
The EINSTEIN DVT Study
'Xarelto' for the Acute and Continued Treatment of Symptomatic Deep Vein Thrombosis

Effective VTE Treatment Matters
Patients who experience acute VTE (DVT or PE) are at risk of recurrent episodes and complications such as post-thrombotic syndrome
PE is a potentially fatal consequence of VTE, and is frequently asymptomatic An estimated 540,000 VTE-related deaths occur annually in Europe1
1. Cohen et al, 2007
*In EuropeCombined deaths VTE-related deaths*
0
100,000
200,000
300,000
400,000
500,000
600,000
209,926
543,454
AIDSBreast cancerProstate cancer
Transport accident
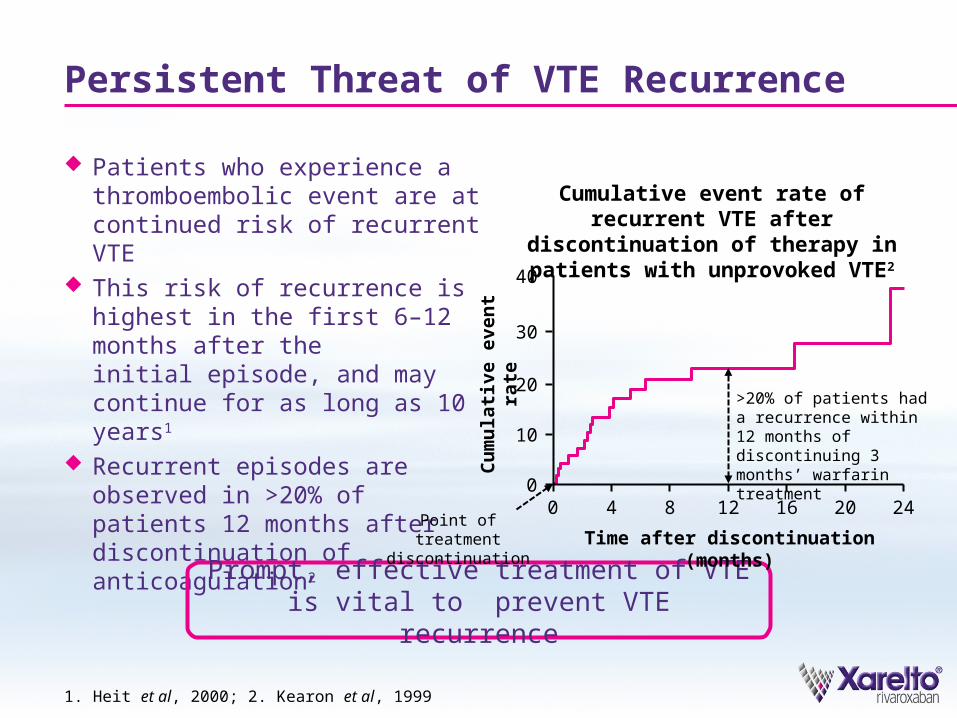
Persistent Threat of VTE Recurrence
Patients who experience a thromboembolic event are at continued risk of recurrent VTE
This risk of recurrence is highest in the first 6–12 months after the initial episode, and may continue for as long as 10 years1
Recurrent episodes are observed in >20% of patients 12 months after discontinuation of anticoagulation2
Prompt, effective treatment of VTE is vital to prevent VTE recurrence
1. Heit et al, 2000; 2. Kearon et al, 1999
Cumulative event rate of recurrent VTE after discontinuation of therapy in
patients with unprovoked VTE2
Cu
mu
lati
ve e
ven
t ra
te
40
Time after discontinuation (months)
30
20
10
00
4 8 12 16 20 24
>20% of patients had a recurrence within 12 months of discontinuing 3 months’ warfarin treatment
Point of treatment discontinuation

'Xarelto': Simple and Effective Single-Drug Approach for VTE Treatment
'Xarelto' is fast-acting and has minimal drug–druginteractions1
'Xarelto' has no need for routine monitoring or frequent dose adjustment1
1. Perzborn et al, 2011; 2. Kubitza et al, 2013
'Xarelto' acts as fast as enoxaparin and can be given at the initiation of DVT and PE treatment
'Xarelto' exerts similarpharmacodynamic effects to enoxaparin2
40
30
20
10
00
4 8 12 16 20 24A
nti
-Fac
tor
Xa
acti
vity
(n
g/m
l en
oxa
par
in)
Time (hours)
Enoxaparin (n=10)'Xarelto' (n=11)

The EINSTEIN DVT Study Design Included an Initial Intensified Regimen of 'Xarelto'
A single-drug approach with 'Xarelto' was used in EINSTEIN DVT An intensified dose of 'Xarelto' (15 mg bid) was given for the first 21 days to provide
protection when patients are at highest risk of recurrence After 21 days 'Xarelto' 20 mg od was given to provide continued protection against VTE
recurrence
Primary efficacy outcome: symptomatic recurrent VTE (composite of recurrent DVT, non-fatal PE or fatal PE)
Principal safety outcome: composite of major or clinically relevant non-major bleeding
The EINSTEIN Investigators, 2010
15 mg bidObjectively confirmed DVT
without symptomatic PE
N=3449
'Xarelto' Day 1 Day 21
Enoxaparin (1.0 mg/kg) bid for at least 5 days,
plus VKA target INR 2.5 (INR range 2.0–3.0)
Predefined treatment period of 3, 6 or 12 months
20 mg od
'Xarelto'
R
30
-da
y
ob
se
rva
tio
n
pe
rio
d

Effective DVT Treatment Matters
Time to event (days)
Cu
mu
lati
ve e
ven
t ra
te (
%)
0 30 60 90 120 150 180 210 240 270 300 330 3600
1.0
2.0
3.0'Xarelto' (N=1731)
Enoxaparin/VKA (N=1718)4.0
HR=0.68 (95% CI 0.44–1.04)
p<0.001 for non-inferiority
p=0.08 for superiority
The EINSTEIN Investigators, 2010
Intention-to-treat population
'Xarelto' and standard of care had similar efficacy in the reduction of symptomatic recurrent VTE

Safety Matters: Similar Rates of Clinically Relevant Bleeding
Enoxaparin/VKA (N=1711)
'Xarelto' (N=1718)
Time to event (days)0 30 60 90 120 150 180 210 240 270 300 330 360
0Cu
mu
lati
ve e
ven
t ra
te (
%)
2
4
6
8
10
12
14
HR=0.97 (95% CI 0.76–1.22)
p=0.77
The EINSTEIN Investigators, 2010
Safety population
'Xarelto' and standard of care had similar rates of major and clinically relevant non-major bleeding
'Xarelto' Enoxaparin/VKA
n (%) n (%)
First major/clinically relevant non-major bleeding
139 (8.1) 138 (8.1)
Major bleeding 14 (0.8) 20 (1.2)
Contributing to death 1 (<0.1) 5 (0.3)
In a critical site 3 (0.2) 3 (0.2)

'Xarelto' can be Used in a Wide Range of Patients With DVT
Efficacy and safety outcomes were consistent across key patient subgroups including age, sex, body weight, renal function and active cancer
'Xarelto' was associated with a similar rate of adverse events, including vascular events, compared with standard of care
There was no evidence of liver toxicity in patients who received 'Xarelto'
The EINSTEIN Investigators, 2010

'Xarelto' (N=1731), %
Enoxaparin/VKA(N=1718), %
HR (95% CI) p-value
Net clinical benefit*
2.9 4.20.67
(0.47–0.95)0.03
Favourable Benefit–Risk Balance Matters
The EINSTEIN Investigators, 2010
*Defined as the composite of the primary efficacy outcome and major bleeding
Enoxaparin/VKA 'Xarelto' 0
1
2
3
4
54.2
2.9
Inci
den
ce (
%) RRR
33%(p=0.03)

Patients Matter: Improved Treatment Satisfaction with 'Xarelto'
A subanalysis of patients in EINSTEIN DVT showed that 'Xarelto' was associated with improved treatment satisfaction in patients with DVT, compared with standard of care1
· This included a reduction in patient-reported anticoagulation burden1
1. Bamber et al, 2013
'Xarelto' offers increased patient satisfaction, potentially improving compliance compared with
standard of care

'Xarelto': Simple DVT Management from Hospital to Home
EINSTEIN DVT supports simplified VTE treatment with a single-drug approach with 'Xarelto'
Similar efficacy and safety outcomes compared with standard of care
Consistent efficacy and safety outcomes irrespective of age, sex, body weight, renal function and cancer
Superior net clinical benefit compared with standard of care
Simplified, effective treatment of DVT

Pack Shot


BACK-UP SLIDES

'Xarelto' (N=1731)
Enoxaparin/VKA(N=1718)
Male patients (%) 57.4 56.3
Age, mean (years) 55.8 56.4
Weight (%)
≤50 kg 2.1 2.9
>50–100 kg 83.4 82.8
>100 kg 14.2 14.3
Creatinine clearance (%)
<30 ml/min 0.3 0.5
30–<50 ml/min 6.6 7.0
50–<80 ml/min 22.7 23.2
≥80 ml/min 68.9 68.1
Patient Characteristics: Similar in Both Study Arms in EINSTEIN DVT
The EINSTEIN Investigators, 2010
Intention-to-treat population

'Xarelto' (N=1731)
Enoxaparin/VKA(N=1718)
Intended treatment duration (%)
3 months 12.0 11.8
6 months 62.6 63.0
12 months 25.4 25.1
Pretreatment with LMWH/heparin/fondaparinux ≤48 h (%)
73.0 71.0
Active cancer (%) 6.8 5.2
Unprovoked VTE (%) 60.9 63.0
Patient and Treatment Characteristics: Similar in Both Study Arms in EINSTEIN DVT
The EINSTEIN Investigators, 2010
Intention-to-treat population

Bleeding Management in Clinical Practice
If bleeding events occur while patients are receiving 'Xarelto', they can be managed easily by measures used in clinical practice1,2
· There is no specific reversal agent currently available for 'Xarelto'; however, studies are ongoing3–5
1. Siegal et al, 2012; 2. Bauer KA, 2012; 3. Eerenberg et al, 2012; 4. Marlu et al, 2012; 5. Lu et al, 2013
Bleeding during anticoagulant treatment with
'Xarelto'
Minor bleeding e.g. gum or nose bleed
Major bleeding
Bleeding that cannot be controlled by
general or supportive measures
General measures Delay next dose or discontinue treatment
Supportive measures Mechanical compression Fluid replacement Haemodynamic support or blood products
Consider haemostatic procoagulant agents Prothrombin complex concentrate Activated prothrombin complex Factor VIIa







