
The use of CRP in Neonatal Early
Onset Sepsis: Experience of a Tertiary
Neonatal Unit in the UK
N Ganjoo, S Ali, M Ayeni
Introduction of NICE guidance (2012)
Neonatal infection (early onset): antibiotics for
prevention and treatment
• 1 Amber flag - observations
• 1 Red flag or 2 Amber flags – perform blood
culture and CRP and start antibiotics
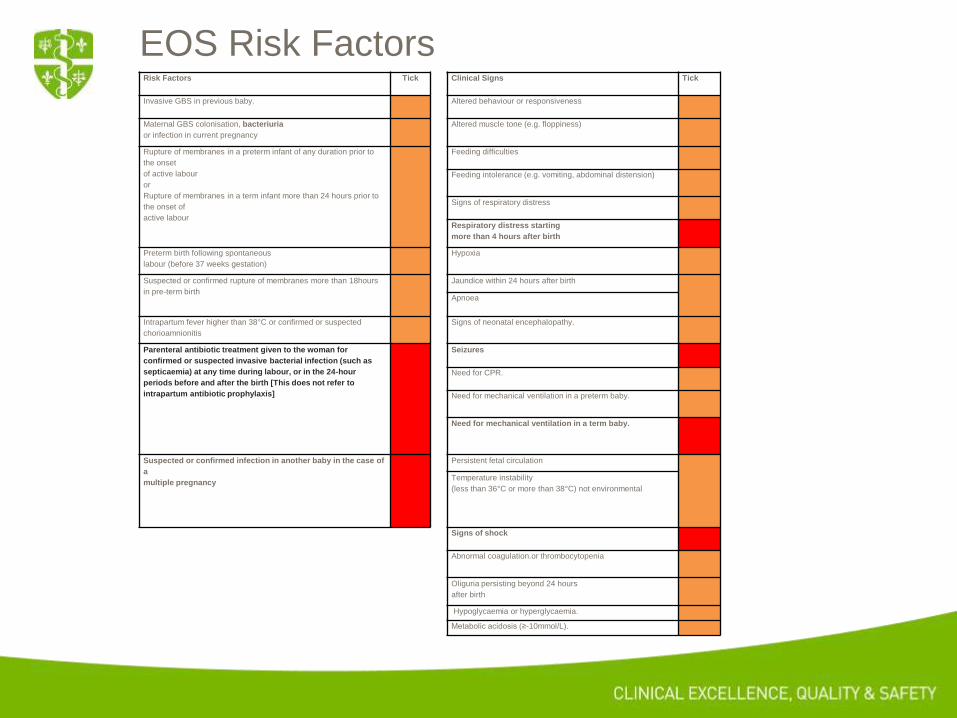
EOS Risk Factors Risk Factors Tick Clinical Signs Tick
Invasive GBS in previous baby. Altered behaviour or responsiveness
Maternal GBS colonisation, bacteriuria
or infection in current pregnancy
Altered muscle tone (e.g. floppiness)
Rupture of membranes in a preterm infant of any duration prior to
the onset
of active labour
or
Rupture of membranes in a term infant more than 24 hours prior to
the onset of
active labour
Feeding difficulties
Feeding intolerance (e.g. vomiting, abdominal distension)
Signs of respiratory distress
Respiratory distress starting
more than 4 hours after birth
Preterm birth following spontaneous
labour (before 37 weeks gestation)
Hypoxia
Suspected or confirmed rupture of membranes more than 18hours
in pre-term birth
Jaundice within 24 hours after birth
Apnoea
Intrapartum fever higher than 38°C or confirmed or suspected
chorioamnionitis
Signs of neonatal encephalopathy.
Parenteral antibiotic treatment given to the woman for
confirmed or suspected invasive bacterial infection (such as
septicaemia) at any time during labour, or in the 24-hour
periods before and after the birth [This does not refer to
intrapartum antibiotic prophylaxis]
Seizures
Need for CPR.
Need for mechanical ventilation in a preterm baby.
Need for mechanical ventilation in a term baby.
Suspected or confirmed infection in another baby in the case of
a
multiple pregnancy
Persistent fetal circulation Temperature instability
(less than 36°C or more than 38°C) not environmental
Signs of shock
Abnormal coagulation.or thrombocytopenia
Oliguria persisting beyond 24 hours
after birth
Hypoglycaemia or hyperglycaemia.
Metabolic acidosis (≥-10mmol/L).

LP
• If strong clinical suspicion of infection
• Clinical symptoms or signs suggesting meningitis
• Consider performing an LP in those who did not have
an LP at presentation if
• CRP≥10mg/l or
• Have a positive blood culture or
• In those not responding satisfactorily to antibiotic treatment
• L&D use first CRP≥20mg/l or second CRP≥50mg/l as guide for
LP
Local Experience: Review
• Total episodes 169.
• 77 Female and 92 male.
• 129 Term and 40 Preterm.
• Gestation between 25+6 to 40+
weeks.
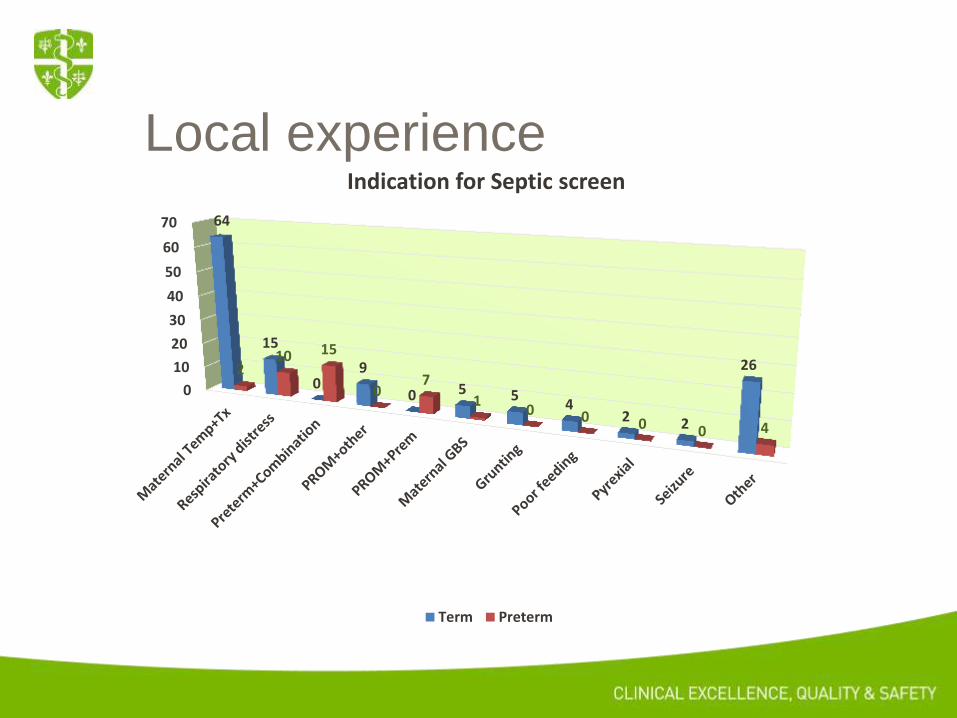
Local experience
0
10
20
30
40
50
60
70 64
15
0 9
0 5 5 4
2 2
26 2 10 15
0 7
1 0 0 0 0 4
Indication for Septic screen
Term Preterm

Local experience
Local experience: LP
Total 23/169 (13.5%) met our criteria for LP ( NICE 53/169- 31%)
• 2 failed attempts and 1 unstable baby-not performed.
• 7/23 LP’s where first CRP >20.
• 13/23 where first CRP <20 and 2nd CRP >50.
Local experience
0
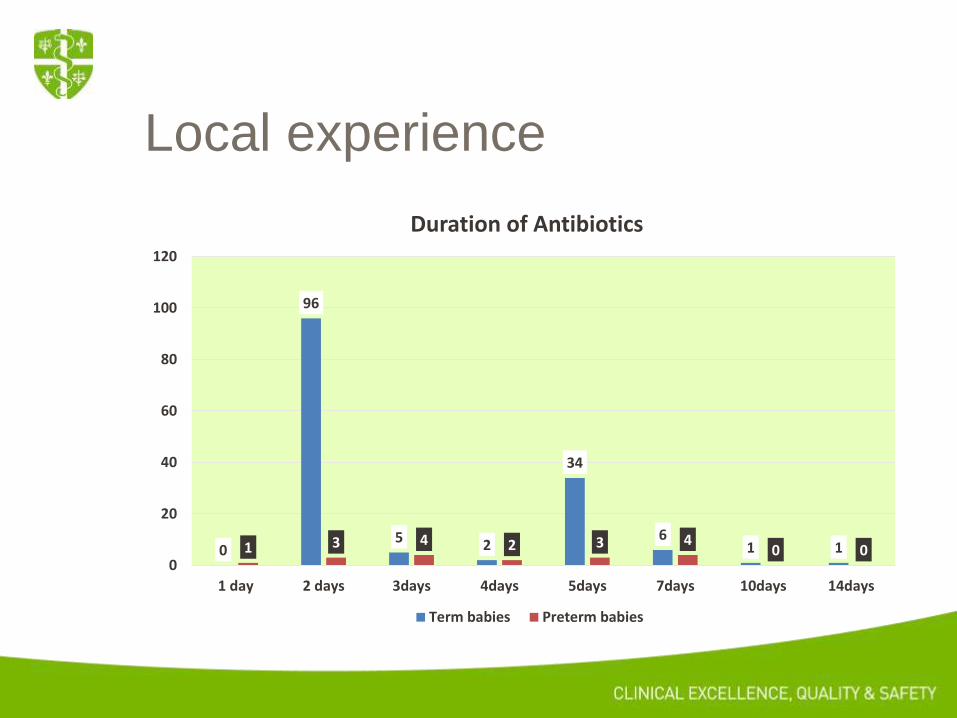
96
5 2
34
6 1 1 1 3 4 2 3 4
0 0 0
20
40
60
80
100
120
1 day 2 days 3days 4days 5days 7days 10days 14days
Duration of Antibiotics
Term babies Preterm babies

Local experience
2
1
4
1
2
1
2
1
Indication for readmission to Paediatrics (Total 15)
Bronchiolitis Abdo distension+temp Apnoeas Shunt infection
Vomiting UTI Poor feeding/floppy Unknown
Readmission
15 representations to Hospital.
• Day of life representation: 8-83days.
• 12/15 presentations within 28days of
life.
• Day 11 life: Blood culture- 1 positive
ESBL E.Coli-, CRP 148-
vomiting+grunting,LP normal.
• LP: 3 performed and normal, no
growth.

Local experience Readmssn day of life, Indication
Indication for NICU admission
NICU CRP,Days of TX CRP, Days of Tx
D15,Bronchiolitis Sibling with GBS Normal, 2 days Normal, 2 days
D21,abdo disten Resp distress Normal, 2days Normal, 2 days
D8,apnoea Prem,resp distress Normal, 2days Normal, 2days
D28,apnoea Prem,resp distress Normal, 2days Normal, 2days
D11, vomiting/PS Mat pyrexia+Tx Raised,5days Normal, transferred
D11,ESBL E.Coli Focal seizure, paeds Raised, ?days-paed Raised, 14days
D15,Tachypnoea Tachypnoea Normal, 2days Normal, 2days
Not treated 4 babies
Other Normal, 2days Normal, no Treatment
D29,Bronchiolitis Tachypnoea Raised, 5days Abnormal, 7days

Conclusions
It is safe to follow our NICU criteria for-
a) identifying at risk neonates and
b) raising the CRP’s limits for otherwise well neonates
without adversely impacting the outcomes for the neonates treated.


Thank You.







