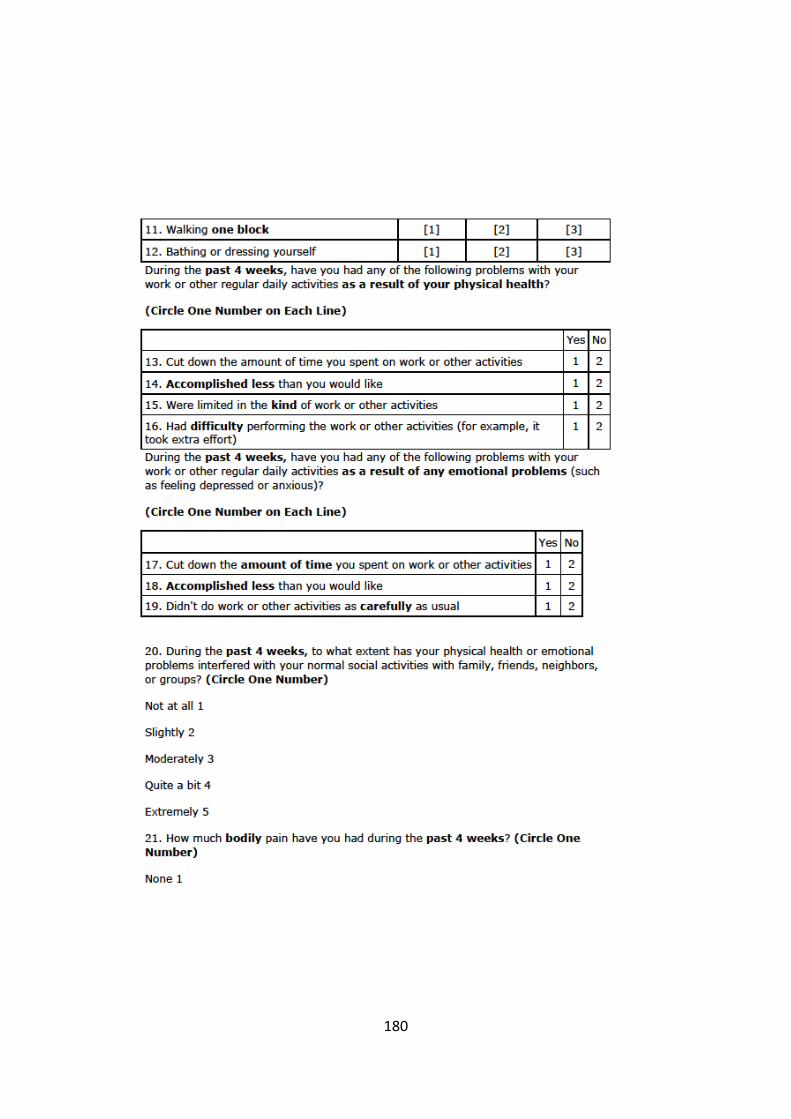
180

181

182

183

184
Appendix G: Qualitative Questions (Study 5)
1. Looking back over the past 6 months, what do you think about your arm function
now?
2. For you, what did you like or not like about your experience with using the tape?
a. Were you able to apply it yourself?
b. Were there any side-effects/complications?
3. What did you think of the tape compared to other treatments you may have used in
the past?
4. Looking back over the past 6 months, how did you manage with your work duties?
a. What did you think about using the tape for work?
b. Did the tape affect the way you performed your work?
c. Did the tape change your pain/symptoms? How?
5. Looking back over the past 6 months, how did you manage with your everyday
activities?
a. Such as self-care, domestic tasks, community access, leisure/recreation
and relationships with friends/family?
b. Do you think the tape changed your pain/symptoms? How?







