The incidence of HIV associated Castleman’s disease
Professor Mark Bower
Chelsea & Westminster Hospital
London, UK

Castleman’s disease
Synonyms
Multicentric Angiofollicular Hyperplasia
Angiofollicular Lymph Node Hyperplasia
Angiomatous Lymphoid Hyperplasia
Castleman Tumor
Giant Benign Lymphoma
Hamartoma of the Lymphatics
Giant Lymph Node Hyperplasia

Castleman’s disease
Hyaline vascular Plasmablastic
Localised
Multi-centric HIV-MCD

IgM light chain restricted (monotypic polyclonal)
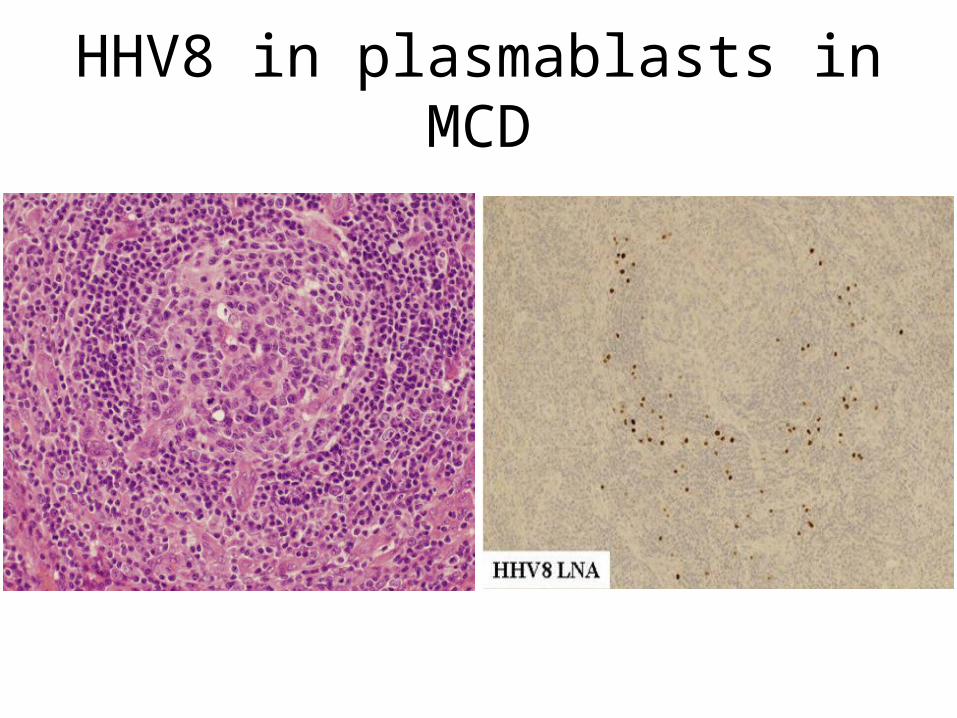
HHV8 in plasmablasts in MCD
MCD incidence in CWH cohort
1983-2007
10,997 patients
56,202 patient years follow-up

Overall incidence KS & MCD
MCD KS
Cases 24 1180
Incidence per 10,000 PY (95%CI)
4.3
(2.7-6.4)
210
(198-222)
MCD incidence multivariate analysis
Unlike KS, incidence not related to:
Gender
Prior AIDS diagnosis
MCD incidence multivariate analysis
MCD risk associated with:
Increasing age
Non-Caucasian ethnicity
Shorter duration HIV positive
Higher CD4 nadir count
Not on HAART

Risk by nadir CD4 count
0.1
1
10
100
1000
>200/mm3 50-200/mm3 <50/mm3
MCD
KS
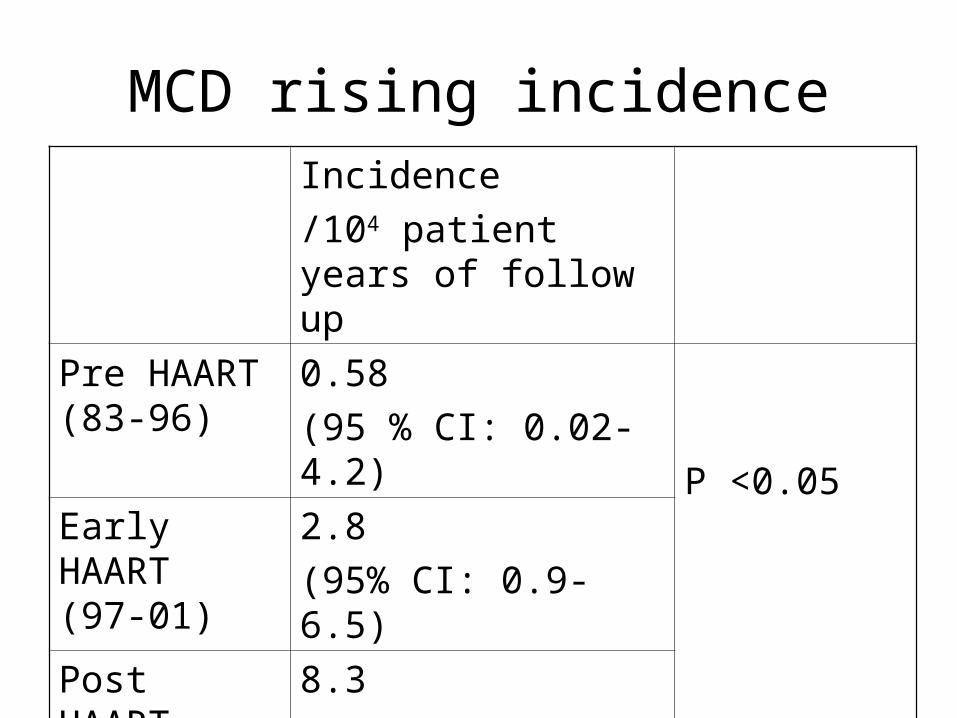
MCD rising incidenceIncidence
/104 patient years of follow up
Pre HAART (83-96)
0.58
(95 % CI: 0.02-4.2)
P <0.05Early HAART (97-01)
2.8
(95% CI: 0.9-6.5)
Post HAART (02-07)
8.3
(95% CI: 4.6-12.6)

Changing incidence over time
0.01
0.1
1
10
100
1000
Pre HAART(1983-1996)
Early HAART(1997-2001)
Post HAART(2001-2007)
MCD
KS

Plasma HHV8 viraemia
HHV8 detectable
HIV+ MCD 25/30 (83%)
2 p <0.0001HIV+ KS 26/73 (35%)
HIV+ Lymphoma 2/74 (3%)
HIV+ controls 0/53 (0%)
Lightcycler quantitative PCR for orf-72
240 HIV+ individuals

Median HHV8 VL
Median in detected
MCD 26,000 41,000
KS 0 3,900
1
10
100
1000
10000
100000
1000000
1E7
HH
V8
VL
MCD KS Other cancer HIV
Higher viral load HHV8 in MCD

Management of MCD
Rituximab
Splenectomy if splenomegally
Etoposide if severe symptoms
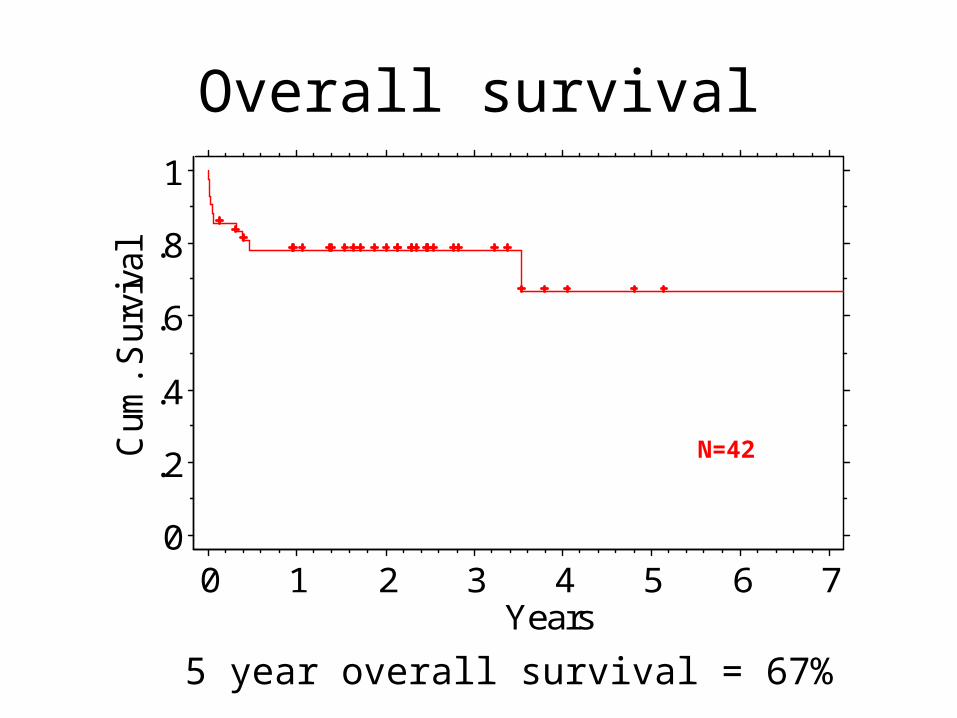
Overall survival
0
.2
.4
.6
.8
1C
um. S
urvi
val
0 1 2 3 4 5 6 7Years
N=42
5 year overall survival = 67%
Conclusions
• The incidence of MCD is rising
• MCD is not associated with degree of immunosuppression
• Plasma HHV8 is a diagnostic marker of MCD
• Long term remissions and 5 year survival of 67% can be achieved







