
The Patient with Aortic Stenosis
and Mitral Regurgitation
Prof. Patrizio LANCELLOTTI , MD, PhD
Heart Valve Clinic, University of Liège, CHU Sart
Tilman, Liège, BELGIUM
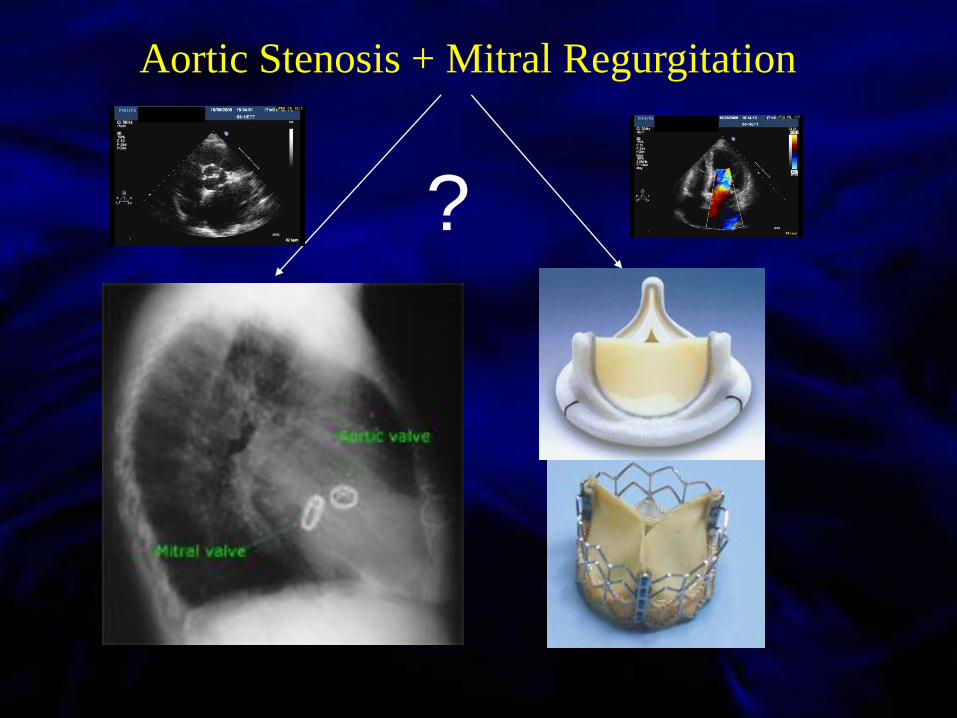
Aortic Stenosis + Mitral Regurgitation
?

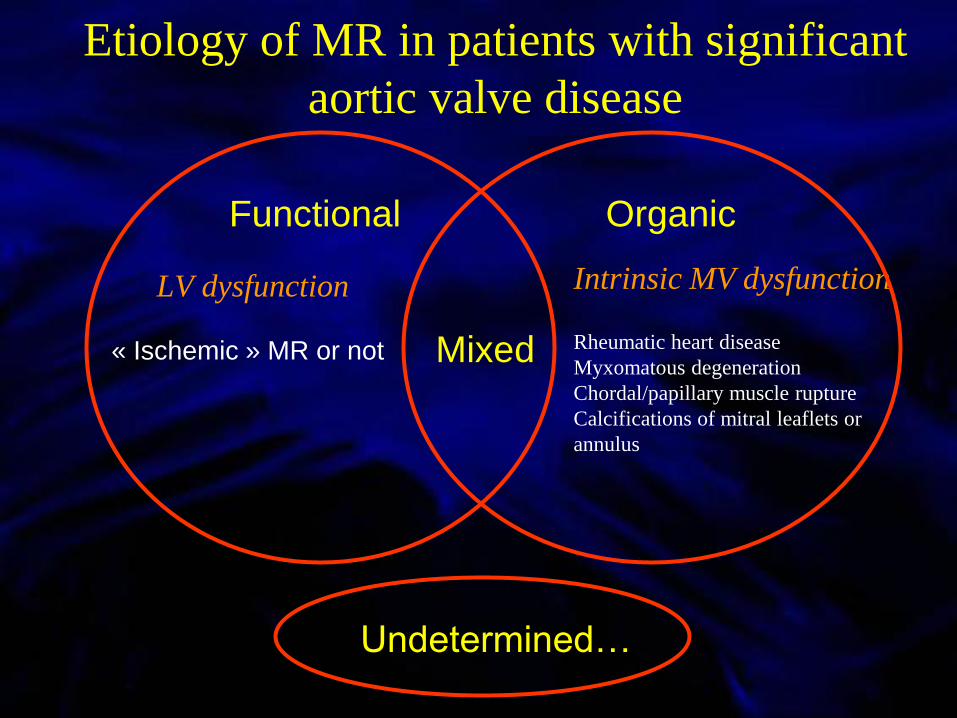
Etiology of MR in patients with significant
aortic valve disease
LV dysfunction
Functional
Mixed
Intrinsic MV dysfunction
Rheumatic heart disease
Myxomatous degeneration
Chordal/papillary muscle rupture
Calcifications of mitral leaflets or
annulus
Organic
Undetermined…
« Ischemic » MR or not
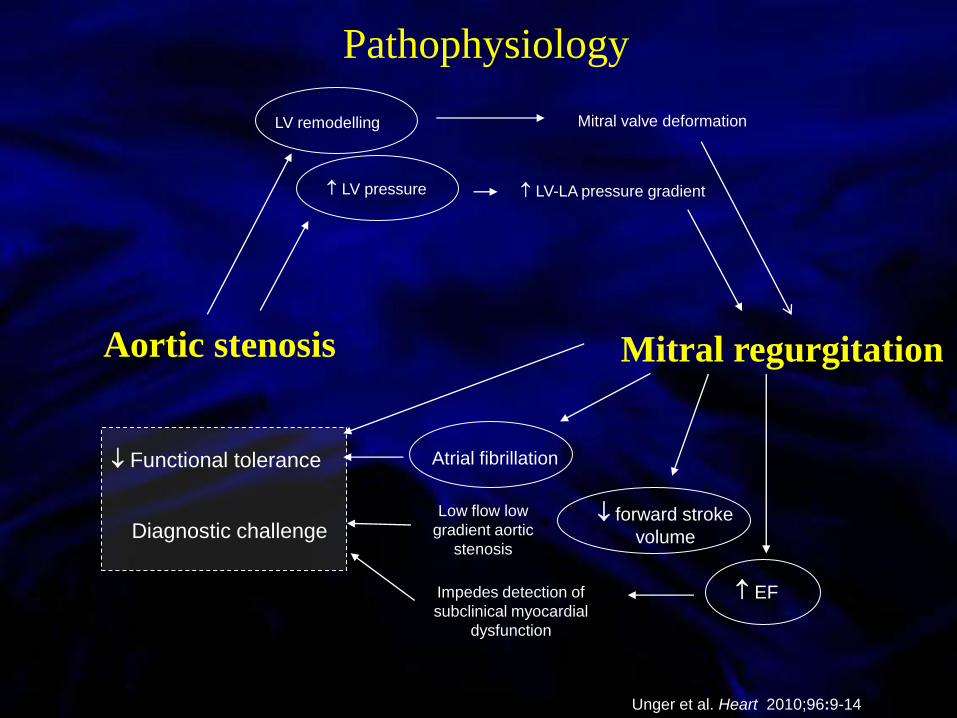
Mitral regurgitation
LV remodelling Mitral valve deformation
LV pressure LV-LA pressure gradient
Impedes detection of
subclinical myocardial
dysfunction
EF
Low flow low
gradient aortic
stenosisDiagnostic challenge
forward stroke
volume
Atrial fibrillation Functional tolerance
Aortic stenosis
Unger et al. Heart 2010;96:9-14
Pathophysiology

LVOT diameter 2,2 cm
Stroke volume 35 ml (18 ml/m²)
AVA 0.65 cm² (0,34 cm²/m²)
LVOT diameter 2,2 cm
Stroke volume 35 ml (18 ml/m²)
AVA 0.65 cm² (0,34 cm²/m²)

STS database 2005
http://sts.org/documents/pdf/Spring2005STS-ExecutiveSummary.pdf
10% of all cardiac procedures
5% of all AVR
+/-1000/yr
Prevalence

Authors, Year Number of
patients
Exclusion criteria Method of MR assessment Percentage of patients with
preoperative MR
Tunick
Am J Cardiol 1990
44 None Colour flow mapping 61% with ≥ mild MR
Adams
Am J Cardiol 1990
56* None Pulsed wave Doppler mapping 82% with ≥ 1+ MR
Tassan-Mangina
Clin Cardiol 2003
30 Severe AR
Unstable haemodynamic state
Arrhythmia
Colour flow mapping 90% with ≥ mild MR
Moazami
J Card Surg 2004
250 Organic mitral valve disease
Previous sternotomy or mitral
valve surgery
Colour flow mapping 78% with ≥ mild MR
Barreiro
Circulation 2005
408 Need for concomitant bypass
surgery
Age > 70 y
Colour flow mapping 17.2% with ≥ moderate MR
Ruel
Circulation 2006
848 Organic mitral valve disease
Patients who did not survive the
operation
2003 American Society of
Echocardiography
recommendations
12.6% with ≥ 2+ MR
Caballero-Borrego
Eur J Cardiothor
Surg 2008
577 Organic mitral valve disease
Predominant AR
Predominant coronary artery
disease
Type A aortic dissection
MR secondary to SAM
Colour flow and pulsed wave
Doppler mapping, pulmonary vein
flow
26.5% with non-severe MR
Waisbren
Ann Thor Surg 2008
227 Organic mitral valve disease
Combined procedure (CABG)
Endocarditis
Right heart valve procedure
Moderate or severe AR
Vena contracta width 74% with moderate MR
Prevalence of MR in patients undergoing isolated AVR
9 studies
N=2550
Variable
organic MVD (4)
≥moderate AR (3)
CAD/CABG (4)
Qualitative
or
semi-quantitative
≥mild: 60-80%
≥moderate: ±15%

Risk associated with double valve replacement
STS database 2005
http://sts.org/documents/pdf/Spring2005STS-ExecutiveSummary.pdf
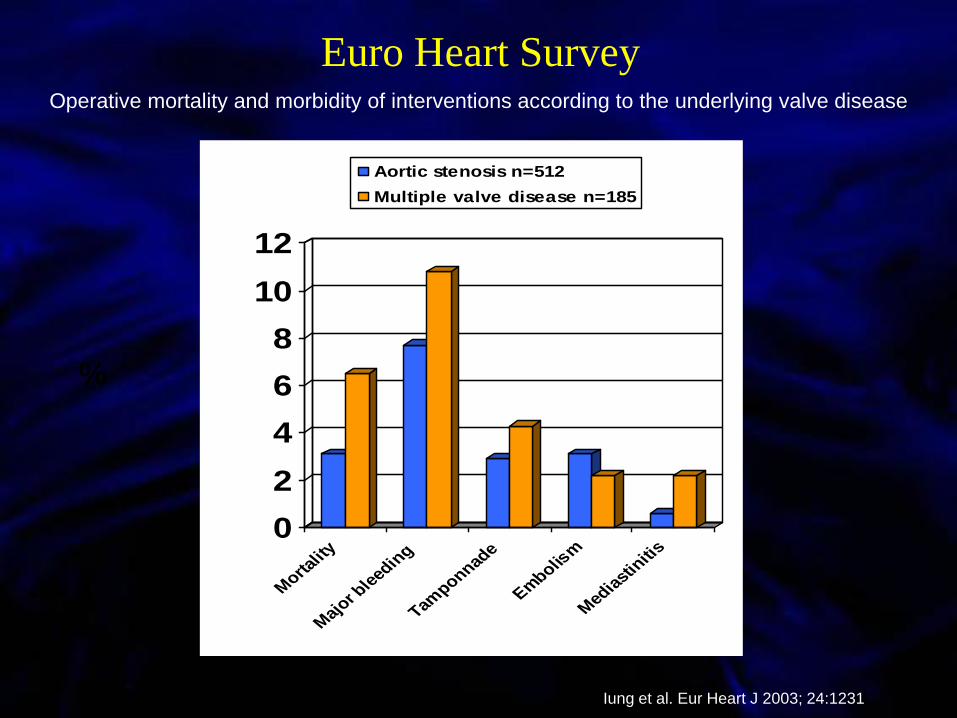
Operative mortality and morbidity of interventions according to the underlying valve disease
Iung et al. Eur Heart J 2003; 24:1231
%
Euro Heart Survey
0
2
4
6
8
10
12
Morta
lity
Maj
or ble
edin
g
Tamponnad
e
Embolis
m
Med
iast
initi
s
Aortic stenosis n=512
Multiple valve disease n=185
0
2
4
6
8
10
12
Morta
lity
Maj
or ble
edin
g
Tamponnad
e
Embolis
m
Med
iast
initi
s
Aortic stenosis n=512
Multiple valve disease n=185

Turina, J. et al. Circulation 1999;100:II-48-II-53
Long-term outcome after aortic
+ mitral valve replacement
Independent predictors of late
outcome:
• Age
• LVEF
• Additional tricuspid surgery
• NYHA class
• CAD requiring CABG

Mitral valve repair with AV replacement is
superior to double valve replacement
Gillinov AM, et al. J Thorac Cardiovasc Surg 2003; 125: 1372
Repair: N=295
Replacement: N=518
0
10
20
30
40
50
60
70
80
90
100
2 4 6 8 10 12 14 16
79
72 63
52
46
34
P=0.01
Mean follow-up 6.9±5.9 yrs
%
years
Surv
ival (%
)l

AVR + MV repair
AVR +
MVR
Talwar S, et al Ann Thorac Surg. 2007:84:1219
AVR + MV repair vs AVR + AVR
replacement/ event-free survival
p < 0.001

First author, Year Number of
patients with
MR ≥2
Aetiology of
MR
Prognostic value
Absil, Eur J
Cardiothoracic Surgery
2003
58 Functional No significant prognostic value
Ruel, Circulation 2006 107 Functional No significant effect on mortality
Wan, JTCVS 2009 190 Functional No independent prognostic value
Caballero-Borrego, Eur J
Cardiothoracic Surgery
2008 155 Functional Independent risk factor for
mortality and morbidity
Functional MR
Prognostic impact of MR in patients
undergoing isolated AVR
Age, diabetes, renal failure, LV dysfunction, Atrial fibrillation
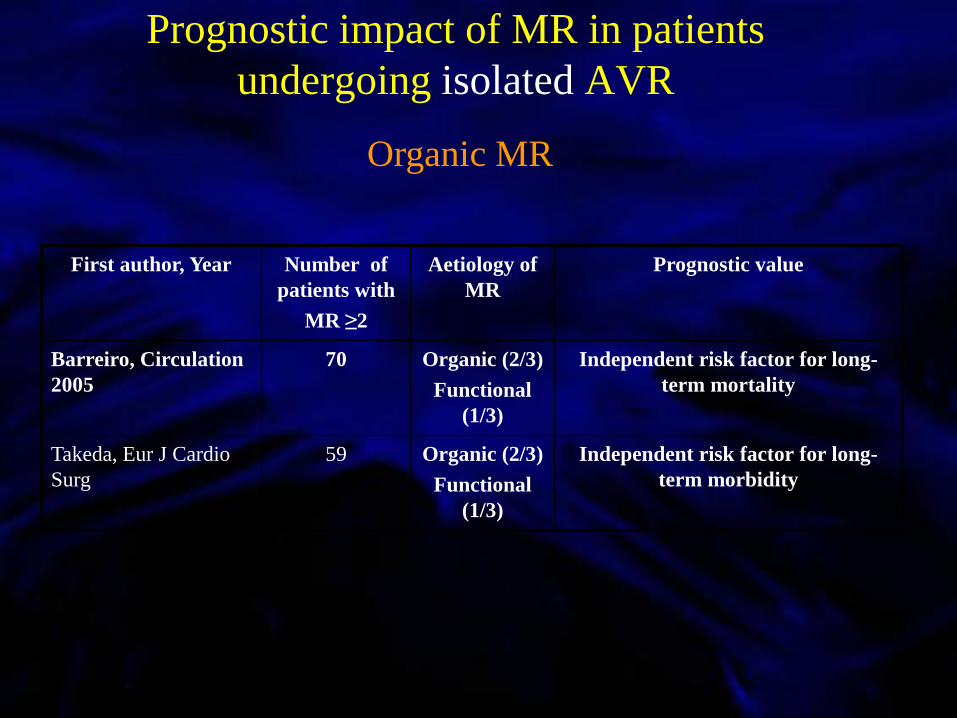
Prognostic impact of MR in patients
undergoing isolated AVR
Organic MR
First author, Year Number of
patients with
MR ≥2
Aetiology of
MR
Prognostic value
Barreiro, Circulation
2005
70 Organic (2/3)
Functional
(1/3)
Independent risk factor for long-
term mortality
Takeda, Eur J Cardio
Surg
59 Organic (2/3)
Functional
(1/3)
Independent risk factor for long-
term morbidity
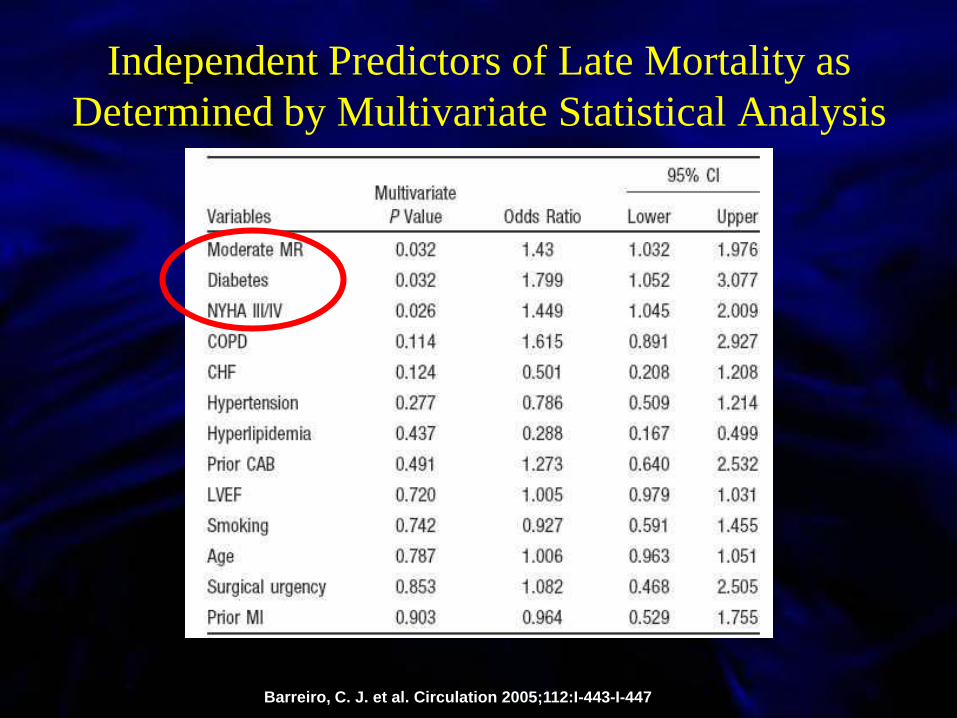
Independent Predictors of Late Mortality as
Determined by Multivariate Statistical Analysis
Barreiro, C. J. et al. Circulation 2005;112:I-443-I-447

First author, Year Aetiology of
MR
Number of patients Timing of the
postoperative echo
examination
Method of MR
assessment
% of patients with
improvement in MR
Tunick 1990 Functional
Organic
N = 27 with ≥ mild MR 58 days CFM 67%
Adams 1990 Organic
Functional
N = 46 with ≥ mild MR 6 months PW Doppler mapping 27%
Harris 1997 Functional N=28 with ≥ mild MR 2.5 months CFM 82%
Brasch 2000 Organic
Functional
N = 16 with ≥ moderate
MR
2.2 months CFM 44%
Christenson 2000 Functional N = 58 with ≥ mild MR 1 week
and
5 months
CFM 46%
and
60%
Tassan-Mangina
2003
Functional in
all except 2
patients
N = 23 with ≥ mild MR 19 days CFM 61%
Moazami 2004 Functional N = 80 with ≥ mild MR > 60 days CFM 45%
Barreiro 2005 Organic
Functional
N = 70 with ≥ moderate
MR
Early postoperative CFM 82% if functional
35% if organic
Ruel 2006 Functional N = 107 with ≥ 2+ MR 18 months 2003 ASE
recommendations
44-74%
Vanden Eynden 2007 Organic
Functional
N = 80 with ≥ moderate
MR
1 year CFM and PW Doppler
mapping, PV flow
35%
Caballero-Borrego
2008
Functional N =153 with non-severe
MR
Before hospital
discharge
CFM and PW Doppler
mapping, PV flow
72%
Waisbren 2008 Functional
No CABG
N = 60 ≤ mild MR
N = 167 ≥ moderate MR
Intraoperative Vena contracta width 66% of preop. moderate
MR
Wan 2009 Functional N=159 with ≥ moderate
MR
Discharge 2003 ASE
recommendations
76%
Impact of isolated AVR on MR
13 studies
Functional: 8
Functional + organic: 5
1014 patients
≥mild or
≥moderate MRFrom OR
up to
18 months
65-75%
(27-82%)
Qualitative or ½
quantitative studies
All retrospective studies
except one

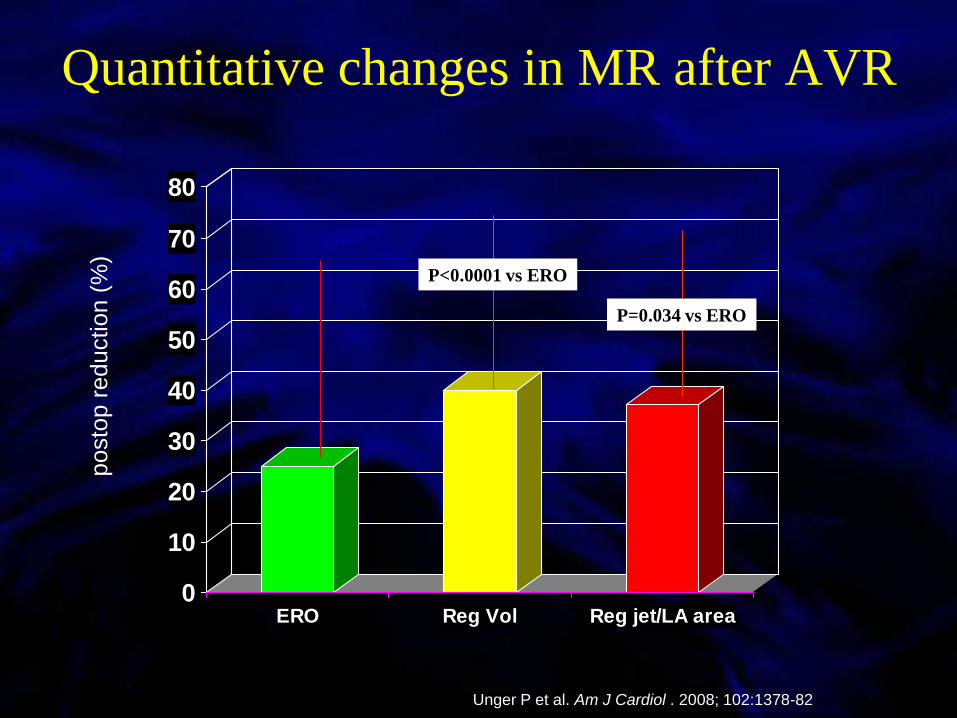
Quantitative changes in MR
after isolated AVR
Unger P et al. Am J Cardiol . 2008; 102:1378-82
0
10
20
30
40
50
60
70
80
ERO Reg Vol Reg jet/LA area
P=0.034 vs ERO
P<0.0001 vs ERO
Quantitative changes in MR after AVR
Unger P et al. Am J Cardiol . 2008; 102:1378-82
posto
p r
eduction (
%)

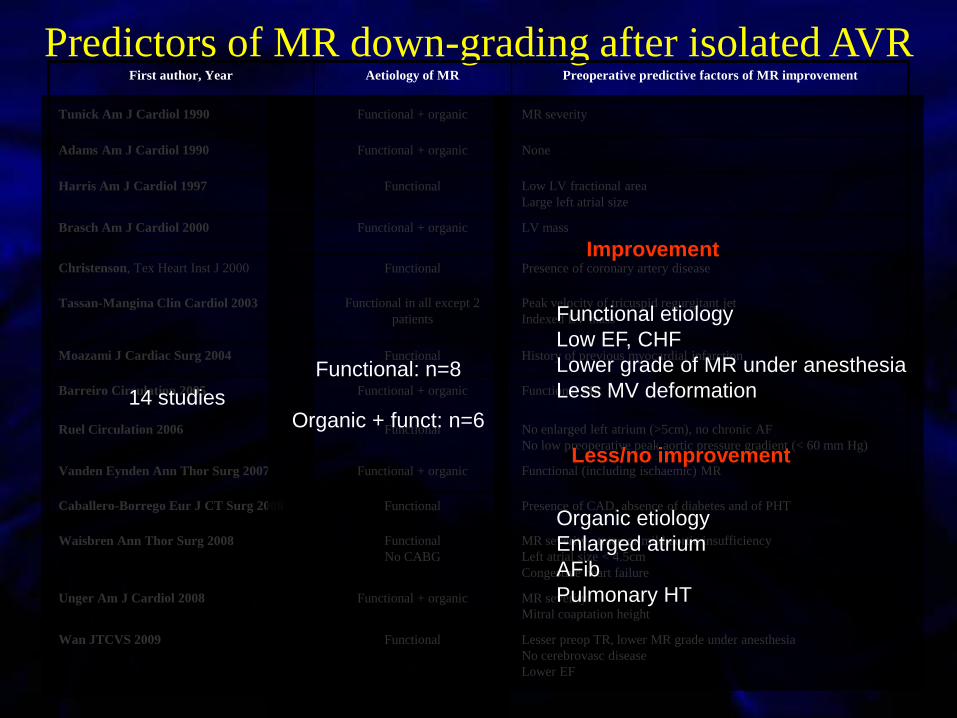
Predictors of MR down-grading after isolated AVRFirst author, Year Aetiology of MR Preoperative predictive factors of MR improvement
Tunick Am J Cardiol 1990 Functional + organic MR severity
Adams Am J Cardiol 1990 Functional + organic None
Harris Am J Cardiol 1997 Functional Low LV fractional area
Large left atrial size
Brasch Am J Cardiol 2000 Functional + organic LV mass
Christenson, Tex Heart Inst J 2000 Functional Presence of coronary artery disease
Tassan-Mangina Clin Cardiol 2003 Functional in all except 2
patients
Peak velocity of tricuspid regurgitant jet
Indexed LV mass
Moazami J Cardiac Surg 2004 Functional History of previous myocardial infarction
Barreiro Circulation 2005 Functional + organic Functional MR
Ruel Circulation 2006 Functional No enlarged left atrium (>5cm), no chronic AF
No low preoperative peak aortic pressure gradient (< 60 mm Hg)
Vanden Eynden Ann Thor Surg 2007 Functional + organic Functional (including ischaemic) MR
Caballero-Borrego Eur J CT Surg 2008 Functional Presence of CAD, absence of diabetes and of PHT
Waisbren Ann Thor Surg 2008 Functional
No CABG
MR severity, trace or mild aortic insufficiency
Left atrial size < 4.5cm
Congestive heart failure
Unger Am J Cardiol 2008 Functional + organic MR severity
Mitral coaptation height
Wan JTCVS 2009 Functional Lesser preop TR, lower MR grade under anesthesia
No cerebrovasc disease
Lower EF
14 studies
Functional: n=8
Organic + funct: n=6
Functional etiology
Low EF, CHF
Lower grade of MR under anesthesia
Less MV deformation
Organic etiology
Enlarged atrium
AFib
Pulmonary HT
Less/no improvement
Improvement

Changes in hemodynamic and echocardiographic data
according to mitral regurgitation etiology
Variables
Functional
MR
(n=20, 48%)
Organic
MR
(n=22, 52%)
P value
LV geometry and function
∆ Indexed LVED volume, ml 12±13 4±7 0.01
∆ Indexed LVES volume, ml 9±12 4±6 NS
∆ Indexed LV mass, g.m-2 9±25 5±26 NS
∆ LV ejection fraction, % -4±11 -5±8 NS
Mitral regurgitation
∆ Effective regurgitant orifice, mm2 5.8±5.2 2.8±4.3 0.04
∆ Regurgitant volume, ml 14.5±7 9.3±8.2 0.03

>1.4 cm²
0.7 cm
9.7 cm²
Preop Predictors of Persistent Functional MR
Matsumura Y et al. Am J Cardiol . 2010; 106: 701-706
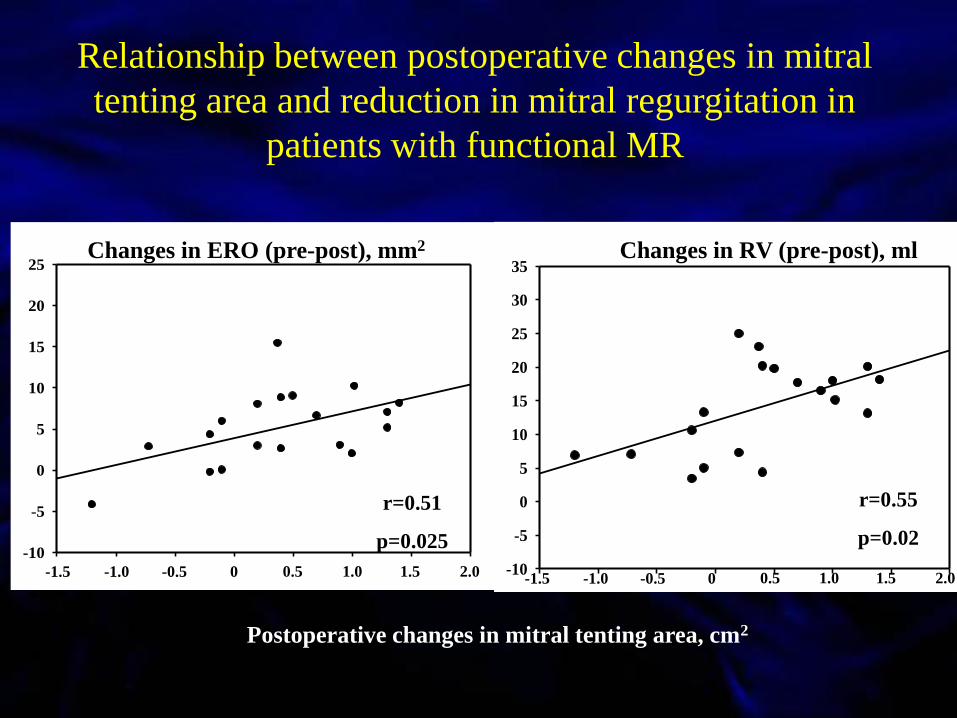
-10
-5
0
5
10
15
20
25
-1.5 -1.0 -0.5 0 0.5 1.0 1.5 2.0
Changes in ERO (pre-post), mm2
Postoperative changes in mitral tenting area, cm2
r=0.51
p=0.025
Relationship between postoperative changes in mitral
tenting area and reduction in mitral regurgitation in
patients with functional MR
-10
-5
0
5
10
15
20
25
30
35
-1.5 -1.0 -0.5 0 0.5 1.0 1.5 2.0
Changes in RV (pre-post), ml
r=0.55
p=0.02
Post
op
erati
ve i
mp
rovem
ent
in E
RO
, m
m2
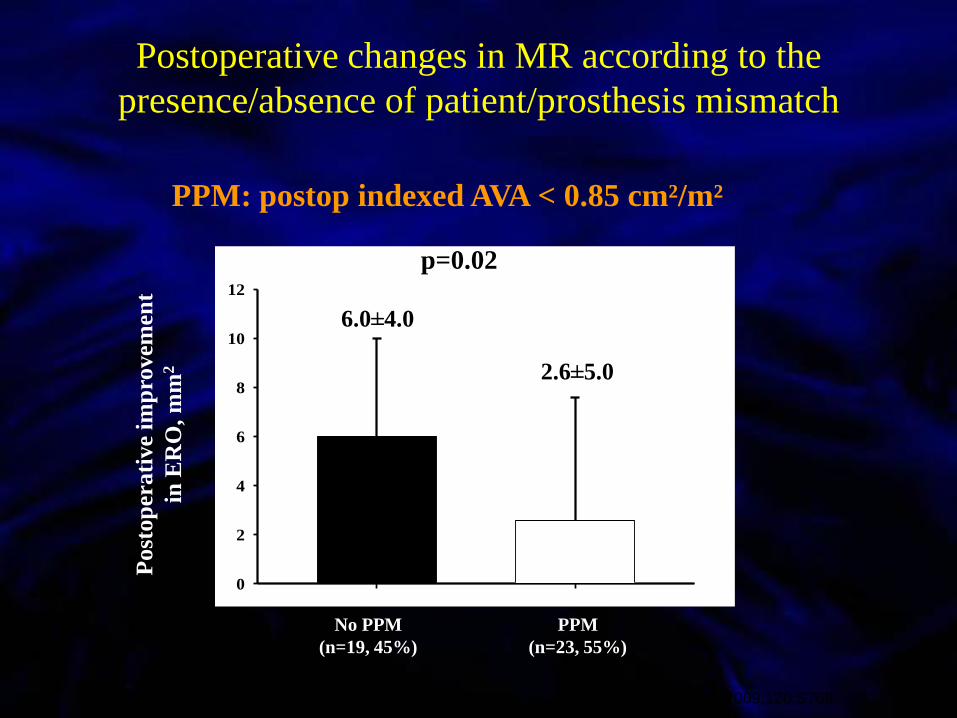
0
2
4
6
8
10
12
No PPM
(n=19, 45%)
PPM
(n=23, 55%)
6.0±4.0
2.6±5.0
p=0.02
Postoperative changes in MR according to the
presence/absence of patient/prosthesis mismatch
Unger P et al. (Abstract) Circulation. 2009;120:S768
PPM: postop indexed AVA < 0.85 cm²/m²

Relationship between aortic projected indexed EOA and
reduction in ERO (preop minus postop value)
A
-10
-5
0
5
10
15
20
r=0.44, p=0.01
Po
sto
per
ati
ve
cha
ng
es i
n E
RO
(p
re-p
ost
), m
m2
Projected indexed EOA, cm2.m-2
r=0.70, p=0.0003
r=0.14, p=NS
Functional MR
Organic MR
0.4 0.6 0.8 1.0 1.2
r=0.44, p=0.01
r=0.14, p=NS
Functional MR
r=0.70, p=0.0003
Organic MR
r=0.44, p=0.01
ACC/AHA 2006 Guidelines for the Management of
Patients With Valvular Heart Disease
« Remarkably few data exist to objectively guide the management of
mixed valve disease…
Hence, each case must be consider individually…
…the committee has developed no specific recommendations. »
2007 ESC Guidelines on the Management of
Valvular Heart Disease
« Data on multiple valve diseases are lacking and do
not allow for evidence-based recommendations.»
When is double-valve surgery indicated?

When is double-valve surgery indicated?
• If MR is severe
• …however,
– There are data on 40 patients with severe MR who
did not undergo surgical mitral valve intervention
• 90% of them had an improvement of at least one grade
• When is MR considered severe?

Ischaemic (functional) MR
≥ 20 mm² (1)
Organic MR
≥ 40 mm² (2)
Threshold of MR severity?
frequent downgrading
after AVR
less frequent downgrading
risk of future reoperation
≥ 30 mm²
1. Lancellotti et al. Circulation 2005
2. Enriquez-Sarano M. et al. N Engl J Med 2005

When is double-valve surgery (not)
indicated?
• Assessment of MR severity (ERO)
• Knowledge of functional or organic aetiology
• Suitability for MV repair
• Operative risk and comorbidities
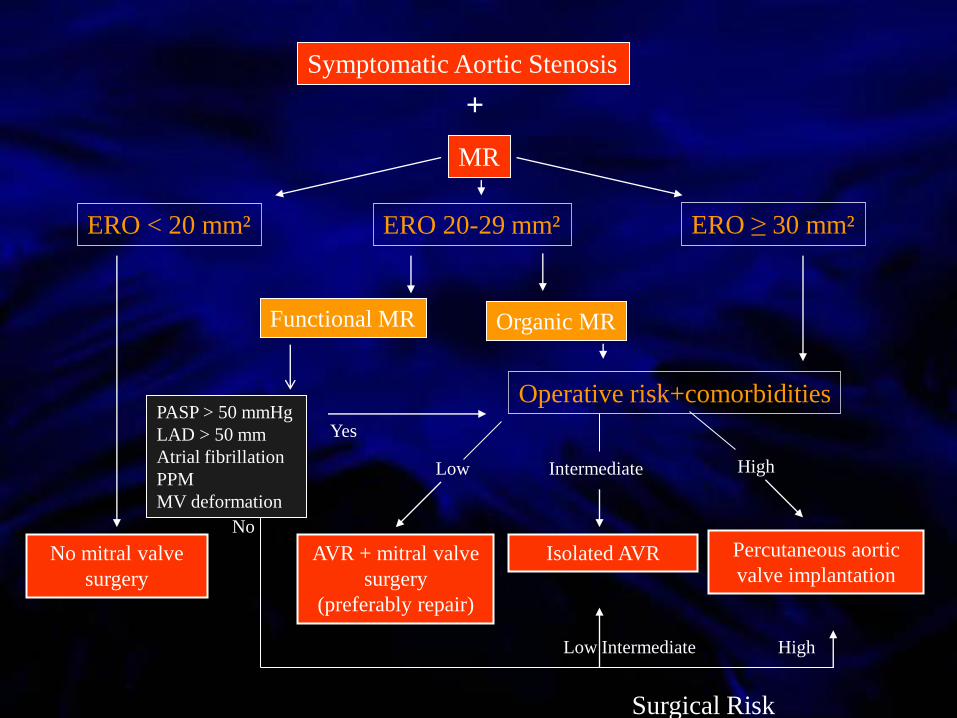
MR
Symptomatic Aortic Stenosis
ERO ≥ 30 mm²
Operative risk+comorbidities
Isolated AVR
Intermediate
AVR + mitral valve
surgery
(preferably repair)
Low
Percutaneous aortic
valve implantation
High
Yes
High
No
Surgical Risk
Low Intermediate
ERO < 20 mm²
No mitral valve
surgery
Organic MRFunctional MR
ERO 20-29 mm²
+
PASP > 50 mmHg
LAD > 50 mm
Atrial fibrillation
PPM
MV deformation







